
Abstract
Introduction
Test Anxiety (TA)
Recent studies suggest that 33% of children and college students suffer from some degree of TA (Whitaker-Sena, Lowe, & Lee, 2007). TA is defined as a specific reaction to examination situations in which the individual is evaluated in some form. TA is manifested in multiple dimensions, among them emotional (mental stress, excitement, and fear), cognitive (forgetfulness, problems in concentration, and fear of failure), and behavioral (lifestyles and improper ways of studying), as well as in physical symptoms such as diarrhea, stomachaches, and headaches (Hembree, 1988; Klingman & Popco, 1990; Whitaker-Sena et al., 2007; Yaeri, 1998; Yousefi, Abu-Talib, Bte-Mansor, Bte-Juhari, & Redzuan, 2010; Zeidner, 1998). According to another typology, TA symptoms comprise three major facets: (a) cognitive obstruction or hindrance of cognitive performance, expressed in terms of being unable to think optimally before and during a test; (b) social derogation, or the fear of negative judgment from others following test failure; and (c) tenseness, expressed through physical and emotional arousal (Friedman & Bendas-Jacob, 1997a, b).
TA Correlates
TA is influenced by many factors. Environmental factors include the nature of the teacher–student relationship, as well as competitive institutional or family demands (Bembenutty, 2009; Goetz, Preckel, Zeidner, & Schleyer, 2008; Hancock, 2001). Individual components include a tendency toward perfectionism, fear of punishment, a tendency toward anxiety, and problems with self-regulation (Scheier, Carver, & Bridges, 1994; Speirs & Finch, 2006; Sud, 2001). TA is exacerbated by deficient testing strategies and weak study skills (Morris & Engle, 1981; Whitaker-Sena et al., 2007). Another correlate of TA is learning disability, which is defined by a collection of significant and chronic difficulties in the study of different subjects (Sharony-Yitzhack, 1998). Students with learning disabilities report higher TA compared with students without learning disabilities (Whitaker-Sena et al., 2007).
TA and Self-Esteem
The concept of self-esteem refers to a person’s evaluation of, or attitude toward, himself or herself (Rosenberg, 1965). People are generally motivated to maintain high levels of self-esteem and to defend their self-esteem when it is threatened (Pyszczynski, Greenberg, Solomon, Arndt, & Schimel, 2004). A meta-analytic study based on around 9,000 participants reported a substantial inverse correlation between self-esteem and TA (Hembree, 1988), a conclusion supported by many recent studies (e.g., Hojat, Callahan, & Gonnella, 2004; O. Peleg, 2009; Thomas & Gadbois, 2007; Wachelka & Katz, 1999). Some studies even supported the view that causality flows from self-esteem to TA (Hodapp, 1989; Krampen, 1988). Yet, although the primacy of self-esteem as a causative factor in TA is clear, the relationships between self-esteem and TA are most likely bidirectional (Zeidner, 1998). Self-esteem and TA are therefore expected to be mutually intertwined and to have a reciprocal impact on each other as they develop.
ADHD
ADHD is a neuropsychiatric disorder. It is one of the most pervasive neuropsychiatric disorders among children (Woo & Keatinge, 2008), but it also affects adults (Bell, 2011). Current prevalence rates for ADHD among children and adolescents in the United States range from 3% to 10-11% (Barkley & Biederman, 1997; Mangeot et al., 2001), whereas rates for the U.S. adult population are 4% to 5% (Bell, 2011; Fischer et al., 2007; Kessler et al., 2006; Tamam, Karakus, & Ozpoyraz, 2008). Although the main symptoms of ADHD depend on the specific type of ADHD, they always include an ongoing history of inability to sustain attention, as well as hyperactive behavior and impulsivity. Consequently, ADHD can cause substantial functional impairments in daily activities, thereby disrupting quality of life.
ADHD also affects academic achievements, with fewer educational milestones achieved beyond high school (Klassen, Katzman, & Chokka, 2010), reduced likelihood of finding full-time employment, and significantly lower average household incomes compared with individuals without ADHD (Faraone, Biederman, & Mick, 2006).
