
Abstract
Introduction
Although ADHD has long been considered a disorder of deficient emotional self-regulation (DESR), research has only recently once again focused on this construct and investigates this association (Barkley, 2010; Martel & Nigg, 2006; Skirrow, McLoughlin, Kuntsi, & Asherson, 2009); the literature is still rather poor and little is known about its etiology (Biederman, Spencer, et al., 2012).
Several studies (Biederman et al., 1995; Biederman, Petty, et al., 2012; Spencer et al., 2011; Dienes et al., 2002; Mick, Biederman, Pandina, & Faraone, 2003) have shown that children with ADHD struggle with emotion-regulation problems (Barkley, 2010). Low frustration tolerance, temper outbursts and mood lability, impatience and quickness to anger, as well as being easily excited in response to emotional reactions are considered hallmarks of DESR (Barkley, 1997; Nigg & Casey, 2005; Wender, 1995). Gottman and Katz (1989) defined emotion regulation as the ability to “(a) inhibit inappropriate behavior related to strong negative or positive emotion, (b) self-soothe any physiological arousal that the strong affect has induced, (c) refocus attention, and (d) organize for coordinated action in the service of an external goal” (p. 373). “For the purposes of clinical intervention or predicting course and outcome, it is important to understand whether it should be considered as an expression of ADHD, of a comorbid condition or a separate condition” (Biederman, Spencer, et al., 2012, p. 640).
Some researchers (Faraone et al., 2005; Spencer et al., 2011; Surman et al., 2011) have operationalized the clinical construct of DESR relied on the Child Behavior Checklist (CBCL) differentiating it from the more stringent cut-off levels in the pediatric bipolar disorder labeled CBCL–Juvenile Bipolar Disorder profile, CBCL–Mania proxy, or CBCL–Pediatric Bipolar Disorder profile (Hudziak, Althoff, Derks, Faraone, & Boomsma, 2005; Galanter et al., 2003; Mick et al., 2003). In a different research, profiles empirically derived from Anxious/Depressed, Attention, and Aggression (AAA)–CBCL scales were evaluated for their validity and reliability. Boomsma et al.(2006) and Hudziak et al. (2005) used in genetic studies the CBCL-Dysregulation profile (CBCL-DP) summed score, and Faraone et al. (2005) used receiver operating characteristic (ROC) curve analyses as a continuous measure of the CBCL-DP profile.
Recently, Spencer et al. (2011) showed that a unique profile of the CBCL consisting of a moderate (1 SD) increase in the CBCL Anxious/depressed, Attention, and Aggression subscales (CBCL-DESR profile: ≥180 and ≤210) identifies a sizable minority of children with ADHD and that ADHD children with this profile display higher levels of impairment than those without.
Specifically, the AAA profile from the CBCL was selected because of its conceptual congruence with the clinical concept of DESR and because its extreme (≥0.210, more than 2 SD above the M) form had been previously associated with severe forms of mood and behavioral dysregulation in children with ADHD (Biederman et al., 2009).
However, these studies were conducted on an American sample; uncertainties as to its generalizability in other samples outside the United States remain. In Europe, estimates of the prevalence of the broad category of ADHD vary from 2% to 5%, with variations among different European countries (Buitelaar et al., 2006; Ralston, Lorenzo, ADORE Study Group, 2004); in Italy, 3.9% of children were rated by educators with an additional 6.9% as potential cases (Gallucci et al. 1993). However, it is estimated that 6.7% of American school-age children are affected by ADHD, although estimates range between 1.7% and 16% (Barbaresi et al., 2004; Woodruff et al., 2004).
In Italy, it is easier to find children drug free because of the difficulty of psychiatric diagnosis and debate about use of pharmacological therapy as a legitimate therapeutic intervention.
From these considerations stems the interest in evaluating cross-cultural differences in relation to scientific, cultural, and ideological factors that have shaped the diagnosis of ADHD and its treatment in Italy.
