
Abstract
Pathological hoarding is characterized by (a) the excessive accumulation of and the inability to discard large volumes of possessions; (b) cluttered, disorganized living spaces; and (c) significant distress or impaired daily living, which affects overall health and well-being (Frost & Hartl, 1996). The community incidence of hoarding behaviors has been estimated between 2% and 5% (Iervolino et al., 2009; Timpano et al., 2011) with hoarding symptoms being related to substantial psychosocial and functional morbidity, such as comorbid psychopathology (Frost, Steketee, Williams, & Warren, 2000; Grisham, Steketee, & Frost, 2008; Mataix-Cols, Baer, Rauch, & Jenike, 2000; Samuels et al., 2002), lower rates of marriage (Frost & Gross, 1993; Samuels et al., 2002), and higher incidences of isolation and limited social networks (Samuels et al., 2002). In addition, hoarding represents a significant public health concern; as many as 12% of hoarders have been evicted or threatened with eviction from their homes, 3% have had a child or elderly relative removed from the home, and 6% of all fire-related deaths are attributed to hoarding (Tolin, Frost, Steketee, Gray, & Fitch, 2008).
Considering the deleterious consequences linked to hoarding behaviors, it is important to understand its etiology and the potential pathways through which hoarding is maintained across development. Until recently, most research on hoarding has been focused on adults, with few empirical data reported on hoarding in children, despite symptoms commonly having onset during childhood (Grisham, Frost, Steketee, Kim, & Hood, 2006; Tolin, Meunier, Frost, & Steketee, 2010). Given this gap in the extant literature, there exists a definitive need to examine hoarding symptoms in a range of pediatric samples, including those with and without other psychiatric difficulties. Such investigations may also help shed light on the nosology of hoarding, which remains unclear. Traditionally, hoarding has been conceptualized as a subtype of obsessive-compulsive disorder (OCD); however, recent findings within the clinical, genetic, treatment, and neuropsychological research fields have provided credence to the notion that hoarding may reflect a separate syndrome (Mataix-Cols et al., 2010; Pertusa et al., 2008).
Emerging data suggest that pathological hoarding may be more closely associated with attention-deficit/hyperactivity disorder (ADHD; Tolin & Villavicencio, 2011). There are several lines of evidence supporting a linkage between hoarding and ADHD. First, the core features of hoarding (i.e., clutter, difficulty discarding, and acquisition) partially arise from observed deficits in executive functioning (e.g., organization, sustained attention, long-term planning), which are very similar to those seen in ADHD (Barkley, 1997). For example, adult hoarders show more problems than nonhoarders on neurocognitive tasks that involve spatial memory, working memory, sustained attention (Grisham, Brown, Savage, Steketee, & Barlow, 2007), planning, and problem solving (Frost & Hartl, 1996; Grisham, Norberg, Williams, Certoma, & Kadib, 2010), and utilize less effective organizational strategies (Hartl, Duffany, Allen, Steketee, & Frost, 2004). Only one study to date directly examined the association between ADHD and hoarding, and demonstrated that the severity of inattention significantly predicted the severity of core features of hoarding, whereas obsessive-compulsive symptoms did not (Tolin & Villavicencio, 2011). Likewise, impulsivity, a core feature of ADHD, has been linked to hoarding symptoms (Grisham et al., 2007; Frost, Meagher, & Riskind, 2001; Frost, Steketee, & Williams, 2002). Hoarding symptoms are often prevalent among compulsive gamblers (Frost et al., 2001) and shoppers/buyers (Frost et al., 2002), suggesting impaired behavioral inhibition. It may be that hoarders impulsively acquire possessions resulting in large quantities of unnecessary belongings and simultaneously are unable to organize their environment effectively, due to impaired executive functions (Frost & Hartl, 1996; Storch, Muroff, et al., 2011; Storch, Rahman, et al., 2011).
Second, although pathological hoarding differs from nonhoarding OCD in a variety of ways, some evidence linking hoarding with ADHD may be gleaned from the OCD literature. Both OCD and ADHD are neurodevelopmental disorders that onset during childhood and exhibit frequent overlap with tic disorders suggesting similar neurobiological etiological pathways (Gaze, Kepley, & Walkup, 2006; Kadesjo & Gillberg, 2000). Although most individuals who hoard do not have OCD (Samuels et al., 2008; Steketee & Frost, 2003), hoarding behaviors are present in 18% to 42% of adults (Hanna, 1995; Rasmussen & Eisen, 1992; Samuels et al., 2002) and 25% to 30% of children with OCD (Storch et al., 2007). Clinicians frequently report symptoms of ADHD among individuals diagnosed with OCD, with as many as 20% of adults (Sheppard et al., 2010) and 30% of children (Geller, Biederman, Griffin, Jones, & Lefkowitz, 1996) being diagnosed with ADHD. Indeed, Sheppard et al. (2010) demonstrated that of adults with OCD and comorbid ADHD, 41.9% also exhibited compulsive hoarding, whereas only 29.2% of participants with OCD and without ADHD presented with pathological hoarding. Furthermore, ADHD was the only marker they examined that was independently associated with pathological hoarding.