ADHD, Self-Esteem, and Anxiety
ADHD affects many aspects of life (e.g., poor peer relationships, aggression, and learning problems), which in turn are associated with academic failure and increased risk for development of low self-esteem (Biederman, 2005). Indeed, many studies have reported negative relationships between ADHD and self-esteem (e.g., Edbom, Lichtenstein, Granlund, & Larsson, 2008). Anxiety disorders are a common comorbid condition among individuals with ADHD (Schatz & Rostain, 2006), with prevalence commonly ranging from 15% to 35% but can even reach 50% (Kessler et al., 2006; Mancini, Van Ameringen, Oakman, & Figueiredo, 1999). Children with ADHD display higher rates of various anxiety disorders, including agoraphobia, simple phobias, separation anxiety disorders, social phobias, and obsessive-compulsive disorder (Spencer, Biederman, & Wilens, 1999). Adult ADHD is often associated with generalized anxiety disorder (Klassen et al., 2010).
ADHD and Poor Test Performance
Several features of ADHD contribute to poor performance in test situations: (a) Lower basic academic skills—Inherent difficulties with impulse control, attention capacity, and hyperactivity disrupt the acquisition of basic academic skills (Lahey et al., 1998; Spira & Fischel, 2005). (b) Poor language and reading skills—ADHD groups were found to have poor language and reading skills compared with controls (Loe & Feldman, 2007; McGee et al., 1991; Rodriguez et al., 2007), thereby affecting potential performance. (c) History of lower academic achievements and failures—Many studies have shown that ADHD is associated with poor grades and academic achievements (Barry, Lyman, & Klinger, 2002; Frazier, Youngstrom, Glutting, & Watkins, 2007; Loe & Feldman, 2007). (d) Cognitive problems—Working memory and executive functions have been found to be impaired among individuals with ADHD in a way that can affect test performance (Barkley, 1997; Tannock, 1998). (e) Test preparedness—Study skills such as note taking, summarizing and outlining, practice using sample tests, time management, concentration, and motivation are weaker in ADHD populations (Javorsky & Gussin, 1994; Reaser, Prevatt, Petscher, & Proctor, 2007). (f) Management of the test situation—Components of testing such as crowded rooms can disrupt sustained attention, and this is exacerbated by long examination times and restrictions on movement (for those with a hyperactive component; Daley & Birchwood, 2010). (g) State anxiety—State anxiety contributes to predicting both learning and delayed recall in adults with ADHD. Findings suggest that decreased verbal learning and memory in adults with ADHD is due in part to situational anxiety (Roth et al., 2004).
Hypotheses
As noted, there are known correlations between learning disabilities and TA (e.g., O. Peleg, 2009; Whitaker-Sena et al., 2007), and between ADHD and other types of anxiety (e.g., Schatz & Rostain, 2006). Moreover, individuals with ADHD are more likely to perform poorly on tests, thereby affecting their self-esteem, which shows a strong correlation to TA. Yet, to the best of our knowledge, no studies to date have directly examined the relationships between ADHD and TA. Taking into consideration the inverse correlations between self-esteem and TA, and between ADHD and anxiety, we hypothesize the following:
Hypothesis 1: Individuals with ADHD will report higher levels of TA and lower levels of self-esteem compared with individuals without ADHD.
Hypothesis 2: The relationships between ADHD and TA will be mediated by self-esteem. The mediation hypothesis includes three parts (according to Baron & Kenny, 1986): (a) ADHD will be negatively correlated with self-esteem. (b) Self-esteem will be negatively correlated with TA. (c) When self-esteem is included in the statistical model, the strength of the relationships between ADHD and TA will decrease.
Method
Participants
A total of 55 female participants (M age 23.47 ± 2.04) were selected from a pool of 287 undergraduate students based on their scores on a self-report ADHD Rating Scale (DuPaul, Power, Anastopoulos, & Reid, 1998) and on an Online Continuous Performance Test (OCPT; Raz, Bar-Haim, Sadeh, & Dan, 2012). They were divided into two groups: participants diagnosed with ADHD (n = 25; M age 23.84 ± 1.84) and female controls without ADHD (n = 30; M age 23.17 ± 2.18). Inclusion criteria for the ADHD group were (a) previous professional diagnosis (made by either neurologist or psychiatrist) of adult ADHD from an established clinic in the field of psychoeducational assessment, (b) at least six symptoms either of inattention or of hyperactivity-impulsivity on the ADHD Rating Scale–IV (DuPaul et al., 1998), 1 and (c) low scores on the OCPT task, defined as at least two standard deviations above the mean number of either omission or commission errors. 2 Inclusion criteria for the control group were (a) no previous diagnosis of ADHD, (b) fewer than four symptoms either of inattention or of hyperactivity-impulsivity on the ADHD Rating Scale–IV, and (c) scores on the OCPT task within the normal range, defined as fewer than two standard deviations above the mean number of omission and commission errors. The ADHD and control groups did not differ with respect to mean age, education, or ethnicity distribution. Participants were given course credit according to their academic requirements. Written informed consent was obtained from all participants. The study was approved by the institutional review board.
