
Abstract
Background
Over the past 40 years, the electroencephalogram (EEG) has been used to study patterns of cortical activity and the neurophysiological underpinnings of childhood psychiatric disorders such as attention-deficit/hyperactivity disorder (ADHD). EEG recorded at the scalp represents the summed cortical activity of large neuronal populations. Early studies of EEG recordings from children with ADHD reported qualitative observations such as excessive slow-wave and/or abnormal spike and wave activity (Satterfield, Cantwell, & Satterfield, 1974). Advances in technology and computer processing led to the quantitative analysis of EEG data using Fast Fourier Transform, which yields estimates of the spectral power contained in the recording that can be subjected to statistical analysis.
The most consistent EEG finding in ADHD is elevated frontocentral theta band (4-7 Hz) power relative to non-ADHD controls, during rest as well as cognitive activation conditions among child, adolescent, and adult populations (Bresnahan, Anderson, & Barry, 1999; Chabot & Serfontein, 1996; Clarke, Barry, McCarthy, & Selikowitz, 1998, 2001b; Hobbs, Clarke, Barry, McCarthy, & Selikowitz, 2007; Koehler et al., 2009; Loo et al., 2010; Matsuura et al., 1993). In a recent meta-analysis that includes 1,498 people, the effect size for theta band power increase was 1.31, with an average 32% increase in ADHD relative to controls (Snyder & Hall, 2006). Lower beta band (13-21 Hz) power is also a commonly reported finding in ADHD; however, the effect size is a more modest −0.51, representing an average decrease of 6% in ADHD compared with controls (Snyder & Hall, 2006).
The combination of these two EEG markers, or the theta to beta ratio (THBR) was first proposed by Lubar (1991) as a better way to capture the relative contributions of both measures. The THBR takes into account individual differences in amplitude or power as a result of skull thickness or other factors. Typically recorded at the vertex (Cz), the THBR was first thought to represent cortical hypoarousal (Lubar, 1991) or cortical slowing (Monastra et al., 1999). Subsequent studies comparing the THBR with measures of skin conductance suggest, however, that no relationship exists between this type of central nervous system arousal and the THBR (Barry, Clarke, Johnstone, McCarthy, & Selikowitz, 2009; Barry et al., 2004). Thus, the functional significance of the THBR is currently unclear. The THBR, however, has been negatively correlated with mean reaction time in adults with and without ADHD (van Dongen-Boomsma et al., 2010), suggesting that increased THBR is associated with a fast, impulsive response style. In contrast, the THBR was not significantly correlated with ADHD symptoms or cognitive performance on a sustained attention task in a sample of children with ADHD (Ogrim, Kropotov, & Hestad, 2012), suggesting age-related interactions. This measure has been proposed to reflect task-related cortical activation, but more research is needed to identify the range of conditions under which these differences appear and to understand the functional significance of these effects in terms of the underlying cortical processes that produce them.
In 2006, Snyder and Hall conducted a meta-analysis of EEG studies in ADHD and reported an effect size of 3.08 for the THBR recorded at Cz, which they suggest predicts a sensitivity and specificity of 94%. Because of such high sensitivity and specificity, some have advocated the use of the THBR in the clinical diagnosis of ADHD; however, this issue remains controversial. In addition, the THBR is reportedly highly stable over time with a 1-month reliability of .96 (Monastra, Lubar, & Linden, 2001) and is correlated strongly (.99) with age-related changes in ADHD behavioral symptomatology over time (Snyder & Hall, 2006). The elevation in the THBR is reportedly more pronounced in the combined subtype compared with the inattentive subtype of ADHD (Barry, Johnstone, & Clarke, 2003; Bresnahan & Barry, 2002; Bresnahan et al., 1999; Clarke, Barry, McCarthy, & Selikowitz, 2001a), although the difference sometimes does not reach statistical significance (Monastra et al., 1999; Monastra et al., 2001; Snyder et al., 2008) and the two ADHD subtypes may have slightly different scalp distributions (Barry et al., 2003). Common comorbidities such as oppositional defiant disorder (ODD) and reading disorder (RD) reportedly do not affect the elevated THBR associated with ADHD (Clarke, Barry, McCarthy, & Selikowitz, 2002a, 2002b), but these studies have been limited in sample size.
Although such a large effect size suggests that an elevated THBR is nearly ubiquitous in ADHD, several studies published since the meta-analysis reported no significant differences in the THBR between individuals with and without the disorder (Coolidge, Starkey, & Cahill, 2007; Lansbergen, Arns, van Dongen-Boomsma, Spronk, & Buitelaar, 2011; Nazari, Wallois, Aarabi, & Berquin, 2011; Ogrim, Kropotov, & Hestad, 2012; van Dongen-Boomsma et al., 2010). Review of these studies suggests there are numerous methodological, sampling, EEG parameters, and data analytic differences that may contribute to the variability across studies. In addition, the effects of psychiatric comorbidity and ADHD remission have not been examined systematically in large samples across the life span.