Finally, hoarding behaviors among those with ADHD may be characteristically different from hoarding behaviors observed among individuals with OCD supporting a link with ADHD. Although not ADHD specific, Grisham, Brown, Liverant, and Campbell (2005) found that the primary difference between OCD-diagnosed individuals with comorbid hoarding and those with pathological hoarding absent of an OCD diagnosis include anxiety-evoking thoughts and compulsions. Specifically, pure hoarders displayed lower levels of negative affect, depression, anxiety, and distress relative to both OCD patients with and without hoarding symptoms. The potential difference between those who hoard with and without comorbid OCD suggests a fundamental difference in etiology of the behavior. As a result, some researchers have argued that hoarding can only be considered a symptom of OCD when in the presence of other primary OCD behaviors (e.g., washing, counting, checking) or when hoarding is secondary to compulsions (Abramowitz, Wheaton, & Storch, 2008; Grisham et al., 2005; Wu & Watson, 2005). It may be that individuals with ADHD who hoard do so as a result of the core symptoms of inattention, hyperactivity/impulsivity of ADHD, indicating a more neurological, rather than compulsive, anxiety-driven etiology.
To date, very few investigations have examined the link between hoarding and ADHD, and they have almost exclusively focused on adult populations. As noted above, these studies highlight the potential associations between pathological hoarding, executive function impairment, and ADHD symptoms. There are three studies that have directly examined hoarding behaviors among children. Storch et al. (2007) demonstrated that, relative to children with OCD without hoarding, children with OCD and hoarding displayed higher levels of attention problems, aggression, and overall externalizing symptoms, all of which are frequently observed among children with ADHD. Storch, Muroff, et al. (2011) examined hoarding behaviors among children diagnosed with OCD and found that parent-reported child hoarding was not related to OCD symptom severity but was significantly related to parent ratings of attention problems and externalizing behaviors. Testa, Pantelis, and Fontenelle (2011) examined the presence of hoarding behaviors among 61 children diagnosed with learning disabilities and found that 16.4% displayed clinically significant hoarding behaviors. Of the group that displayed hoarding symptoms, only 30% exhibited OCD, whereas 50% of those with hoarding symptoms met criteria for a diagnosis of ADHD.
Although the few studies of hoarding in children have been informative, no data exist on the occurrence of pathological hoarding among children diagnosed with ADHD without a primary diagnosis of OCD. Given the associations of ADHD symptoms with hoarding behaviors identified in adults and preliminary data in children, the investigation of hoarding within a childhood ADHD sample has important implications with regard to understanding the etiology of hoarding, as well as relevance for assessment and treatment in children with ADHD. With regard to etiology, these data may demonstrate a linkage between childhood ADHD and hoarding, which may be suggestive of mechanisms through which hoarding behaviors may emerge. Regarding assessment, these data will provide a foundation for clinicians who work with children with ADHD to understand the extent to which hoarding behavior is problematic and what factors are associated with hoarding severity. Finally, given that hoarding behaviors were uniquely associated with impairment beyond obsessive-compulsive symptoms (Storch et al., 2007), targeting this domain in treatment may yield clinical benefits for those families of a child with ADHD.
Accordingly, this study seeks to examine the nature of pathological hoarding among children and adolescents with ADHD. We had five specific research questions:
Research Question 1: What is the frequency of clinically significant hoarding behaviors among children with ADHD?
Research Question 2: Do children with ADHD who hoard differ in clinical characteristics relative to nonhoarding children with ADHD?
Research Question 3: To what extent are hoarding symptoms associated with symptoms of inattention and/or hyperactivity/impulsivity?
Research Question 4: Do ADHD symptoms predict hoarding behaviors more robustly than nonhoarding obsessive-compulsive symptoms?
Research Question 5: Do hoarding symptoms mediate the relationship between ADHD symptom severity and disruptive behaviors?
Within such a model, ADHD severity is hypothesized to increase hoarding, which in turn increases disruptive behavior by virtue of limit setting, having to discard possessions, and child frustration due to an inability to meet the demands of organization due to impairment.
Method
Participants and Procedures
Participants included 99 treatment-seeking children and adolescents diagnosed with ADHD who were seen in a general outpatient child and adolescent psychiatry clinic. All participants had a primary or coprimary diagnosis of ADHD according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000). Diagnoses were determined via best estimate procedures (Leckman, Sholomaskas, Thompson, Belanger, & Weissman, 1982) in which consensus between two psychiatrists (one the treating clinician) regarding the ADHD diagnosis and the presence of comorbid diagnoses was required for inclusion. In this procedure, all available information was incorporated into ascertaining an accurate diagnostic profile. This involved having two attending psychiatrists experienced in pediatric ADHD examine past clinical records and review participants’ completed measures as part of this study. Participants were excluded in the absence of 100% agreement for the ADHD or comorbid diagnoses or if diagnosed with psychosis, autism spectrum disorder, or mental retardation.
Sample demographics are shown in Table 1. The sample consisted of 99 children outpatients (35% female) diagnosed with primary ADHD-inattentive (20.2%) or ADHD-combined type (79.8%). Ages of participants ranged from 8 to 17 years (M = 11.54, SD = 2.5 years). Race and ethnicity were reported as the following: 89% Caucasian, 1% Asian/Pacific Islander, 5% African American, and 3% Hispanic. A total of 68 participants (68%) were diagnosed with a comorbid psychiatric disorder.
