
Abstract
Keywords
ADHD is a neurodevelopmental disorder that affects approximately 1 in 20 children (Polanczyk, De Lima, Horta, Biederman, & Rohde, 2007). The cause of ADHD is unclear; however, the frontostriatal (Teicher et al., 2000) and cerebellar brain circuitry (Berquin et al., 1998) have been implicated. ADHD–combined type (ADHD-CT) is characterized by symptoms of hyperactivity, inattention, or impulsivity. These symptoms may present as an inability to focus on a single task for extended periods of time, interrupting others, impatience, and hyperactive motor output such as fidgeting (American Psychiatric Association [APA], 2000). In addition to the psychosocial symptoms, up to 50% of children with ADHD-CT are reported to show motor performance below age expectancy (Piek, Pitcher, & Hay, 1999) and may meet diagnostic criteria for developmental coordination disorder (DCD; Flapper, Houwen, & Schoemaker, 2006).
In the last 10 years, there have been several studies investigating various aspects of motor ability in children with ADHD-CT (Racine, Majnemer, Shevell, & Snider, 2008) including investigations of handwriting proficiency. Handwriting is a goal-oriented task that requires fine motor coordination and is thus likely to be sensitive to subtle deficits. Previous findings in children with ADHD-CT indicate that handwriting impairments appear to be characterized by faster and more efficient movements with poorer quality of writing, irregular spatial arrangement, and more unrecognizable letters (Adi-Japha et al., 2007; Racine et al.,2008; Rosenblum, Epsztein, & Josman, 2008). In addition, Flapper et al. (2006) found decreased performance in a manual dexterity task, lower quality handwriting, and faster and more fluent grapho-motor drawing in 12 children with ADHD-CT and combined DCD. Adi-Japha et al. (2007) reported a similar handwriting profile in children with ADHD-CT without comorbid DCD—faster, but more inaccurate and more inefficient handwriting than in typically developing (TD) children (Adi-Japha et al., 2007). Furthermore, Adi-Japha et al. reported larger height and width of words and increased pen pressure in children with ADHD-CT. Both studies concluded that a speed-accuracy trade-off may be occurring in children with ADHD-CT, based on the common pattern of results that children with ADHD-CT appear to sacrifice accuracy for speed, resulting in faster movements overall. However, these studies did not use kinematic analysis. A sensitive kinematic analysis of handwriting will shed new insights on the issue, in particular allowing comparisons with disturbances of movement trajectory associated with known disorders (e.g., cerebellar dysfunction). Recently, Frings et al. (2010) compared the handwriting size of children diagnosed with ADHD-CT(n = 10) with children with cerebellar lesions, as well as TD children. Children with ADHD-CT displayed a similar handwriting profile to those with cerebellar lesions, exhibiting increased letter size across a sentence-writing task. These authors concluded that the cerebellum might be involved in the maintenance of a consistent movement size in individuals with ADHD-CT (Frings et al., 2010).
A potentially confounding factor in past ADHD-CT motor research is the failure to account for the presence and extent of comorbid psychiatric and developmental factors. While comorbidity is often described as the norm, rather than the exception, for children with ADHD-CT, recent studies have focused on particular subgroups of comorbidity involving autism spectrum disorders, with findings suggesting that up to 30% of children with ADHD-CT have clinically significant autistic symptoms (Reiersen, 2007). Large cohort studies suggest that children in this ADHD-autism clinical subgrouping have greater impairments in motor functioning than children with ADHD-CT who do not have clinically elevated autistic symptoms (Reiersen, Constantino, Grimmer, Martin, & Todd, 2008). While the current Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000) does not allow for comorbid clinical diagnoses of autism and ADHD-CT, as stated in a recent review by Gargaro, Rinehart, Bradshaw, Tonge, and Sheppard (2011), “recent clinical opinion, research practice and theoretical models seem to suggest that co-morbidity between disorders is a real, relevant, and frequent occurrence” (p. 1086).