The purpose of this article is to replicate and extend the current findings by characterizing the THBR in a large sample of community and clinical participants and across a wide age range with regard to (a) current ADHD status and subtype, (b) common psychiatric comorbidities, and (c) cognitive correlates. Based on previous studies, we hypothesize that children, adolescents, and adults with ADHD will exhibit higher THBR compared with participants without ADHD, particularly among those with the combined subtype. We further predict that psychiatric comorbidity in ADHD will not affect the THBR and that this will be correlated with specific aspects of cognitive performance such as reaction time and reaction time variability.
Method
The sample includes 871 participants, 595 children and adolescents (5-18 years old), and 276 adults (32-64 years old). Participants were recruited between 2005 and 2011 into two concurrently running research studies on ADHD that used the same diagnostic, cognitive, and EEG measures. The first study is a clinical trial of medication treatment (MH077248) for ADHD, from which children with ADHD (n = 254) and non-ADHD, typically developing controls (n = 74) were enrolled. Used here are the children’s data from the baseline visit, which were used to determine study eligibility and conducted before any medication treatment began. The second study is the ADHD Genetics Study (NS054124) where all members of multiplex families with ADHD (i.e., 2 or more children with ADHD) were seen as part of the research protocol. From the genetics study, we used one child per family to maintain independence of the data (n = 267) and their parents, some of whom had ADHD (n = 81), but most of whom were unaffected (n = 195). Children and parents were analyzed separately in all analyses to maintain data independence. After receiving verbal and written explanations of study requirements, and prior to initiation of any study procedures, all parents/participants provided written informed consent/assent as approved by the Institutional Review Board.
Procedure
All participants underwent extensive phenotypic assessment, including diagnostic interviews and EEG recording. Participants aged 18 years and above were interviewed directly using the Schedule for Affective Disorders and Schizophrenia (SADS-LAR; Fyer, Mannuzza, Klein, & Endicott, 1995) supplemented with the Behavioral Disorders supplement from the Schedule for Affective Disorders and Schizophrenia for School-Age Children (KSADS-PL; Kaufman et al., 1997) to screen for the presence of ADHD and other childhood psychiatric disorders. Adults were asked to report the presence (and, if present, age of onset) of every ADHD symptom during childhood (primarily during school-age) and currently. In addition, the spouse (or parent if a proband) was asked to report current ADHD symptoms on a symptom checklist, the ADHD Rating Scale (ADHD-RS-IV; DuPaul, Power, Anastopoulos, & Reid, 1998). All children were evaluated based on an interview with the primary caretaker (usually mother) using the KSADS-PL and a direct interview with the child (if 8 years of age or above). Teacher reports were solicited for all participants and obtained for ~45% of youth. The teacher data were used to supplement data obtained during clinical interviews; if teacher’s report indicated that there was no impairment in the school setting while the youth was off-medication, the diagnosis of ADHD was changed to reflect the lack of impairment in two settings.
For adults, both past and current diagnoses of ADHD had to be consistent in order to be included in the current sample. Participants who did not have ADHD in the past (childhood) and currently were considered controls and only those who did have ADHD in the past and currently were included in the ADHD group. Participants (adults n = 24, adolescents = 1) who met diagnostic criteria for ADHD in the past, but did not currently meet ADHD diagnostic criteria (i.e., ADHD remitters), were excluded from the analysis. For the child and adolescent samples below the age of 18, psychiatric disorders were considered “present” if the participant currently met full Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) diagnostic criteria. If participants met full diagnostic criteria for ODD or conduct disorder (CD), they were considered to have a comorbid disruptive behavior disorder (DBD). Participants were considered to have a comorbid anxiety disorder if they met diagnostic criteria for simple phobia, social phobia, generalized anxiety disorder, obsessive-compulsive disorder, posttraumatic stress disorder, or panic disorder (with or without agoraphobia). Participants were classified as having comorbid depression if they met diagnostic criteria for major depression, bipolar disorder, or dysthymic disorder.
All interviews were conducted by clinical psychologists or highly trained interviewers with extensive experience in psychiatric diagnoses and training in using the KSADS. “Best estimate” diagnoses were determined after individual review of diagnoses, symptoms, and impairment level by senior clinicians (JJM, JTM). Interrater reliabilities were computed with a mean weighted kappa of .84 across all diagnoses with a greater than 5% occurrence in the sample. Participants were excluded from participation if they were positive for any of the following: neurological disorder, head injury resulting in concussion, lifetime diagnoses of schizophrenia or autism, or estimated Full Scale IQ (FSIQ) < 80. In addition, control participants were excluded if they had any major Axis I diagnosis with the exception of ODD or simple phobia or were on any type of psychoactive medication. Participants with ADHD who were on stimulant medication were asked to discontinue use for 24 hr prior to their visit.
Cognitive measures
The age-appropriate Wechsler Scale was used to derive a two-subtest estimate of general intellectual functioning or FSIQ. The Vocabulary and Block Design subtests were used to estimate FSIQ, which had a .9 correlation with FSIQ derived from the full battery (Sattler, 1992). A Go/No-go (GNG; Conners, 2000) was also administered as a measure of response inhibition. The GNG is a 14-min computerized task during which participants sat approximately 27 to 36 inches away from the 19-inch presentation screen and were asked to press the space bar when any letter except the target letter “X” appeared. Task specifications are as follows: 360 trials, 36 presentations of the inhibition target (X), targets (including “go” targets: A,B,C,D,F,I,L,O,T) were presented in randomized order for 250 ms in Arial 80-point font with variable intertrial intervals of 750, 1,750, and 3,750 ms).
