
Abstract
Many advances in our clinical and neuropsychological understanding of autism spectrum disorders (ASD) have taken place in the last decade. Notably, there is an increasing recognition of the clinical overlap between ASD and ADHD. This will be reflected in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-V; American Psychiatric Association [APA], 2010) proposal to remove the diagnostic rule precluding a comorbid diagnosis of ASD and ADHD. ADHD shows a number of similarities with high-functioning autism and Asperger’s disorder: All are complex genetic, neurodevelopmental conditions with male predominance, which involve similar brain regions such as the frontostriatal area. Notably, the last few decades of research have predominately focused on males with these conditions, with comparatively less focus on females. Often this is justified by findings that suggest, on average, four males for every one female are diagnosed with an ASD (Fombonne, 2003) and at least three males for every one female are diagnosed with ADHD (APA, 2000; Graetz, Sawyer, Hazell, Arney, & Baghurst, 2001). In ASD, the gender ratio differs with cognitive ability, with a 2:1 ratio in individuals with intellectual disability compared with around 6:1 in high-functioning populations (Fombonne, 2003). In ADHD, the gender ratio is higher in clinical populations, likely due to males exhibiting more externalizing behavior problems and subsequently gaining clinical attention (Levy, Hay, Bennett, & McStephen, 2005). In contrast, females typically exhibit more covert internalizing behaviors, like anxiety, resulting in fewer girls compared with boys referred to clinics (Levy et al., 2005; Staller & Faraone, 2006). These gender differences in behavior may affect the ascertainment of girls with ASD and ADHD, and contribute to the male predominance found in these conditions. Importantly, gender differences found in the prevalence, symptomatology, and time course of a disorder may provide clues to underlying etiology (Rutter, Caspi, & Moffitt, 2003). Examining gender differences in ASD and ADHD may therefore provide insight into causal mechanisms, as well as aide in the identification and treatment of girls with these conditions if symptomatology and time course do differ by gender. As ADHD is around 5 times more prevalent than ASD, there have been far greater opportunities to study girls with ADHD than girls with ASD (APA, 2000; Graetz et al., 2001). To date, gender differences in the behavioral symptoms of ASD have received the most research attention, yet some inconsistent findings have emerged.
In general, past research suggests males with ASD have higher levels of repetitive and stereotyped behaviors than females; however, social-communicative symptom disturbance is reported as similar across genders. However, the research findings in this area are mixed with some studies reporting more social difficulties in girls, particularly post puberty (Holtmann, Bolte, & Poustka, 2007; McLennan, Lord, & Schopler, 1993), and fewer social difficulties in adult females (Lai et al., 2011; Rivet & Matson, 2011). Findings that males tend to exhibit more repetitive behaviors (Hartley & Sikora, 2009; Hattier, Matson, Tureck & Horovitz, 2011; Mandy et al., 2011; Sipes, Matson, Worley, & Kozlowski, 2011; Wing, 1981) may reflect a gender difference found in the general population (Leekam et al., 2007). Yet, other studies have found no gender differences in social, communication, or repetitive behaviors in children with ASD (Kozlowski & Matson, 2012; Lai et al., 2011; Pilowsky, Yirmiya, Shulman, & Dover, 1998; Rivet & Matson, 2011; Solomon, Miller, Taylor, Hinshaw, & Carter, 2012). Overall, no consistent gender differences in ASD symptom severity exist in the research literature, which could relate to small sample sizes, heterogeneous study methodology, and possible changes in symptoms across development, or there may simply be no robust gender differences.
The behavioral symptoms of ADHD also appear to vary across gender in individuals with ADHD; however, findings in this area are also mixed. In clinically referred samples of individuals with ADHD, males exhibit higher levels of hyperactivity, impulsivity, and inattention than girls (Gershon, 2002). However, ADHD gender ratios, when taken from nonreferred, population-based samples, are narrowed compared with clinical samples, and the level of ADHD symptom severity is also similar across genders (DuPaul et al., 2006; Staller & Faraone, 2006). It is plausible that the way in which ADHD symptoms overlap in ASD in regard to gender may be similar to that found in ADHD. Overall, the rates of ADHD symptoms in individuals with ASD have been estimated at up to 70% (Gadow, Devincent, Pomeroy, & Azizian, 2005; Yoshida & Uchiyama, 2004; see also Cornish & Wilding, 2010, for a review). In regard to gender differences in ADHD symptoms in ASD, past research has shown the prevalence of ADHD to be similar in males and females with ASD in childhood and adulthood (Brereton, Tonge, & Einfeld, 2006; Gadow et al., 2005; Hofvander et al., 2009; Simonoff et al., 2008). However, most of these studies have examined very few females compared with males, including wide age bands, and not reported whether samples were IQ matched. Recently, Mandy et al. (2011) found more teacher-reported, but not parent-reported, ADHD symptoms in boys than in girls with ASD.
