
Abstract
Keywords
ADHD is one of the more common childhood syndromes: It accounts for almost half of all pediatric referrals of children to health services in the United States (Glicken, 1997; Goldman, Genel, Bezman, & Slanetz, 1998). The most conspicuous difficulties of patients with ADHD are lack of attention, hyperactivity, and impulsivity (Diagnostic and Statistical Manual of Mental Disorders, 4th ed., text rev. [DSM-IV-TR]; American Psychiatric Association [APA], 2000). Still, many other difficulties are associated with the syndrome, which makes it difficult to diagnose and treat children, adolescents, and adults with ADHD. Among the wide variety of factors seen in children and adolescents with ADHD are oppositional and aggressive behaviors, anxiety, depression, difficulties in parent–child relations, lack of social skills, low self-ratings, and being underachievers in academic skills (Anastopoulos, 2000; MTA Cooperative Group, 1999a, 1999b). Sleep and sensory processing functions have been researched less than other functions; they are the topic of the present research.
Sensory modulation is a very important adaptive functioning used by humans to function in the ever-changing physical environment. It affects the quality of our life and our physical adaptation to our surroundings (Bar-Shalita, Seltzer, Vatine, Yochman, & Parush, 2009). Miller, McIntosh, and McGrath-Clarke (2001) defined sensory modulation as “. . . the capacity to regulate and organize the degree, intensity, and nature of responses to sensory input in a graded and adaptive manner, so that an optimal range of performance and adaptation to challenges can be maintained” (p. 400). Sensory modulation has various neural, behavioral, and emotional aspects. It can be evaluated in various ways through physiological means, by measures such as hearing- and vision-evoked response potentials, and electrodermal reactions (Miller et al., 2001); by subjective measures of reports filled out by parents or the person himself or herself (using the Sensory Responsiveness Questionnaire, Bar-Shalita et al., 2009; Short Sensory Profile, McIntosh, Miller, Shyu, & Dunn, 1999); and by direct observation (using the Sensory Integration and Praxis Tests, Ayres, 1989).
In recent years, various aspects of sensory modulation among patients with ADHD have been explored. It has been found that many children with ADHD also have sensory processing disorders (Cermak, 1991; Miller et al., 2001; Parush, Shomer, Steinberg, & Kaitz, 1997). During childhood, children with ADHD reported more sensitivity to sensory stimuli and being easily upset by environmental changes in infancy (Kaplan, Sadock, & Grebb, 1994). More specifically, Parush et al. (1997; Parush, Shomer, Steinberg, & Kaitz, 2007) reported that children with ADHD had higher amplitudes of somatosensory-evoked potentials, whereas behavioral manifestation of impaired sensory modulation was related to somatosensory deficiencies. The reason for this ineffective functioning was inadequate filtering of tactile stimuli characterized by hypersensitivity and other aversive reactions to tactile sensations. Yochhman, Ornoy and Parush (2006) and Dunn (1994) found differences in measures of sensory processing and modulation with emotional and behavioral responses. Others, including Miller et al. (2001), used physiological measures and parental reports; they found greater abnormalities in sensory modulation and high variability in sensory responses among children with ADHD. An additional finding of this study indicated that sensory modulation measures correlated highly with measures of psychopathology. Yochman, Ornoy, and Parush (2006) found that preschool children with symptoms of ADHD were lower than a control group in measures of fine motor, gross motor, visuomotor, and oral motor functioning. These results confirmed the researchers’ assumptions that children with ADHD have perceptuomotor deficits; they recommended early assessment and treatment for these children.
Difficulties replicating some of the above-mentioned results (Barkley, 1998; Rosenthal & Allen, 1978) initiated the idea that children with ADHD are not a homogeneous group in their autonomic nervous system reactions (Miller et al., 2001); this finding might serve as a partial explanation for the difficulties in replicating results of studies with sensory modalities among the population with ADHD.
During adolescence, various neurological, physiological, and behavioral changes take place; one of these is sleep. These changes include later sleep phases resulting in a preference for later bedtimes and later waking-up times, lack of sleep, and longer sleep time during the weekends as compared with sleep time during the weekdays (Carskadon, Acebo, & Jenni, 2005; Carskadon, Vieira, & Acebo, 1993; Carskadon, Wolfson, Acebo, Tzischinsky, & Seifer, 1998; Crowley, Acebo, & Carskadon, 2007). These changes have a greater impact on the functioning of children and adolescents with ADHD, although the etiology is not clear (Weiss & Salpekar, 2010).