Electrophysiological methods
EEG recording was carried out using 40 Ag/AgCl surface electrodes that were embedded in an electrode cap in an extended International 10/20 location system (ElectroCap, Eaton, Ohio) and was referenced to linked ears. Impedance was below 10 kOhms and EEG signal was recorded using MANSCAN (Sam Technology, San Francisco, CA) hardware and software. EEG data were sampled at a rate of 256 samples per second. Eye movements were monitored by electrodes placed on the outer canthus of each eye for horizontal movements and by electrodes above the eye for vertical eye movements. EEG recording for all participants consisted of two baseline conditions lasting 5 min each during which participants sat quietly with their eyes closed (EC) or eyes open (EO) in a fixed gaze.
Continuous EEG data were reviewed offline by a technician experienced in EEG and all segments containing eye, head movement or muscle artifact were removed from further analysis. Using a Fast Fourier Transform, EEG power (µV2) was averaged for each condition and exported in the following bandwidths: theta (4-7 Hz), alpha (8-11 Hz), and beta (13-21 Hz). The primary dependent variables (DVs) are the EO and EC THBR at the electrode Cz, which were calculated by dividing theta band power by beta band power for each condition. Variables were checked for skewness and kurtosis and subsequently natural log (ln) transformed to assume a normal distribution. EEG technicians were blind to ADHD diagnostic status.
Statistical analyses
Statistical analyses were run in SPSS 17.0. Because age has significant effects on EEG power, all analyses were run according to three age groups, children (6-11 years old), adolescents (12-18 years old), and adults (19 years old and above). These age groups were chosen based on age groups previously reported in THBR studies. First, to test the effect of ADHD diagnostic status on the THBR, separate univariate ANOVAs were run using ADHD diagnosis and subsequently, ADHD subtype as the independent variables (IVs) and EO and EC THBR as the DVs. Omnibus effects significant at the p < .05 level were followed by post hoc contrasts using Tukey tests for least significant difference (LSD). Second, we tested the effect of ADHD comorbidity with depression, anxiety, or other DBD (i.e., ODD or CD) on the THBR. Again, ANOVAs were run using ADHD comorbidity (participants were coded according to if they were a control, ADHD without the comorbidity or ADHD with the comorbidity) as the IV and the EO and EC THBR as the DVs. Due to power concerns (sometimes low rates of comorbidities) and to reduce the number of comparisons, we combined child and adolescent groups for the comorbidity analyses and used an ANCOVA, controlling for age. Separate analyses were run for the psychiatric comorbidities in the adult group. Finally, we ran Pearson product–moment correlations between the THBR and behavioral and cognitive variables to assess the functional significance of the THBR. The Pearson correlations were run separately for child and adult groups and partial correlations, controlling for age were used. Effect size was estimated using Cohen’s d, which is interpreted according to the following guidelines: small d = .2, medium d = .5, large d = .8 (Cohen, 1988).
Results
Sample characteristics
Presented in Table 1 are demographics and clinical correlates for participants in each of the age groups. Within each age group, participants did not differ with regard to mean age, FSIQ, socioeconomic status (SES), or ethnic/racial status. There were, however, significant differences in the gender distribution within the child sample, where there was a much larger percentage of males in the ADHD sample (71%) compared with the control sample (48%; χ2 = 12.8, p = .001). We therefore used sex as a covariate in all analyses. As expected, the ADHD sample exhibited significantly more inattentive and hyperactive-impulsive behaviors compared with controls (p < .001) across all age groups. Within each age group, the THBRs were significantly skewed (range across age groups EO THBR: 1.2-2.8; EC THBR: 1.9-6.4) and were natural log (ln) transformed prior to analyses.
Sample Demographic and Clinical Description.
