
Abstract
Introduction
In the national debate regarding health care reform, physician-level differences in treatment practices are often cited as an indication of inappropriate care (Wennberg, 2002). In recent decades, prescription of stimulants for the treatment of ADHD has risen rapidly in the United States (Olfson, Gameroff, Marcus, & Jensen, 2003) with the prevalence of stimulant prescriptions in pediatric populations exceeding 4% (Cox, Motheral, Henderson, & Mager, 2003; Visser, Lesesne, & Perou, 2007). Although physicians overwhelmingly appear to agree that ADHD symptoms cause problems for their pediatric patients and that stimulants are an effective treatment (Stockl, Hughes, Jarrar, Secnik, & Perwien, 2003), significant variations in prescription rates have been documented. For example, regional differences have been widely noted, with higher use of stimulant medications in the South and parts of the Midwest, with additional significant variation at the county level (Cox et al., 2003; Hoagwood, Jensen, Feil, Vitiello, & Bhatara, 2000; Stevens, Harman, & Kelleher, 2004). Patient characteristics, such as Caucasian race and health insurance coverage, only partially explain these differences (Cox et al., 2003; Hoagwood et al., 2000; Olfson et al., 2003; Stevens et al., 2004).
Two types of physicians prescribe the vast majority of stimulant medications in the United States: pediatricians and psychiatrists. Primary care pediatricians have been found to differ in their management and treatment of ADHD. In general, pediatricians vary in their identification of psychosocial problems among their patients (Vogels et al., 2008; Wasserman et al., 1999), their reliance on practice guidelines for ADHD (Rushton, Fant, & Clark, 2004; Wolraich, Bard, Stein, Rushton, & O’Connor, 2010), and their stimulant prescription rates (Gardner et al., 2000). However, little is known about physician characteristics that are associated with these differences. In the identification of psychosocial problems, Wissow and others found that aspects of physicians’ interview styles may be predictive, such as attentive listening, frequency of supportive statements, and lack of avoidant responses (Wissow, Larson, Anderson, & Hadjisky, 2005; Wissow, Roter, & Wilson, 1994). To understand variation in prescription rates, Gardner and others found no evidence of effects of pediatricians’ training, beliefs about mental health, or practice structure, but did confirm that parental agreement with the treatment plan and a history of recognition of a psychosocial problem led to more prescriptions (Gardner et al., 2000).
In comparison with primary care pediatricians, child and adolescent psychiatrists are more likely to treat children with multiple comorbid conditions (Harpaz-Rotem & Rosenheck, 2006), prescribe medication in any given visit (Goodwin, Gould, Blanco, & Olfson, 2001; Thomas, Conrad, Casler, & Goodman, 2006), and use multiple medications. Nevertheless, because pediatricians far outnumber child and adolescent psychiatrists in the United States, pediatricians provide the majority of stimulant medication prescriptions (Beardsley, Gardocki, Larson, & Hidalgo, 1988; Goodwin et al., 2001). Although psychiatrists differ in their attitudes regarding the risks and benefits of antipsychotic (Newcomer, Nasrallah, & Loebel, 2004; Patel, Nikolaou, & David, 2003) and stimulant medication (Beck, Silverstone, Glor, & Dunn, 1999), little is known about differences in their prescribing patterns.
In this study, we describe a novel use of a standard method of preference elicitation to explain provider-level differences in willingness to prescribe ADHD medications. The standard gamble is a technique for eliciting “utilities,” a patient-centered measure of health-related quality of life (HRQL) based on patients’ and/or providers’ preferences for medical outcomes associated with a disorder (Zimmerman, 2003). Utilities are typically indexed on a standard 0 (dead) to 1 (perfect health) scale and are directly comparable across different health conditions. Large-scale studies have been conducted that use the standard gamble to elicit patient preferences regarding pediatric outcomes (Carroll & Downs, 2009; Matza et al., 2005), primarily for use in decisions about allocation of health care resources (Zimmerman, 2003).