In regard to the time course of ADHD symptomatology, a profile of decline in ADHD symptoms with age has been found for males and females with ADHD, but with some evidence that ADHD may be more persistent in girls than boys (Hinshaw, Carte, Fan, Jassy, & Owens, 2007; Mick et al., 2011; Monuteaux, Mick, Faraone, & Biederman, 2010). In contrast to this, Mandy et al. (2011) recently found no age profile of ADHD symptoms in ASD; however, they used a unitary hyperactivity/inattention construct in a sample aged from 3 to 18 years. As hyperactivity tends to decrease with age, but inattention may remain persistent, using a unitary construct for these separate domains may obscure age effects in symptom change. Hence, it is not clear whether the time course of ADHD symptoms in boys and girls with ASD shows a similar gender profile to that of ADHD.
Finally, when examining gender, it is important to examine a typically developing (TYP) group to determine whether any gender differences are specific to a disorder or reflect general population gender differences. Numerous studies of gender in ASD have failed to include a TYP group of boys and girls (Koenig & Tsatsanis, 2005). If there are gender differences found in ASD that reflect typical gender differences, these will require different interpretation than gender differences unique to ASD, and will have different implications in regard to causal mechanisms.
The aim of the current study was to first examine gender differences in autistic and ADHD symptoms in a well-defined IQ- and age-matched group of boys and girls with ASD. The second aim was to determine whether ADHD symptoms in this group would show a decline with age. Third, our aim was to examine these relationships in the context of typical gender development by including a normally developing comparison group. Our hypotheses were threefold: (a) that boys with ASD would exhibit more repetitive and stereotyped behaviors than girls with ASD, but similar levels of social and communication deficits, and these relationships would be reflected in TYP children; (b) that boys with ASD would show more hyperactive-impulsive and inattentive symptoms than girls with ASD, a pattern that would also be present in the TYP children; and (c) that there would be lower levels of hyperactive and inattentive symptoms in older children with ASD than in younger children with ASD, regardless of gender, and this age pattern would also be reflected in the typical group.
Method
Participants
The participants were 124 children aged 7 to 12 years, 64 with autistic disorder or Asperger’s disorder, including 32 males (16 autistic disorder, 16 Asperger’s disorder) and 32 females (7 autistic disorder, 25 Asperger’s disorder), and 60 TYP children, 30 female and 30 male. Of the participants, 93.5% were Caucasian, 5.6% Asian, and 0.9% other. The clinical groups were recruited from the Monash University Centre for Developmental Psychiatry and Psychology register of volunteers, the Autism Victoria “Get Involved” register of volunteers, and from private clinics in the Melbourne metropolitan area. Only children who had a current diagnosis of ASD from their pediatrician or psychologist were invited into the study. The Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev., DSM-IV-TR; APA, 2000) criteria for autistic disorder or Asperger’s disorder were confirmed for all clinical participants using our standard process of confirmation involving reviewing diagnostic reports from registered psychologists and pediatricians with a symptom checklist to ensure the DSM-IV-TR criteria were fulfilled. Only children with Full Scale IQs (FSIQ) of 70 and above were included. The TYP group was recruited from a local primary school and had no history of parent-reported developmental delay or psychopathology. The groups were matched based on gender and age.
Measures
Cognitive functioning
Cognitive functioning in the clinical group was assessed using the Wechsler Preschool and Primary School Intelligence (WPPSI), or the Wechsler Intelligence Scales for Children–Fourth Edition (WISC-IV) Australian versions. The cognitive functioning of the TYP group was assessed using the Wechsler Abbreviated Scales of Intelligence (WASI).
Parent-reported autism symptoms
Clinical symptoms of ASD were assessed using parent reports from the Social Responsiveness Scale (SRS), Children’s Communication Checklist–Second Edition (CCC-2), and the Repetitive Behaviours Questionnaire–Second Edition (RBQ-II). The CCC-2 is a 70-item parent report used to assess children’s communication abilities (Bishop, 2003). The device is used to screen for language and pragmatic impairment in children with communication problems. Higher scores indicate less impairment. Subscale reliability estimates from .66 to .80 have been reported in typical children. The SRS is a 65-item questionnaire used to assess social awareness, social information processing, capacity for reciprocal social communication, social anxiety/avoidance, and autistic preoccupations and traits in children from 4 to 18 years (Constantino, 2002). It has acceptable levels of internal consistency (.93-.97) and test–retest reliability (.77-.85). Parents use a 4-point rating scale to rate the severity of symptoms. The RBQ-II is a questionnaire that assesses the presence of repetitive behaviors in children (Leekam et al., 2007). Four subscales are measured in the RBQ-II, which closely link to the ICD-10 criteria for autism: unusual sensory interests, repetitive motor movements, rigidity/adherence to routine, and preoccupations with restricted patterns of interest. Parents answer 20 questions using a 3-point rating scale. Internal consistency for the 20 items was .85 (Leekam et al., 2007).