Sample Characteristics of Hoarders and Nonhoarders Among Youth With ADHD.
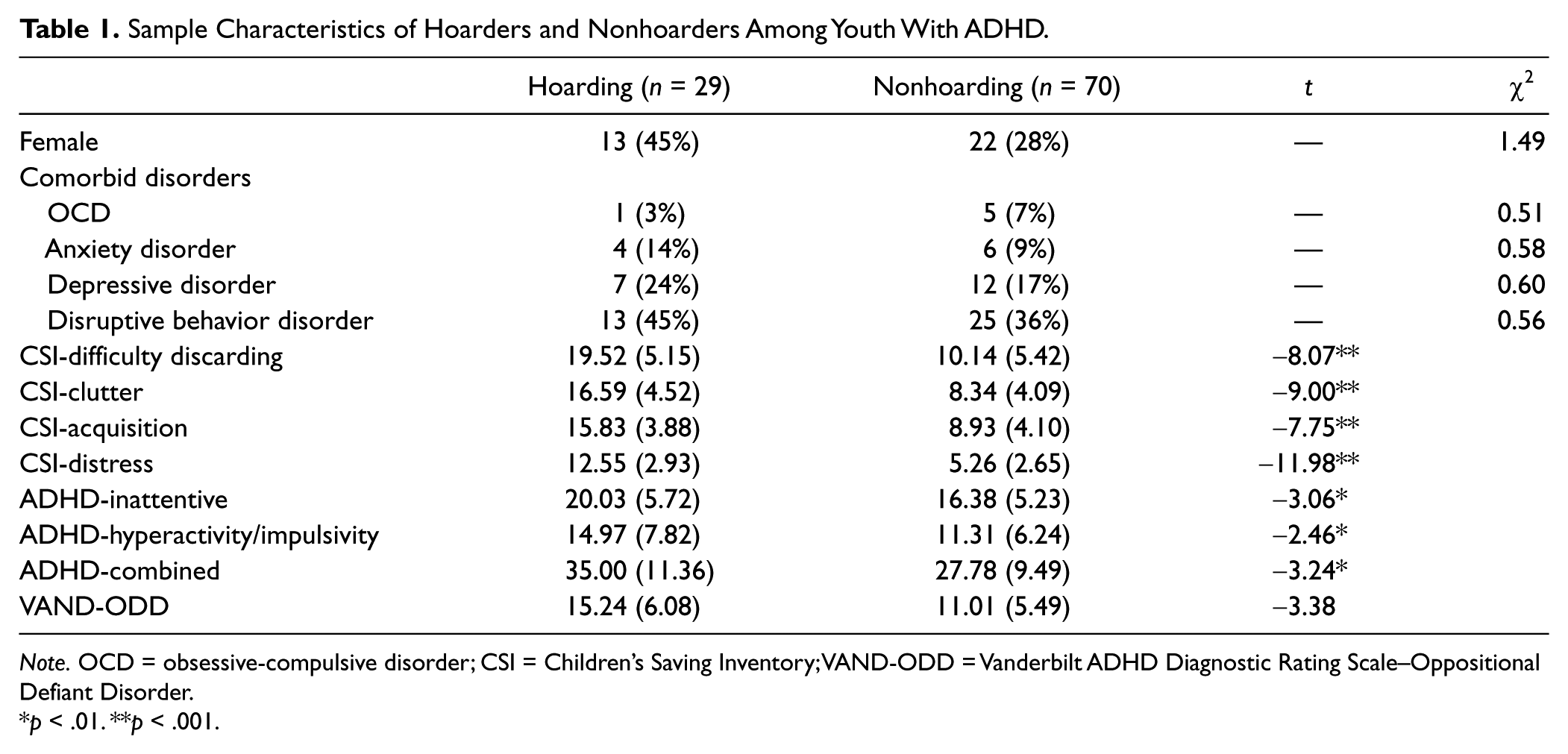
Note. OCD = obsessive-compulsive disorder; CSI = Children’s Saving Inventory; VAND-ODD = Vanderbilt ADHD Diagnostic Rating Scale–Oppositional Defiant Disorder.
p < .01. **p < .001.
Permission to conduct this research was approved by the local institutional review board, and written parental consent and child assent were collected before initiating study procedures. Following the participant’s regularly scheduled appointment with the clinician, those participants who met study inclusion criteria and were interested in participating were referred to research staff. Thereafter, a trained member of the research staff reviewed all consent and assent forms and all measures with both parent and child. To protect confidentiality, the parent and child were provided with separate rooms to independently complete questionnaire measures. A member of the research staff remained available to answer any questions and/or assist the child in completing the assessment packet.
Measures
Demographic Information Form
The Demographic Information Form is an intake form collecting the following information from the parent: his or her relationship to child, socioeconomic status, parents’ education level, family structure (married, single, divorced, etc.), child’s age, gender, grade level, current psychiatric medication, and other treatment being received (e.g., psychotherapy).