Thus, the main objective of this study was to replicate and extend previous results reported in the work by Spencer et al. (2011) in an Italian sample of children with and without ADHD and, just reasons of comparability, the choice of the methodology has tried to trace the studies made by Biederman research group (Hudziak et al., 2005; Mick et al., 2003; Spencer et al., 2011). In particular, our goals were (a) to examine the prevalence and correlates of the CBCL-DESR profile defined by Spencer et al. in a U.S. sample subgroup of children with ADHD using an aggregate cut-off higher than 180 but lower than 210 on the AAA subscales of the CBCL and (b) to assess the sensitivity and specificity of the CBCL DESR using ROC curve analysis (Zweig & Campbell, 1993; Metz, 1978).
Method
Participants
We studied 358 children, 190 with a clinical diagnosis of ADHD according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed., DSM IV; American Psychiatric Association, 1994) criteria and 168 children of similar age and sex without ADHD as a control group.
The 190 ADHD children (167 males, M age = 9.01, SD = 2.32; 23 females, M age = 8.21, SD = 2.46) were Caucasian outpatients, newly diagnosed and drug naïve, who were consecutively referred to the Department of Child Neuropsychiatry at the La Scarpetta Hospital in Rome from January 2006 to December 2010. The composition of the sample by gender in our sample is somewhat biased, because the ADHD sample is 88% male. Actually, the percentage of females (12.0) was lower compared with the percentage found in the North American population of children with ADHD but similar to those found in European studies (Buitelaar et al., 2006). The control group consisted of 185 healthy Caucasian children (136 males, M age = 9.00, SD = 2.50, age range = 17-6; 32 females, M age = 9.28, SD = 2.76, age range = 14-6), matched for age and sex and randomly recruited from a community-based survey, who were attending seven elementary and junior high schools from the same urban area of Rome as the ADHD children. We excluded participants with cerebral palsy, deafness, blindness, autism, psychosis, and a Full-Scale IQ < 80.
Assessment
All the children and their parents underwent a semistructured psychiatric interview, the Schedule for Affective Disorders and Schizophrenia for School-Age Children–Present and Lifetime Version (K-SADS-PL1.0; Kaufman, Birmaher, Brent, Rao, & Ryan, 1996) and the Children’s Global Assessment Scale (CGAS; Schaffer et al., 1983), which were administered by an experienced child psychiatrist. All the children also received an additional clinical diagnostic assessment, including the ADHD–Rating Scale (ADHD-RS; DuPaul, Power, Anastopulous, & Reid, 1998) adapted for the Italian population (Marzocchi & Cornoldi, 2000), which was completed by parents and teachers, and the Wechsler Intelligence Scale for Children–Revised (WISC III; Wechsler, 2006; children with IQ < 80 were excluded). The children’s medical history and electroencephalogram were used to exclude comorbid medical and neurological conditions.
Finally, all the children were also assessed by means of the CBCL (Achenbach, 1991), which was completed by a parent. As the index of DESR, we used an aggregate cut-off ≥180 and ≤210 on the AAA scale of the CBCL. Children with a score above 210 on these scales were excluded.
Statistical Analysis
The statistical analysis was carried out with the usual descriptive statistics (measures of central tendency and dispersion) on the measures in the analysis using parametric and nonparametric analysis. We calculated percentages of DESR (CBCL-AAA scales >180 and <210) and non-DESR children in ADHD and control participants compared using the chi-square test difference testing. Finally, we used an imperfect golden standard as a composite score of severity (prevalence of comorbid disorders evaluated using K-SADS-PL1.0; Kaufman et al., 1996) and psychosocial impairment (derived from CGAS; Schaffer et al., 1983), and evaluated the discriminative accuracy of the CBCL-DESR profile as a continuous measure of the CBCL-DESR profile, by means of the ROC curve analysis (Metz, 1978; Zweig & Campbell, 1993).
Results
The two groups (ADHD and controls) were equivalent in age, t(356) = − 0.54, p = .59, Table 1, and sex (Mann-Whitney U Test: Z = −1,815, p = .069).
