
Abstract
The implication of self-perceived competence for later adjustment has long been a controversy in developmental and clinical literatures. Some have suggested that positive self-perceptions are adaptive because they buffer individuals in failure situations and lead to greater task persistence and mastery of skills (Bjorklund, 1997; Taylor & Brown, 1988). However, others have argued that the benefits (or lack thereof) of positive self-perceived competence depend on children’s competency level (Colvin & Block, 1994) and may differ based on the area of adjustment examined (e.g., depression, aggression, or social abilities; Guerra, Asher, & DeRosier, 2004; Kistner, Balthazor, Risi, & Burton, 1999; McElhaney, Antonishak, & Allen, 2008). For instance, researchers suggest that positive self-perceptions, despite poor competency, may be protective with regard to the development of depression (Cole, 1990; Taylor & Brown, 1988) but may be a risk factor for aggressive behavior (Baumeister, Smart, & Boden, 1996). Some have also suggested that a lack of awareness of poor competence will inhibit improvement of skills (Colvin & Block, 1994) whereas others suggest that this thinking will increase persistence and skill development (Bjorklund, 1997). The implications of self-perceived competence may be especially important in the social domain given the importance of social functioning to later adjustment (Cowen, Pederson, Babigian, Izzo, & Trost, 1973) and the weight children and adolescents place on social relationships (e.g., Hartup, 1992).
Despite the suggestion by researchers that competency level should matter (Baumeister et al., 1996; Bjorklund, 1997; Colvin & Block, 1994), studies that have examined whether self-perceived social competence is moderated by social-functioning level have found that in normative samples, positive self-perceived social acceptance (SA) is adaptive regardless of social impairment level (Kistner et al., 1999; McElhaney et al., 2008). However, a major limitation of this research is that studies have not examined whether implications are comparable in clinical populations of children. For instance, in children with Attention-Deficit/Hyperactivity Disorder (ADHD), those that overestimate their social competence tend to have lower concurrent levels of depression but greater aggressive behavior and social impairments (Hoza et al., 2004; Hoza, Murray-Close, Arnold, Hinshaw, & MTA Cooperative Group, 2010; Hoza, Pelham, Dobbs, Owens, & Pillow, 2002; Murray-Close et al., 2010). Thus, for children with ADHD, positive self-perceived SA may have greater adaptive as well as maladaptive implications for those with poor social functioning. However, research has not directly tested whether social functioning moderates self-perceived SA in predicting adjustment for children with ADHD. To address this limitation in the literature, this study uses the Multimodal Treatment Study of Children With ADHD (MTA), which follows a sample of children with ADHD and a local normative comparison group (LNCG) longitudinally. Specifically, this study examines whether the relation between self-perceived SA and changes in three different areas of adjustment (depression symptoms, aggression/conduct problems, and social skills) is moderated by social-functioning level (as measured by peer-rated social preference) and ADHD diagnosis.
In normative samples, the implications of positive self-perceptions of SA differ depending on the domain of adjustment examined. Depression is one domain of adjustment that may be affected by self-perceived SA (see Jacobs, Reinecke, Gollan, & Kane, 2008, for a review). Cole’s (1990) competency-based model of depression posits that for children with poor social functioning, negative appraisals by important others, such as peers, lead to negative self-perceptions of competence and greater depression. This model suggests that children with low self-perceived SA and low peer status should be at greater risk for depression over time. In normative studies, research does find that low self-perceived SA predicts increases in depression symptoms over time (Uhrlass, Schofield, Coles, & Gibb, 2009); however, the only study examining peer status as a moderator of this association failed to find evidence supporting moderation (Kistner et al., 1999). Instead, Kistner and colleagues (1999) found that low self-perceived SA predicted increases in dysphoria 7 years later, regardless of children’s peer status. Thus, within a nonclinical sample, level of social functioning, as measured by peer status, does not appear to affect the relative protective function of self-perceived SA. However, to our knowledge, this is the only study to directly test moderation, and processes have not been examined within more at-risk samples.
Self-perceptions of SA also have been proposed to relate to aggressive and delinquent behaviors. Baumeister and colleagues (1996) argue that children with high self-perceptions of SA are more likely to be aggressive when self-perceptions are challenged by negative social feedback. This perspective suggests that positive self-perceptions of SA should be associated with increases in aggression for children with poor social functioning. Indeed, research finds that children labeled as “rejected and aggressive” report positive social self-perceptions that do not differ from the self-perceptions of children with “average” peer status (Patterson, Kupersmidt, & Griesler, 1990), suggesting that relatively high self-perceived SA may be associated with aggression among low peer status children. On the other hand, McElhaney and colleagues (2008) tested moderation directly and found that adolescents who reported higher self-perceived SA were rated as lower in aggression regardless of peer status. However, adolescents with low self-perceptions of SA and low peer status were at increased risk for later aggression. To our knowledge, studies have not directly examined whether self-perceived SA also predicts delinquent behaviors. Some evidence does suggest that low self-esteem is associated with greater delinquency, although others have failed to find this association (see Baumeister, Campbell, Krueger, & Vohs, 2003, for a review). Differences in findings across studies may suggest that positive self-perceived SA serves as a protective function against aggression and delinquency for some children but is a risk factor for others (e.g., at-risk or rejected children).
Development of social abilities and skills may be another domain of adjustment affected by self-perceived SA. Bjorklund (1997) suggests that among preschool and early elementary schoolchildren, positive self-perceptions, despite low competence, help children persist in difficult tasks. Through persistence and practice, children have greater opportunity to try new behaviors and master skills (Bjorklund, 1997). However, Colvin and Block (1994) suggest that an awareness of poor competence may be necessary for individuals to alter future behavior and learn from mistakes. If so, high self-perceived SA may actually limit the acquisition of new skills for individuals with low peer status. When examined empirically, most evidence from normative populations suggests that positive self-perceived SA is associated with greater social abilities. For instance, in a sample of fourth- and fifth-grade students, a composite measure of positive self-perceptions of competence was associated with greater concurrent teacher-rated prosocial interpersonal skills (Scharf & Mayseless, 2009). Only one study has examined whether peer status moderates the relationship between self-perceived SA and social abilities. Results indicated that adolescents who reported positive self-perceived SA demonstrated greater peer-rated companionship regardless of their peer status but that those with low self-perceived SA were low in companionship only if they were also low in peer status (McElhaney et al., 2008). Thus, existing evidence suggests that in normative samples positive self-perceived SA may be adaptive with regard to increased social skills and abilities.