Children’s Saving Inventory (CSI)
The CSI (Storch, Muroff, et al., 2011) is a 23-item parent-rated measure designed to assess child-hoarding behaviors. Items assess parent perceptions of their child having problems with discarding unneeded items, compulsive acquisition, and clutter on a 5-point rating scale, ranging from 0 = none to 5 = almost all/completely. The rating scale has been shown to exhibit strong internal consistency, excellent retest reliability, and favorable validity (Storch, Muroff, et al., 2011).
Obsessive-Compulsive Inventory–Child Version (OCI-CV)
The OCI-CV (Foa et al., 2009) is a 21-item child-report measure assessing the presence and associated distress of obsessive-compulsive behaviors. The measure has six-factor analytically derived subscales, including Washing, Checking, Ordering, Obsessing, Hoarding, and Neutralizing. The OCI-CV nonhoarding total score derived from the Washing, Checking, Ordering, Obsessing, and Neutralizing subscales. The OCI-CV has shown strong retest reliability and internal consistency, as well as significant correlations with clinician-rated obsessive-compulsive symptom severity (Foa et al., 2009).
Vanderbilt ADHD Diagnostic Rating Scale–Parent Version (VAND-P)
The VAND-P (Wolraich et al., 2003) is a widely used parent-report ADHD symptom rating scale that includes a short Oppositional Behavior subscale. A total of 26 items are answered on a 4-point scale from 0 = never to 3 = very often. Items 1 to 9 assess inattentive subtype (ADHD-inattentive), Items 10 to 18 assess hyperactive/impulsive subtype (ADHD-hyperactive/impulsive), and Items 1 to 18 assess combined subtype (ADHD-combined). Items 19 to 26 assess symptoms of oppositional defiant disorder (Vanderbilt ADHD Diagnostic Rating Scale–Oppositional Defiant Disorder [VAND-ODD]). The VAND-P has shown good to excellent internal consistency and reliability for each of the subscales. The Vanderbilt has adequate psychometric properties including strong internal consistency and factor structure (Wolraich et al., 2003).
Revised Child’s Anxiety and Depression Scale (RCADS)
The RCADS (Chorpita, Yim, Moffitt, Umemoto, & Francis, 2000) is a 47-item self-report inventory that assesses anxiety and depression within six separate subscales: Separation Anxiety Disorder, Social Phobia, Generalized Anxiety Disorder, Panic Disorder, OCD, and Major Depressive Disorder. Two subscales were used: the Major Depressive Disorder subscale, 10 items, and the Generalized Anxiety Disorder subscale, 6 items. The scale is answered on a 4-point scale from 0 = never to 3 = always. The scale has shown excellent psychometric properties and has robust construct validity (Chorpita et al., 2000).
Rosenberg’s Self-Esteem Scale (SES)
The SES (Rosenberg, 1989) is a 10-item self-report scale, which assess the child’s overall self-esteem. Appropriate for children ages 8 to 17, the SES is answered on a 4-point scale ranging from strongly agree to strongly disagree and has demonstrated strong reliability and validity properties (Blascovich & Tomaka, 1993).
Data Analysis
Cutoff scores for clinical levels of hoarding were determined by utilizing the total score that would be obtained if an individual answered “2” or “Moderate” on each item of the CSI, which is generally consistent with the cutoff empirically determined for the Saving Inventory–Revised (Frost & Hristova, 2011). Those receiving a CSI score of ≥46 were classified as exhibiting significant hoarding, whereas those below the cutoff score were defined as not presenting with significant hoarding. Comparisons regarding differences in comorbidity patterns and clinical characteristics as a function of hoarding status were conducted utilizing χ2 and t tests. Pearson product–moment correlation coefficients were computed to examine associations among study variables.
Five multiple regressions were conducted to examine associations between ADHD and hoarding symptoms. Inattention and hyperactivity/impulsivity symptoms were set as predictors of each of the four areas of hoarding (clutter, difficulty discarding, acquiring, distress) and the CSI-total score.
To examine the predictive power of ADHD symptoms when controlling for nonhoarding obsessive-compulsive symptoms, a hierarchical multiple regression was conducted with child-reported nonhoarding obsessive-compulsive symptoms (OCI-CV nonhoarding total score) entered in the first block, and ADHD-combined symptoms (ADHD-combined) entered in the second block. For all above-mentioned statistical tests, significance levels were set at p < .05.
Finally, a mediation analysis via bootstrapping methods (Hayes, 2009) was conducted to examine the relationship between inattentive symptoms, hoarding symptoms, and oppositional symptoms. Combined ADHD symptoms (ADHD-combined) were set as the independent variable, oppositional symptoms (VAND-ODD) as the dependent variable, and hoarding symptoms (CSI-total score) as the mediating variable. A total of 5,000 bootstrap samples were evaluated, and the presence of a statistically significant indirect effect, indicating a statistically significant mediational effect, was determined by the exclusion of the value zero from the 95% confidence intervals (CIs).
Results
Sample Characteristics
In all, 29 of 99 participants (29%) reported clinical levels of hoarding. Descriptive statistics for hoarders and nonhoarders are presented in Table 1. Groups did not differ significantly in regard to gender or comorbidity rates. The hoarding group reported higher CSI scores across each of the subscales. Relative to the nonhoarding group, the hoarding group exhibited higher scores on measures of inattention, hyperactivity/impulsivity, and oppositional symptoms. No differences were found between the hoarding and nonhoarding groups in regard to rates of child-reported depressive and anxiety symptoms, or child-reported self-esteem.