Parent-reported ADHD symptoms
Two measures of ADHD symptomatology were utilized, the Conners 3 and the Strengths and Weaknesses in Attention Deficit Hyperactivity Symptoms (SWAN). The Conners 3 Parent Short form is a 43-item parent report that identifies ADHD symptoms in a child based on DSM-IV-TR criteria (Conners, 2003). Six items identify hyperactive symptoms, and 5 identify inattentive symptoms. Responses are indicated on a 4-point scale from not true at all to very much true. Test–retest reliability ranges from .71 to .98 and internal consistency ranges from .77 to .97. The SWAN (Swanson et al., 2006) is an 18-item parent report scale with subscales in the domains of inattention (9 items) and hyperactivity (9 items) based on the DSM-IV ADHD symptoms. Responses are indicated using a 7-point Likert-type scale from far below (−3), below (−2), slightly below (−1), average (0), slightly above (1), above (1), and far above (3). This allows for a normal distribution of data and also provides more sensitivity in assessing symptoms. The scale asks for ratings in comparison with the participant’s peers and therefore can be used across a range of age groups. Reliability using Cronbach’s alpha has been reported to be .98 (Wilding & Burke, 2006).
Procedure
The study was approved by the Monash University Human Research Ethics Committee and the Victorian Department of Education and Early Childhood Ethics Committee. Parents received an explanatory statement and provided written informed consent. Participation was voluntary and participants did not receive any monetary reward for participation other than reimbursement for travel costs.
Parents of participants were invited to participate via email or letter and follow-up telephone call. Participants were tested at a home visit, at the Monash University Clayton campus, or at their primary school. Cognitive assessments were administered according to standardized instructions. Parents completed the questionnaires as per their standard instructions. Age-based standardized scores were utilized for the IQ tests. Raw scores were used for the SRS, RBQ-II, CCC-2, Conners 3, and SWAN. All data were entered into Statistical Package for the Social Sciences (SPSS) version 18.0 for statistical analyses.
Results
The data were assessed for outliers. An outlier in each of the SWAN inattention and Conners 3 hyperactivity scale was detected and corrected with the next most extreme score plus one, as per Tabacknich and Fidell (2007). A one-way ANOVA revealed there was no difference in age between the groups (Table 1). ANOVA revealed a group difference in FSIQ, Verbal Comprehension Index (VCI), and Perceptual Reasoning Index (PRI). The boys and girls with ASD were matched on FSIQ, VCI, and PRI. Post hoc Bonferroni tests showed the TYP group had higher FSIQ scores than the ASD group, TYP boys had higher VCI scores than the ASD girls and boys, but there was no difference in the four groups on PRI despite the significance of the main ANOVA. Consequently, FSIQ was used as a covariate in the analyses. For the main analyses, two-way multiple ANOVAs were conducted with group (TYP and ASD) and gender (male and female) entered as independent variables and the SRS, CCC, RBQ, C3, and SWAN subscales as dependent variables, with FSIQ used as a covariate.
Summary Age and IQ Characteristics for the Autism Spectrum Disorder and Typically Developing Groups.
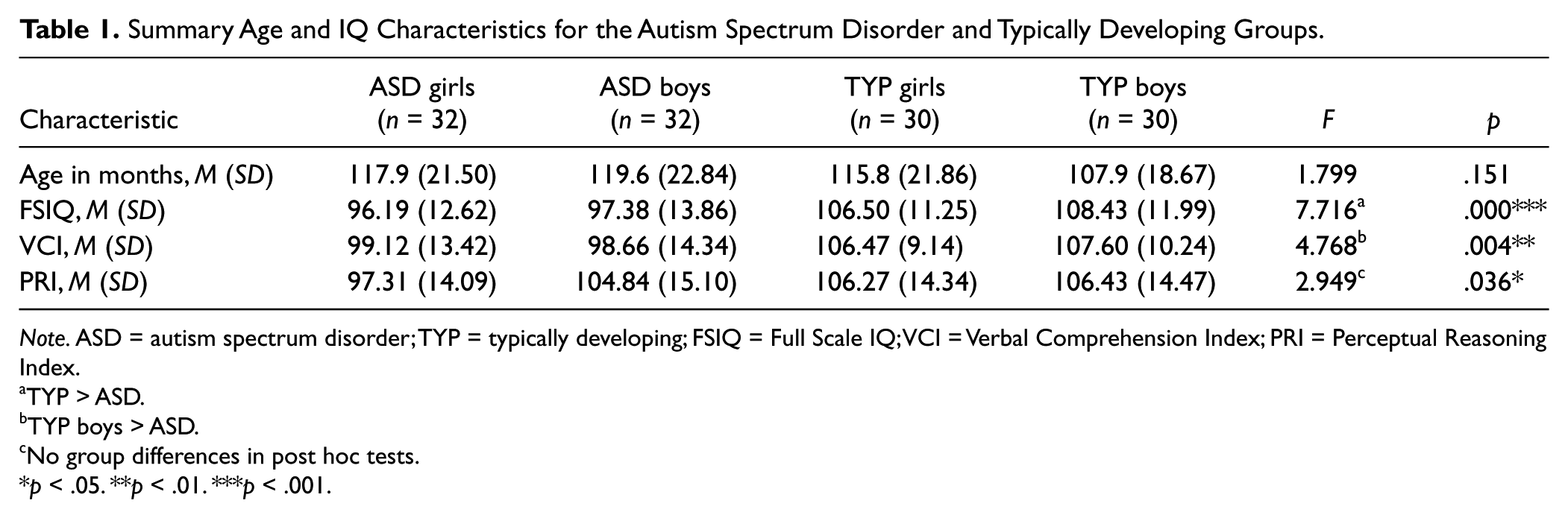
Note. ASD = autism spectrum disorder; TYP = typically developing; FSIQ = Full Scale IQ; VCI = Verbal Comprehension Index; PRI = Perceptual Reasoning Index.