In sum, although limited, normative studies generally suggest that positive self-perceptions of SA are adaptive regardless of social-functioning level. However, a major limitation of research thus far has been that studies have failed to consider whether implications may differ in clinical populations, such as in children with ADHD. Understanding the implications of self-perceived SA to adjustment may be especially important for children with ADHD given that they are at greater risk for depression, aggression/delinquency, and poor social skills (Biederman et al., 2006; Jensen, Shervette, Xenakis, & Richters, 1993; McQuade & Hoza, 2008; Molina et al., 2009; Thaper, van den Bree, Fowler, Langley, & Whittinger, 2006). In addition, more than 50% of children with ADHD are labeled as rejected by their peers (Hoza, 2007) and a subset demonstrate a positive bias and report high self-perceptions of SA despite being rated by adults as poor in social competence (McQuade, Tomb et al., 2011). To date, studies examining the implications of self-perceived SA for children with ADHD have typically examined discrepancy scores of child self-ratings and teacher ratings of competence in relation to adjustment. These studies have found that a greater overestimation of SA relative to teacher report is associated with fewer concurrent (but not future) depression symptoms (Hoza et al., 2010) and with greater aggression and conduct problems and social skill deficits (Murray-Close et al., 2010). However, studies utilizing discrepancy scores provide a measure of the extent of children’s overestimation of competence but fail to consider children’s level of self-perceived SA and social functioning as separate constructs. Thus, research has not examined whether the implication of positive self-perceived SA to changes in adjustment is moderated by peer status in children with ADHD.
We contend that for children with ADHD, positive self-perceived SA may be a stronger protective factor against depression for those who are low in peer status. Socially impaired children with ADHD are likely to encounter frequent negative social interactions with peers because of their high frequency of negative and annoying social behavior (Hoza, 2007). Cole’s (1990) competency-based model of depression would suggest that greater negative feedback from peers would place these children at increased risk for depression if they also internalize that feedback and have low self-perceptions of SA. Thus, children with ADHD and low peer status, more so than children without ADHD, may be at even greater risk of developing depression if they have low self-perceptions of SA. Although evidence does suggest that a reduction in self-perceived SA over time is associated with increases in depression symptoms in children with ADHD (McQuade, Hoza, Waschbusch, Murray-Close, & Owens, 2011) research has not examined whether peer status moderates the relationship between self-perceived SA and depression in this population.
Unlike comparison children, positive self-perceived SA also may have greater risks for aggressive and delinquent behaviors in children with ADHD. It is suggested that positive self-perceived SA should lead to aggression and delinquency specifically for individuals who experience negative social feedback (Baumiester et al., 1996) or who already have antisocial tendencies (Baumeister et al., 2003). This may be true for children with ADHD, whose poor impulse control may predispose them to aggressive and delinquent behaviors. This risk may be further exacerbated for children with ADHD and low peer status, who are likely to encounter more frequent negative social interactions (Pelham & Bender, 1982) and may therefore have more opportunities to respond aggressively. Thus, in contrast to the findings of McElhaney and colleagues (2008) reviewed earlier, high self-perceived SA may predict greater aggressive and delinquent behavior for children with ADHD, especially when accompanied by low peer status.
Finally, although it has been argued that positive self-perceptions lead to improvement in skills because of greater persistence on tasks (Bjorklund, 1997), this benefit may not be observed in children with ADHD. For instance, in a laboratory social interaction task, children with ADHD were actually less likely to persist during the task relative to control children, despite reporting positive perceptions of their social performance (Hoza, Waschbusch, Pelham, Molina, & Milich, 2000). These results support Colvin and Block’s (1994) assertion that positive self-perceptions in spite of poor social functioning may actually limit the ability to learn from mistakes and improve behavior. This may be especially true when children have attentional and impulse control problems that make it more challenging for them to attend to relevant input and adjust their behavior. Thus, unlike in comparison children, positive self-perceived SA despite low peer status may not lead to greater social skills for children with ADHD.
Thus, the goal of this study was to use the MTA sample of children with ADHD and normative comparison children to examine whether the relationship between positive self-perceived SA and adjustment over a 1-year period was moderated by peer-rated social preference and ADHD diagnosis. Implications were examined in three different domains of adjustment: depression symptoms, aggression and conduct problems, and social skills. Consistent with prior research examining moderation in a normative sample (Kistner et al., 1999; McElhaney et al., 2008), we expected that for comparison children, positive self-perceptions of SA would be adaptive regardless of peer status. However, for children with ADHD, it was hypothesized that peer status would moderate the relation between self-perceived SA and adjustment such that greater self-perceptions of SA would be protective against increases in depression but would be a risk factor for greater aggression and poorer social skills, particularly among those who were lower in peer status.
Method
Participants
A subset of 349 participants from the Multimodal Treatment Study of Children With ADHD (MTA) composed the sample for this study. The MTA was originally a randomized 14-month clinical trial of ADHD treatments jointly conducted by six independent research teams and the National Institute of Mental Health (NIMH). Children with ADHD (baseline n = 579) were recruited through schools, primary medical care facilities, mental health offices, advertisements, parent self-help groups, and word of mouth. In the original MTA study, children with ADHD met full diagnostic criteria for ADHD–combined type. Detailed descriptions of diagnostic and data collection procedures have been previously reported (Arnold et al., 1997; Greenhill, Abikoff, Arnold, & Cantwell, 1996; Hinshaw et al., 1997; MTA Cooperative Group, 1999).
At the 24-month time point (10 months following termination of treatment), a local normative comparison group (LNCG; baseline n = 289) was recruited from the same grades and schools with age and demographic characteristics similar to those of the children in the ADHD group. The LNCG was recruited for the ongoing follow-up portion of the study, comparing outcomes of LNCG and ADHD participants. The LNCG screening used the same inclusion/exclusion criteria (e.g., English speaking; IQ) as the ADHD sample except that they were not required to meet ADHD categorical or dimensional criteria. At the 24-month time point, a subset of children with ADHD and LNCG children completed sociometric procedures (47% of baseline sample). Thus, the first time point analyzed in this study corresponded to the 24-month assessment in the main MTA study, 2 years after initial recruitment and random assignment of children with ADHD to a 14-month period of intervention. At the 24-month time point, 111 of the 226 participants with ADHD in the present study (49%) continued to meet full diagnostic criteria for ADHD; 63 met criteria for ADHD–combined type, 11 met criteria for ADHD–hyperactive/impulsive type, and 37 met criteria for ADHD–inattentive type. Importantly, prior research reported that at the 24-month time point there were no significant effects of MTA treatments on levels of biased self-perceptions in this sample (Hoza et al., 2004); consequently, treatment assignment was not considered further. For purposes of the present investigation, this first time point is referred to as Time 1 and the 36-month assessment point is referred as Time 2. The number of participants in this study reflects children with relevant measures at Time 1 and Time 2. The final sample size was 226 children with ADHD (184 males, 42 females) and 123 LNCG children (94 males, 29 females) 1 ; however, due to missing outcome data, participants ranged from 282 to 349 across analyses.
