
Abstract
Introduction
The objective of this article is to review the research on slow cortical potential (SCP) feedback in children, adolescents, and adults with ADHD and report the possible standard “one size fits all” application for this type of neurofeedback.
This review is divided into three parts. The first part gives an overview about relevant ADHD factors and describes the rationale and procedure of SCP feedback in ADHD. The second part reviews ADHD and SCP feedback studies, highlighting the strengths and limitations of this approach for treating ADHD. The last section discusses open questions and future challenges regarding the use of SCP feedback in ADHD and the possible standard protocol.
ADHD
ADHD is one of the most common disorders of childhood. However, 30% to 65% of the children with ADHD continue to have symptoms in adulthood (Faraone, Biederman, & Mick, 2006). The appropriate treatment of ADHD is still a matter of debate because of, for example, side effects (Graham et al., 2011), high rate of nonresponders, and short- and long-term effects after washout of medication. Physiological and neurophysiological models led to new treatment modules. One of these alternative treatments is of SCPs targeting the neurophysiological variations in ADHD.
Rationale of SCP-Feedback
SCP feedback was originally developed for the treatment of epilepsy (Rockstroh et al., 1993), but it is well researched and applied in the treatment of ADHD as well, as both conditions are characterized by difficulties in regulation of cortical excitation thresholds. Neurofeedback is a variant of electroencephalogram (EEG) biofeedback that aims to acquire self-regulation over certain brain activity patterns in an operant conditioning paradigm (Sherlin et al., 2011). A meta-analysis of the efficacy of frequency and SCP feedback treatment in ADHD reported clinical effects with a large effect size (ES) on inattention and impulsivity and a medium ES on hyperactivity (Arns, De Ridder, Strehl, Breteler, & Coenen, 2009). Frequency feedback targets abnormal activity in frequency bands such as increased theta/beta or theta/alpha ratios, elevated relative theta power, and reduced relative alpha and beta power in children (for a review, see Barry, Clarke, & Johnstone, 2003) and similar parameters in adults (Bresnahan, Anderson, & Barry, 1999; Bresnahan & Barry, 2002; Clarke et al., 2008).
SCP feedback is focused on the difficulties in regulation of cortical activation and inhibition. These threshold regulation mechanisms are very slow electrical shifts in brain activity, also known as SCPs. They change periodically from being electrically positive to negative and are described as a phasic tuning mechanism in the regulation of attention (Rockstroh, Elbert, Lutzenberger, & Birbaumer, 1990). They are generated cortically and subcortically, involving brain stem reticular mechanisms, the thalamus and the basal ganglia. The main factor contributing to SCP recordings are synaptic activities at apical dendrites in superficial layers of the cortex. Negativation represents activation, increasing the firing probabilities of the underlying cortical areas, and is due to long-lasting depolarization of superficial layer apical dendrites. Positivation represents an inhibition and a decrease in firing probabilities. SCPs are related to cognitive performance and motor actions. A positive shift reflects consumption of resources and disfacilitation of excitation thresholds. A negative shift reflects provision of resources and facilitates attention as well as initiation of goal-directed behavior that can be observed in enhanced reaction time, stimulus detection, and short-term memory during the negative shift phase (Birbaumer, Elbert, Canavan, & Rockstroh, 1990). Therefore, self-regulation of SCPs is important in disorders with impaired excitation thresholds like epilepsy or ADHD.