Instruments
TA questionnaire
The Friedben Test Anxiety Scale (FTAS; Friedman & Bendas-Jacob, 1997a, b) is a 23-item scale consisting of the following three subscales: (a) Cognitive Obstruction—poor concentration, failure to recall, difficulties in effective problem solving before or during a test (e.g., “On a test I feel like my head is empty, as if I have forgotten all I have learned”); (b) Tenseness—physical and emotional discomfort (e.g., “I am very tense before a test, even if I am well prepared”); and (c) Social Derogation—concerns about being socially belittled and deprecated by significant others following failure on a test (e.g., “If I fail a test I’m afraid I’ll be considered stupid by my friends”). Respondents were asked to answer how frequently, along a 6-point scale (1 = almost never, 6 = almost always), they felt the described situations. Scores were calculated by reversing raw scores on four items and averaging the mean scores of all items in each subscale. Their range, therefore, was 1 to 6, with lower scores reflecting a lower level of TA. In the present study, Cronbach’s alpha coefficients were .92 for Cognitive Obstruction, .87 for Tenseness, and .93 for Social Derogation.
ADHD questionnaire
The assessment questionnaire for ADHD (a version of the ADHD Rating Scale–IV; DuPaul et al., 1998) included 18 items based on the symptoms listed in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) for ADHD diagnosis. These symptoms include measurements of attentiveness, hyperactivity, and impulsivity. In an attempt to address possible response bias, inattention symptoms were designated as odd-numbered items and hyperactivity-impulsivity symptoms were displayed as even-numbered items. Participants were asked to choose whether each described situation was correct or incorrect with respect to them. In the present study, for the Attention Deficit Disorder (ADD) scale, alphas were .80, and for the Hyperactivity and Impulsivity scale, alphas were .74.
The self-esteem inventory
The Rosenberg 10-item Self-Esteem Scale (Rosenberg, 1965) was used to measure general self-esteem. These items were rated on a 6-point scale (1 = strongly disagree, 6 = strongly agree). An example item is “I feel I am a worthwhile person, at least on an equal plane with others.” Scores were calculated by averaging the mean scores of all items. Therefore, the scores ranged from 1 to 6, with lower scores reflecting a lower level of self-esteem. This instrument is well known for its high reliability and validity for measuring general self-esteem. Its internal reliability in previous research ranged from .93 to .86. In the present study, alphas were .94.
OCPT
Continuous Performance Tests/Tasks (CPTs) require participants to maintain vigilance and react to the presence (or absence) of a specific stimulus within a set of continuously presented distracters. CPTs have a long history of use in measuring processes related to vigilance, sustained attention, response inhibition, and other aspects of attention and cognitive function (Conners, Epstein, Angold, & Klaric, 2003; Riccio, Reynolds, & Lowe, 2001). CPTs (e.g., the Conners’ CPT–II and the Test of Variables of Attention [TOVA]) have been extensively used in the context of ADHD diagnosis (Barkley, 1998; Epstein et al., 2003; Losier, McGrath, & Klein, 1996; Nichols & Waschbusch, 2004; Riccio & Reynolds, 2001).
The OCPT (eAgnosis, Inc., Delaware; Raz et al., 2012; Sadeh, Dan, & Bar-Haim, 2011) is a standard CPT designed and programmed for delivery over the Internet. The task uses two geometric stimuli: equilateral triangles (~5 cm sides) and circles (~5 cm diameter), both displayed in a light blue color delineated by a black one-pixel stroke contour. The geometric stimuli are shown in the middle of the screen against a gray background, within a 4-pixel-stroke 7.5 × 11 cm black rectangle presented continuously throughout the task.