TYP > ASD.
TYP boys > ASD.
No group differences in post hoc tests.
p < .05. **p < .01. ***p < .001.
Social ability
A two-way MANOVA revealed the ASD group had higher scores than the TYP group across all subscales and for the total SRS score (Table 2). There were no gender differences in any of the SRS subscales or total score, and no Group × Gender interactions (Table 2).
Differences Between SRS, RBQ, and CCC by Group and Gender.
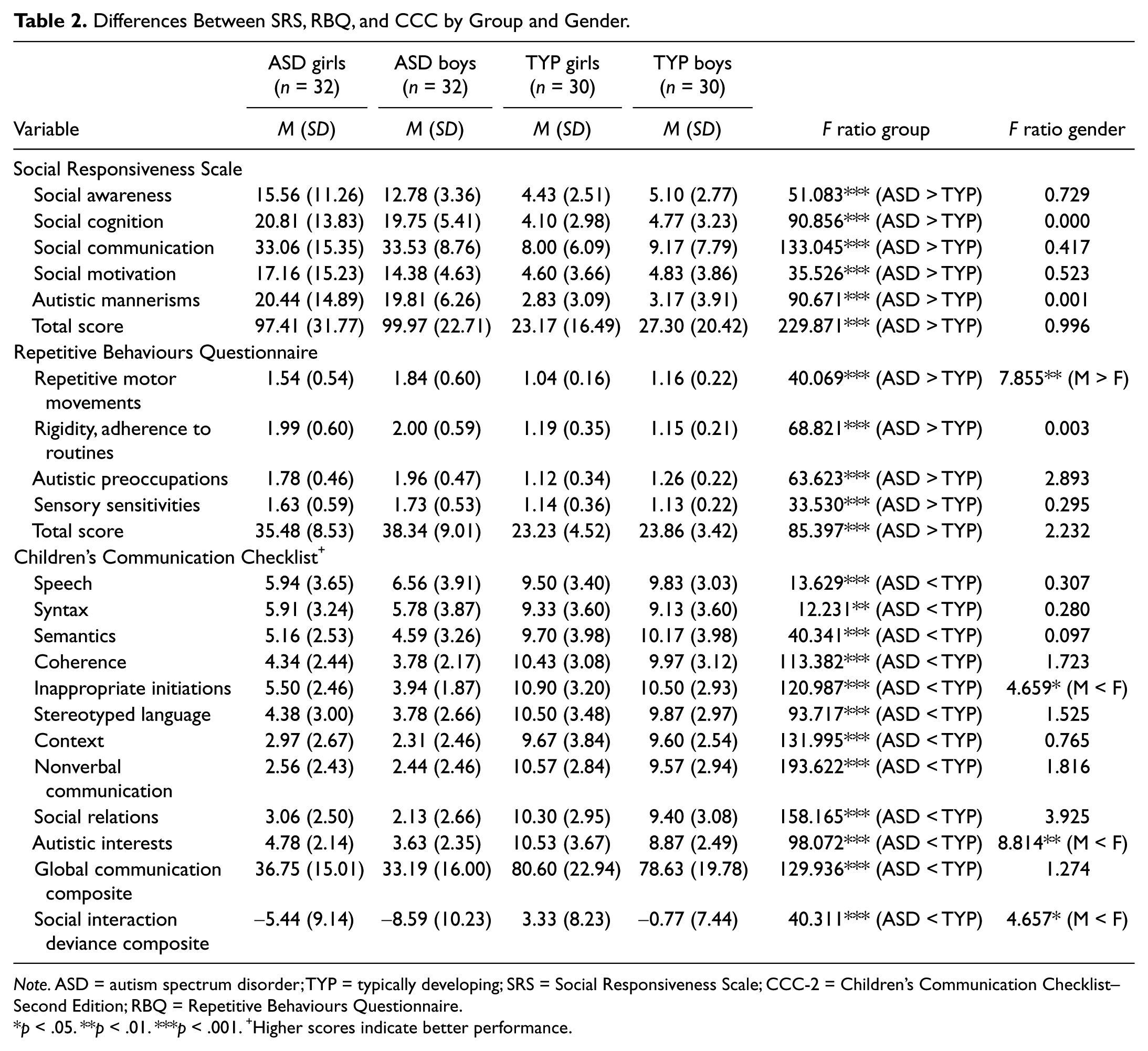
Note. ASD = autism spectrum disorder; TYP = typically developing; SRS = Social Responsiveness Scale; CCC-2 = Children’s Communication Checklist–Second Edition; RBQ = Repetitive Behaviours Questionnaire.
p < .05. **p < .01. ***p < .001. +Higher scores indicate better performance.