Children were aged 8 to 12 at Time 1 (M = 9.7, SD = 0.88) and 9 to 13 at Time 2 (M = 10.7, SD = 0.88). The sample was 78% male. At Time 1, the mean household income ranged from US$40,000 to $50,000 and the percentage of children whose families received part or all of their income from public assistance was 16%. One percent of participants’ mothers completed eighth grade or less, 7% completed some high school, 24% completed high school/general education diploma (GED), 32% completed some college/post–high school training, 21% completed a 4-year college degree, and 15% completed an advanced graduate/professional degree. The majority of parents were married (67%). The sample was racially and ethnically diverse, with 65% Caucasian, 15% African American, 1% Asian, 11% Hispanic or Latino, 7% mixed race, and 1% Other races.
Procedure
Relevant measures were part of a larger battery of questionnaires administered to children, their parents, and their teachers at Times 1 and 2. Sociometric data were collected at Time 1 from all consented children in the classrooms of the study children. 2
Measures
Peer-rated social preference
Participant’s peer status was assessed using sociometric nominations collected at Time 1. Abiding by the standard in the field, this study obtained active parental consent before administering any sociometric measures except for in one of the six data collection sites where school officials determined that parental consent was not required. Positive nomination, negative nomination, and rating scale procedures were administered to the children with ADHD and LNCG children as part of the main MTA study, but only the positive and negative nomination procedures employed in this study are described herein. The mean, median, and modal percentage of same-sex peers participating in each classroom was 71%, 71%, and 100%, respectively.
For the group-administered positive and negative nomination procedures, children were given a list with the names of all participating children within the classroom and asked to circle the names of all the same-sex classmates who were their “best friends in the class” and the same-sex classmates whom they “do not want to be friends with.” Children were allowed to nominate as many or as few children as they felt appropriate. Individual reading assistance was provided to children in need of help (see Hoza et al., 2005, for full description of study procedures).
Positive and negative nominations were summed separately to reflect the extent to which each child was accepted (positive nominations) and rejected (negative nominations) by their peer group. As the number of classmates providing nominations varied between classrooms and affected the number of positive and negative nominations each child could receive, and consistent with usual practice in sociometric research (e.g., Coie & Dodge, 1983), scores were converted to z scores within each class. This procedure made scores for students with different class sizes comparable. A preference score was calculated by subtracting the standardized number of negative nominations from the standardized number of positive nominations and then restandardizing the score, with higher scores indicating greater social preference.
Self-perceived SA
Participants’ perception of their own SA at Time 1 was assessed using the Self-Perception Profile for Children (SPPC; Harter, 1985), a 36-item child-rated questionnaire assessing domain-specific self-perceptions as well as global self-worth. According to Harter, self-perceptions are domain specific and can be differentiated into five domains of competence: academic competence, social acceptance (SA), behavioral conduct, athletic competence, and physical appearance. In the SPPC, six items assess each domain and are rated on a 1 to 4 scale; items are averaged to yield a competence score, with higher scores reflecting higher self-perceived competence. For the purposes of this study, only the SA subscale of competence was used. The SA subscale includes items assessing the child’s perception of his or her ability to make friends, the number of friends he or she has, the frequency of time spent with friends, and popularity with others. In the present sample, the SA subscale’s coefficient alpha was .75.
Depression symptoms
Participants’ levels of depression symptoms at Time 1 and Time 2 were assessed with the Children’s Depression Inventory (CDI; Kovacs, 1992), a 27-item self-report measure of cognitive, affective, and behavioral signs of depression symptoms. Items are scored from 0 to 2 and can be summed to obtain a total score, with higher scores reflecting greater depression symptoms. The total score can be converted into a T-score based on gender and age norms. The CDI is a widely used self-report measure of childhood depression symptoms and has adequate reliability and validity data (see Kovacs, 1992, for a review). In the present study, the total depression symptom T-score was used; Cronbach’s alphas for the total T-score were .86 at Time 1 and .83 at Time 2.
Aggression and conduct problems
Participants’ aggression and conduct problems were assessed with the Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM-IV) Conduct Disorder Checklist (Hinshaw et al., 1997), a 38-item parent-rating measure of the frequency of behaviors defining conduct disorder (CD) according to DSM-IV (American Psychiatric Association, 1994) on a scale of 1 (never) to 4 (often), with additional aggression and conduct items that assess frequency of damaging items in different contexts (e.g., “broke or damaged property in house on purpose”), stealing in different contexts (e.g., “has taken anything at school”), physical aggression (e.g., “hit other children”), and other delinquent behaviors (e.g., “graffiti on walks, sidewalks, cars, etc.” or “carry weapon”). Items were summed to yield an overall aggression and conduct problem score. Reports from female primary caretakers were employed in the present study. Cronbach’s alpha for the total score at Time 1 was .89 and at Time 2 was .86.
Social skills
Participants’ social skills were assessed using teacher reports on the Social Skills Rating System (SSRS; Gresham & Elliott, 1990). There are two versions of the SSRS: a kindergarten through 6th-grade version and a 7th- through 12th-grade version. In the present study, all participants were assessed with the kindergarten through 6th-grade version at Time 1. At Time 2, a subset of participants were in 7th grade (n = 9) and were therefore assessed with the 7th- through 12th-grade version; all other participants were assessed with the kindergarten through 6th-grade version at Time 2. Items are rated on a 0 to 2 scale based on frequency, with higher scores indicating greater use of the social skill. Items assess social skills in three areas: self-control, assertion, and cooperation. Items tapping self-control measure adaptive behaviors in social interactions (e.g., controls temper in conflict situations with peers), items tapping assertion measure behaviors when initiating interactions with peers (e.g., invites others to join in activities), and items tapping cooperation measure helping, sharing, and compliance in academic situations (e.g., easily makes transition from one classroom activity to another). The majority of items are the same across the two age versions of the SSRS. However, some social skill items differ to account for developmental differences. For instance, only the 7th- to 12th-grade version includes “give compliments to members of the opposite sex.” In the present study, the total score was used based on the sum of all 30 social skill items. For children with multiple teachers, an aggregate score was calculated based on all available teachers’ reports. Substantial evidence of the validity of the SSRS is available (Demaray & Ruffalo, 1995; Flanagan, Alfonso, Primavera, Povall, & Higgins, 1996). Cronbach’s alphas for the total score were .80 at Time 1 and .83 at Time 2.
Results
Preliminary Analyses
As only a subset of children from the MTA took part in peer sociometrics, preliminary analyses compared participants with (n = 349) and without (n = 502) complete relevant data on demographic variables. Variables examined included gender, ethnicity, IQ, 3 mother and father’s highest level of education, and family income. No significant differences emerged between children with and without complete data. The mean and standard deviation of all predictor and independent variables for the ADHD and LNCG groups are presented in Table 1.
Descriptive Statistics of Predictor and Adjustment Variables for Children With ADHD and Comparison Children (LNCG).