In each trial, one geometric shape is displayed for 100 ms, followed by a 1,900 ms intertrial interval. Participants are instructed to respond to the triangle shape as fast as possible without compromising accuracy by pressing the spacebar on the computer keyboard and to withhold their response to the circle shape. The test has two conditions: low target frequency and high target frequency (see Greenberg, Kindschi, Dupuy, & Corman, 1996; Greenberg & Waldman, 1993, for a similar task presentation). The first half of the test (low target frequency) includes 224 trials (56 targets, 168 nontargets), with a target to nontarget ratio of 1:3. This half of the test is boring and fatiguing. In the second half of the test (high target frequency), the target to nontarget ratio is reversed and set to 3:1 (168 targets, 56 nontargets). In this half of the test, participants expect to respond most of the time but occasionally must inhibit their tendency to respond. Manipulation of target frequency in CPTs is designed to highlight the sustained attention component in the low target frequency condition and the response inhibition component in the high target frequency condition. Throughout the task, the geometric shapes are presented in a fixed, pseudorandom sequence. To minimize practice effects, each half of the test is preceded by a 2-min practice phase reflecting the target to nontarget ratios of the actual test to follow. Participants are not informed of the practice nature of these 2-min practice sessions and consider them part of the test. The total net test time of the OCPT (including the two practice sessions) is 19 min. Three breaks are allowed (following the first and second practice sessions and following the low target frequency session). Participants are instructed not to exceed 2 min of break time. Responses with reaction times (RT) faster than 150 ms were considered anticipatory and eliminated from the analyses. When a participant presses the spacebar more than once per stimulus presentation, only the data from the first response were included in data analysis.
The software automatically records the participant’s omission and commission errors as well as RT. Four primary measures are extracted for analyses: errors of omission (defined as the number of targets to which a participant did not respond), errors of commission (defined as the number of times a participant incorrectly responded to a nontarget), response times, and response time consistency (standard deviations of response times). These measures are extracted per condition (low and high target frequencies), and can also be extracted by test blocks (quartiles) per condition. The software issues an alert for any unusual pattern of results it detects (i.e., considerable amount of missing data during significant portions of the test). All data are stored offline and are available as a Microsoft Excel spreadsheet.
Procedure
Participants were invited to the laboratory and completed the TA, self-esteem, and ADHD questionnaires in a quiet room. Answering all the questions took approximately 30 min. On completion of the questionnaires, participants were instructed how to access the OCPT from home and how to complete the test. Participants were also requested to take the test in a quiet room and to avoid potential distracters and interruptions. In addition, they were instructed to abstain from using methylphenidate on the day of testing.
Results
Comparing Levels of TA and Self-Esteem Among Participants With and Without ADHD
Four t tests were generated to assess differences between ADHD participants and controls in levels of reported TA and self-esteem. Analyses revealed significant differences between the two groups for all three types of TA (Figure 1). Participants with ADHD reported higher levels of cognitive obstruction TA (M = 3.98, SD = 1.07) compared with controls (M = 2.54, SD = 0.70), t(53) = 5.98, p = .0001; Cohen’s d = 0.63. Similarly, they reported higher levels of tenseness TA (M = 4.71, SD = 0.98) compared with controls (M = 3.43, SD = 0.81), t(53) = 5.27, p = .0001; Cohen’s d = 0.58, as well as higher levels of social derogation TA (M = 3.35, SD = 1.17) compared with controls (M = 2.09, SD = 0.87), t(53) = 4.55, p = .0001; Cohen’s d = 0.52. Finally, participants with ADHD reported lower levels of self-esteem (M = 4.10, SD = 0.95) compared with their control counterparts (M = 5.10, SD = 0.76), t(53) = −4.33, p = .0001; Cohen’s d = 0.50.