A well-researched negative SCP is the contingent negative variation (CNV). The CNV belongs to the family of event-related potentials (ERPs), which are widely used to investigate the neurophysiological basis of cognitive functions. ERPs are reactions of the brain to a specific stimulus or in preparation of a motor or cognitive answer. To make them “visible,” the raw EEG has to be averaged locked to a specific stimulus over many trials. The CNV is a slow negative potential over central sites. It occurs in reaction to a warning stimulus in go- or cue trials and represents anticipation and/or preparation, attentional behavior, and motor preparation (Walter, 1964). The negative amplitude increases with the amount of “cognitive energy” in anticipation of task performance. However, in ADHD decreased CNV amplitudes have been observed. During various experiments, reduced CNV amplitudes have been observed for children with ADHD (Banaschewski & Brandeis, 2003; Banaschewski et al., 2004; Hennighausen, Schulte-Körne, Warnke, & Remschmidt, 2000; Perchet, Revol, Fourneret, Mauguière, & Garcia-Larrea, 2001; Sartory, Heine, Müller, & Elvermann-Hallner, 2002; van Leeuwen et al., 1998) and similarly in adults with ADHD (Dhar, Been, Minderaa, & Althaus, 2010; Mayer, Wyckoff, Schulz, & Strehl, 2012; Weate, Newell, Bogner, Andrews, & Drake, 1993) compared with healthy controls. The findings of a decreased CNV in ADHD are in line with the cognitive energetic model of ADHD, which states a dysfunctional regulation of energetical resources in ADHD (Sergeant, 2000, 2004). Several studies found an increased CNV after SCP feedback, supporting the relationship between the experimentally provoked CNV and SCP feedback (Gevensleben et al., 2010; Heinrich, Gevensleben, Freisleder, Moll, & Rothenberger, 2004; Mayer et al., 2012; Wangler et al., 2011).
Practice of SCP Feedback
In SCP feedback, participants learn to voluntarily generate surface-negative and surface-positive SCP shifts over the sensorimotor cortex on electrode position Cz. In addition to the EEG electrode, the reference, and the ground, two or four electrodes are needed to record and correct for vertical and/or horizontal eye movements, as the SCP signal is especially vulnerable to artifacts. SCP feedback is discontinuous trial-based feedback, which consists typically of three phases: a baseline phase (2 s), an active phase (5-8 s), and a reinforcement phase (2 s). During the active phase, the participant has to move an object or change the color of an object reflecting the brain activity in the cued direction, up for activation (negativation) and down for deactivation (positivation). To generalize the regulation skills to everyday life situations, part of the treatment consists of “transfer trials” in which no visual feedback is presented during the active phase (Strehl, 2009). A visual stimulus, given as a “reward” during the reinforcement phase if the cued brain state is reached, informs the participants whether they were successful. Positivation and negativation trials are presented randomized. About 40 trials constitute a “run.” A session may contain two to four runs. More details will be given with the report of each study (see below).
Unlike the variety of frequency feedback protocols (frequency bands, thresholds, electrode sites, and feedback modalities), SCP feedback has a “one size fits all” protocol with only slight possible variations. Advantages and disadvantages will be discussed later.
Method
Studies were selected based on searches in PubMed, Ovid MEDLINE, ERIC, and Google Scholar using combinations of the following keywords: neurofeedback or EEG biofeedback or neurotherapy and SCP or slow cortical potentials and ADHD or attention deficit hyperactivity disorder. The search was run independently by the authors and yielded identical results.
Research Review
Six studies met the search criteria outlined above and were included in this review. Six subsequent publications investigating additional behavioral and neurophysiological parameters, session data, and long-term treatment effects of these studies were also included (see Table 3). Three major workgroups emerged during the review search, including research contributions from the University of Göttingen, University of Tübingen, and University of Zürich. A summary of the treatment studies conducted by these institutions, with emphasis on study design, participant population, treatment duration, outcome variables, and study limitations, are presented in detail below and in Tables 1 to 4. For an overview of the SCP protocol details discussed throughout the review, see Table 1. Examples of the protocol screens used in each study are provided in Figure 1. For information on the additional behavioral components for “transfer to daily life” of the SCP protocols presented, see to Table 2. Information related to the study design and assessments are summarized in Table 3. Finally, a summary of study results and treatment outcome is provided in Table 4.
Overview of SCP Feedback Protocol Details.