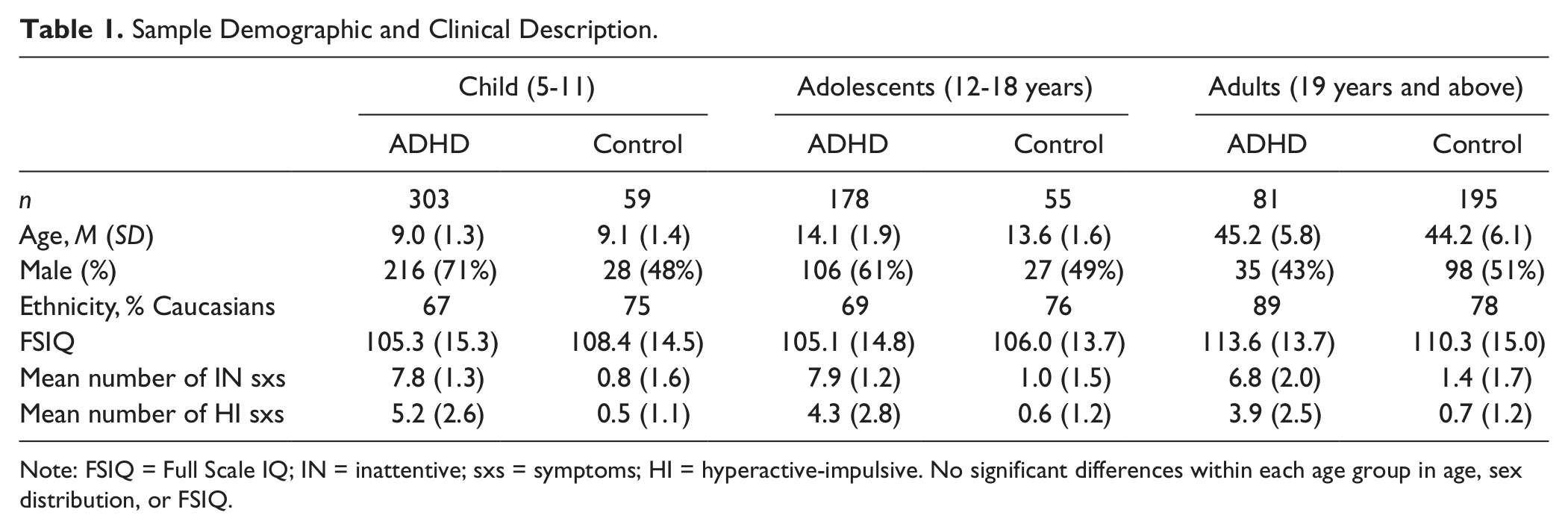
Note: FSIQ = Full Scale IQ; IN = inattentive; sxs = symptoms; HI = hyperactive-impulsive. No significant differences within each age group in age, sex distribution, or FSIQ.
THBR by ADHD diagnostic status
Presented in Table 2 are the mean THBRs according to ADHD diagnostic status and ADHD subtype for each age group. Inspection of the means reveals an age effect, with decreasing THBR as age increases, for ADHD and controls. The THBR collected during EO or EC conditions did not differ significantly by ADHD status for children—EO: F(1, 251) <1, d = .15; EC: F(1, 270) = 2.0, p = .16, d = .24, or adolescents—EO: F(1, 178) <1, d = .09; EC: F(1, 211) = 1.03, p = .31, d = .14. In adults, the EO THBR was not significantly different by ADHD status, F(1, 251) = 2.02, p = .16, d = .20; however, the EC THBR differed significantly by ADHD status, F(1, 260) = 5.10, p = .02, d = .28. Inspection of the means (see Table 2) suggests that the THBR is lower in adults with ADHD compared with controls, which is in the opposite direction of the hypothesized ADHD effect. Effect sizes for ADHD across all age groups were small.
Theta–Beta Ratio (ln Transformed) at Cz by Age Group.
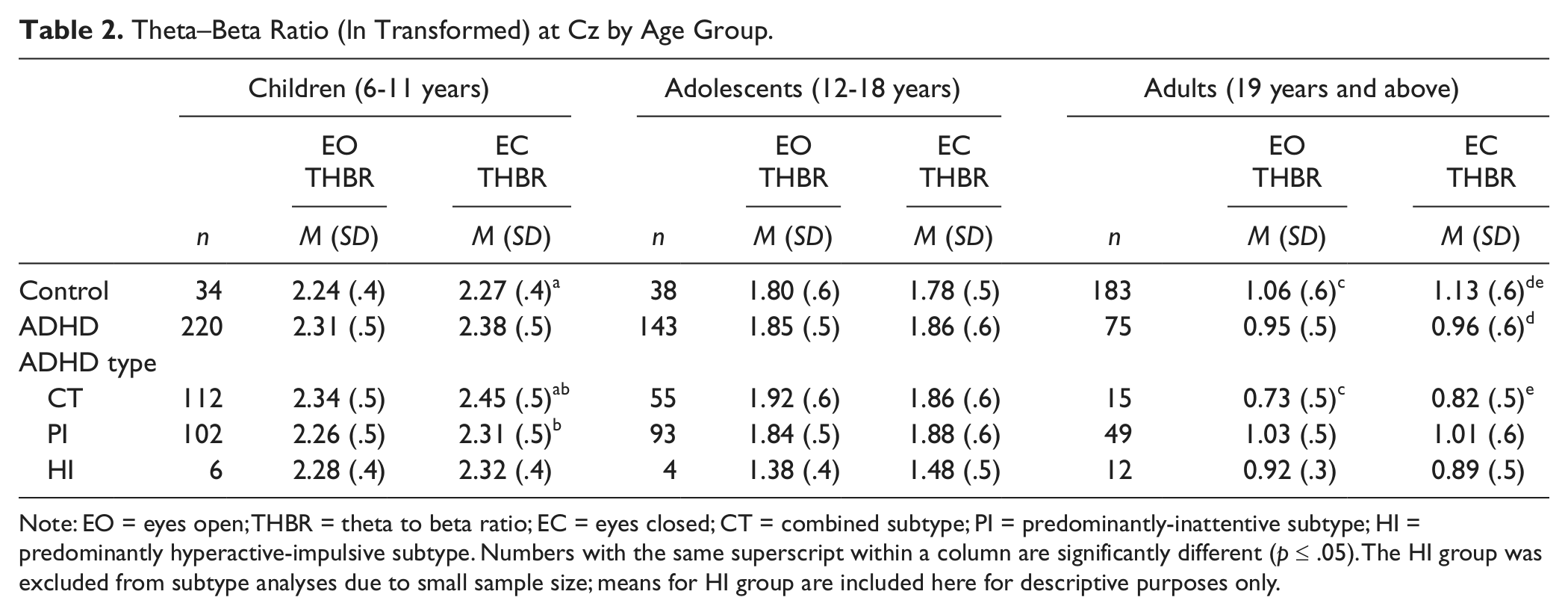
Note: EO = eyes open; THBR = theta to beta ratio; EC = eyes closed; CT = combined subtype; PI = predominantly-inattentive subtype; HI = predominantly hyperactive-impulsive subtype. Numbers with the same superscript within a column are significantly different (p ≤ .05). The HI group was excluded from subtype analyses due to small sample size; means for HI group are included here for descriptive purposes only.