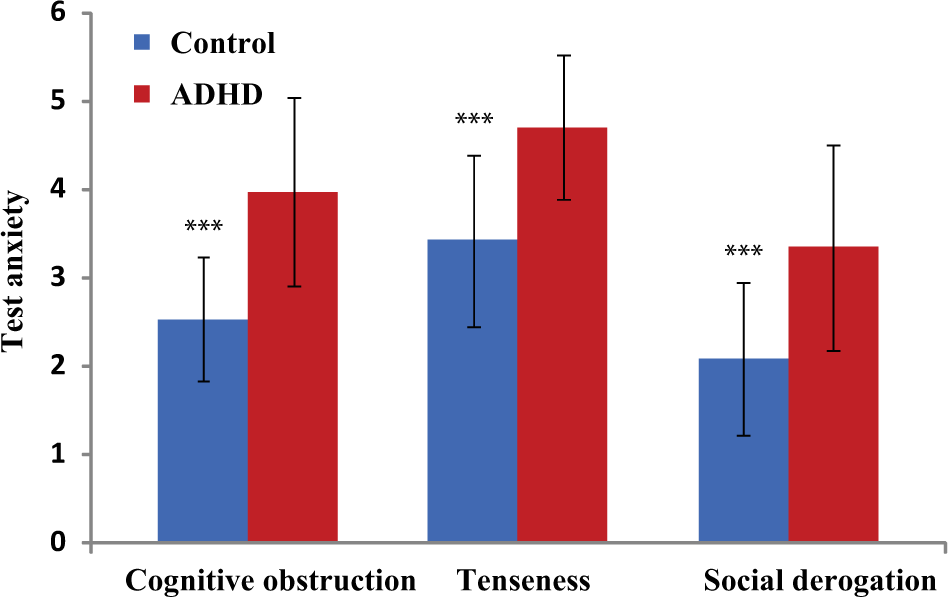
Differences between ADHD and control groups in levels of cognitive obstruction, social derogation, and tenseness test anxiety
Self-Esteem As a Mediator Between ADHD and TA
The second hypothesis of the study pertained to the role of self-esteem as a possible mediator between ADHD and TA. Pearson correlations computed between these variables showed moderate to strong correlations (Figure 2a, b, c).
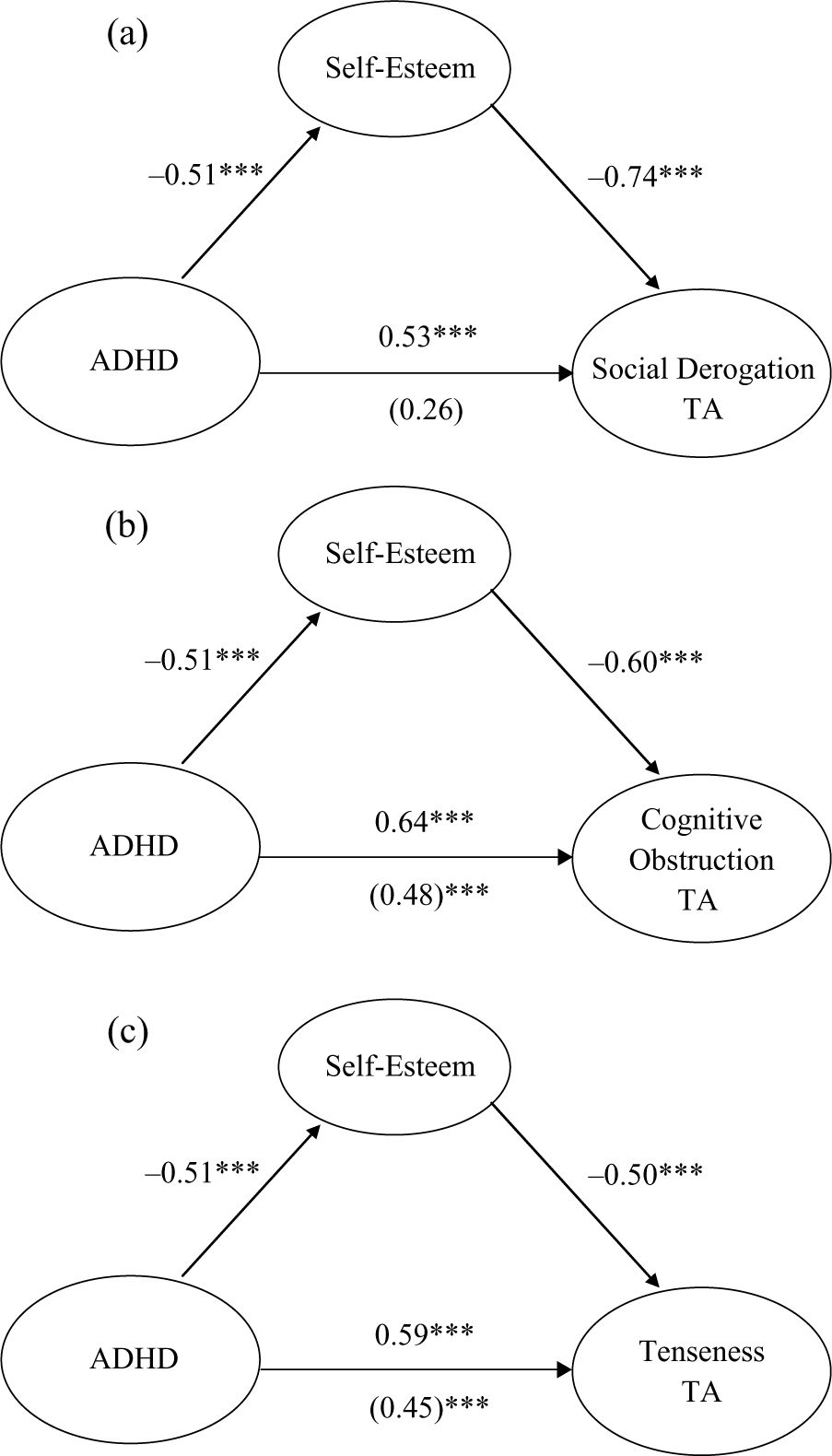
(a) Self-esteem as a full mediator between ADHD and social derogation TA (Sobel = −3.46, p = .0005); (b) self-esteem as a partial mediator between ADHD and cognitive obstruction TA (Sobel = −2.62, p = .008), and (c) no mediation effect in the relationships between ADHD and tenseness TA (Sobel = −1.91, p = .06)
Three Sobel tests were computed with TA scales as predicted variables, ADHD as the predictor variable, and self-esteem as the mediator variable. Results of the mediation analysis revealed that self-esteem significantly mediated the association between ADHD and social derogation (Sobel statistic = −3.46, p = .0005; Figure 2a), and partially mediated the association between ADHD and cognitive obstruction (Sobel statistic = −2.62, p = .008; Figure 2b). However, no mediation effect of self-esteem was found for the association between ADHD and tenseness, which was solely predicted by ADHD (Sobel statistic = −1.91, p = .06; Figure 2c).
Discussion
The purpose of the present study was to examine the relationships between ADHD and TA, and to test the mediation effect of self-esteem in the relationships between ADHD and each subtype of TA.
Our first hypothesis was that individuals with ADHD will report higher levels of TA and lower levels of self-esteem compared with individuals without ADHD. This hypothesis was clearly confirmed. The results indicate that participants with ADHD perceive the test situation as much more threatening compared with those without ADHD because they reported significantly higher levels of anxiety for all three TA subtypes compared with controls.