While utilities have typically been used to assess an individual’s or a specific population’s preference for one health state over another, in this study, we assess physicians’ utilities for ADHD health states of differing degrees of severity and investigate the association between these utilities and physicians’ self-reported prescribing practices. Physicians’ responses to standard gambles have been found to predict a number of provider-level variations, including physicians’ decisions to hospitalize patients (Nightingale, 1988), their recommendations regarding medical procedures (Nightingale & Grant, 1988), and their use of medical tests (Nightingale, 1987; Zaat & van Eijk, 1992), but have not previously been used to examine pediatric medication treatment decisions. Reporting a lower utility value for a given ADHD health state reflects a physician’s belief that children who have this health state will, on average, experience lower HRQL. We operationalize this to mean that lower utilities reflect the belief that ADHD is a serious disorder—one that may be more likely to require a treatment intervention. We hypothesized that believing that ADHD is a more serious disorder relative to colleagues will increase the likelihood that a physician will emphasize the benefits of treating ADHD symptoms over the risks of medication side effects. Below, we report the results of a two-part survey in which we tested these hypotheses.
Method
Participants and procedures
For the initial survey about practice patterns (hereafter, “initial survey”), 1,600 psychiatrists were randomly selected from the American Academy of Child and Adolescent Psychiatry membership of over 7,500 (Leslie et al., in press), and 1,600 pediatricians were randomly selected from the American Academy of Pediatrics membership of over 65,000 (Leslie et al., 2012). Retirees, trainees, fellows, and non-U.S.-based physicians were excluded. Eligibility criteria included providing direct patient care to children aged 5 to 18 years with ADHD. Among these, 1,140 (36%) responded and were eligible for the initial survey, which ended with a request to participate in a follow-up survey of provider preferences (hereafter, “preference survey”). Following the institutional review board approval, the 291 (26%) respondents who volunteered to participate in the preference survey were mailed two rounds of surveys (at 3-week intervals) between May and June 2011. In all, 127 physicians (44%) responded to the preference survey.
Measures
The preference survey consisted of standard gamble exercises for four separate health states. Respondents were asked to read a vignette that describes a given health state in detail. They were then asked to choose between that health state for certain or to take a gamble between perfect health or death. For example, respondents might be asked to consider a state of metastatic liver cancer. They are then asked whether they would prefer to have metastatic liver cancer or to take a magic pill that offers a 75% chance of returning them to perfect heath, but with a 25% chance of immediate, painless death. The probabilities in the gamble are systematically altered until each respondent’s threshold is found, and the HRQL for metastatic cancer then equals the chance of returning to perfect health. For health states perceived to be more serious than others, respondents should be willing to accept higher levels of risk for the chance to obtain perfect health. The standard gamble has been used in pediatrics and other fields to assess the utility of a variety of health states (Carroll & Downs, 2009; Zimmerman, 2003), usually for measuring either societal or parental utilities for different screening and/or diagnostic tests or treatments.
In particular, we used a version known as the Paper-Standard Gamble (P-SG) as a feasible, cost-effective way to conduct standard gamble assessments. To ease respondent burden, the P-SG systematically alters risk of death from low to high over a series of 18 yes/no questions, each presenting a different gamble with a different balance between the probability of cure and death. For example, the first item asks whether the respondent would recommend living in the health state described in the vignette or wearing a magic skin patch if they knew “it had a 100% chance of cure and 0% risk of causing death in your patient’s sleep tonight?” The next question alters these probabilities by asking whether respondents would recommend a patch if they knew “it had a 99.9999% chance of cure and a 1 in 1 million (0.0001%) risk of causing death in your patient’s sleep tonight?” The score on the P-SG is equivalent to the lowest probability of cure endorsed by the respondent, as indicated by a “yes” response. Because there are 18 questions, 18 different scores on the P-SG are possible. The P-SG has demonstrated good retest reliability and concurrent validity, evidenced by strong correlations with assessments of HRQL and close approximation of the results of a standard gamble conducted by computer using interval division method questions (Littenberg, Partilo, Licata, & Kattan, 2003; Ross et al., 2003).
In the preference survey, the health states included mild ADHD, moderate ADHD, severe ADHD, and worst-case ADHD. Vignettes describing each ADHD state were directly adopted from an instrument used in a previously published study of parents’ preferences regarding ADHD states (Matza et al., 2005). Data from the preference survey were linked to the initial survey, which included questions about prescribing practices for stimulant medications and attitudes regarding risks of side effects. Questions relevant to this article included respondent demographics and practice setting characteristics, and questions about prescribing practices for stimulant medication.