According to the parents’ reports, 25% to 50% of the children with ADHD have sleeping problems (Corkum, Tannock, & Moldofsky, 1998). One cross-sectional survey reported such problems among 73.3% of children with mild to severe ADHD (Sung, Hiscock, Sciberras, & Efron, 2008). However, more typically, it is around 50% (Bullock & Schall, 2005; Cohen-Zion & Ancoli-Israel, 2004; Owens, 2005). The older version of the Diagnostic and Statistical Manual of Mental Disorders (the DSM-III; APA, 1980) included a diagnostic criterion for ADHD: restless sleep. In more recent versions of the DSM, this criterion was omitted, probably due to the feeling that further research was needed to strengthen the association between ADHD and sleep difficulties (Weiss & Salpekar, 2010). Various studies showed that sleep problems prevalent among children with ADHD include delayed sleep onset, difficulty maintaining sleep, tiredness on waking, frequent nocturnal awakenings or restlessness, and daytime sleepiness (Lecendreux & Cortese, 2007; Owens, 2005; Owens et al., 2009; Sung et al., 2008; Van der Heijden, Smits, & Gunning, 2005). Objective studies, using electronic measures of actigraphy and polysomnography, assessed mainly the sleep architecture, sleep quantity, and quality. Studies using these techniques found the following sleep problems in children with ADHD: a reduced length of rapid eye movement stage, increased sleep latency, decreased overall sleep time, increased nocturnal activity, increased movement time, increased waking after the sleep onset, and reduced sleep efficiency (Bullock & Schall, 2005; Goraya et al., 2009; Kirov, Banaschewiski, Uebel, Kinkelbur, & Rothenberger, 2007; Owens, Sangal & Sutton, 2009; Tirosh, Sadeh, Munvez, & Lavie, 1993). Other sleep problems seemed to be less prevalent among children with ADHD. Still, problems were identified among children with ADHD in sleep-related breathing disorders (Chervin et al., 2002) and periodic limb movement disorder (Cortese et al., 2005; Crabtree, Ivanenko, O’Brien, & Gozal, 2003; Van der Heijden et al., 2005). Owens (2005) concluded her study by saying that ADHD and sleep disturbances show a complex bidirectional relation while each element, sleep or ADHD, can exacerbate or be exacerbated by the symptoms of the other.
Regardless of the vast research dealing with ADHD and the numerous reports about sensory modulation and sleep, not much has been done in an attempt to understand the relationships between these behavioral aspects among children with ADHD. It was, however, carried out in one research project (Shochat, Tzischinsky, & Engel-Yeger, 2009) involving children without ADHD. The purpose of the present study is to bridge the gap by combining the modalities of senses and aspects of sleep among children diagnosed as having ADHD. It was hypothesized that the research group of children with ADHD would exhibit more problems in sensory modulation. The second hypothesis was that children with ADHD would present more sleep problems as compared with a control group. No hypothesis was set for the combination of sensory and sleeping difficulties, with the hope that the results would give an answer to this interesting question.
The ethical standards of our college were followed in the conduct of the present study.
Method
Participants
A total of 58 adolescents, ages 13 to 17, participated in the study. In all, 30 of them (27 males and 3 females, M age = 15.10, SD = 1.27) who were diagnosed as having ADHD served as the research group. They were compared with 28 adolescents (14 males and 14 females, M age = 15.64, SD = 1.50) who had no ADHD or learning disabilities and were used as a control group. All the participants lived in Northern Israel in small- and medium-sized communities of fewer than 50,000 inhabitants and attended regular middle schools and high schools. The participants in the research group were diagnosed as having ADHD (a combined type, as predominantly inattentive, or as predominantly hyperactive/impulsive) by psychiatrists or clinical psychologists before the study. The possibility of comorbid diagnoses in this group was not evaluated systematically. All the participants ingested medications to treat their inattention in the past or the present (Ritalin, Slow-Release (SR) Ritalin, or Concerta). A total of 90% of them were taking medication while they participated in the study.