Demographic Characteristics of Pediatrically Referred ADHD Youths and Control Group
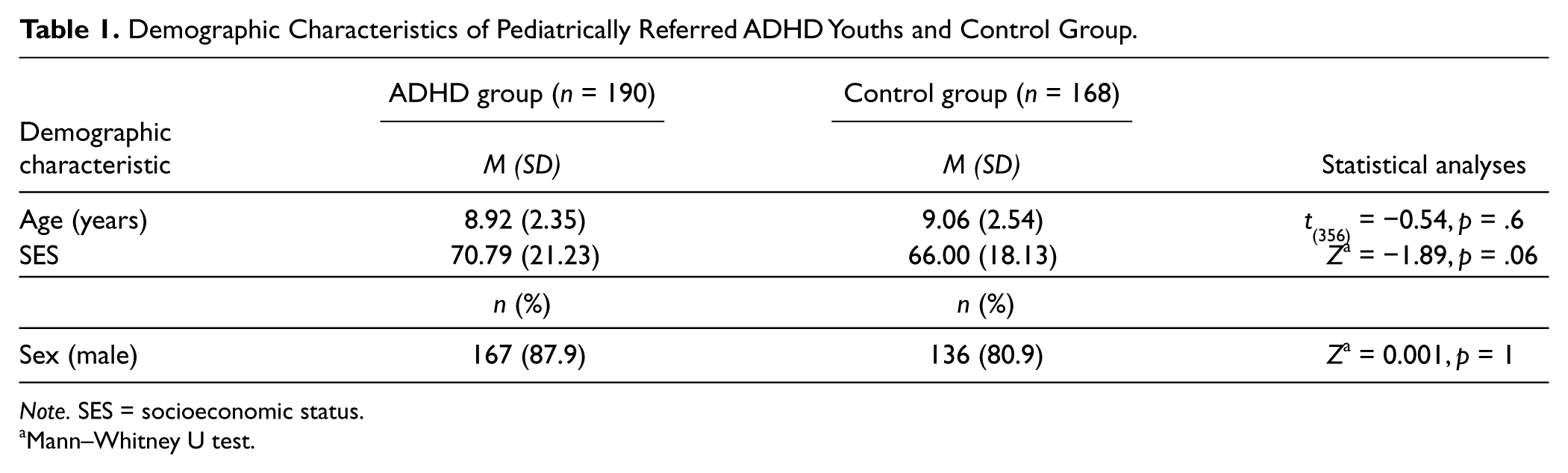
Note. SES = socioeconomic status.
Mann–Whitney U test.
All the participants were balanced according to the socioeconomic status score (Mann-Whitney U Test: Z = −1.89, p = .06) and were in the middle class status level, with the ADHD group having a mean score of 70.79 (SD = 21.23) and the control group having a mean score of 66.00 (SD = 18.13) according to the Hollingshead (1957) two-factor model.
With regard to the type of ADHD, the group composition was as follows: inattentive type (ADHD-I) accounted for 36.3% (n = 69) of the children, the combined type (ADHD-C) for 49% (n = 93), and the hyperactive/impulsive type (ADHD-HI) for 14.7% (n = 28).
In the Italian sample, 40.4% of the children with an ADHD diagnosis had a positive CBCL-DESR profile compared with only 3.5% of the children in the control group (χ2 = 104.27, >0.001).
As Table 2 shows, the ROC curve analysis, in which the true positive rate (sensitivity) is plotted as a function of the false positive rate (100-specificity) for different cut-off points of the CBCL-DESR Index Profile, documents an area under the curve of 0.91 and a significance level of p < .0001. This means that the test value in a randomly selected individual from the positive group is higher than that in a randomly chosen individual from the negative group in 91% of the cases (Zweig & Campbell, 1993).