Associations With Hoarding Severity
The OCI-CV Hoarding subscale and CSI-total score were significantly and modestly correlated, r(94) = .31, p < .01. Table 2 presents associations between the ADHD-inattentive, ADHD-hyperactive/impulsive, ADHD-combined, and the CSI-total score and subscales. Inattentive symptoms were significantly correlated with CSI-total score, difficulty discarding, clutter, and hoarding-related distress. Hyperactivity/impulsivity symptoms were significantly correlated with CSI-total score, difficulty discarding, acquisition, and hoarding-related distress. Combined ADHD symptoms were significantly associated with CSI-total score as well as all CSI subscales.
Associations Between ADHD and Hoarding Symptoms.
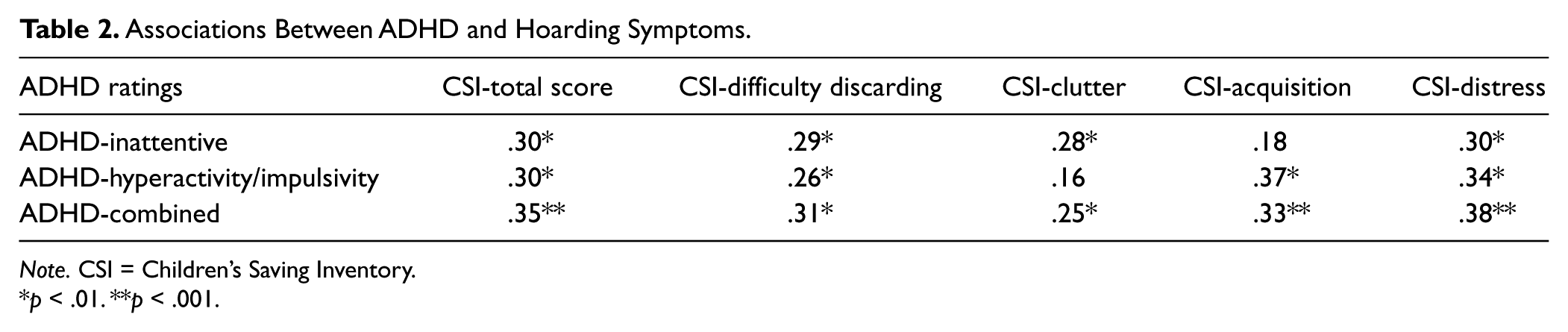
Note. CSI = Children’s Saving Inventory.
p < .01. **p < .001.
Predictors of Hoarding Severity
Table 3 presents results of regression analyses predicting overall hoarding symptoms, clutter, difficulty discarding, acquisition, and hoarding-related distress. Inattentive symptoms were significant predictors of overall hoarding symptoms, difficulty discarding, and clutter. Hyperactivity/impulsivity symptoms were significant predictors of acquisition and hoarding-related distress. Inattentive symptoms approached significance when predicting hoarding-related distress, and hyperactivity/impulsivity symptoms approached significance to overall hoarding symptoms.
Results of Multiple Regressions Predicting CSI-Total Score and Subscales.
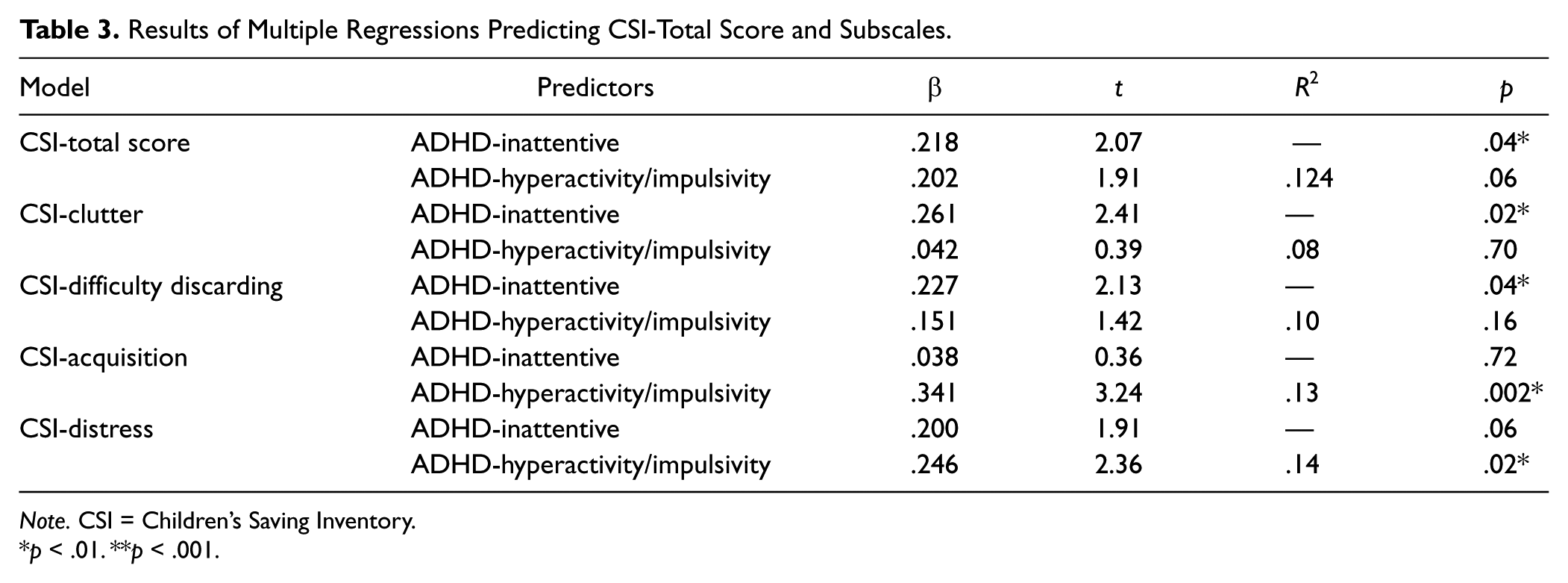
Note. CSI = Children’s Saving Inventory.