Repetitive behaviors
The two-way MANOVA revealed the ASD group had higher levels of repetitive behaviors across all subscales than the TYP group (Table 2). There was a main effect of gender on the Repetitive Motor Movements subscale, with males exhibiting more of these behaviors than females (p = .006). There were no Group × Gender interactions.
Communication ability
A two-way MANOVA revealed the ASD group had lower scores than the TYP group across all subscales (on this measure lower scores indicate poorer performance; Table 2). There was a main effect of gender on the Inappropriate Initiations (p = .033) and Unusual Interests (p = .004) subscales, where males had lower scores indicating more inappropriate initiations and autistic interests than females. Males also scored lower on the social interaction deviance composite (SIDC; p = .033), which indicates their language structure was better than their pragmatic language ability compared with females. There were no Group × Gender interactions.
Relationship between inattention, hyperactivity, group, and age
Data for inattention and hyperactivity scores were missing for 2 control girls and 1 control boy. To understand the interaction between age, sex, and group, the sample was divided in two based on the median age in the total sample of 116 months. There were 58 participants in the younger group (84-116 months of age; ASD: 12 males, 15 females; TYP: 12 females, 19 males) and 63 participants in the older group (117-155 months of age; ASD: 20 males, 17 females; TYP: 16 females, 10 males). A three-way MANOVA was used with group (ASD and TYP), gender (male and female), and age (older and younger) as the independent variables, and Conners 3 inattention and hyperactivity, and SWAN inattention and hyperactivity as the dependent variables. There were significant main effects of group, gender, and age (Table 3). The combined ASD group had higher levels of hyperactivity and inattention on both the SWAN and Conners 3 than the TYP group. The main effects of gender showed that boys had high levels of hyperactivity/impulsivity than girls on both the Conners 3 (p = .004) and the SWAN (p = .036). There was no gender difference in levels of inattention on the Conners 3, but boys had higher levels of inattention on the SWAN scale compared with girls (p = .041). There was also a main effect of age for Conners 3 (p = .005) and SWAN (p = .025) hyperactivity scales, with inspection of means revealing there was more hyperactivity in the younger age group. There was a significant interaction between group and gender for Conners 3 hyperactivity, F(1, 122) = 4.598, p = .034. Inspection of Figure 1 indicated that males with ASD had higher levels of hyperactivity than females with ASD, which was not reflected in the TYP group. There was also a significant interaction between group, gender, and age for Conners 3 hyperactivity, F(1, 122) = 4.279, p = .041. Inspection of Figure 2 and the means indicated that the level of hyperactivity was similar in young TYP boys (M = 3.00) and young TYP girls (M = 3.08), with older TYP boys (M = 2.50) having slightly higher levels of hyperactivity than older TYP girls (M = 1.38). In contrast, younger boys with ASD (M = 13.25) had much higher levels of hyperactivity than younger girls with ASD (M = 7.47). Older boys with ASD (M = 8.15) had more similar levels of hyperactivity than older girls with ASD (M = 6.82), reflecting the gender relationship in older TYP children.
Differences Between Conners 3 and SWAN Inattention and Hyperactivity Scales by Group and Gender and Age.