Instruments
Two questionnaires were administered to the parents to verify the diagnosis of ADHD and two different questionnaires were administered to the adolescents to assess their sleeping habits and sensory measures. The questionnaires for the parents were as follows:
Conners’ Parent Rating Scale–Revised Long Form (CPRS-R:L; Conners, 1998). This contains 80 items with 14 subscales. The questionnaire’s subscales were created by using a factor analysis of large sets of items and are based on the DSM-IV criteria for diagnosing ADHD (APA, 1994). Test–retest reliability of the various subscales during the construction of the questionnaire showed correlations of .47 to .85. In the present study, Cronbach’s alpha reliability of the scale was .97.
The DSM-IV Questionnaire (Robin, 1995). This is a short scale of 18 items derived from the 18 symptoms for diagnosing ADHD (9 symptoms for inattention and 9 symptoms for hyperactivity/impulsivity). In the present study, the Cronbach’s alpha reliability of the scale was .94.
Questionnaires to the participants were as follows:
3. Adolescents Sensory Profile (Brown & Dunn, 2002). This is a self-rating questionnaire containing 60 items, answered on a 5-point Likert-type scale (from 1 corresponding to almost never to 5 corresponding to almost always). The items are divided into the following six sensory modalities: Taste/Smell, Movement, Vision, Touch, Level of Activity, and Hearing. In addition, each item pertains to one of the following four general sensory modalities, named quadrant, reflecting the following four different sensory processing patterns: Low Registration, Sensation Seeking, Sensory Sensitivity, and Sensation Avoiding. Internal consistency, alpha, of the four quadrants reported in the manual to range from .64 to .70. In the present study, the Cronbach’s alpha reliability of the scale was .80.
4. Sleep Schedules (Wolfson & Carskadon, 1998). This questionnaire is a self-rating questionnaire with 38 items assessing various sleep habits. The questionnaire was translated and adapted for the Israeli population with Cronbach’s alpha reliability of .67 to .79 for the various measures (Shochat, Flint-Bretler, & Tzischinsky, 2010). The questionnaire is a Likert-type scale with four options, while it has questions on various aspects of sleep during the week and during weekends. The items of the questionnaire are aggregated into the following three measures: Sleepiness, Sleep Behavior, and Mood. In the present study, the Cronbach’s alpha reliability of the scale was .78.
Procedure
The adolescents diagnosed as having ADHD were recruited from several middle and high schools in Northern Israel with the help of the school counselors. The control group participants were recruited from the same schools at the same time. The questionnaires were given to the participants and their parents by each child’s teacher. Collecting the completed questionnaires was controlled by the teacher.
Results
A comparison of the ages of the two groups showed no significant differences between the mean age of the two groups (the mean age for the research group was 15.10, whereas the mean age for the control group was 15.64,
The results of the CPRS-R:L (Conners, 1998) administered to the parents showed that in 11 of the 14 subscales, the research group scored significantly higher, indicating more behavioral problems associated with ADHD.
The results of the second questionnaire administered to the parents, the DSM-IV Questionnaire (Robin, 1995), showed that in the inattention and combined score (including inattention and hyperactivity/impulsivity), the research group scored significantly higher than the control group. No significant differences between the two groups were found in the measure of hyperactivity/impulsivity. These results indicated higher more ADHD symptoms in the research group as compared with the control group. The results of the two questionnaires administered to the parents can be seen in Table 1.
Means, Standard Deviations, and T-Scores of All the Participants of the CTRS-R:L (Conners, 1998) and the DSM-IV Questionnaire (Robin, 1995).