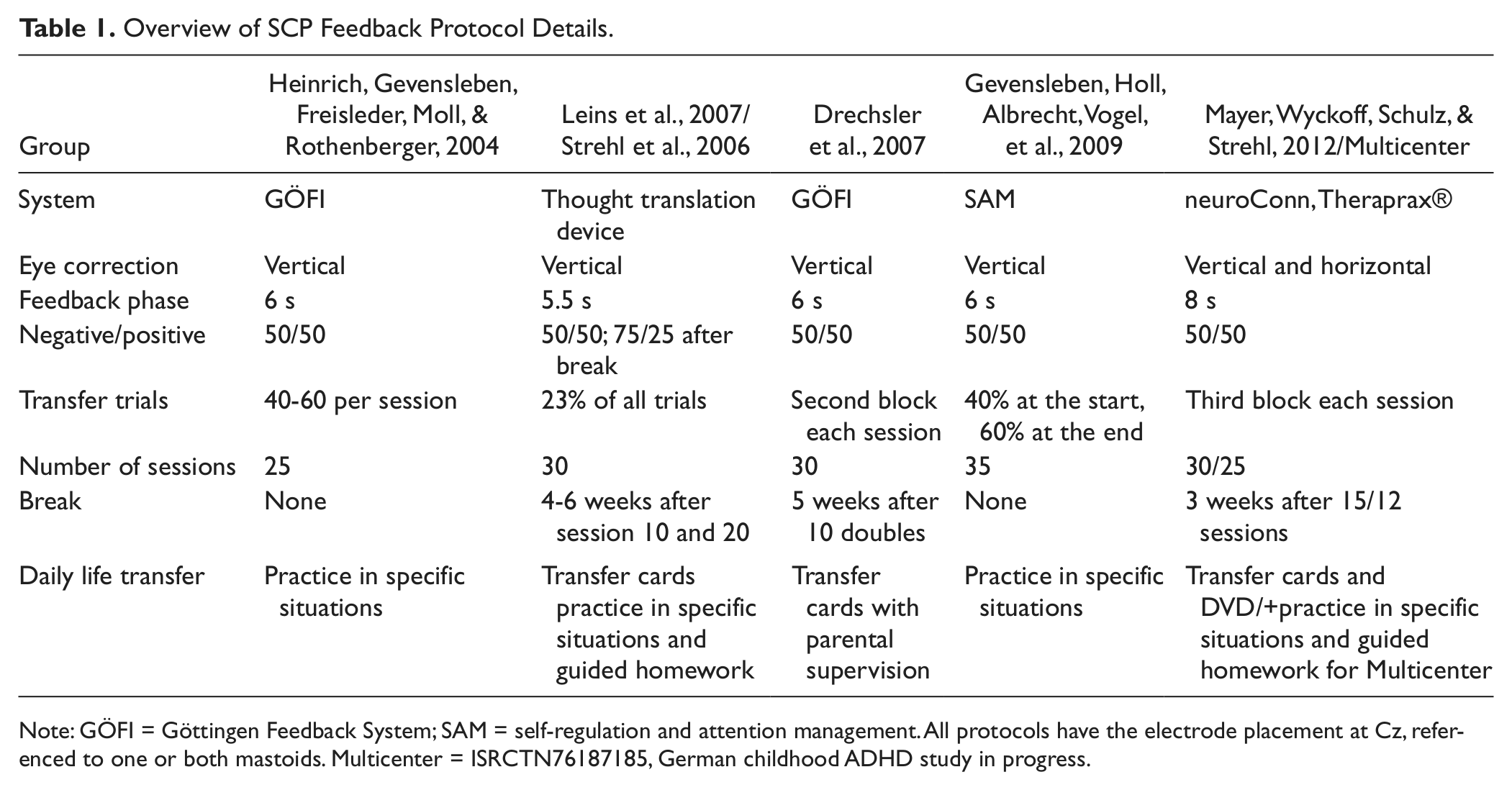
Note: GÖFI = Göttingen Feedback System; SAM = self-regulation and attention management. All protocols have the electrode placement at Cz, referenced to one or both mastoids. Multicenter = ISRCTN76187185, German childhood ADHD study in progress.
Overview of Additional Behavioral Components for “Transfer to Daily Life” of SCP Protocols.