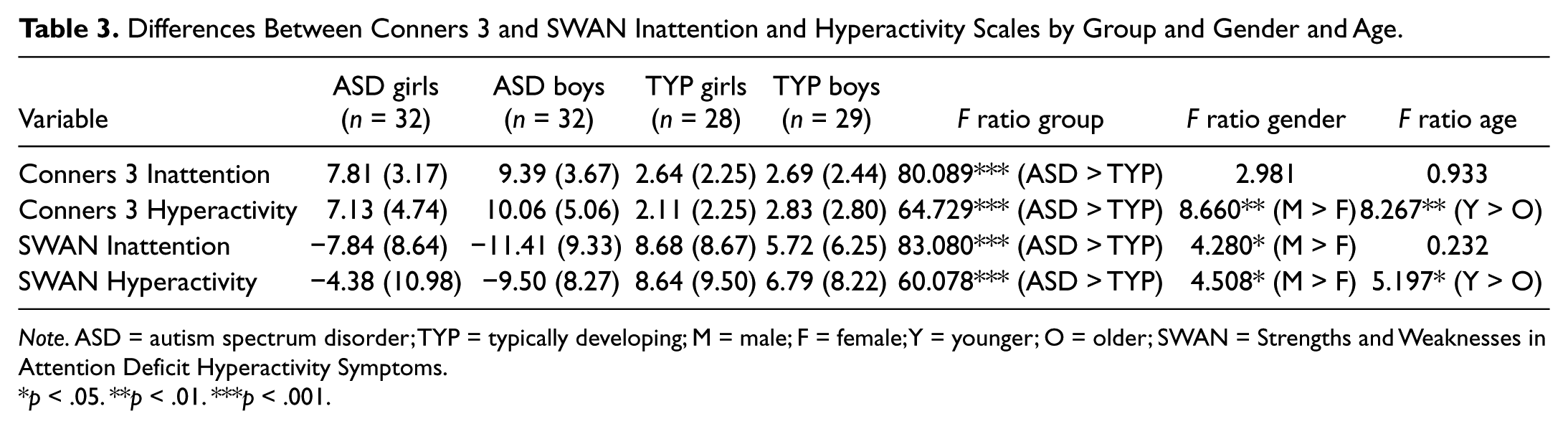
Note. ASD = autism spectrum disorder; TYP = typically developing; M = male; F = female; Y = younger; O = older; SWAN = Strengths and Weaknesses in Attention Deficit Hyperactivity Symptoms.
p < .05. **p < .01. ***p < .001.
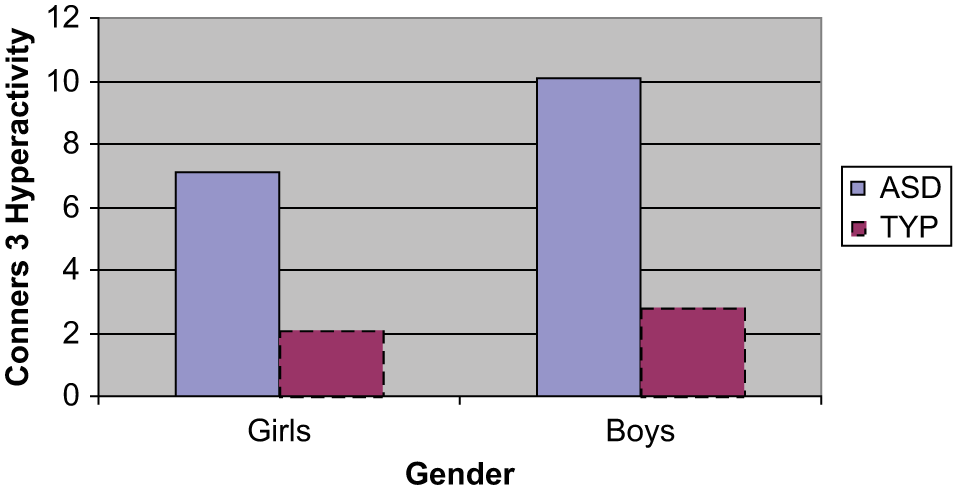
Gender by Mean Conners 3 hyperactivity raw score for the autism spectrum disorder and typical groups.
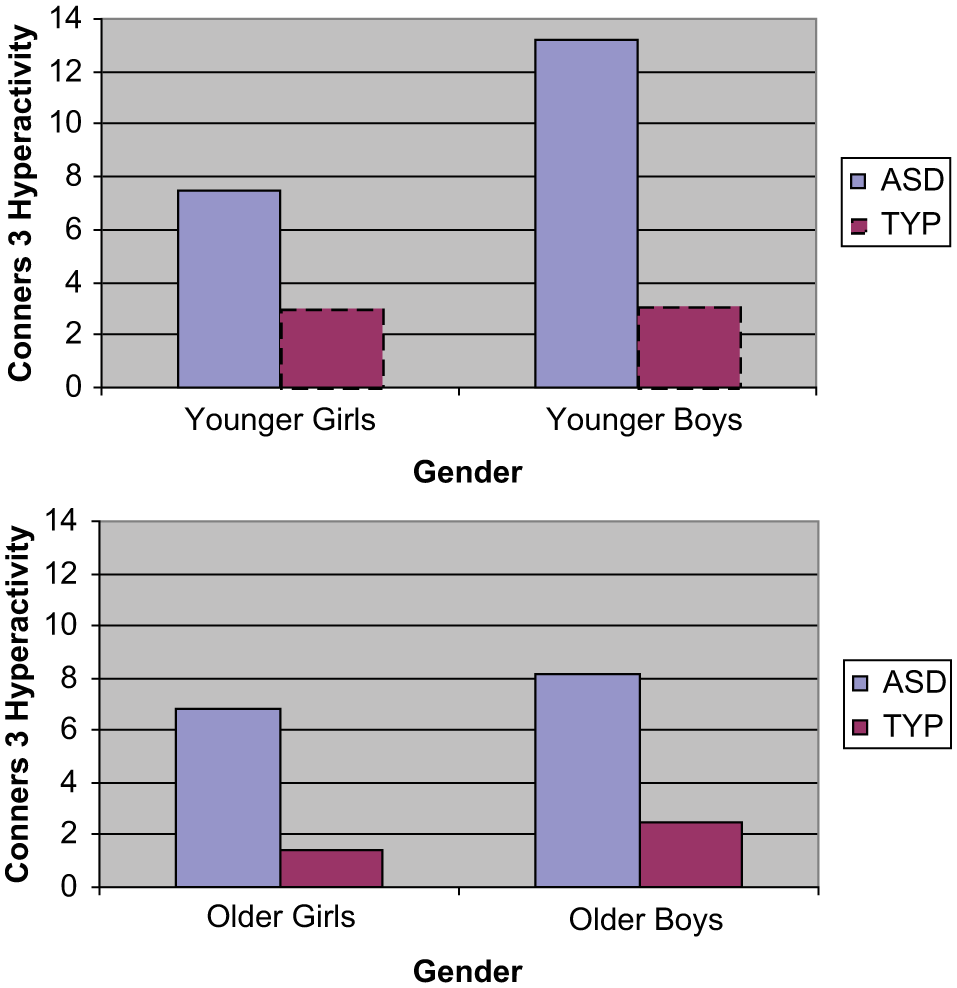
Gender by Mean Conners 3 Hyperactivity raw score for the autism spectrum disorder (ASD) and typical (TYP) group by age group.
Discussion
The last decade of ASD research has led to changes in our clinical conceptualization of ASD; for example, it is presently proposed for the DSM-V that ADHD and ASD can be dually diagnosed. Apropos of this, we know very little about girls with ASD and less about the ASD–ADHD profile in girls and boys. This study examined an age- and IQ-matched group of primary-school-aged boys and girls with ASD on parent-reported behavioral symptoms of ASD and ADHD. The study also included a TYP group to examine how gender differences may be unique to ASD or reflect gender differences found in the general population. Overall, our findings were that males with ASD showed more difficulties with repetitive motor movements, communication, and inattention, which were reflected in the TYP children. Younger boys with ASD also had higher levels of hyperactivity than younger girls with ASD, a gender finding unique to the ASD group, which could contribute to the difficulties of boy’s with ASD being more obvious than girls with ASD.
As hypothesized, there were no significant gender differences in level of social responsiveness in boys and girls with ASD or between typical boys and girls, suggesting that girls and boys with ASD present similarly regarding this core deficit of autism in this age group. This finding mirrors recent findings of similar social impairments in boys and girls with ASD (Mandy et al., 2011; Sipes et al., 2011; Solomon et al., 2012). In older adults, females have been reported to show better social abilities (Lai et al., 2011; Rivet & Matson, 2011), which may indicate improvement in social abilities with age in females with ASD. Longitudinal studies of well-matched samples of high-functioning girls are needed to understand whether gender differences in social ability (and other autistic symptom domains) show a specific trajectory across development.