Independent variables
Eight primary independent variables were identified a priori to be consistent with study hypotheses. Participants used 4-point Likert-type scales, ranging from not at all to a lot, to answer the question, “How much does each of the following factors influence your willingness to initiate treatment with stimulants for a child with ADHD?”: (a) the severity of ADHD symptoms, (b) degree of ADHD impairment, (c) parental concerns about side effects, (d) prescriber attitudes about the benefits of stimulant medications, (e) prescriber concerns about side effects, and (f) prescriber concerns about the variable effectiveness of stimulant medication. Respondents were also asked how much they agreed or disagreed with the following statements, using a 4-point Likert-type scale, ranging from strongly disagree to strongly agree, to answer: (g) “Stimulants represent the best first-line treatment for ADHD in children” and (h) “The risk for sudden cardiac death in children is sufficiently high to warrant cardiac assessment before initiating treatment with stimulants.”
In addition, we analyzed the following potentially confounding respondent demographic and practice characteristics: specialty (psychiatrist or pediatrician), gender, race/ethnicity (non-Hispanic/White vs. others), years in practice (categorized by quartile based on initial survey), practice setting (urban, rural, or suburban), and proportion of patients with private insurance (more than 50% of patients with private insurance vs. not).
Dependent variable
The dependent variable consisted of responses to the P-SG for the four different ADHD health states (mild, moderate, severe, worst case). As described above, the P-SG assesses each health state with 18 separate questions, yielding 18 possible responses. Ordered categories corresponded to the top 7 response options, ranging from a 100% to 99% chance of cure (corresponding to utilities of 1.00 to 0.99), and captured the large majority of participants’ responses, with an eighth category to capture responses below 99%. Because each response on the standard gamble corresponds to a particular utility value, differences on the dependent variable can be interpreted as difference in utility.
Statistical analysis
Stata Version 11 was used for all analyses. Descriptive statistics (M, SD, frequency, percentage) were computed for respondent demographic and practice setting characteristics. To support a subanalysis of two P-SG administration methods unrelated to this manuscript, respondents were randomly assigned to either (a) complete all P-SGs with death as the worst outcome in the gamble or (b) complete the P-SG for mild, moderate, and severe ADHD with “worst-case ADHD” as the worst outcome. The latter approach is often referred to as “chaining,” and it is commonly employed in the medical literature when investigators are concerned that participants may not accept any probability of death to improve HRQL, as may be the case for non-life-threatening conditions, and therefore ask participants to consider gambles between perfect health and a more severe health condition, rather than death (Carroll & Downs, 2009; Matza et al., 2005). Randomization status was controlled for in all analyses. Chained scores were adjusted to be comparable with unchained standard gamble (SG) scores using a standard equation, Uadjusted chained = Pworst case ADHD + (1 − Pworst case ADHD) × Pchained SG. Some responses that were transformed for chaining did not correspond precisely to responses on the P-SG. Chained scores were therefore assigned to the category of the dependent variable corresponding to the closest value.
Bivariate analyses using logistic regression were used to compare demographic and setting characteristics among the following groups: (a) preference survey respondents, (b) physicians who volunteered for the preference survey but did not complete it, and (c) physicians who completed the initial survey but did not volunteer for follow-up.
An ordinal logistic regression model was used to analyze the effects of independent variables on standard gamble responses. Because each physician rated four ADHD health states, the model included four times as many scores as participants. To account for intraclass correlations among responses, robust standard errors were specified (White, 1980; Williams, 2000). We included all responses in a single analysis because it is more parsimonious than conducting separate analyses for each of the four questions, and because it is more consistent with our hypotheses, which did not vary by health state. A dummy variable reflecting randomization status was included to account for chaining of P-SG results.
We used this model to examine whether physicians assigned lower utilities to more severe ADHD health states, that is, the within-participant effect of severity of ADHD health state across questions on utility. Further tests of bivariate associations used the same model, controlling for severity of ADHD health state to improve precision. In this way, we examined the bivariate effects of respondent demographic variables, practice setting characteristics, and responses to questions about prescribing patterns on utility. For each nonbinary independent variable, we tested for nonlinearity using Box–Tidwell tests. Following recommendations of Hosmer and Lemeshow (2000), variables that were significant at the p < .25 level were then included in a final multivariate ordinal logistic regression model.