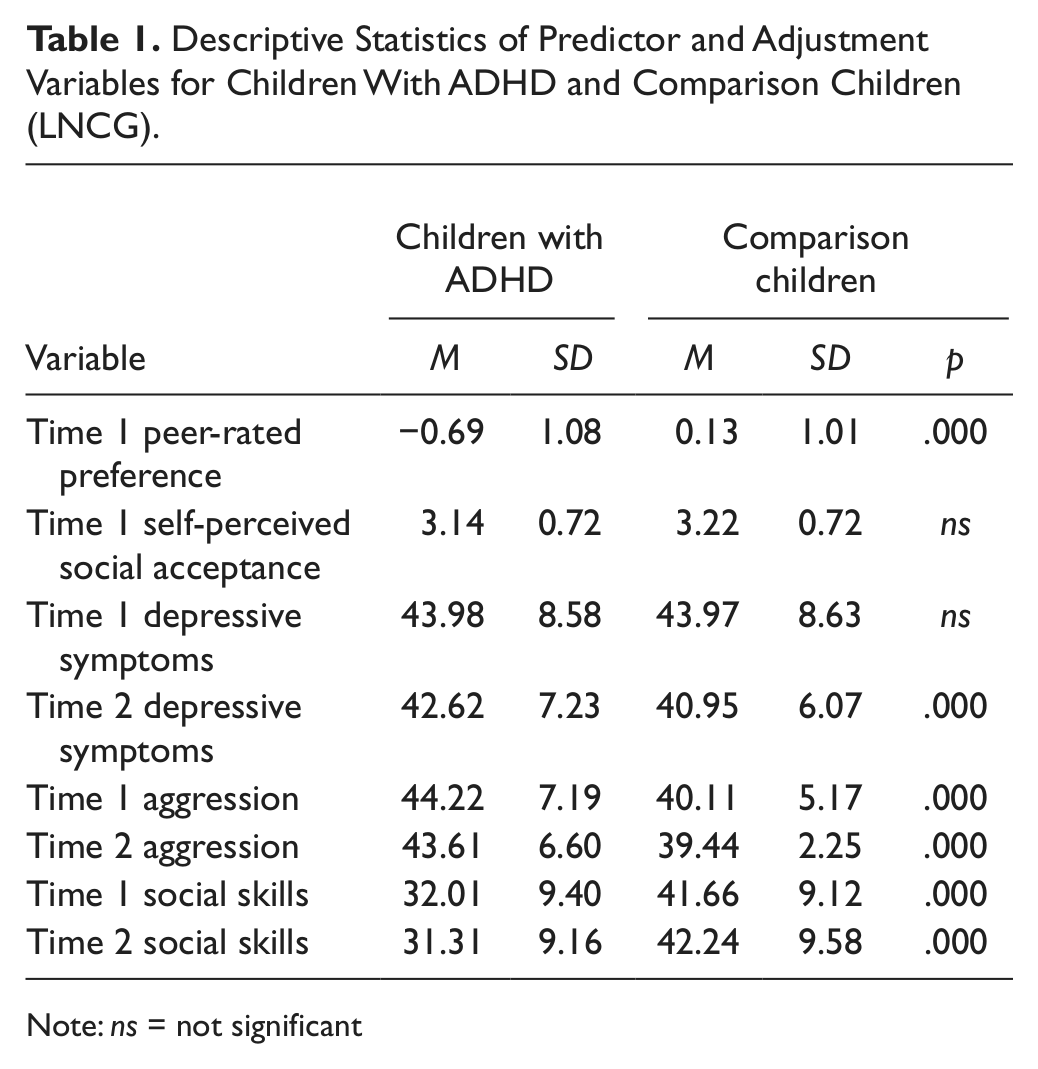
Note: ns = not significant
Primary Analyses
Data analytic strategy
A series of hierarchical regressions were conducted to examine the degree to which ADHD diagnosis, children’s self-perceptions of SA, peer-rated preference, and their interactions predicted Time 2 adjustment variables (depression symptoms, aggression/conduct, and social skills) when controlling for Time 1 level of adjustment. Given gender differences in rates of depression symptoms, aggression, and social skills (e.g., Block, 1983; Crombie, 1988; Petersen, Sarigiani, & Kennedy, 1991) and that in the present sample males were significantly lower in Time 1 and Time 2 depression and social skills and significantly higher in Time 1 and Time 2 aggression relative to females, gender was included as an additional predictor in all analyses. Using the procedures outlined by Aiken and West (1991), continuous variables were centered by subtracting the mean from each individual score and the dichotomous ADHD diagnosis variable was weight-effect coded to reduce multicollinearity. For each regression, Time 1 level of the dependent variable and gender were entered at Step 1. At Step 2, ADHD diagnosis, self-perceptions of SA, and peer-rated sociometric preference were entered. At Step 3, all two-way interactions were entered. At Step 4, the three-way interaction term was entered.
Predicting Time 2 depression symptoms
The first regression examined the effects of self-perceived SA, peer preference, and ADHD diagnosis as predictors of Time 2 depression symptoms, controlling for Time 1 depression symptoms and gender. As can be seen in Table 2, there was a significant interaction of self-perceived SA, peer preference, and ADHD diagnosis. Gender was not a significant predictor when Time 1 depression symptoms were also in the model. Post hoc analyses of this interaction were based on recommendations by Aiken and West (1991). Simple slopes were calculated at one standard deviation above and below the centered mean for peer preference. Among children with ADHD who were lower in peer preference, there was a significant inverse relationship (β= –.35, p < .001) between self-perceived SA and Time 2 depression symptoms. Specifically, for children with ADHD with lower peer preference, higher self-perceived SA predicted lower depression symptoms at Time 2 when controlling for Time 1 levels. For children with ADHD who were higher in peer preference and for all LNCG children, the relationship between self-perceptions of SA and Time 2 depression symptoms was nonsignificant (see Figure 1).
Regression Analyses Predicting Time 2 Depressive Symptoms From Self-Perceived Social Acceptance, Sociometric Preference, and ADHD Diagnostic Status (n = 319).