Two handwriting and fine motor control studies have taken into consideration the association of the severity of ADHD symptoms when investigating motor difficulties (Pitcher, Piek, & Hay, 2003; Tucha & Lange, 2004). These studies indicate that ADHD symptoms, particularly inattention, are strongly associated with motor difficulty. Pitcher et al.(2003) found that the different subtypes of ADHD(primarily inattentive, primarily hyperactive, and combined type) had a different motor profile measured on the Movement Assessment Battery for Children (MABC). The inattentive and combined subtypes performed worse on manual dexterity and ball skills compared with TD children. The primarily hyperactive children did not differ from TD children on any motor measures. The authors concluded that motor ability may be more impaired in individuals with poorer attention skills. Tucha and Lange (2004) reported similar attention findings, noting that medication improved attention in children and adults with ADHD, in turn improving handwriting performance. There have been many varied findings with regard to the handwriting profile of children with ADHD-CT. These varied findings probably stem from differences in handwriting tasks and screening procedures for the participants. Flapper et al. (2006) reported handwriting impairments in a group of children with ADHD-CT and comorbid DCD that were similar to those found by Adi-Japha et al. (2007) in a sample of children with ADHD-CT without DCD. However, the findings were stronger and more apparent in the ADHD-DCD sample than in the clean ADHD sample.
The aim of the present study was to investigate the handwriting profile of a sample of individuals diagnosed with ADHD-CT who have been screened and excluded if they meet diagnostic criteria for DCD or autism. Based on studies conducted by Flapper et al. (2006), we predicted that children with ADHD-CT will exhibit handwriting deficits, such as faster, more inaccurate, and more variable handwriting; however, we anticipated these deficits may be more subtle than those found in studies where comorbid disorders such as autism and DCD were not accounted for (e.g., Flapper et al., 2006). Second, based on findings by Pitcher et al. (2003), we predict a positive correlation between handwriting kinematics and ADHD-CT symptom severity measured on the Conner’s Rating Scale, considered the gold standard measure of ADHD symptoms. In particular, higher inattention scores (poorer attention skills) were predicted to correlate with more variable handwriting.
Method
Participants
Initial assessment and diagnosis of ADHD-CT was made by private pediatricians in Melbourne who referred participants to this study. To ensure that the participants met Diagnostic and Statistical Manual of Mental Disorders(4th ed.; DSM-IV; APA, 1994) criteria for ADHD-CT and did not have comorbid autistic symptoms, a doctoral-level trained graduate student (Author, N. P.), under the supervision of an experienced clinical psychologist (Author, N. R.), took a medical, behavioral, and developmental history during an interview with parents and tested participants for clinically significant autistic symptoms.
ADHD-CT group
In all, 16 boys diagnosed with ADHD-CT aged between 7 and 15 years were recruited from private pediatricians in Melbourne. These children fulfilled DSM-IV-TR (APA, 2000) criteria for ADHD-CT. Exclusion criteria included other comorbid neurodevelopmental disorders (such as autistic disorder or Asperger’s disorder); comorbid medical (e.g., tuberous sclerosis); or hearing or visual, movement (e.g., DCD), or genetic (e.g., fragile X syndrome) disorders other than the primary diagnosis of ADHD-CT. Participants were administered the Conners’ Rating Scale–Parent report, which measures ADHD symptom severity (Conners, 2001). The rating scale has several subscales, but only inattention, hyperactivity, and total ADHD scores were used. Internalizing disorders, autistic symptoms, and DCD were measured using the Developmental Behavior Checklist (DBC; Einfeld & Tonge, 2002), the Social Responsiveness Scale (SRS; Constantino & Gruber, 2007), and the MABC–second edition (MABC2; Henderson, Sugden, & Barnett, 2007), respectively. Two ADHD-CT participants who scored in the clinical range on the SRS and MABC2 were excluded, leaving 14 children with ADHD-CT for analyses. In all, 11 of 14 ADHD participants in the study were on medication ranging from long to short acting. Participants on stimulant medication such as methylphenidate (Ritalin) were asked to discontinue medication at least 24 to 72 hr prior to testing as standardized procedure reported in previous studies (Langleben et al., 2006; Leitner et al., 2007).
TD group
A total of 18 TD boys aged between 7 and 15 years with no prior history of psychological, neurological, or psychiatric diagnoses were recruited from local schools and communities. The DBC, SRS, and MABC2 were also administered to the TD group to screen for internalizing disorders, autistic symptoms, and DCD. Furthermore, the Conners’ Rating Scale (Conners, 2001) was used to screen the TD group for ADHD symptoms. In all, 4 TD children were excluded: 1 for having motor proficiency scores indicative of DCD, 1 for SRS scores indicative of severe autistic traits, and 2 were excluded for having Conners’ Rating Scale scores indicative of ADHD symptoms, leaving a total of 14 TD participants in the sample.