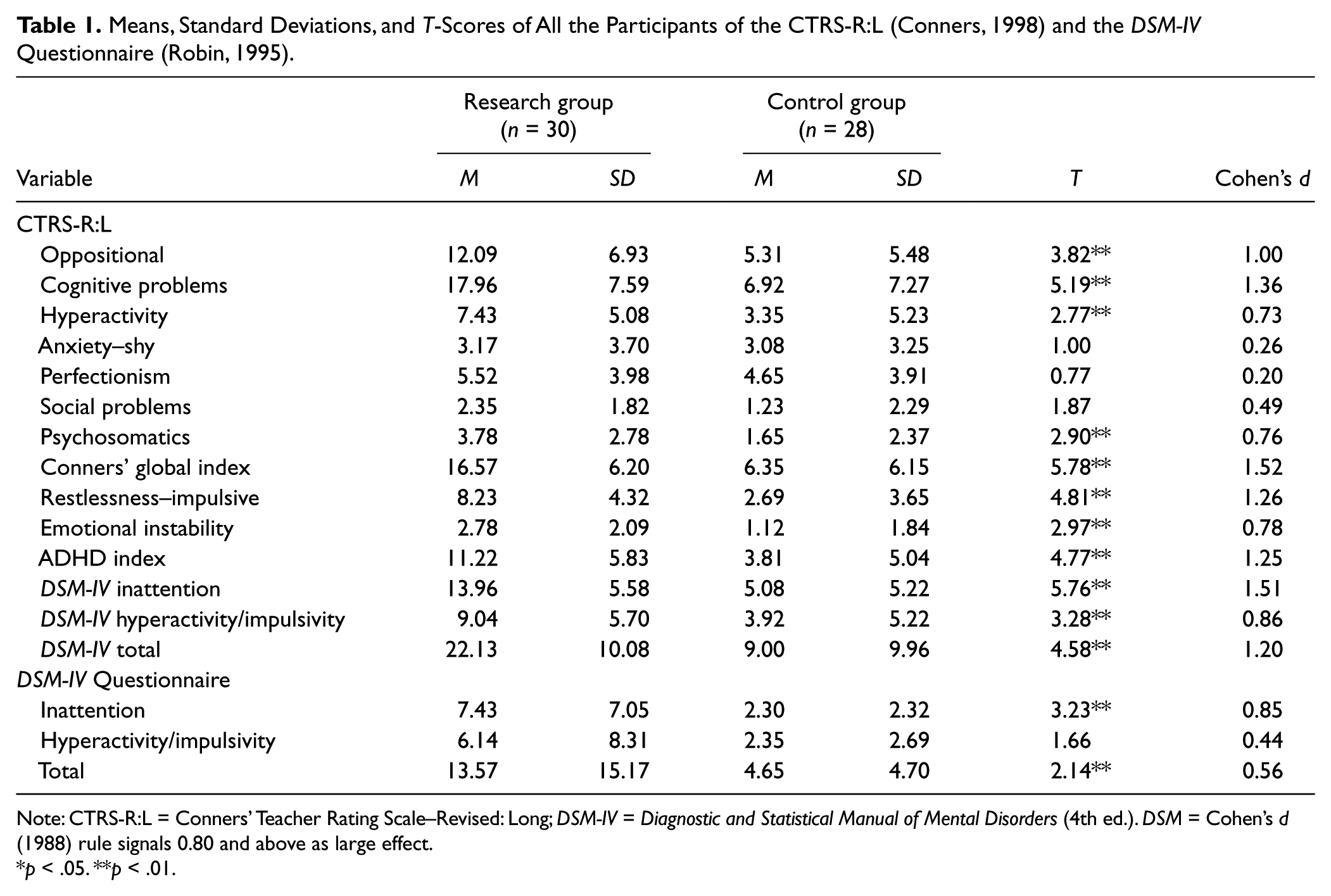
Note: CTRS-R:L = Conners’ Teacher Rating Scale–Revised: Long; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.). DSM = Cohen’s d (1988) rule signals 0.80 and above as large effect.
p < .05. **p < .01.
The results of the Adolescents Sensory Profile (Brown & Dunn, 2002) showed that in three sensory modalities, the research group had experienced more difficulties. In the Level of Activity (for the research group, M = 17.73, SD = 3.57, and for the control group, M = 15.07, SD = 3.68,
The results of the Sleep Schedules (Wolfson & Carskadon, 1998) showed that in one measure, Sleep Behavior, the research group scored higher indicating more problems in this variable (for the research group, M = 38.53, SD = 9.99, and for the control group, M = 33.35, SD = 6.49,
Means, Standard Deviations and T-Scores of All the Participants of the Sensory Profile (Brown & Dunn, 2002) and the Sleep Schedules (Wolfson & Carskadon, 1998).