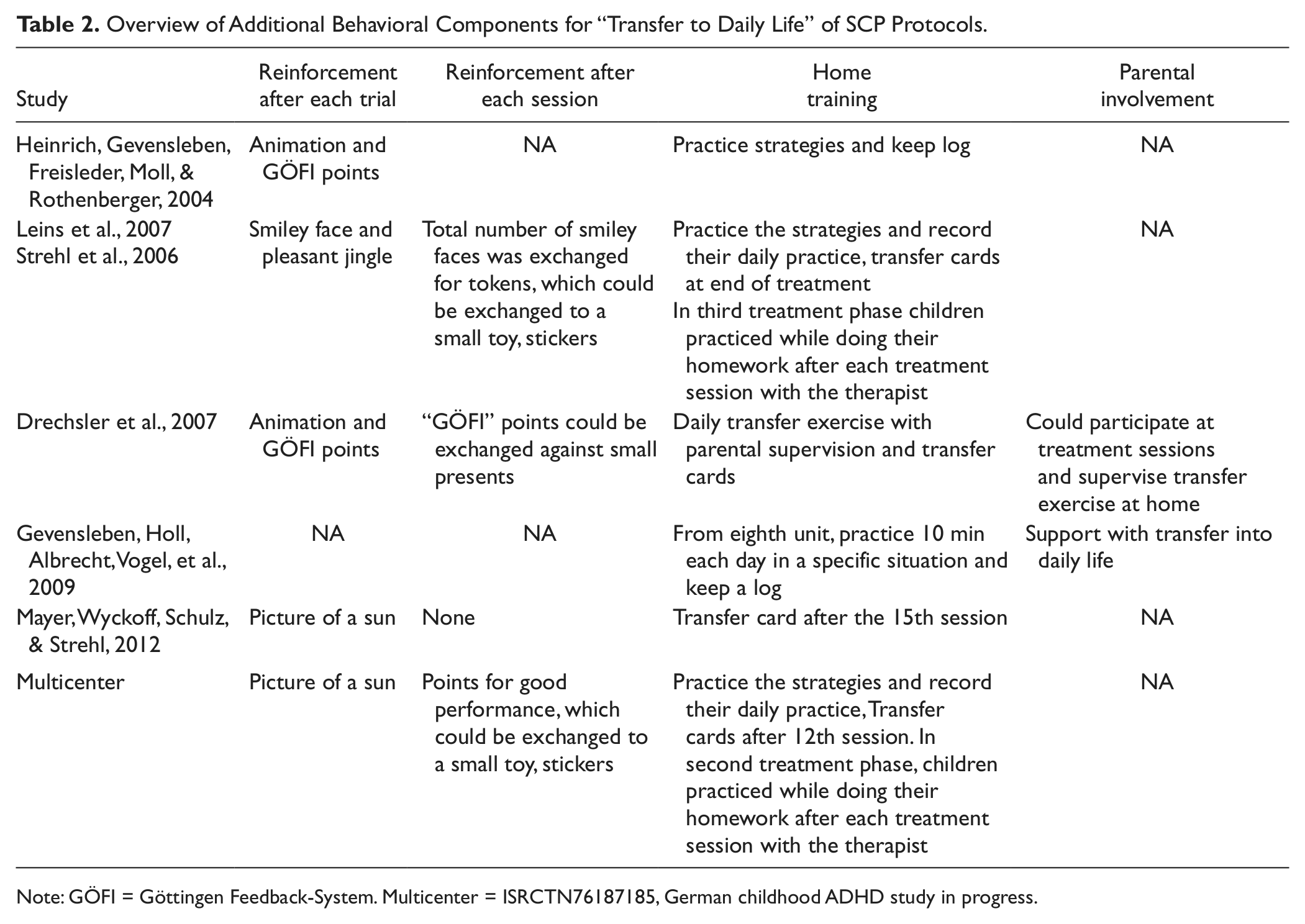
Note: GÖFI = Göttingen Feedback-System. Multicenter = ISRCTN76187185, German childhood ADHD study in progress.
Overview of SCP Feedback Study Design Details.