For each independent variable, we report a regression coefficient. The valence (±) of these scores indicates whether associations are positive (i.e., higher scores on the independent variable are related to a higher ADHD HRQL on the standard gamble) or negative (i.e., higher scores on the independent variable are related to lower ADHD HRQL on the standard gamble). We also summarize key findings using histograms indicating the proportion of scores that fell at or below the overall median outcome category.
We hypothesized that the following variables would be negatively associated with utilities across the four ADHD states (i.e., greater levels of each would be related to lower ADHD HRQL as assessed by the P-SG): effect of ADHD symptoms on willingness to prescribe, effect of ADHD impairment on willingness to prescribe, effect of belief in the benefits of stimulants in treating ADHD on willingness to prescribe, and agreement that stimulants represent the best first-line treatment for ADHD in children. We further hypothesized that the following variables would be positively associated with utilities (i.e., greater level of each would be related to higher ADHD HRQL): effect of parent concerns about stimulant side effects on willingness to prescribe, effect of personal concerns about side effects on willingness to prescribe, and the degree of influence of concerns about variable effectiveness of stimulant medication on willingness to prescribe.
Results
Of the 291 physicians who volunteered for the follow-up survey, 127 (44%) responded. Descriptive data for respondent demographic and practice setting characteristics are presented in Table 1. No differences were found between follow-up survey respondents and nonrespondents, whether or not they had volunteered for the second survey.
Demographic and Practice Setting Characteristics by Response Status.
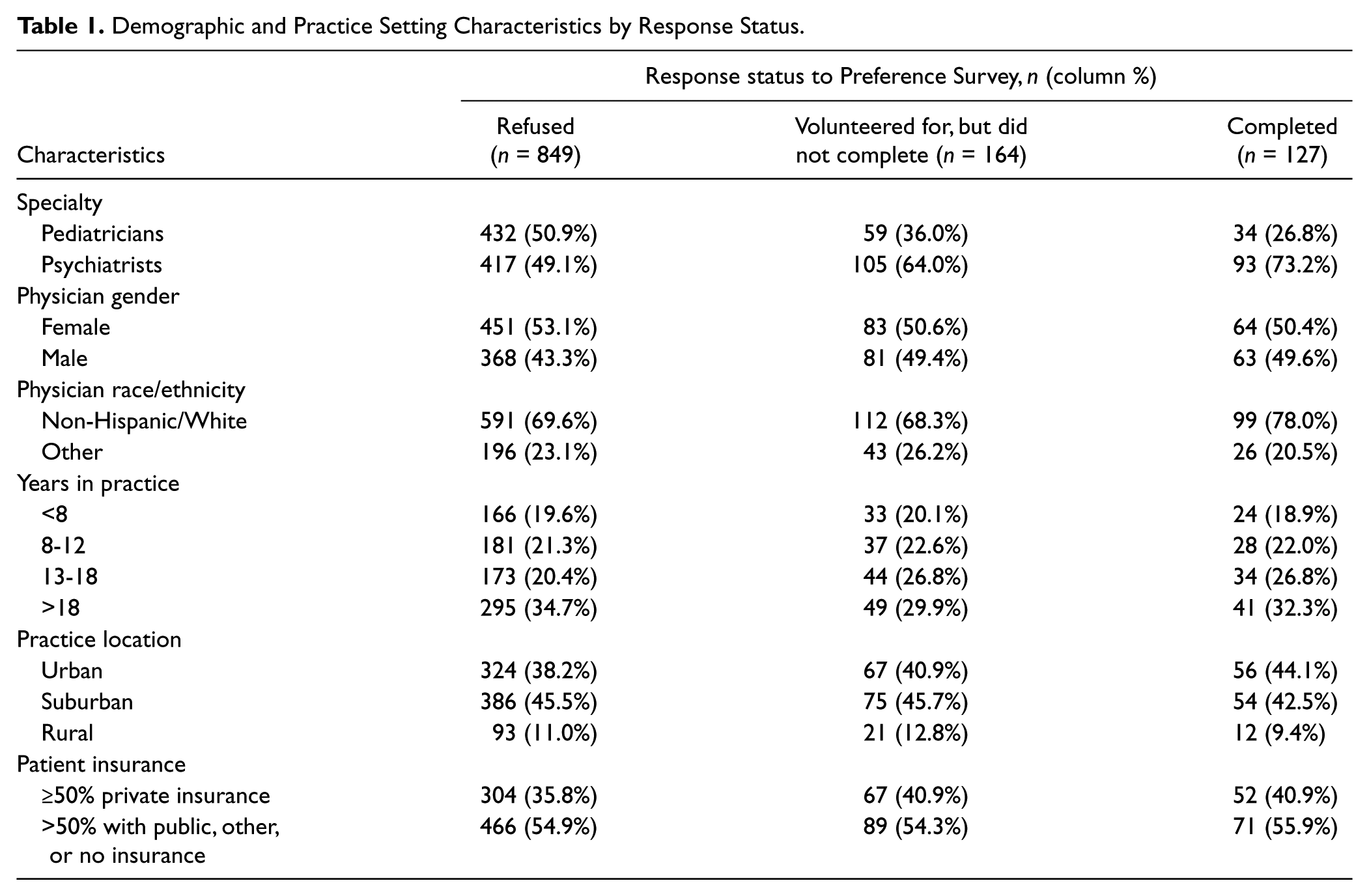