These differences in TA levels between ADHD and controls were also reflected in satisfactory effect size values. According to the widely used conventions or operational definitions suggested by Cohen (1988), effect sizes (Cohen’s d) of 0.2, 0.5, and 0.8 are considered “small,” “medium,” and “large,” respectively. In the present study, effect sizes ranged from 0.52 to 0.63, therefore representing medium between-groups differences. Cohen stated that a medium effect size represents an effect likely to be visible to the naked eye of a careful observer. These results are consistent with studies that focused on learning disabilities, which found that students with learning disabilities have higher levels of TA than do students without learning disabilities (Hembree, 1988; Lufi, Okasha, & Cohen, 2004; O. Peleg, 2009; Whitaker-Sena et al., 2007). These findings suggest the emergence of a vicious cycle in which problems with attention, concentration, hyperactivity, and impulsivity culminate in problems with test performance. The level of TA rises, test performance is compromised due to elevated TA, and the student attributes the failure to ADHD. Hence, fear of tests increases even more, thus further interfering with test performance. The results of the present study also indicate that participants with ADHD report significantly lower levels of self-esteem compared with participants without ADHD.
The second hypothesis was that self-esteem would serve as a mediator variable in the relationships between ADHD and TA. The mediation model exhibited medium to strong positive correlations between ADHD and cognitive obstruction, tenseness, and social derogation TA, as well as a medium negative correlation between self-esteem and TA. These results replicate previous findings showing that ADHD and self-esteem are negatively related (e.g., Edbom, et al., 2008).