p < .01. **p < .001.
Table 4 presents results revealed from the hierarchical regression analysis predicting CSI-total score. In the first block, OCI-CV nonhoarding total score was not a significant predictor of the CSI-total score. In the second block, ADHD-combined significantly predicted CSI-total score above and beyond OCI-CV nonhoarding total score.
Results of Linear Regression Predicting CSI.
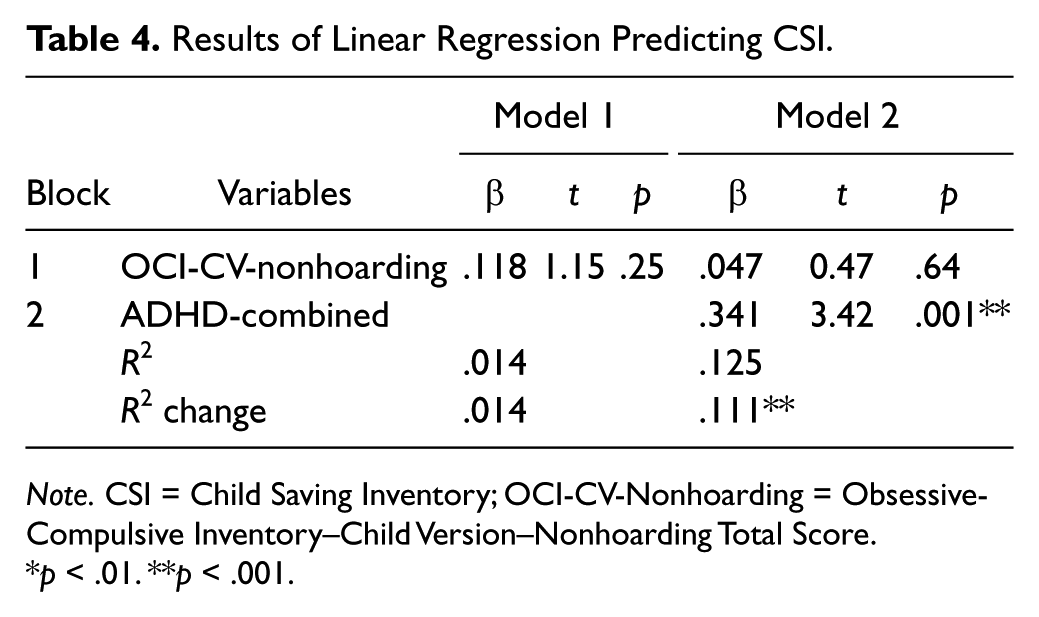
Note. CSI = Child Saving Inventory; OCI-CV-Nonhoarding = Obsessive-Compulsive Inventory–Child Version–Nonhoarding Total Score.
p < .01. **p < .001.
Mediational Analysis
Results of the mediation analyses are shown in Table 5. There was a significant direct effect between ADHD symptoms and oppositional behaviors. In the presence of hoarding symptoms as a mediator, the effect was still significant. However, given that the 95% limits did not include zero (CI = [.005, .093]), the model was consistent with mediation.
Results of Analyses Examining Hoarding Severity As a Mediator of ADHD-Combined and Oppositional Symptoms.