Cognitive functioning
The cognitive functioning of children with ADHD was assessed using an age-appropriate Wechsler Intelligence Scale for Children–fourth edition (WISC; Williams, Weiss, & Rolfhus, 2003). In the interests of saving time (given that a majority of TD children were tested during school hours), the Wechsler Abbreviated Scale of Intelligence (WASI; consisting of two verbal, Similarities and Vocabulary, and two performance, Block Design and Matrix Reasoning, subtests; PsychCorp, 1999) was used. The WASI is an abbreviated version of the WISC, which has verbal comprehension, perceptual reasoning, and Full Scale IQ scores that are comparable with the WISC; verbal comprehension = 0.82, perceptual reasoning = 0.76, and Full Scale IQ = 0.87 (PsychCorp, 1999).
TD participants were matched to clinical participants based on Full Scale IQ and age. Independent measures t tests revealed no significant IQ or age difference between the two groups; age, t(26) = 0.76, p > .05; IQ, t(26) = −0.37, p > .05. The two groups also had similar motor proficiency; t(26) = 1.17, p > .05 (see Table 1 for participant variables). As previous studies (e.g., Frings et al., 2010; Flapper et al., 2006) have reported significant effects in sample sizes of n = 10 and n = 12, respectively, we predicted that our sample size of n = 14 would yield sufficient power to detect any differences.
Mean and Standard Deviations of Age, IQ measures, MABC, and Conner’s Scores.

Note: MABC = Movement Assessment Battery for Children; ADHD-CT = ADHD–combined type; TD = typically developing; CRS = Conners’ Rating Scale; WISC-IV = Wechsler Intelligence Scale for Children–fourth edition; WASI = Wechsler Abbreviated Scale of Intelligence.
IQ was assessed using the WISC-IV in children with ADHD-CT and using the WASI in TD children.
Apparatus and Procedure
Participants were asked to write four cursive letter l’s at their preferred size. This task has previously been used to investigate motor abnormalities in individuals diagnosed with known frontostriatal (e.g., Parkinson’s disease) and cerebellar deficits (Phillips, Ogeil, & Müller, 2009; Phillips, Stelmach, & Teasdale, 1991), and it is known to reduce attentional demands, therefore tapping the motor rather than higher level cognitive end of the cognitive-motor processes involved in handwriting. Cursive letter l’s represent a simple letter combination, which is often executed in script, and additionally, the pen is not lifted from the surface so a continuous movement can be recorded. Participants first practiced five trials using pen and plain A4 sheet of paper, and then five trials were recorded on a graphics tablet (WACOM UD1212-R; www.wacom.com; see Van Gemmert, Teulings, Contreras-Vidal, & Stelmach, 1999) and noninking stylus controlled by a laptop computer. The digitizing device had an active surface area of 30.48 cm × 30.48 cm, a resolution of 0.001 cm, and a sampling frequency of 100 Hz. Recording commenced as soon as the pen touched the surface of the graphics tablet, and finished after the pen had been lifted for >1 s. Experiments were designed and conducted using MovAlyzeR (Version 5.8.1) software by Neuroscript L.L.C (http://www.neuroscript.net/movalyzer.php; see Caligiuri, Teulings, Dean, Niculescu, & Lohret, 2010).
Measures were averaged for each stroke per trial per condition. Stroke size (height in centimeters), duration (in milliseconds), and average pen pressure (Newtons) were calculated using MovAlyzeR software. The variability of handwriting strokes was indicated by a signal-to-noise ratio (SNR), calculated by dividing the mean value of each parameter by its standard deviation. Higher values indicate less (or better control over the) kinematic variable (Phillips et al., 1991). This was calculated for vertical size (stroke height) and pen pressure. An index of ballisticity was used as a measure of handwriting dysfluency (Phillips et al., 2009). Ballisticity was calculated by dividing the number of zero crossings in the acceleration function by the number of zero crossings in the velocity function. Higher values on this measure reflect less ballistic (more inefficient) movements. A profile of the relative duration of the accelerative phase with respect to total movement duration was calculated as an asymmetry ratio (Phillips et al., 2009).
Handwriting indices were compared between the two groups using six independent measures t tests on the handwriting variables. A Bonferroni adjustment was performed to account for inflated Type I error. Furthermore, we ran correlations on handwriting kinematics and Conners’ Rating Scale scores (as a measure of ADHD-CT symptom severity) for all participants. The Conners’ Rating Scale scores we used were the Inattentive and Hyperactive subscales as well as the total ADHD severity score. Typically, we deemed correlations between 0.21 and 0.4 to be fair, 0.4 and 0.6 to be moderate, 0.61 and 0.8 to be good, and 0.81 and 1.0 to be very good (Altman, 1991).