THBR by ADHD subtype
To examine the effect of ADHD subtype on the THBR, participants were coded according to their current ADHD subtype, as follows: predominantly inattentive (PI) type: 6+ inattentive (INN) and <6 hyperactive-impulsive (HI) symptoms; hyperactive-impulsive (HYP) type: 6+ HI and <6 INN symptoms; combined type (CT): 6+ IN and 6+ HI symptoms. Because of small sample size of the HYP subtype, these participants were dropped from the analysis and the two remaining ADHD subtypes were compared with controls (see means in Table 2). A strong developmental effect was seen in the effect of ADHD subtype, with significantly higher THBRs in the ADHD-CT group among children, but lower THBR among adults with ADHD-CT. Within the child sample, a significant effect of ADHD subtype emerged on the EC THBR, F(2, 263) = 3.09, p = .05, d = .40. Individual contrasts indicate that children with ADHD-CT exhibited a higher EC THBR compared with controls (p = .04) and those with ADHD-PI (p = .04). The THBR did not differ according to ADHD subtype for the child sample in the EO condition, F(2, 243) = 1.18, p = .31, d = .22, in the adolescent sample, EO: F(2, 170) < 1, d = .20; EC: F(2, 201) < 1, d = .18, but showed trends toward significance for adults in the EO condition, F(2, 239) = 2.39, p = .09, d = .60, and EC condition, F(2, 248) = 2.45, p = .09, d = .56. Individual contrasts suggest that, compared with controls, the adults with ADHD-CT had a significantly lower EO THBR (p = .03) and EC THBR (p = .05).
THBR by psychiatric comorbidity
Because ADHD is often comorbid with other psychiatric disorders, we tested whether psychiatric comorbidity had significant effects on the THBR. To reduce the number of comparisons, we conducted all subsequent analyses solely on the EC THBR, which appears to be marginally more sensitive to ADHD status. In addition, the child and adolescent samples were collapsed (and are hereafter referred to as “youth”) and age was used as a covariate in all subsequent analyses. The adult sample was analyzed separately given the reverse direction of the THBR ratio findings. Findings are presented in Table 3.
Theta to Beta Ratio (ln Transformed) by Psychiatric Comorbidity.
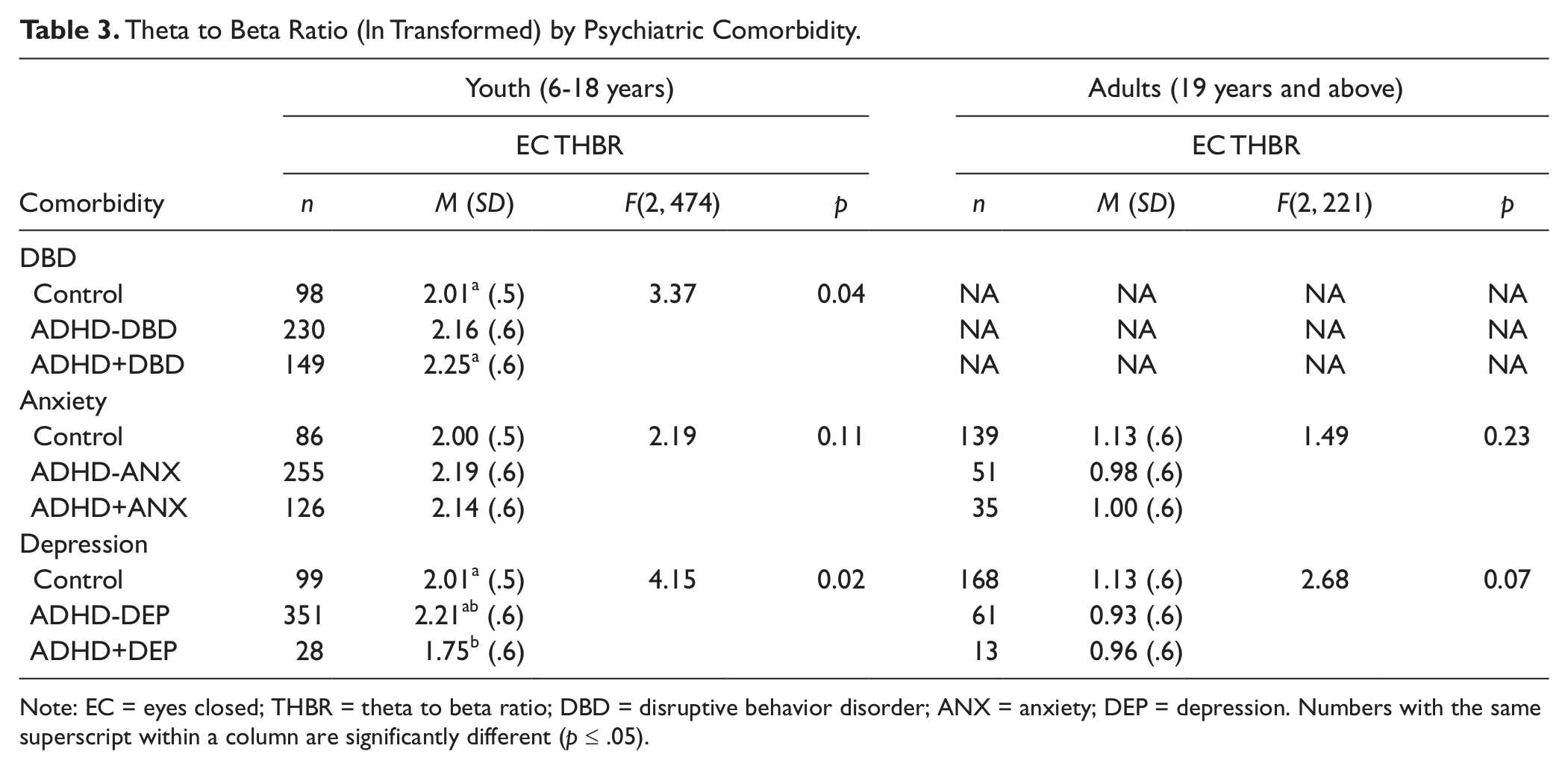
Note: EC = eyes closed; THBR = theta to beta ratio; DBD = disruptive behavior disorder; ANX = anxiety; DEP = depression. Numbers with the same superscript within a column are significantly different (p ≤ .05).