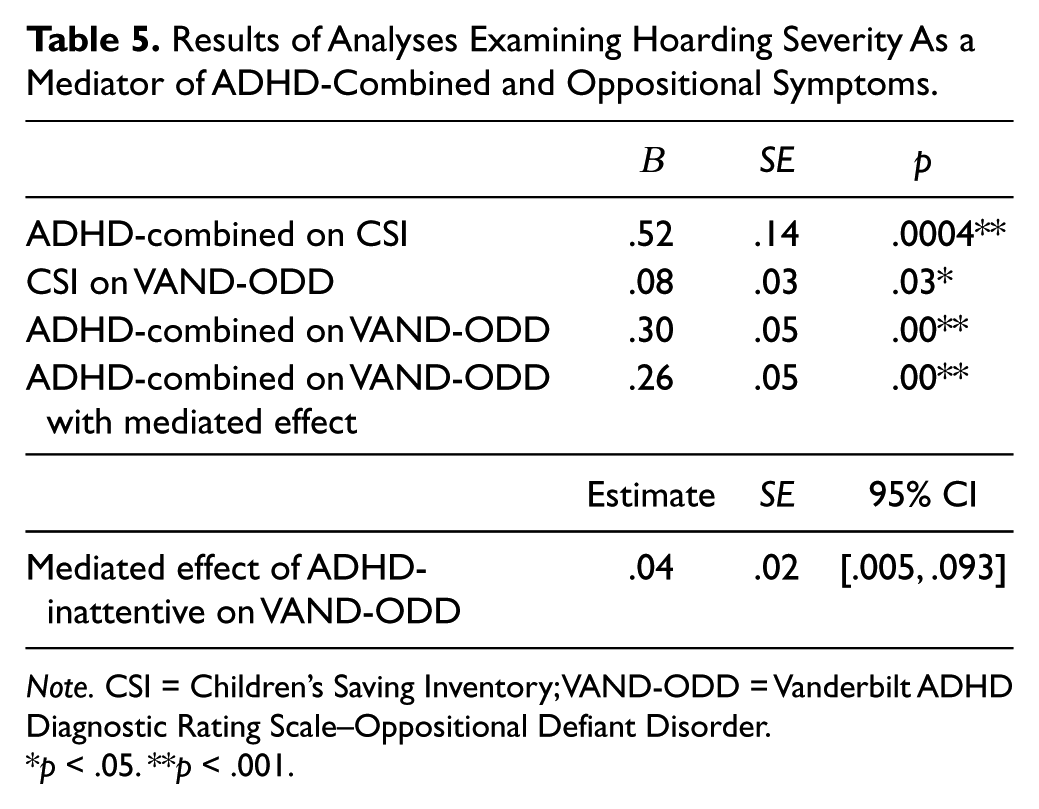
Note. CSI = Children’s Saving Inventory; VAND-ODD = Vanderbilt ADHD Diagnostic Rating Scale–Oppositional Defiant Disorder.
p < .05. **p < .001.
Discussion
We report data examining the nature of pathological hoarding among children with ADHD. Some data in adult samples suggest an association between hoarding behaviors and ADHD (e.g., Sheppard et al., 2010; Tolin & Villavicencio, 2011) although, to date, this has not been examined in youth. Overall, the frequency of hoarding symptoms among children with ADHD (29%) was comparable with that reported in pediatric OCD samples (Storch et al., 2007; Storch, Muroff, et al., 2011; Storch, Rahman, et al., 2011) and highlights the relative frequency with which clinically significant hoarding occurs among youth with ADHD. The lack of significant difference in terms of comorbidity or self-reported depression or anxiety between the hoarding and nonhoarding groups is interesting considering that youth with OCD who hoard experience higher rates of internalizing disorders (Storch et al., 2007). The lack of differences may suggest that hoarding is maintained through a specific pathway of cognitive deficits associated with ADHD. Therefore, comorbidity, although common to ADHD (Jarrett & Ollendick, 2008), may not influence the presence of ADHD-related hoarding. Rather, comorbid conditions may emerge later in life associated, in part, with social, family, and occupational issues due to hoarding (Frost & Gross, 1993; Samuels et al., 2002). The absence of gender differences in this sample is consistent with findings in recent epidemiological studies, in which males and females did not differ in terms of hoarding (Fullana et al., 2010; Mueller, Mitchell, Crosby, Glaesmer, & de Zwaan, 2009; Timpano et al., 2011).
Interestingly, ADHD symptom severity was the only indicator that differentiated the two groups, in that those with clinically significant hoarding displayed significantly greater ADHD symptom severity than the nonhoarding group. Consistent with Tolin and Villavicencio (2011), nonhoarding obsessive-compulsive symptoms did not significantly predict hoarding in the present sample, whereas ADHD symptoms did. This suggests that hoarding may not originate in anxiety-driven obsessions, and rather stem from clinical features common to ADHD such as impaired executive functioning, which may be secondary to neurologic dysfunction (Krain & Castellanos, 2006). These data support and extend findings of poor sustained attention and increased impulsivity among adult hoarders (Grisham et al., 2007) to children, providing preliminary evidence for a developmental pathway through which hoarding may develop. Considering individual domains of hoarding, inattention significantly predicted clutter, hyperactivity/impulsivity significantly predicted acquisition, and combined symptoms (inattention and hyperactivity/impulsivity) significantly predicted difficulty discarding, hoarding-related distress, and greater overall hoarding symptoms. One way to understand the relationship between hoarding and ADHD symptoms is through the functional deficits associated with ADHD symptoms. Children with ADHD often have severe impairment with organization, project initiation and long-term planning, sustained attention, and working memory due to executive function deficits (Barkley, 1997). It may be that children with ADHD are more likely to excessively acquire through impulse, yet due to executive function deficits are unable to adequately organize their environment and/or discard unneeded items leading to an excessive accumulation of clutter. The associations between hoarding and ADHD suggest the possibility of shared etiology in executive function and visual–spatial memory deficits and neurocircuitry (e.g., basil ganglia dysfunction), and may also indicate a potential pathway in which hoarding is maintained. Throughout development, the ADHD symptoms of hyperactivity/impulsivity tend to lessen, whereas executive function deficits appear to persist through adulthood (Biederman, Mick, & Faraone, 2000; Starvo, Ettenhofer, & Nigg, 2007). It may be that hoarding among children with ADHD is initially secondary to ADHD symptoms, yet over time, hoarding behavior and associated cognitive patterns are formed, which maintains future hoarding. In other words, children with ADHD-related hoarding may initially impulsively acquire objects, and then subsequently form strong emotional attachments once the object becomes “theirs.” Furthermore, as cognitive capacities mature with age, children with ADHD-related hoarding may develop beliefs about the intrinsic value and meaning of hoarded objects (e.g., the item may be needed at a later time) and/or may come to rely on hoarding as a strategy, albeit problematic, to cope with ADHD-associated impairments (e.g., disorganization, losing things). These emotional and cognitive attachments may then contribute to difficulties with discarding possessions in a similar pattern as noted with adults (Grisham et al., 2009).