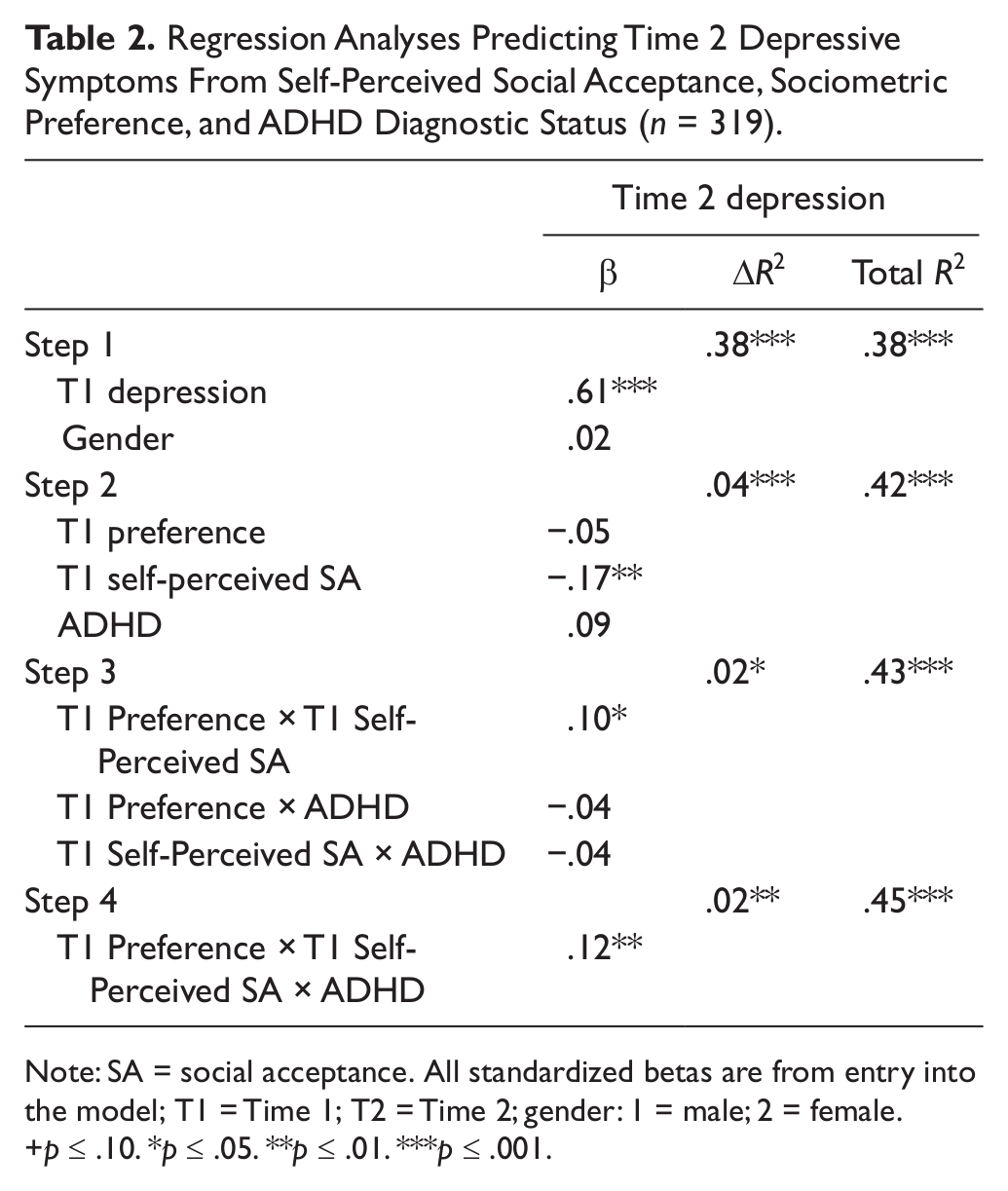
Note: SA = social acceptance. All standardized betas are from entry into the model; T1 = Time 1; T2 = Time 2; gender: 1 = male; 2 = female.
p ≤ .10. *p ≤ .05. **p ≤ .01. ***p ≤ .001.
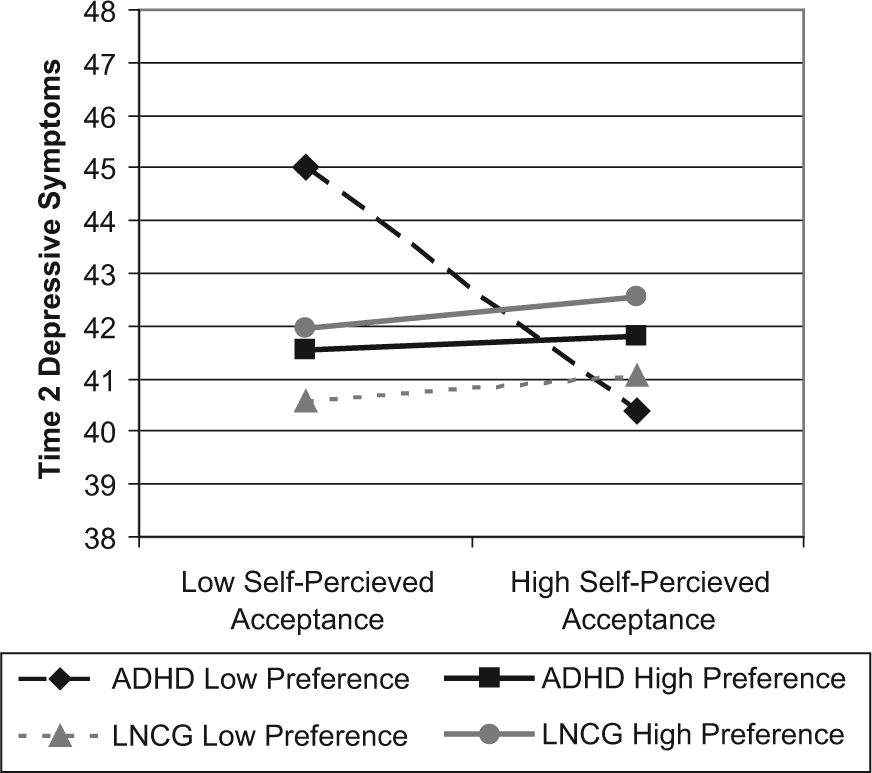
The interaction of self-perceived social acceptance, peer preference, and ADHD diagnostic status in predicting Time 2 self-reported depression symptoms.
Predicting Time 2 aggression/conduct problems
The second regression examined the effects of self-perceived SA, peer preference, and ADHD diagnosis as predictors of Time 2 maternally rated aggression/conduct problems, controlling for Time 1 aggression/conduct problems and gender. The interaction of self-perceived SA, peer preference, and ADHD diagnosis was significant at the last step of the regression equation (see Table 3). Gender was not a significant predictor when also accounting for Time 1 aggression/conduct problems. Post hoc analyses with simple slopes calculated at one standard deviation above and below the mean peer preference score indicated that for children with ADHD who were lower in peer preference, there was not a significant relationship between self-perceived SA and Time 2 aggression/conduct problems. Instead, an examination of Figure 2 suggests that children with ADHD with lower peer preference demonstrated greater aggression/conduct problems at Time 2, relative to all comparison children, regardless of self-perceived SA. However, for children with ADHD higher in peer preference, lower self-perceived SA predicted lower aggression/conduct problems at Time 2 when controlling for Time 1 levels (β = .31, p < .01). In contrast, for all comparison children, the relation between self-perceptions of SA and Time 2 aggression/conduct problems was nonsignificant (see Figure 2).
Regression Analyses Predicting Time 2 Aggression and Conduct Problems From Self-Perceived Social Acceptance, Sociometric Preference, and ADHD Diagnostic Status (n = 319).