THBR by DBD comorbidity
Within the youth (6-18 years) sample, the presence of comorbid DBD was tested using an ANCOVA controlling for age. The presence of ODD or CD results in a modest increase in THBR, F(2, 474) = 3.4, p = .04, d = .43. Post hoc contrasts suggest that youth with comorbid ADHD and ODD/CD had a significantly higher THBR relative to controls (p < .05). Because ODD and CD are childhood disorders, we did not assess DBDs in adults.
THBR by anxiety disorder comorbidity
Within the youth sample, the effect of a comorbid anxiety disorder on the THBR trended toward significance, F(2, 463) = 2.19, p = .11, d = .34, suggesting comorbid anxiety results in a nonsignificant decrease in the THBR. A similar, nonsignificant effect of comorbid anxiety was found in the adult sample, F(2, 221) = 1.49, p = .23, d = .25.
THBR by depressive disorder comorbidity
The effect of comorbid depression in ADHD appears to significantly lower the THBR, F(2, 474) = 4.15, p = .02, d = .47. Individual contrasts suggest that the youth with ADHD and no depression had a significantly higher THBR compared with controls (p = .02) and those with comorbid depression (p = .04). Among youth with ADHD, depression has a strong mediating effect on the THBR. Among adults, a trend toward significance emerged, F(2, 238) = 2.68, p = .07, d = .33, but reflects the difference between controls and ADHD and no depression (p = .03) who were no different from ADHD with depression.
Behavioral and cognitive correlates of the THBR
We then conducted Pearson correlations between the THBR and ADHD symptoms and DVs from the GNG to assist with interpretation of functional significance of the THBR. As can be seen in Table 4, resting state THBR is significantly correlated with the number of inattentive symptoms in both youth and adult samples (ps < .05). However, the direction of the correlation is not the same in the two samples. In the youth sample, the THBR is positively correlated with inattentive symptoms, suggesting more inattentive symptoms are associated with higher THBR. In contrast, the THBR is negatively correlated with inattentive symptoms in the adult sample, suggesting that a lower level of inattention is associated with higher THBR; this finding is consistent with the earlier result of adults with ADHD exhibiting a lower THBR relative to non-ADHD adults.
Correlations Between Theta to Beta Ratio and ADHD Symptoms and Cognitive Performance.