Contrary to our hypothesis, the present study found gender differences on the communication measure. Boys showed more inappropriate initiations than girls, which involves talking repetitively about things that no one else is interested in. Boys also had more unusual interests relating to autism than girls on the CCC-2. Boys were also reported to have lower SIDC scores on the CCC-2 than girls, which indicates that girls had better pragmatic language relative to language structure than boys, regardless of group. Hartley and Sikora (2009) also found more communication deficits, and Carter et al. (2007) found more social and communication deficits, in girls compared with boys, although both of these studies examined younger children (1.5-3.9 years). The finding of more inappropriate verbal initiations, more autistic interests, and poorer pragmatic language skills in boys than in girls with ASD provides some evidence that impairment in boys with ASD may be more behaviorally obvious than in girls. These gender findings in relation to communication were not specific to the ASD group but were also reflected in the TYP group, indicating that these gender differences may reflect differences present in the general population.
As hypothesized, boys exhibited more repetitive motor movements than girls with ASD. This gender difference was also present in the TYP group, again indicating this finding was not unique to the ASD phenotype. Importantly, having more repetitive motor movements could make boys’ impairment more behaviorally noticeable than that of girls with ASD. There were no significant differences on the other repetitive behavior scales or on the total score, and potentially the sample size lacked power to detect more subtle differences, given findings of more repetitive and stereotyped behaviors in other studies (Hartley & Sikora, 2009; Hattier et al., 2011; Mandy et al., 2011; Sipes et al., 2011; Wing, 1981). Overall, in regard to autistic symptoms, the present findings indicate similar levels of social symptoms in girls and boys with ASD, but with some specific aspects of communication and repetitive behaviors showing more impairment in boys. These gender differences mirrored those found in the TYP group and hence were not specific to ASD. Of course, the causes of these differences can only be speculated upon in this study. These differences could be due to genetic or biological differences in the development of girls and boys. However, these differences could equally be due to the different socialization of boys and girls.