Results from mediational analyses suggested that ADHD-combined symptoms may contribute to increased hoarding behaviors, which in turn are associated with increased disruptive behavior. One reason for this may be that parents impose limitations on a child’s surroundings and tidiness, requiring children to clean and maintain the organization of their own living spaces and bedrooms. Children who are unable to meet parents’ requests (e.g., may not be capable of organizing, sorting, or determining importance of items to keep vs. discard without specified instruction) may respond with disruptive behavior and/or distress. Some children may also be emotionally connected with their collected possessions resulting in an unwillingness to discard items and/or distress when parents enforce limitations (Frost & Gross, 1993; Frost & Hartl, 1996; Grisham et al., 2009). Perhaps this is an early reflection or origin of resistance for help seen in many adults who hoard (Steketee & Frost, 2003).
This study is not without limitations. First, we did not include clinician-rated measures for hoarding, symptom severity, diagnostic status, and neuropsychological functioning, which would allow for a more comprehensive examination of hoarding phenomenology in those with ADHD. We highlight the inclusion of these assays in future research. It is important to delineate that this study examines hoarding behavior, not hoarding disorders, among children with ADHD. Although 29% of this sample presented with significant hoarding tendencies, this is not synonymous with having a hoarding disorder, possibly due to parents executing more control over their child’s environment and not allowing their children to impulsively acquire or save possessions. Second, we only assessed child-report of obsessive-compulsive symptoms and internalizing symptoms. Children may have under- or overreported symptoms. Future research using multiple informants of symptoms and impairment is highlighted. Finally, the current sample consisted of primarily Caucasian participants; it is unclear how our findings generalize to other populations.
These data have important clinical implications. First, given the prevalence and positive relationships between hoarding and ADHD symptoms, these data may provide insight into the etiology of hoarding behaviors. Our data offer support for the information-processing deficit theory in hoarding as well as the suggestion that hoarding may prospectively emerge in childhood in association with executive function deficits. It is possible that the association observed between hoarding features and ADHD symptoms may be indicative of shared neurologic dysfunction (e.g., basil ganglia, frontal cortex; Krain & Castellanos, 2006; Mataix-Cols et al., 2004) common to each condition. Second, our findings provide a foundation for understanding the extent to which hoarding is a problematic behavior for children with ADHD and their families and in turn, inform assessment and potential treatment planning. These data preliminarily suggest that children with ADHD-related hoarding exhibit a unique clinical profile with worsened ADHD symptoms and disruptiveness relative to children with ADHD without hoarding; it is unclear if those who hoard experience different clinical outcomes. Treatment of hoarding has remained notoriously difficult. The only treatment interventions that have been empirically studied in hoarding have been serotonin reuptake inhibitor medications and cognitive behavioral therapy (CBT; Tolin, 2011). Unfortunately, these methods of treatment have seen poor to modest response rates, with pretreatment inattentive symptoms corresponding with reduced CBT adherence (Steketee, Frost, Tolin, Rasmussen, & Brown, 2010; Tolin, Frost, & Steketee, 2007). More recently, psychosocial treatment approaches that consider the clinical characteristics of those who hoard have yielded more positive, but still modest, outcomes (Muroff, Steketee, Bratiotis, & Ross, 2012; Steketee & Tolin, 2011). It may be that multimodal treatment involving CBT and stimulant medications for those patients who exhibit comorbid ADHD symptoms yields improved treatment outcomes, which is something that may warrant further investigation. Importantly, it remains unclear whether successful treatment during childhood of ADHD symptoms may result in reduced hoarding behavior concurrently, as well as improved prognosis in this domain over time. It may be that as treatment is discontinued as the youth enters adulthood, hoarding behaviors increase in the absence of external controls (e.g., parents). Nonetheless, in a patient population that experiences considerable disability, early intervention among youth who hoard may provide an opportunity to alter the illness trajectory prior to the symptom presentation being ingrained.
Footnotes
Acknowledgements
The contributions of Barbara Bradbury-Feinberg, Angela Celis, Shawn Alderman, Amanda Keene, Shannon Schroeder, and Diana Barrera are gratefully acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Kiara R. Timpano, PhD, is an Assistant Professor at the University of Miami. Her clinical and research interest include anxiety and obsessive compulsive disorders. Dr. Timpano leads the clinical research program, Program for Anxiety, Stress, and OCD, at the University of Miami.