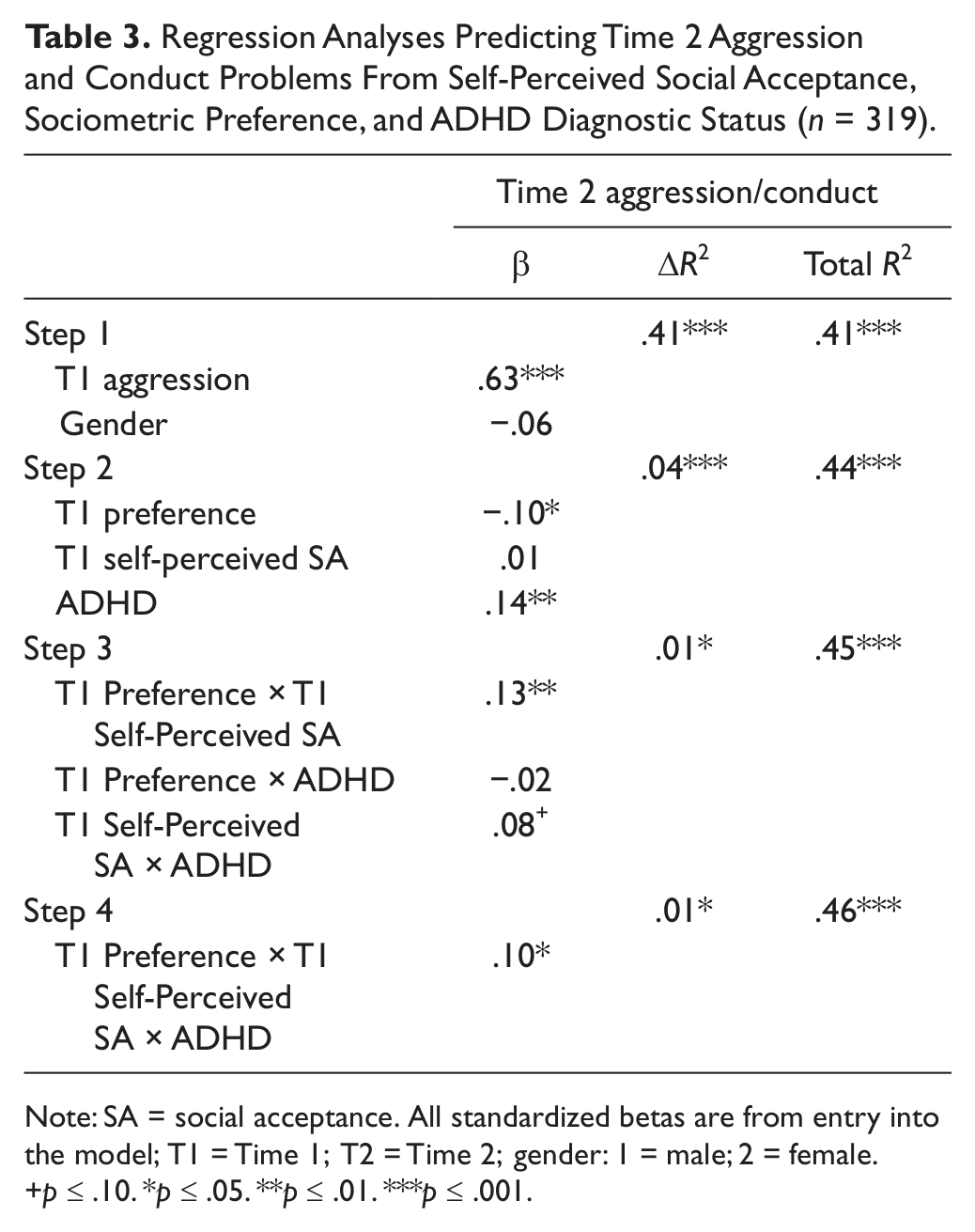
Note: SA = social acceptance. All standardized betas are from entry into the model; T1 = Time 1; T2 = Time 2; gender: 1 = male; 2 = female.
p ≤ .10. *p ≤ .05. **p ≤ .01. ***p ≤ .001.
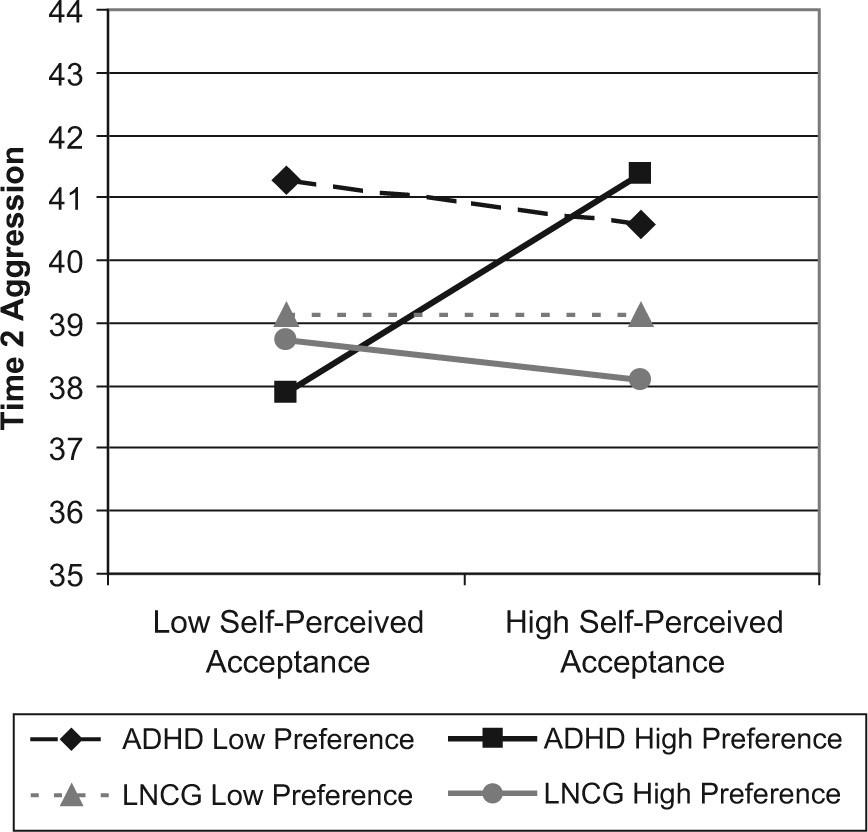
The interaction of self-perceived social acceptance, peer preference, and ADHD diagnostic status in predicting Time 2 maternally reported aggression and conduct problems.