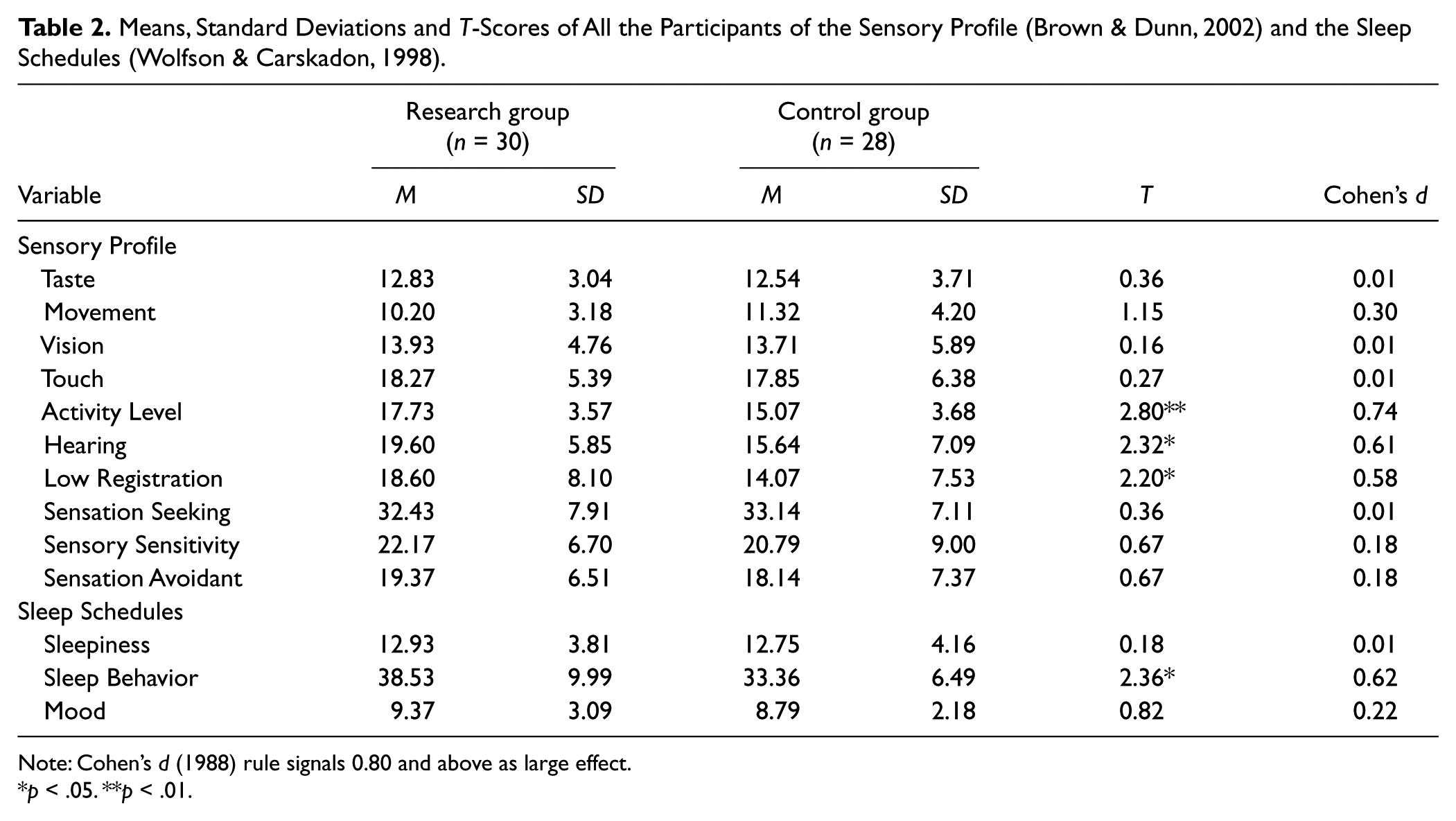
Note: Cohen’s d (1988) rule signals 0.80 and above as large effect.
p < .05. **p < .01.
Within the specific items of the Sleep Behavior, the research group scored significantly higher in Item 25j: “I need to be awakened more than once by someone in the morning,” Item 25k: “It takes me a long time to fall asleep,” and Item 25n: “I perform dangerous activities without thinking.”
Trying to understand the relationships between sensory measures and sleep variables between the two groups, a correlation between the variables for each group separately was calculated. The correlations between the sensory measures and the sleep variables were much higher in the research group as compared with the control group. There were 12 significant correlations between the variables in the research group as compared with only 1 significant correlation between the variables in the control group. Five comparisons of the correlations showed significant differences between correlations of the variables of the research group as compared with the control group. These correlations are shown in Table 3.