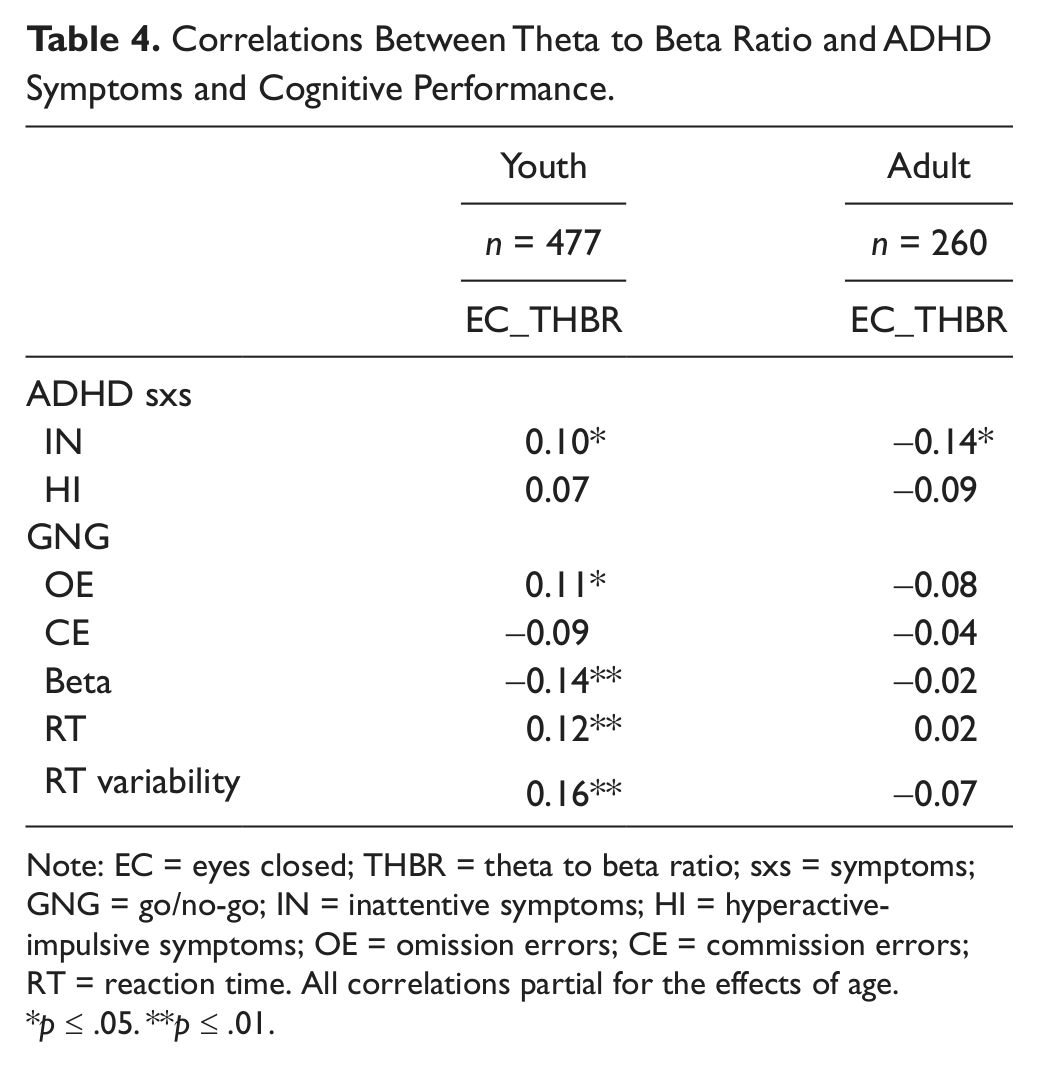
Note: EC = eyes closed; THBR = theta to beta ratio; sxs = symptoms; GNG = go/no-go; IN = inattentive symptoms; HI = hyperactive-impulsive symptoms; OE = omission errors; CE = commission errors; RT = reaction time. All correlations partial for the effects of age.
p ≤ .05. **p ≤ .01.
In addition, significant correlations emerged between several cognitive variables that indicate inattention in the youth sample. The THBR marker was associated with omission errors, lower beta (which indicates a more conservative response style that emphasizes errors of omission rather than commission errors), and a slow and variable reaction time (all ps < .05). None of the cognitive variables were significantly correlated with the THBR marker in the adult sample. Furthermore, all correlations were very modest (>.2) and reached the threshold for significance primarily due to power afforded by such large sample sizes.
Discussion
The goal of this article was to characterize the THBR in a large community and clinical sample of individuals with and without ADHD and to examine sources of heterogeneity within this well-characterized sample. The results reported here can be summarized as follows. First, the association between increased THBR and ADHD was not replicated for children, adolescents, or adults within this sample. Second, the nonreplication may have occurred because the THBR is influenced by numerous factors beyond ADHD categorical status, such as age, ADHD subtype, and comorbid psychiatric diagnoses. EEG-related factors such as recording condition and (possibly) the sample distribution of the THBR may also represent other confounding effects. Finally, the THBR is associated with inattention; however, the relationship is modest and differs according to developmental stage. These factors may underlie the heterogeneity of THBR findings across studies within ADHD.
Consistent with more recent studies (Nazari et al., 2011; Ogrim et al., 2012; van Dongen-Boomsma et al., 2010), we did not find that individuals with ADHD per se exhibited significantly higher THBR. Closer inspection of the actual (non-ln transformed) THBR values indicates that, in the current study, children and adolescents with ADHD had a similar THBR as those reported in other studies. However, the non-ADHD comparison group in this study had higher THBRs compared with controls in other studies. This trend for controls of all ages to have higher THBR is seen among the more recent studies (within the past 2 years) and is discussed in detail in Arns et al. (in press). This may bring into question the controls used for the current study; however, the child and adolescent controls had very low levels of inattentive and hyperactive-impulsive symptoms and were largely free of other psychiatric diagnoses (11/114 [9.6%] and 4/114 [3.5%] had one and two psychiatric diagnoses, respectively).