Results
Descriptive statistics for the cursive letter l’s task are reported in Table 2.
Mean ± Standard Deviations of Handwriting Measures in Children With ADHD-CD and TD Children.
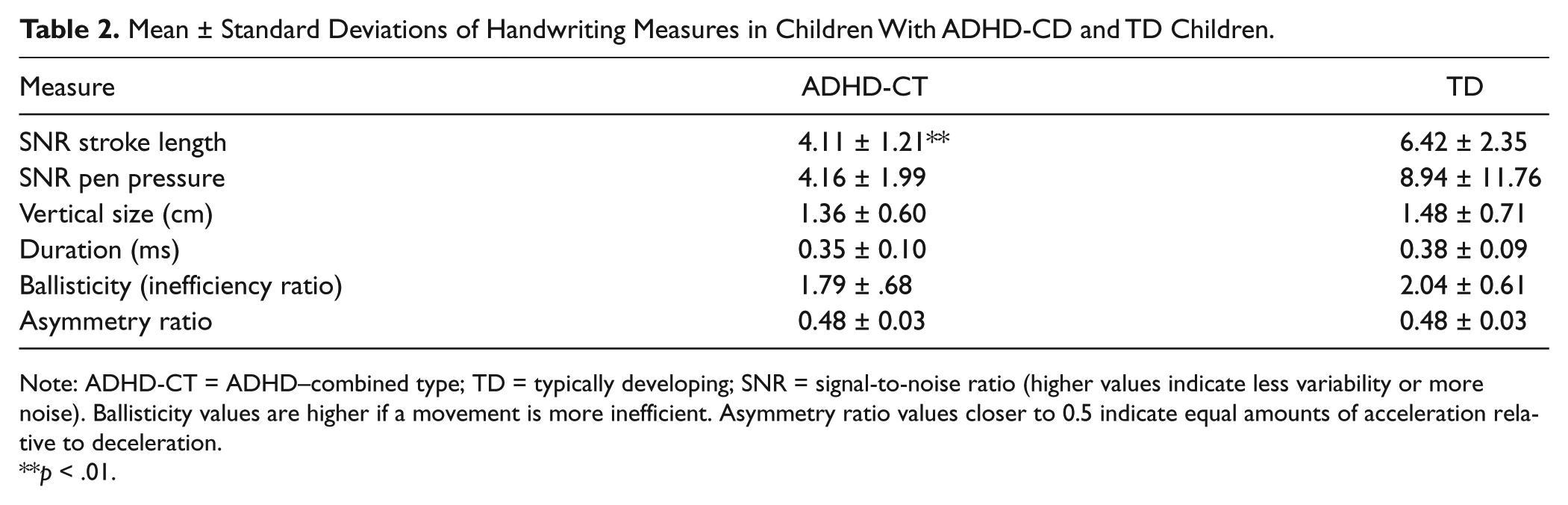
Note: ADHD-CT = ADHD–combined type; TD = typically developing; SNR = signal-to-noise ratio (higher values indicate less variability or more noise). Ballisticity values are higher if a movement is more inefficient. Asymmetry ratio values closer to 0.5 indicate equal amounts of acceleration relative to deceleration.
p < .01.
Independent measures t tests revealed that children with ADHD-CT had a lower SNR for stroke length (more variable or inconsistent stroke height) than TD children; t(26) = 3.27, p < .01, r = .29 (Table 2). The ADHD-CT group was not statistically different from the TD groups on any of the other kinematic variables.
Spearman’s correlations were performed to determine whether ADHD-CT symptom severity scores were associated with handwriting impairment (Table 3).
Spearman’s Correlation Coefficients for ADHD Symptom Severity and Handwriting Performance.