Predicting Time 2 social skills
The third regression examined the combined effects of self-perceived SA, peer preference, and ADHD diagnosis as predictors of Time 2 teacher-rated social skills, controlling for Time 1 levels. All two-way interactions and the three-way interaction were nonsignificant (see Table 4). However, self-perceived SA, peer preference, and ADHD diagnosis were each unique predictors of Time 2 social skills. Specifically, greater self-perceived SA, higher peer status, and non-ADHD status significantly predicted greater social skills at Time 2, when controlling for Time 1 social skills level. Gender also was a predictor and indicated that female participants had greater Time 2 social skills. 4
Regression Analyses Predicting Time 2 Social Skills From Self-Perceived Social Acceptance, Sociometric Preference, and ADHD Diagnostic Status (n = 319).

Note: SA = social acceptance. All standardized betas are from entry into the model; T1 = Time 1; T2 = Time 2; gender: 1 = male; 2 = female.
p ≤ .10. **p ≤ .05. ***p ≤ .01. ****p ≤ .001.
Discussion
To our knowledge, this is the first longitudinal study to examine the interaction of self-perceived SA, peer-rated preference, and ADHD diagnosis in predicting multiple measures of adjustment. Previous research suggests that the implications of positive self-perceptions may differ based on the area of adjustment examined, children’s social-functioning level (Kistner et al., 1999; McElhaney et al., 2008), and whether a normative or clinical sample is used (Hoza et al., 2010). However, a major limitation of previous research has been a failure to consider all three of these factors together. This study fills this gap by examining the longitudinal relation between self-perceived SA and changes in different areas of adjustment using the MTA sample, which includes a local normative comparison group and a clinical group of children diagnosed with combined-type ADHD. By examining relations over time and controlling for baseline levels of adjustment, this study was able to examine how self-perceived SA and peer status relate to changes in adjustment for children with ADHD and comparison children. Consistent with hypotheses, results indicated that for some measures of adjustment, the implications of high self-perceived SA differed for children with ADHD and comparison children and also depended on their level of peer status. Thus, our findings provide a critical step in understanding the complex relations between positive self-perceptions of SA and changes in adjustment in a normative sample and a clinical sample of children with ADHD.
Researchers have argued that positive self-perceptions of competence should be protective with regard to the development of depression (Taylor & Brown, 1988). Consistent with hypotheses, our results support this notion, but only for children with ADHD who are less preferred by peers. For these children, depression scores were comparable with those of children without ADHD when self-perceived SA was high. In contrast, children with ADHD who appeared to recognize their social difficulties had the highest depression scores of the two samples. Thus, for children with ADHD, recognition of social impairment that is validated by external indicators (classmate’s ratings) predicts an increase in depression symptoms 1 year later. Results are not surprising when the severity of social impairment of some children with ADHD is considered. Research consistently finds that children with ADHD are rated as more intrusive, argumentative, and aggressive in social situations relative to comparison children (see McQuade & Hoza, 2008, for a recent review). These behaviors are likely to lead to frequent negative social feedback from peers, which may place children with ADHD at greater risk for increases in depression if they also have low self-perceived SA (Cole, 1990). Of interest, for comparison children, level of depressive symptoms did not differ based on self-perceived SA or peer preference. This difference in the protective function of positive self-perceived SA may be a result of differences in initial risk. Children with ADHD often experience a range of other impairments at home and school (Abikoff et al., 2002; Pelham, Fabiano, & Massetti, 2005) that may, in combination with awareness of negative peer status, make them more vulnerable to depression. These findings also are potentially helpful toward understanding the course of depression in children with ADHD because not all children with ADHD develop this outcome (Chronis-Tuscano et al., 2010, Molina et al., 2009). Future research will need to examine additional factors that may explain why certain children with ADHD form an awareness of poor competence and how this awareness contributes to depression. It will also be important to understand whether the connection between awareness and depression leads to long-term difficulties with depression or to greater motivation to work on one’s social deficits. If increased depression is temporary and results in better reality orientation, there may be benefits to this increased self-awareness.
Although higher self-perceived SA protected against depression symptoms in children with ADHD and lower peer status, higher self-perceived SA also was a risk factor for increased aggression and conduct problems for children with ADHD and higher peer status. In fact, socially preferred children with ADHD who perceived themselves as socially successful were as aggressive as those with ADHD who were not preferred by peers (see Figure 2). However, high–peer status children with ADHD who reported low self-perceptions of SA had comparable rates of aggression as comparison children. Thus, results suggest that for children with ADHD, being socially successful and having a more modest perception of competence is actually protective and reduced the risk for greater aggressive and delinquent behaviors 1 year later. Interestingly, this finding is in contrast to our prediction that greater self-perceived SA combined with lower peer status would be associated with greater risk for aggression for children with ADHD. Though at first results may seem surprising, studies do find that minor delinquent and aggressive behaviors can incur some social benefits as children reach adolescence (Moffitt, 1993; Parkhurst & Hopmeyer, 1998). Given the impulsivity of children with ADHD, those who are more socially successful and also more socially confident may be more likely to use aggressive or delinquent behaviors as a means to gain attention or maintain social status. In contrast, children with ADHD who are low in peer status may be at greater risk for aggression and delinquency for other reasons, such as an association with deviant peers (Marshal & Molina, 2006) or lack of effective social skills (Thaper et al., 2006). To fully understand these findings additional research that examines the strategies that more socially successful children with ADHD employ to gain or maintain social status is needed.
Unlike with depression symptoms and aggression/conduct problems, evidence of moderation was not found when examining the relationship between self-perceived SA and changes in social skills. Instead, ADHD diagnosis, lower peer status, and lower self-perceived SA were each independent predictors of poorer social skills 1 year later. Thus, contrary to predictions, when examining social skill changes, the implications of self-perceived SA did not depend on peer status or differ for children with and without ADHD. It may not be surprising that each of these factors is associated with social skills. As noted previously, a large body of research suggests children with ADHD tend to have significant social impairments (e.g., McQuade & Hoza, 2008) and may therefore be less likely to show improvements in social skills over time. Children who are less preferred by peers also may be less likely to show improvements in social skills because of less opportunity to interact with peers or because of social deficits that limit their ability to acquire new skills. With regard to self-perceived SA, researchers have suggested that more negative self-perceptions may make children less persistent and therefore less likely to master new skills (Bjorklund, 1997). Interestingly, although we found that positive self-perceived SA predicted improved social skills for all children, other research suggests that positive self-perceptions of social performance may not relate to greater persistence in social tasks for children with ADHD (Hoza et al., 2000). Thus, although evidence of moderation was not found, it may be the case that there is a different mechanism explaining the association between self-perceived acceptance and changes in social skills for children with ADHD. It will be important for future research to consider this possibility empirically. Results may also suggest that for some domains of adjustment, implications of self-perceived SA do not depend on social functioning or differ for children with ADHD. Thus, differences in findings across the three domains of adjustment examined in this study highlight the complex relations between self-perceived competence and adjustment for clinical and nonclinical samples.