ROC Curve
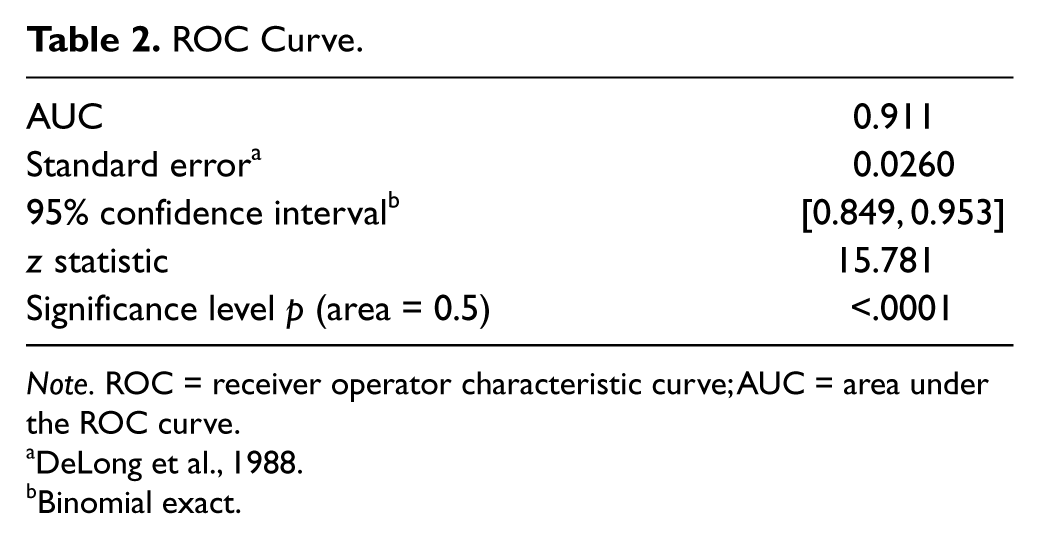
Note. ROC = receiver operator characteristic curve; AUC = area under the ROC curve.
Binomial exact.
Table 3 shows the criterion values and coordinates of the ROC curve: The true positive rate (sensitivity = 97.33) is plotted as a function of the false positive rate (100-specificity = 79.66) for the cut-off point “179” (CBCL-DESR Index Profile as a continuous measure of the CBCL-DESR profile).
Criterion Values and Coordinates of the ROC Curve
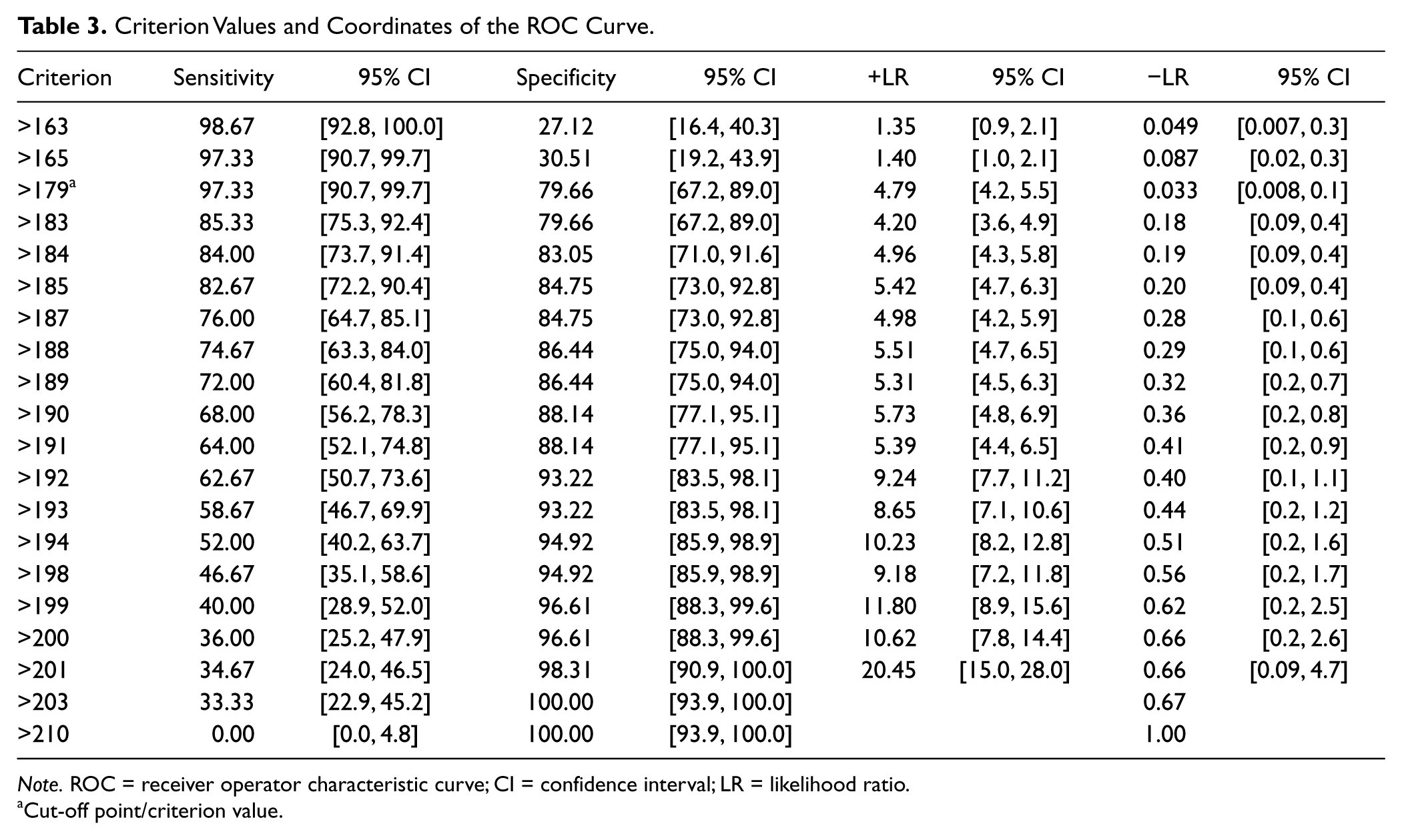
Note. ROC = receiver operator characteristic curve; CI = confidence interval; LR = likelihood ratio.