As Table 1 illustrates, 73% of respondents were child and adolescent psychiatrists, and 27% were pediatricians. Approximately half (50%) were female, and slightly more than three quarters (78%) were non-Hispanic/White. The majority of respondents had been practicing at least 13 years. Urban and suburban practice settings were most common (44% and 43%, respectively). Fewer than half (41%) reported serving patient populations among whom at least 50% had private insurance.
Bivariate ordinal regression analyses:
Among demographic and practice setting characteristics, only years-in-practice was significantly associated with utility value (see Table 2), specifically the subcategory of physicians in practice for greater than 18 years.
Nonsignificant effects (p > .25) were found for specialty (psychiatrist or pediatrician), gender, race/ethnicity, practice setting, and proportion of patients with private insurance. All other effects as measured by regression coefficient scores fell in the expected direction except one: Although its regression coefficient was close to zero, the effect of “the benefit of stimulants in treating ADHD” on willingness to prescribe was negative.
Associations Between Standard Gamble Utilities, Initial Survey Questions, and Demographic and Practice Setting Characteristics.
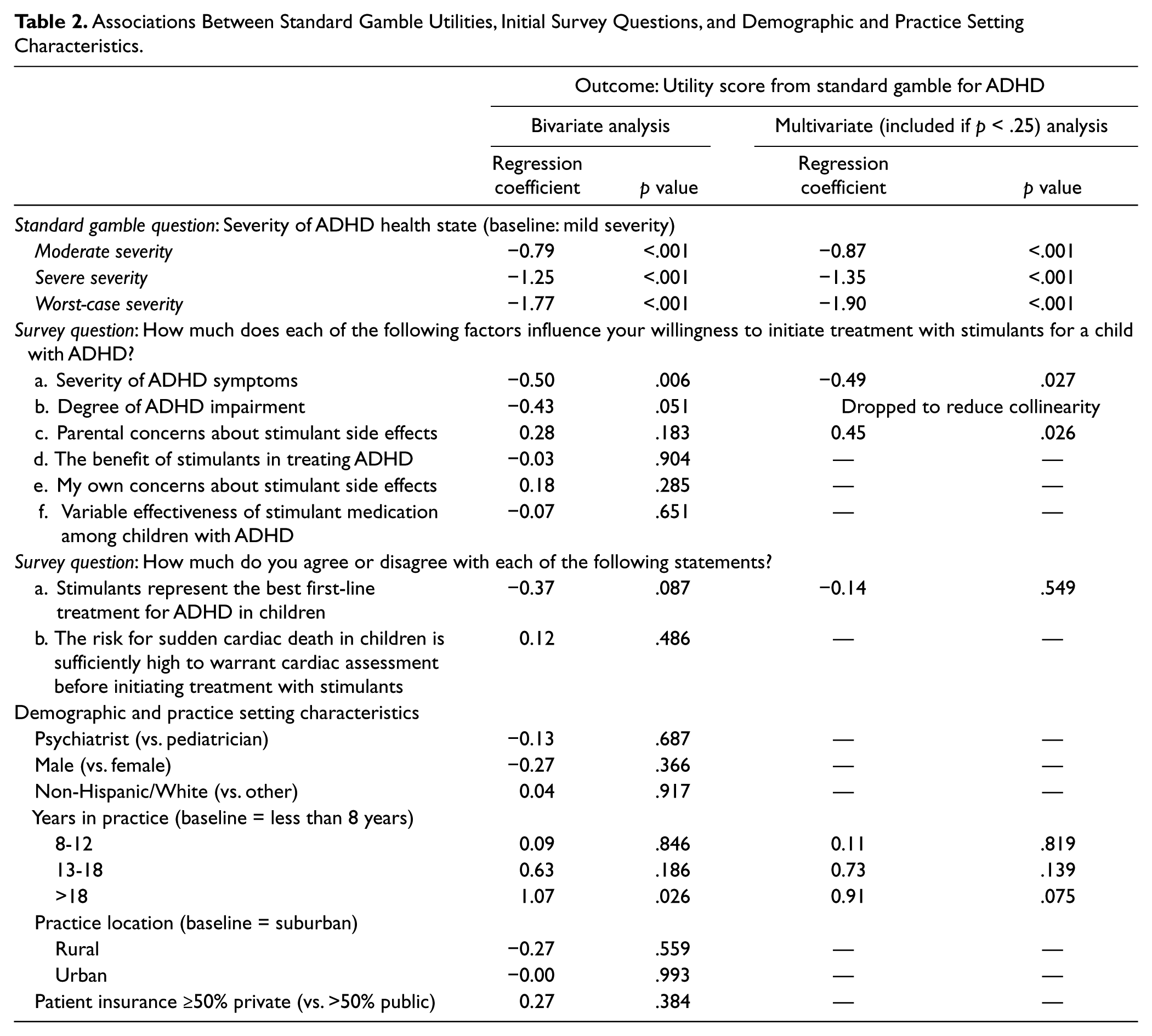
As a group, physicians rated the vignettes that described severe ADHD health states with the lowest utility scores (p < .001). Compared with their colleagues, physicians who assigned lower ADHD HRQL scores on the P-SG were more likely (a) to emphasize ADHD symptoms when prescribing stimulant medications (p < .01), (b) to consider ADHD impairment when prescribing stimulant medications (p = .051), and (c) to agree that stimulants represent the best first-line treatment for ADHD (p = .087). Box–Tidwell tests revealed no evidence of nonlinearity in the relationship between any independent variable and the dependent variable.
Multivariate ordinal regression analysis
Five variables were significant at the p < .25 level in bivariate regression analyses and were considered for the multivariate model (see Table 2). Emphasis on ADHD symptoms when prescribing stimulant medications was highly correlated with emphasis on ADHD impairment (r = .82, p < .05), and the two displayed notable collinearity in the regression model. Therefore, emphasis on ADHD impairment was dropped from the final model.