Thus, results of this study suggest that positive self-perceptions of SA have risks and benefits for children with ADHD. Risk of depression is decreased for socially impaired children if they do not perceive their low peer status among peers; however, risk of aggression is increased for children with ADHD when they are liked and accurately perceive it. Given these findings, future research will need to examine whether it is clinically advantageous to modify the self-perceptions of children with ADHD. Clinical wisdom has traditionally suggested that high self-esteem is adaptive and important for all children, including those with ADHD. However, our results suggest that clinicians may have to be cautious to attend to the social self-perceptions and the social functioning of children with ADHD. Though yet to be examined empirically, it may not be clinically advantageous to target increases in self-perceived competency in children with ADHD. Instead, for children with ADHD who are low in peer status and who have an awareness of their poor social functioning, clinicians may need to incorporate strategies targeting the prevention of depression and an increase in social competence. In addition, even if children with ADHD are demonstrating more positive peer functioning, clinicians may need to monitor aggressive and delinquent behaviors in treatment, especially for children with positive self-concepts. Other evidence also suggests that the magnitude of children’s over- or underestimation of competence is important to adjustment and that a greater overestimation of competence is associated with greater aggression and social skill deficits over time (Hoza et al., 2010; Murray-Close et al., 2010). Thus, clinicians also may need to be aware of the extent to which children with ADHD are overestimating their social abilities. Despite these cautions, studies that examine the implications of modifying self-perceptions in treatment and the effects of possible intervention strategies are needed.
Though these results have promising implications for intervention and future research, study limitations must be noted. First, only children with a diagnosis of ADHD–combined type were accepted into the MTA. Although some of them had attenuated to inattentive or hyperactive/impulsive subtype by the time of the 24-month assessment, the results cannot freely generalize to children with ADHD–inattentive type and ADHD–hyperactive/impulsive type. Given research suggesting that ADHD subtypes may differ in their self-perceptions of competency (Owens & Hoza, 2003) and that there may be changes to ADHD classification in DSM-V, it will be important for future work to examine this pattern in children with a range of ADHD symptomatology presentations. Finally, child reports were used to measure self-perceptions of social competency as well as depressive symptoms, introducing the possibility of a common rater bias for this set of analyses. Thus, we cannot exclude the possibility that some of the association between our independent and dependent variables may be due to the use of the same rater. However, having the same rater may increase reliability by excluding rater variance, and the child may be the best reporters of their internal mood (Flanery, 1990).
Despite these caveats, this study adds to existing literature by examining the different longitudinal implications of self-perceptions of SA for children with ADHD and comparison children and by considering peer status as a moderator. There has remained substantial controversy in the literature about the relative adaptive and maladaptive implications of positive self-perceived SA for children with and without ADHD (Baumeister et al., 1996, 2003; Colvin & Block, 1994; Hoza et al., 2010; Owens, Goldfine, Evangelista, Hoza, & Kaiser, 2007; Taylor & Brown, 1988). Results from this study suggest that the implications depend on the population examined. For children with ADHD, lower self-perceived SA may be a double-edged sword; lower social self-perceptions protect against risk for aggression and conduct problems for children preferred by peers but increase risk for depression for those not preferred by peers. At the same time, positive self-perceived SA appears to incur the same benefits with regard to increased social skills for children with and without ADHD, regardless of peer status. It will be important for future research to examine why implications differ for children with ADHD and whether there are ways to simultaneously increase insight and reduce risk for maladjustment for these children.
Footnotes
Authors’ Note
The Multimodal Treatment Study of Children With ADHD (MTA) was a National Institute of Mental health (NIMH) cooperative agreement randomized clinical trial involving six clinical sites. Collaborators from the National Institute of Mental Health are as follows: Peter S. Jensen, MD (currently at REACH Institute and Mayo Clinic), L. Eugene Arnold, MD, MEd (currently at Ohio State University), Joanne B. Severe, MS (Clinical Trials Operations and Biostatistics Unit, Division of Services and Intervention Research), Benedetto Vitiello, MD (Child & Adolescent Treatment and Preventive Interventions Research Branch), Kimberly Hoagwood, PhD (currently at Columbia); previous contributors from NIMH to the early phase: John Richters, PhD (currently at National Institute of Nursing Research); Donald Vereen, MD (currently at National Institute on Drug Abuse). Principal investigators and coinvestigators from the clinical sites are as follows: University of California, Berkeley/San Francisco: Stephen P. Hinshaw, PhD (Berkeley), Glen R. Elliott, PhD, MD (San Francisco); Duke University: C. Keith Conners, PhD, Karen C. Wells, PhD, John March, MD, MPH, Jeffery N. Epstein, PhD (currently at Cincinnati Children’s Hospital Medical Center); University of California, Irvine/Los Angeles: James Swanson, PhD (Irvine), Dennis P. Cantwell, MD, (deceased, Los Angeles), Timothy Wigal, PhD (Irvine); Long Island Jewish Medical Center/Montreal Children’s Hospital: Howard B. Abikoff, PhD (currently at New York University School of Medicine), Lily Hechtman, MD (McGill University); New York State Psychiatric Institute/Columbia University/Mount Sinai Medical Center: Laurence L. Greenhill, MD (Columbia), Jeffrey H. Newcorn, MD (Mount Sinai School of Medicine); University of Pittsburgh: William E. Pelham, PhD (currently at State University of New York, Buffalo), Betsy Hoza, PhD (currently at University of Vermont), Brooke Molina, Ph.D. Original statistical and trial design consultant: Helena C. Kraemer, PhD (Stanford University). Follow-up phase statistical collaborators are the following: Robert D. Gibbons, PhD (University of Illinois, Chicago), Sue Marcus, PhD (Mt. Sinai College of Medicine), Kwan Hur, SEQ CHAPTER \h \r 1PhD (University of Illinois, Chicago). Collaborator from the Office of Special Education Programs/U.S. Department of Education: Thomas Hanley, EdD, Collaborator from Office of Juvenile Justice and Delinquency Prevention/Department of Justice: Karen Stern, PhD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work reported was supported by cooperative agreement grants and contracts from the National Institute of Mental Health to the following: University of California, Berkeley: U01 MH50461 and N01MH12009; Duke University: U01 MH50477 and N01MH12012; University of California, Irvine: U01 MH50440 and N01MH 12011; Research Foundation for Mental Hygiene (New York State Psychiatric Institute/Columbia University): U01 MH50467 and N01 MH12007; Long Island-Jewish Medical Center U01 MH50453; New York University: N01MH 12004; University of Pittsburgh: U01 MH50467 and N01 MH 12010; and McGill University N01MH12008. Additionally, data preparation and analysis was supported by National Institute of Mental Health grant R01 MH62583 to Betsy Hoza. The Office of Special Education Programs of the U.S. Department of Education and the Office of Juvenile Justice and Delinquency Prevention of the Justice Department also participated in funding. The views expressed in this paper are solely those of the authors, and do not necessarily reflect the views of the National Institute of Mental Health.