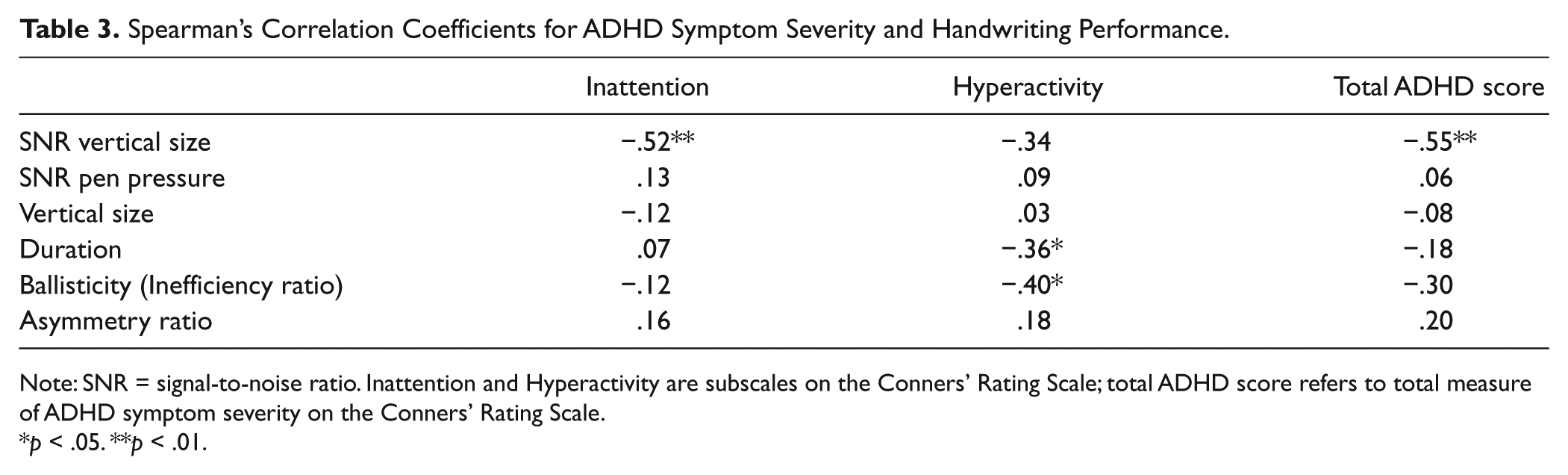
Note: SNR = signal-to-noise ratio. Inattention and Hyperactivity are subscales on the Conners’ Rating Scale; total ADHD score refers to total measure of ADHD symptom severity on the Conners’ Rating Scale.
p < .05. **p < .01.
Moderate correlations were found for SNR (variability) of stroke height (vertical size); higher scores on the inattentive and total ADHD-CT subtests were significantly correlated with more noisy (variable) writing size (Table 3). There were also fair correlations for stroke duration and ballisticity with hyperactivity; stroke duration was significantly related to hyperactive behavior such that a more hyperactive child had strokes of shorter duration (faster writing). Finally, ballisticity (lower scores indicate more efficient writing) was significantly associated with hyperactive behavior, indicating that a child who is more hyperactive will have movements that are more ballistic/efficient.
Discussion
The aim of this study was to investigate the handwriting profile of children diagnosed with ADHD-CT without elevated autistic or DCD symptoms. As predicted, when children with ADHD-CT were screened for other high prevalent comorbid neurodevelopmental diagnoses, the profile of handwriting difficulties was more subtle than that reported in previous studies (see Rosenblum et al., 2008, as an example). The current study found that children with ADHD-CT had more variable handwriting size compared with TD children (reflected in a lower SNR). In addition, ADHD symptomatology predicted performance on several handwriting variables, including variability of stroke size, stroke duration, and ballisticity (inefficiency). Greater ballistic efficiency was associated with hyperactivity as was stroke duration.
In contrast to findings of increased writing size being associated with cerebellar impairment by Frings et al. (2010), handwriting variability in our sample did not trend toward overall increased stroke size, but rather generally inconsistent sizing between strokes. This may be reflecting a form of dysmetria (lack of coordination of movement, usually presenting as undershoot or overshoot of target) or inability to judge distance or scale. Dysmetria may also refer to an inability to receive and process information rapidly to produce a fine-tuned response: http://en.wikipedia.org/wiki/Dysmetria-cite_note-sourcefour-0. Dysmetric movement is a common feature of disruption to the cerebellum (Hore, Wild, & Diener, 1991). Consequently, our finding of variable handwriting in a task without visual cues in children with ADHD-CT is consistent with the idea that cerebellar dysfunction contributes to motor abnormalities in this group.
Interestingly, pen pressure variability (SNR) appeared to differ between the groups, however, the TD group had a greater variability in their SNR which may account for the lack of significance. There were no significant differences in overall stroke size, stroke duration, ballisticity or movement asymmetry.