In this final model, all effects fell in the expected direction, and three were statistically significant (Figure 1). As a group, physicians assigned progressively lower utilities scores to more severe ADHD health state descriptions (p < .001). Compared with their colleagues, physicians who assigned lower ADHD HRQL scores on the P-SG were (a) more likely to emphasize ADHD symptoms when prescribing stimulant medications (regression coefficient = −0.49, p < .05) and (b) less likely to emphasize parental concerns about side effects (regression coefficient = 0.45, p < .05). Note that approximately 80% of physicians reported that they strongly emphasize ADHD symptoms when prescribing. Response frequencies for parental concerns about side effects were more evenly distributed, with the most frequent response being “a moderate amount” at 44%.

Associations between P-SG utility variables from multivariate model. (a) ADHD health state assessed. (b) Effect of “severity of ADHD symptoms” on willingness to prescribe. (c) Effect of “parent concerns about side-effects” on willingness to prescribe.
Discussion
The results of this study are consistent with the hypothesis that physicians’ attitudes regarding the impact of ADHD on HRQL are associated with their prescribing practices. In short, we found that physicians who reported lower utilities for ADHD health states—suggesting that they believe ADHD to have a greater impact on HRQL relative to their colleagues—were more likely to emphasize ADHD symptoms while prescribing stimulant medications and less likely to emphasize parents’ concerns about side effects. These findings are consistent with our hypothesis that believing that ADHD has a significant effect on HRQL relative to colleagues will increase the likelihood that a physician will positively view the trade-off between the benefits of treating ADHD symptoms versus the risks of medication side effects.