The hypothesis that boys would exhibit more hyperactive-impulsive behaviors than girls was also supported. This finding is consistent with other studies that have found more hyperactive behaviors in boys than in girls with ASD (Mandy et al., 2011) but not other studies (Brereton et al., 2006; Gadow et al., 2005). This finding mirrors the gender profile often observed in referred ADHD samples (Biederman, Mick, & Faraone, 2000; Gershon, 2002) where girls present with less hyperactive-impulsive symptoms and therefore may be underrepresented in clinical settings, and hence, underdiagnosed. However, there have also been findings of more difficulties in cognitive inhibition in girls than in boys with ASD (Lemon, Gargaro, Enticott, & Rinehart, 2011). Hence, behaviorally reported symptoms may not correspond to cognitive deficits, and factors such as rater bias needs to also be considered.
When the relationship between age and ADHD symptoms was examined, it was found that younger boys with ASD had much higher parent-reported levels of hyperactivity-impulsivity than younger girls with ASD. This difference was not reflected in the TYP group with the younger boys showing similar levels of hyperactivity to the younger girls. Older boys and girls with ASD had more similar levels of hyperactivity, with boys exhibiting slightly more symptoms. This was similar to the older TYP group. This finding indicates that boys with ASD may show a decrease in hyperactivity symptoms with age, which is typically found in boys with ADHD (Biederman et al., 2000; Monuteaux et al., 2010). However, this relationship was not found for girls with ASD which indicates levels of hyperactivity-impulsivity may remain more persistent, but at lower levels for girls than boys, across this age range. The finding of more hyperactivity in younger boys was in contrast to Mandy et al. (2011) who found no age changes; however, they used a combined inattention and hyperactivity construct, which may obscure age-related changes, given inattention may not be as remittent as hyperactivity. Boys were also found to show more inattention on the SWAN scale, but not the Conners 3 scale. The different findings between the measures may relate to the SWAN being more sensitive with a 7-point scale and based on a normal distribution compared with the Conners 3. The finding of more inattention in boys was not dependent on group, again indicating a more general population difference. There was no decline with age for inattention symptoms in the sample, indicating persistent levels of difficulties with inattentive behaviors in children with ASD over this age range.
A limitation of this study is the sample size of approximately 30 in each group, as there may not have been enough statistical power to detect subtle differences between groups. However, this sample of girls is still larger than a number of prior studies (Holtman et al., 2007; Lai et al., 2011; McLennon et al., 1993; Pilowsky et al., 1998; Solomon et al., 2012) and has employed a narrower age range. It is also important to note the large number of comparisons in the current study which were not corrected with Bonferroni adjustments; therefore, some findings may be Type II errors. Hence, our findings should be interpreted with caution and we have included p levels to indicate the strength of the findings. Children in this study were also clinically referred and hence may be more severely impaired and show a different pattern of difficulties than a non-referred sample. Furthermore, this sample is cross-sectional; therefore, the changes with age need to be confirmed in a longitudinal study. Finally, this study has used parent reports of symptoms, which may be biased by parental expectations based on gender stereotypes. For example, parents may rate girls as having fewer repetitive behaviors and better social-communication ability, in line with common gender expectations of these behaviors in girls (McLennon et al., 1993).
In summary, girls and boys with ASD showed similar social difficulties, but boys were reported to have more repetitive motor movements and communication impairments. These differences reflected typical population differences rather than being unique to the autism phenotype. This highlights the importance of including a TYP comparison group when conducting research into gender differences in this field. Hyperactivity-impulsivity appears to show an age–gender profile in ASD: Younger boys were significantly more hyperactive than younger girls, a pattern not present in younger TYP boys and girls. Inattention levels were persistent in boys and girls with ASD across this age range. Clinicians need to be aware of the particularly high levels of hyperactivity in younger males with ASD and appropriately treat and manage these symptoms. The proposed change in the DSM-V to allow a comorbid diagnosis of ADHD in ASD may assist in this regard. Notably, high levels of hyperactivity in younger males may prompt clinical assessment. Combined with the subtle gender differences in communication and repetitive behaviors found in this study, these factors could partially contribute to more high-functioning early-school-age boys than girls being referred and subsequently diagnosed with an ASD. These findings call for future work on gender differences in ASD to move beyond core autistic symptomatology, to more fully elucidate other factors like attentional profiles, which may result in gender-based referral bias and the underrepresentation of girls with ASD.
Footnotes
Acknowledgements
The authors would like to thank all the children and families who participated in this research study, Dr Katie Heathershaw from the Melbourne Children’s Clinic, and AMAZE (Autism Victoria).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nicole Rinehart is an Associate Professor at Monash University and is also a clinical psychologist who consults at the Melbourne Children’s Clinic where children with autism were recruited from. Associate Professor Rinehart is also a member of the Australian National Health and Medical Research Council Expert Working Group on ADHD Clinical Practice Points.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.