Correlations Between Sensory Profile (Brown & Dunn, 2002) and the Sleep Schedules (Wolfson & Carskadon, 1998) in the Research Group (n = 30) and the Control Group (n = 28).
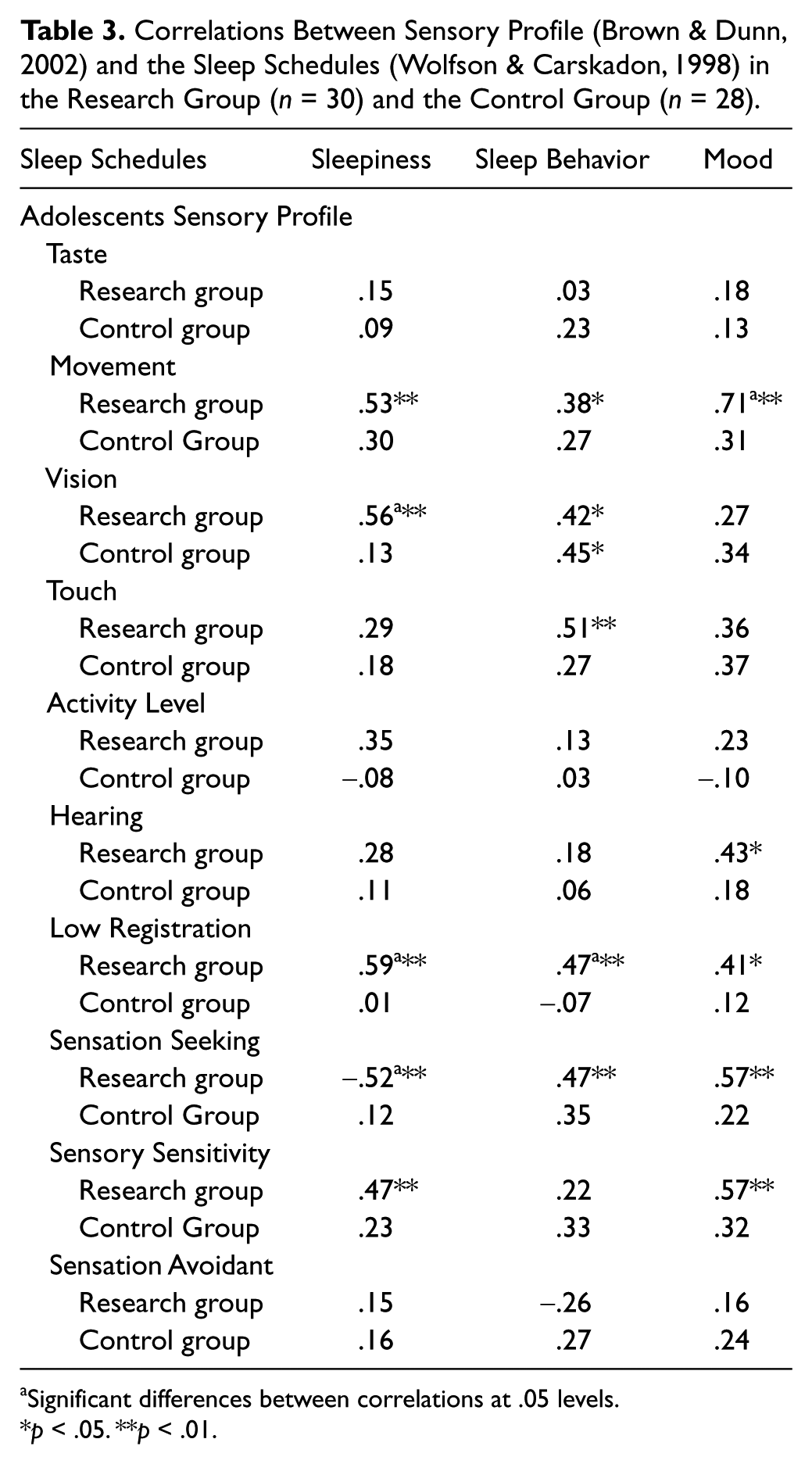
Significant differences between correlations at .05 levels.
p < .05. **p < .01.