Cut-off point/criterion value.
Discussion
This study examined DESR as assessed by means of the CBCL (Achenbach, 1991) using an aggregate cut-off above 180 but below 210 on the AAA of the CBCL subscales. Using this approach, we identified a clinically significant subgroup of Italian ADHD children who had a higher clinical severity of ADHD (p < .05 for CGAS). Biederman, Spencer, et al., (2012) stressed the importance of investigate association between ADHD and a disorder of DESR “for the purposes of clinical intervention or predicting course and outcome, it is important to understand whether DESR should be considered as an expression of ADHD, of a co-morbid condition or a separate condition” (p. 640). Within this line of study, these results in an Italian sample replicate those previously reported by Spencer et al. (2011) in a U.S. sample. The results seems to be highly relevant to the particular Italian contest in relation to scientific, cultural and ideological factors shaped the diagnosis of ADHD and its treatment in Italy where it is easier to find children drug free.
Indeed, we found that 40.04% of the children with ADHD met the criteria for our a priori definition of DESR based on the CBCL, compared with only 3.57% of the control participants.
These figures are almost identical to those documented by Spencer et al. (2011) in a sample of American children (44% vs. 2%).
The second aim of this study was to evaluate the discriminating power of the CBCL-DESR profile to identify ADHD children with DESR from those without DESR by means of ROC curve analysis (Zweig & Campbell, 1993; Metz, 1978). We found an area under the curve of 0.91, which is associated with a very high level of statistical significance (p < .0001). In other words, these results mean that a randomly selected ADHD child with a positive profile would have a higher test value than a randomly chosen ADHD child with a negative profile in 91% of the cases (Zweig & Campbell, 1993).
As the DESR is a fairly new construct, the absence of a “golden standard” that allows an unrestricted basis to identify the DESR has affected us in the process of observation; therefore, like other studies of emotion dysregulation in individuals with psychopathology, we have chosen empirically observed data using clustering techniques to verify the specificity and sensitivity with the CBCL-AAA profile. Specifically, studies that have dealt with DESR stressed that DESR is an emotional component of ADHD associated with a higher number of comorbidities and later severe psychosocial impairment (Faraone et al., 2005; Spencer et al., 2011; Surman et al., 2011). Therefore, we clustered the individuals who had these values thereby defining an imperfect gold standard, and we have therefore assessed the reliability of this measurement with the three scales of the CBCL-AAA. In this case, we viewed the problem of evaluating an index test in the absence of a gold standard as a latent variable problem.
It is desirable to have a reference test in the future so that it can implement a procedure, but to date, to our knowledge, none exist if for adults (such as the self-report Current Behavior Scale, developed by Barkley to assess DESR in adults; Surman et al., 2011).
In conclusion, these results support the clinical utility of the CBCL-DESR profile as a means of identifying a sizable number of children with ADHD afflicted by DESR. In view of the fact that DESR worsens the already marked morbidity associated with ADHD, more efforts are warranted to develop treatment approaches to help address this problem.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.