The findings for the THBR among adults with ADHD ran counter to the hypothesized direction and suggested a significantly lower THBR in adults with ADHD relative to those who did not ADHD. This is in contrast to previous studies that found a significantly increased THBR among adults with ADHD (Bresnahan et al., 1999; Clarke et al., 2011) or no significant differences in THBR between adults with and without ADHD (van Dongen-Boomsma et al., 2010). Sampling may be the reason for such divergent results. The non-ADHD adult sample is comprised of parents of children with ADHD and, thus, may have a stronger loading of gene variants that contribute to risk for ADHD as well as traits associated with ADHD (such as the THBR). In addition, the non-ADHD adults tended to have other psychiatric diagnoses (45/189 [23.8%] and 10/189 [5.3%] had one and two diagnoses, respectively), whereas the other studies used adults who were free of all psychiatric diagnoses. Further research using larger samples of adults and controlling for ADHD familial status may help to clarify this finding.
We also found that ADHD subtype and certain psychiatric comorbidities also had a significant impact on the THBR. A previous study reported that the presence of ODD, the most common comorbidity in ADHD, did not significantly affect the THBR (Clarke et al., 2002a). Inspection of the Clarke (2002a) data suggests that the comorbid ADHD and ODD group had higher THBRs that did not meet the threshold for significance, which may have been affected by low power due to modest sample size (n = 25 per group). The inclusion of CD and the larger sample size in the current study likely provided additional power to detect group differences. Previous studies have not directly examined the impact of comorbid anxiety and depression on the THBR. Snyder et al. (2008) reported that their presence did not significantly affect the classification accuracy when both (ADHD and non-ADHD) had the comorbid disorder but did not report actual THBR values. Thus, the presence of comorbid DBD and depression appear to mediate the expression of the THBR in ADHD. The degree to which a particular study sample includes those comorbidities may alter the association of the elevated THBR and ADHD.
Overall, the THBR is associated with several measures reflecting inattention, including number of inattentive symptoms and cognitive measures such as omission errors, reaction time, and reaction time variability. In the youth sample, higher THBR was associated with greater number of inattentive symptoms, omission errors, and a slow and variable reaction time, suggesting it does reflect several aspects of inattention. These results are in contrast to Ogrim et al. (2012), who did not find any significant correlations between the THBR and behavioral or cognitive measures; however, the smaller sample size may not have afforded sufficient power to detect such modest associations. The adults in this sample did not show similar associations between the THBR and behavioral/cognitive indicators of ADHD, which is in contrast to a previous study of adults with ADHD that found association with a fast, impulsive response style (van Dongen-Boomsma et al., 2010). Methodologic differences such as the method for calculating THBR, type of inhibition task, and sampling may have contributed to different results. Similar to the overall finding of lower THBR among adults with ADHD, the THBR was negatively associated with number of inattentive symptoms. It is not clear whether this finding reflects some sort of compensatory mechanism as the adults in the ADHD group are relatively higher functioning with mean IQ in the high average range. Overall, more studies with large samples of adults with and without ADHD are needed to confirm the direction and strength of association between the THBR and markers of inattention.
There are several limitations that may hamper the generalizability of the results. As previously mentioned, the adult sample was made up of parents ascertained for having two children affected with ADHD. It is possible that these non-ADHD parents have a higher THBR than other parents without ADHD children. Some gene variants that are shared by the non-ADHD parent may be associated with higher THBR even when their diagnostic status is not ADHD. In this case, other genes may be required to result in ADHD, which can be contributed to the child by the other parent or even in a few cases by mutation. The size of our comparison groups for the child and adolescent analyses were relatively smaller than the ADHD sample size, raising questions about power limitations and Type I error. We note that the current sample size of youth controls (n = 114) is quite a bit larger than previous studies that have demonstrated large differences in THBR according to ADHD status, such as Monastra et al. (2001; n = 74 controls, ages 6-20 years) and Snyder et al. (2008; n = 62 non-ADHD controls, ages 6-18 years). In addition, we chose to use an uncorrected p < .05 threshold for significance with no correction for multiple comparisons. This may have introduced Type I (false positive) error; however, the goal was to better understand sources of heterogeneity in the THBR marker. As many of the effects were modest, some of the significant effects may in fact be nonsignificant.
Overall, this study suggests that more research is needed into the sources of heterogeneity and functional significance of the THBR EEG marker before it can be proposed for clinical application in any manner as a diagnostic tool for ADHD. Based on our data, and that of others, it appears unlikely that the Cz THBR is sufficient to sensitively discriminate the complex differences in brain electrical activity involving multiple brain circuits believed to underlie the syndrome of ADHD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institutes Health (R01 NS054124 and RO3 MH92829 (PI: Loo) and P50MH077248 (PI: McCracken). Dr. McGough has received consulting honoraria from Eli Lilly & Co., Next Wave Pharmaceuticals, Noven Pharmaceuticals, and Shire Pharmaceuticals. Dr. McCracken reports receiving research grants from Seaside Therapeutics and Bristol-Myers Squibb, and has received consultant income from Shionogi, BioMarin, Novartis, PharmaNet, and Noven. Other authors do not have financial interests to disclose.