Discussion
The study was aimed at assessing sensory modalities and sleep variables, and how different they are in adolescents with ADHD as compared with adolescents without ADHD. The results of the CPRS-R:L (Conners, 1998) and the DSM-IV Questionnaire (Robin, 1995) confirmed that the classification of the research group and the control group was appropriate. Significant differences in many of the variables assessing ADHD between groups showed that the diagnosis of the participants, as a group, prior to the beginning of the study was accurate.
Assessing the sensory scale showed that in 3 of the 10 sensory measures, there were significant differences: Level of Activity, Hearing, and Low Registration. These measures are problems usually seen as difficulties among children with ADHD. Level of Activity is closely associated with hyperactivity, whereas Hearing may be associated with a lack of attention or being distracted and not hearing difficulties per se. The third sensory variable was a high score on the quadrant of Low Registration. This variable refers to individuals who are oversensitive and overactive, who seek for rich sensations. Dunn (2001) indicated that the sensory processing patterns might be related to biologic or genetic factors, although it is believed to be a biosocial phenomenon. No differences were found in the other sensory measures: Taste/Smell, Movement, Vision, Touch, and three quadrants of Sensation Seeking, Sensory Sensitivity, and Sensation Avoiding. This shows that these sensory modalities are not major difficulties among adolescents with ADHD; the difficulties are found only in those functions closely associated with the major symptoms of ADHD, as described above.
Trying to evaluate the results of the sleep questionnaire, one looks at the significant differences between the two groups of Sleep Behavior, which includes 15 different measures relating to behaviors of staying awake during the day, difficulties falling asleep, staying asleep, and difficulties in waking up. Among these, the more conspicuous items were those indicating difficulties in falling asleep, difficulties in waking up, and doing dangerous activities without thinking. These difficulties belong to a wide spectrum of Sleep Behavior. Difficulties in sleep in the population with ADHD has been documented in the past extensively in various studies (among these are Bullock & Schall, 2005; Cohen-Zion & Ancoli-Israel, 2004; Corkum et al., 1998; Owens, 2005; Sung et al., 2008). Our findings confirmed these previous reports.
Assessing the correlations between measures of sensory modalities and sleep measures showed that there are much higher correlations between these variables among the population with ADHD. These findings indicated that the appearance of a problem in one area (sensory modalities or sleep measures) is a predictor of the appearance of problems in another area (sensory modalities or sleep measures). This was true only in the research group, that is, the children with ADHD. These findings were strengthened by the fact that in four measures, there were significant differences between the correlations of the sensory modalities and the sleep measures (Movement, Vision, Low Registration, and Seeking Sensation). There is a need to understand which difficulty, either sensory modalities or sleep, is more prominent in its influence on the ADHD symptoms. Our study does not give an answer to this question. On this point, however, a partial answer can be found in the conclusion of Shochat et al. (2009) who concluded their study with a “normal” community sample by saying, “We conclude that the relationships found in the present preliminary study between sensory modulation, sleep, and behavior suggests that sensory modulation dysfunction may be a contributing factor for nighttime insomnia and daytime behavioral disturbances in school-aged children” (p. 60). However, the question regarding which variable contributes more to ADHD remains unanswered.
The results of the present study join results in other areas leading to a better understanding of the ADHD syndrome. Various studies (including Pennington, 1991) have reported that ADHD is not a distinct syndrome. Almost half of the children with ADHD indicate comorbidity when they are also diagnosed as having another psychological or behavioral disorder (Tannock, 1998). Taking into consideration our findings requires those who diagnose ADHD to expand the diagnostic procedure of ADHD and to assess sensory modalities, sleep problems. It is possible that a better treatment for ADHD should include treating these other behavioral problems. Such a strategy may reduce the ADHD symptoms or may bring those who suffer from the problem to a normal functioning.
A limitation of the study was the use of questionnaires as the only measure of sensory modalities and sleep measures. Adding objective procedures such as those evoking response potentials and/or electrodermal responses for sensory aspects and an actigraph or polysomnograph for sleep measures may add another dimension to the results. Using more participants with different subgroups of the ADHD (combined type, hyperactivity/impulsivity type, and inattention type) can shed more light on the topic.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.