These findings indicate that in this simple “l” drawing task, there are still differences in children with ADHD; however, in comparison to a more complicated task, such as paragraph copying, there are fewer significant group differences. The advantage of this task, however, is that inattention is less confounding to results than in a more complicated task. That is, children with ADHD may be performing worse than TD children on other tasks (see Adi-Japha et al., 2007; Rosenblum et al., 2008) purely because of their inattention, such that findings may not be representing a motor impairment but a cognitive one. The aim of this study was to determine whether children with ADHD-CT would exhibit motor differences during a handwriting task, and it seems that this simple task has allowed us to do so.
A recent systematic review by Brossard-Racine, Majnemer, and Shevell (2011) reported that ADHD studies have proposed several different brain-behavior hypotheses to explain motor disturbance in children with ADHD. The authors found that none of the hypotheses were sufficient to explain all motor problems in ADHD. In support of our findings, however, the authors concluded that motor and cognitive pathways are simultaneously and equally affected in ADHD and that neurobiological motor deficits can be linked to cognitive deficits (Brossard-Racine et al., 2011).
In accordance with this theory and previous motor findings (Pitcher et al., 2003), more variable vertical size correlated with higher inattention scores. Higher total ADHD impairment score also correlated with more variable writing size. A more hyperactive child was also more likely to have shorter stroke duration (faster writing). Higher hyperactivity and total ADHD impairment scores also correlated with more ballistic movements. This is in accordance with a proposal by Adi-Japha et al. (2007) that a child who is more hyperactive will have movements that are more hyperkinetic and efficient (Adi-Japha et al., 2007). More ballistic movements have also been associated with other hyperkinetic movement disorders such as Huntington’s disease (Phillips, Bradshaw, Chiu, & Bradshaw, 1994). These findings indicate that ADHD symptomatology may be influencing motor performance in children with ADHD.
A limitation of the current study is that some ADHD medications have been found to have a protective effect such that, despite a wash-out period, there may be significant differences in the brains of children who have been medicated and medicine-naive children (Bledsoe, Semrud-Clikeman, & Pliszka, 2009). To improve on this, a medication-naive population should be used; however, this would be difficult to obtain as 20% of individuals with ADHD-CT are known to be on medication (Gargaro et al., 2011). Another limitation is the small sample size; given that ADHD-CT is a heterogeneous disorder, a larger sample size would improve the overall power of the study, although our sample size is comparable with other handwriting studies in ADHD-CT (Flapper et al., 2006; Frings et al., 2010). There is also a limit to the task used in this study. The task was chosen to minimize the cognitive end of the cognitive-motor spectrum in handwriting tasks, and our findings indicate that fine motor differences do exist independently of cognitive impairment, which is a key contributing factor to poor handwriting in ADHD-CT. Although the simplistic nature of the task may limit the ability to draw conclusions and inferences regarding more complex handwriting task, these results do indicate that there are fundamental motor differences in ADHD-CT that warrant further exploration.
In conclusion, children with ADHD-CT experience handwriting differences that are related to ADHD-CT inattention severity. It appears that in an ADHD-CT sample without comorbid autism and DCD, motor differences are present, but subtle. The subtlety is important as it indicates that the two groups are performing differently, but that the motor impairment is not as pronounced as would be expected to be universally acknowledged or included as a criterion for a diagnosis of ADHD, as is the case for autism (Fournier, Hass, Naik, Lodha, & Cauraugh, 2010). Future research comparing the neuromotor and handwriting profile of medication-naive individuals diagnosed with ADHD-CT only, autism only, and those who exhibit both ADHD and autism is needed to increase our understanding of the neurobehavioral and clinical definitions of these two closely related disorders.
Footnotes
Acknowledgements
The authors would like to thank all the children and families who participated in this research study, Monbulk Primary School, and Dr. Anne-Marie Turner, Dr. Katie Heathershaw, and Dr. Harriet Hiscock from the Melbourne Children’s Clinic.
Authors’ Note
Nicole Rinehart is an associate professor at Monash University and is also a clinical psychologist who consults at the Melbourne Children’s Clinic where children with ADHD were recruited from. She is also a member of the Australian National Health and Medical Research Council (NHMRC) Expert Working Group on ADHD Clinical Practice.
Declaration of Conflicting Interests
Nicole Rinehart is an associate professor at Monash University and is also a clinical psychologist who consults at the Melbourne Children’s Clinic where children with ADHD were recruited from. Assoc. Professor Rinehart is also a member of the Australian National Health and Medical Research Council Expert Working Group on ADHD Clinical Practice Points.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The funding for this research was provided in part by the National Health and Medical Research Council (NHMRC) and Monash University [Project Grant 436609; Project Grant APP1004387].