The results of the present study indicate that self-esteem fully mediates the relationships between ADHD and social derogation TA. The tendency to actually perform poorly on a sustained attention task (reflected in higher rates of omission errors) or a response inhibition task (reflected in higher rates of commission errors) as well as the self-perception of having such a tendency to perform poorly on those tasks (ADHD self-report questionnaire) have been found to be related to social derogation TA through the mediation of self-esteem. Whether an individual fears negative judgment or worries about being socially belittled and deprecated by significant others following failure on a test depends on his self-esteem. Thoughts like “I certainly feel useless at times” (low self-esteem) may increase feelings of stress before and during a test, thereby contributing to failure and increasing the tendency toward social derogation TA.
The results also showed that the relationships between ADHD and cognitive obstruction TA were only partially mediated by self-esteem because TA was also predicted directly by ADHD. However, the results revealed direct relationships between having ADHD and being unable to think optimally before and during a test, with level of self-esteem influencing the magnitude of these relationships. A tendency toward high self-esteem involves feelings and thoughts such as “I feel I am a worthwhile person” or “I am able to do things as well as most other people.” Thoughts like these seem to help reduce cognitive obstruction TA or hindrance of cognitive performance. Finally, the results revealed that the relationships between ADHD and tenseness TA were not mediated by self-esteem. Self-esteem did not contribute significantly to TA expressed through physical and emotional arousal.
In summary, the present study has demonstrated the importance of self-esteem as a mediator between ADHD and TA, particularly in highlighting the dominant role of self-esteem in social derogation TA.
The present study has some limitations. First, it depended on participants’ self-reports of their TA levels. Some participants may have been unable to give accurate reports of their feelings in the described situations or may have been embarrassed about sharing their true feelings. Future studies should incorporate physical assessment of TA, preferably during the test itself. Second, this study comprised an all-female sample. As the relationships between ADHD, TA, and self-esteem may be somewhat different for males, it would be useful to replicate the present study with male participants and to analyze possible gender-related differences in the pattern of results. In addition, the ADHD sample included participants with both inattentive (ADD) and combined (ADD + hyperactivity-impulsivity) subtypes (according to the self-report rating scale) because there were no differences in their TA or self-esteem levels. Nonetheless, future studies should further explore possible differences in TA levels between ADHD subtypes and the role of self-esteem as a mediator between ADHD and TA, using larger samples and more strict criteria in distinguishing between those ADHD subtypes. Finally, this study did not include a rigorous assessment of possible ADHD comorbidities and other psychiatric disorders. Given the relatively high rates of comorbidity in ADHD, it is possible that the current results may be, at least partially, attributed to comorbidities rather to ADHD per se. This should be taken into account in interpreting the current results as well as in future studies.
Previous studies showed that TA is influenced by many factors, including academic achievements, cognitive disturbances, communication with parents, self-esteem, comparison with peer groups, parents’ opinions, child’s position in the family, and test difficulty (Ergene, 2003; Hembree, 1988; A. Peleg, 2003; O. Peleg, 2009; Swanson & Howell, 1996). The findings of the present study shed more light on the contribution of ADHD to the prevalence of TA. Another contribution of this study is that it validates the importance of dividing TA into several subscales or subtypes. The results showed that self-esteem differentially mediates the different TA subtypes.
The results presented here can be applied in interventions for students with ADHD by encouraging them to participate in courses or treatments to reduce TA, preferably those that address the specific needs arising from the disorder. Furthermore, test environments appropriate to ADHD students should be offered, such as shorter examination times or scheduled breaks, thereby allowing them to fulfill their intellectual potential.
Previous studies have found correlations between self-esteem and TA, and between learning disabilities and TA. To the best of our knowledge, the preliminary study presented here shows, for the first time, strong correlations between TA and ADHD. Our findings suggest that participants with ADHD have higher degrees of TA than their non-ADHD peers. ADHD factors can be used to explain TA, and especially tenseness TA, beyond the contribution of self-esteem alone. More studies are needed to establish the exact relationships between the different ADHD factors and the manifestations of TA. Our results clearly demonstrate that effective treatment of ADHD must take TA into account. The present study highlights a potentially important problem that can be an impairment for adults with ADHD in a learning environment and provides preliminary evidence that ADHD symptoms may predict additional problems with TA.
Footnotes
Acknowledgements
The authors wish to thank Shiran Lunski, and Yulia Gonzales for their valuable contribution to this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.