Results also highlight the potential use of the standard gamble to measure not only population-level preferences regarding health states but also individual physicians’ differences in preferences toward those health states. Our results suggest that such individual differences in standard gamble utilities may help explain real-world variation among physicians in prescribing patterns for ADHD medications. Similar associations have been demonstrated between standard gamble results and physicians’ decisions to hospitalize patients with medical conditions (Nightingale, 1988), their recommendations regarding medical procedures (Nightingale & Grant, 1988), and their use of medical tests (Nightingale, 1987). We suggest that the standard gamble may function as a method for ascertaining the impact of physician attitudes on prescribing patterns in future research.
Our study has notable strengths. Hypotheses and relevant analyses were specified a priori; thus, these findings are consistent with prior theory. Moreover, in the national debate regarding health care reform, physician-level differences in treatment practices are often cited as an indication of inappropriate care (Wennberg, 2002). Our study suggests that characteristics of individual physicians—namely, their beliefs about the impact of a diagnosis of ADHD on HRQL—affect their determination of what appropriate care entails, including the appropriate balance between considerations of ADHD symptoms and parents’ concerns about side effects. Thus, physician training on ADHD’s impact on HRQL may be important when developing consensus on appropriate prescribing practices and in fostering shared decision making. For health care policy, such efforts may prove important in standardizing treatment practices, thus providing appropriate care more consistently across the health system.
Several limitations should also be noted. We purposely restricted our sample to participants of our previous survey so that we could leverage available information from both surveys. We acknowledge that although our sample size was adequate to detect significant effects, it is small for a national survey. Furthermore, although we found no evidence that respondents differed from nonrespondents, small sample size reduced our power to detect such effects.
In this article, we focus on individual differences in utility scores, and, with the exception of the y-axis in Figure 1, we do not report their magnitude. Although the P-SG is a validated measure of utility, the high scores we obtained may be an artifact of the anchoring effect (Kuhberger, 1998; Kuhberger, Schulte-Mecklenbeck, & Perner, 1999) induced by the way in which probabilities are altered in this measure (Lenert, Cher, Goldstein, Bergen, & Garber, 1998). Although there is evidence that physicians assign higher utilities than patients for a number of different medical conditions (Brown, Brown, & Sharma, 2000; Chung, Shauver, Saddawi-Konefa, & Haase, 2011; Schackman, Teixeira, Weitzman, Mushlin, & Jacobson, 2008; Suarez-Almazor & Conner-Spady, 2001; Suarez-Almazor, Conner-Spady, Kendall, Russell, & Skeith, 2001), we urge caution in comparing the magnitude of utility values we found to those of similar studies that assessed ADHD utilities in parent populations using different forms of the standard gamble (Carroll & Downs, 2009; Matza et al., 2005). Nevertheless, the alignment of results with the severity of ADHD health states assessed and with our prior hypotheses suggests that the individual differences revealed by the P-SG are valid.
Finally, because the standard gamble measures respondents’ preferences for outcomes by assessing their willingness to accept risk, the resulting utility scores are likely a function of both respondent’s preferences and their risk tolerance. In this article, we interpret the standard gamble as a measure of preferences. However, interpreting standard gamble scores to reflect differences in risk tolerance among physicians may be equally valid, and is consistent with previous research in this area (Nightingale, 1988, 1987; Nightingale & Grant, 1988; Zaat & van Eijk, 1992).
In the future, additional research is needed to confirm the relationship between physicians’ attitudes regarding the impact of ADHD on HRQL and their practices for prescribing stimulant medications, and to determine whether this association applies to other pediatric disorders as well. In addition, we recommend incorporating the standard gamble into studies of provider-level differences in use of psychoactive medications.
Footnotes
Acknowledgements
We thank Norma Terrin, PhD, from The Institute for Clinical Research and Health Policy Studies at Tufts Medical Center for her statistical guidance. We also thank all the participating physicians who kindly participated in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Grant 1RC1HL100546-01 from the National Heart, Lung, and Blood Institute. Consultation from the Tufts CTSI was supported by Grant UL1RR025752 from the National Center for Research Resources.