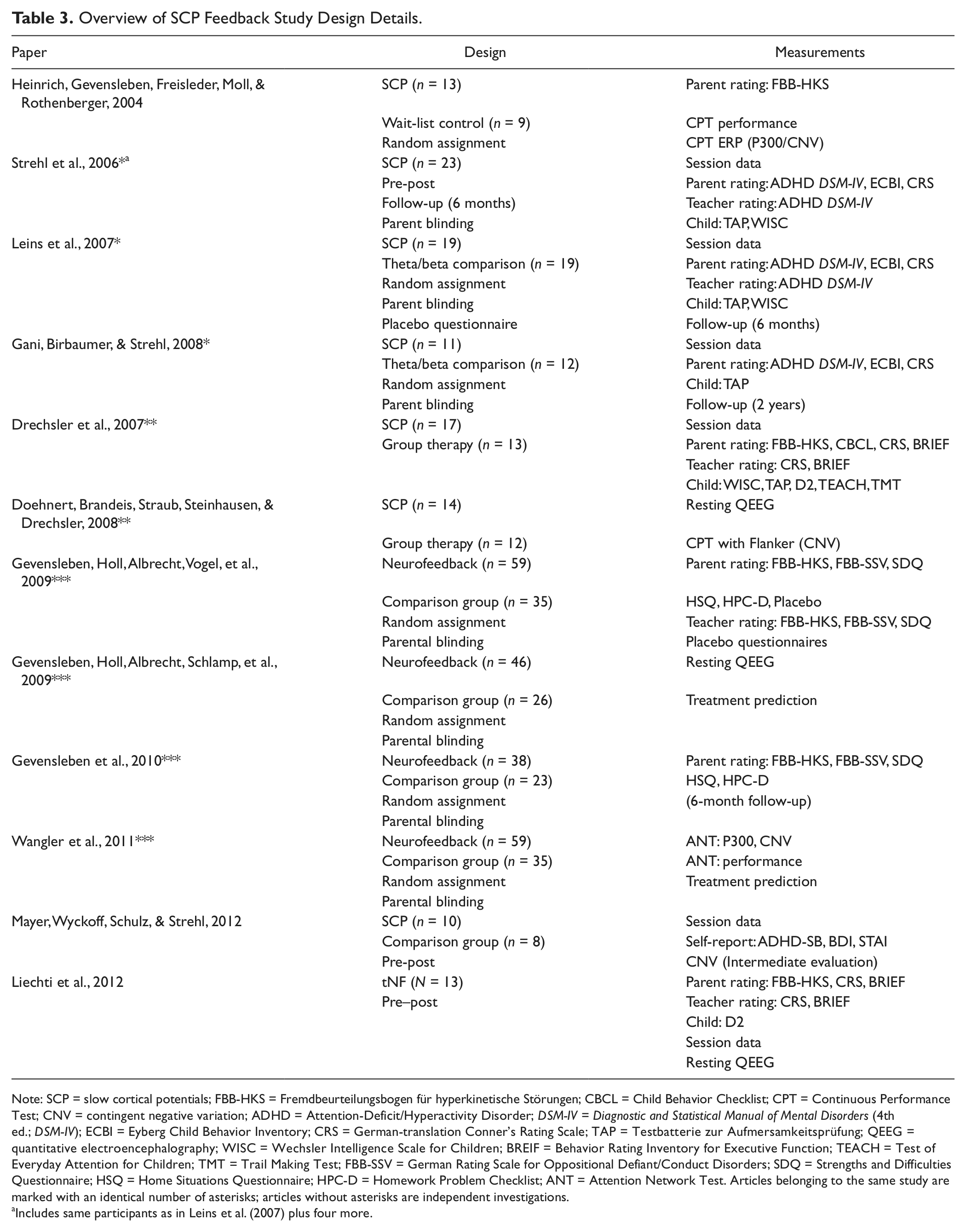
Note: SCP = slow cortical potentials; FBB-HKS = Fremdbeurteilungsbogen für hyperkinetische Störungen; CBCL = Child Behavior Checklist; CPT = Continuous Performance Test; CNV = contingent negative variation; ADHD = Attention-Deficit/Hyperactivity Disorder; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV); ECBI = Eyberg Child Behavior Inventory; CRS = German-translation Conner’s Rating Scale; TAP = Testbatterie zur Aufmersamkeitsprüfung; QEEG = quantitative electroencephalography; WISC = Wechsler Intelligence Scale for Children; BREIF = Behavior Rating Inventory for Executive Function; TEACH = Test of Everyday Attention for Children; TMT = Trail Making Test; FBB-SSV = German Rating Scale for Oppositional Defiant/Conduct Disorders; SDQ = Strengths and Difficulties Questionnaire; HSQ = Home Situations Questionnaire; HPC-D = Homework Problem Checklist; ANT = Attention Network Test. Articles belonging to the same study are marked with an identical number of asterisks; articles without asterisks are independent investigations.
Includes same participants as in Leins et al. (2007) plus four more.
Overview of Significant Results After SCP Feedback for all Described SCP Studies.
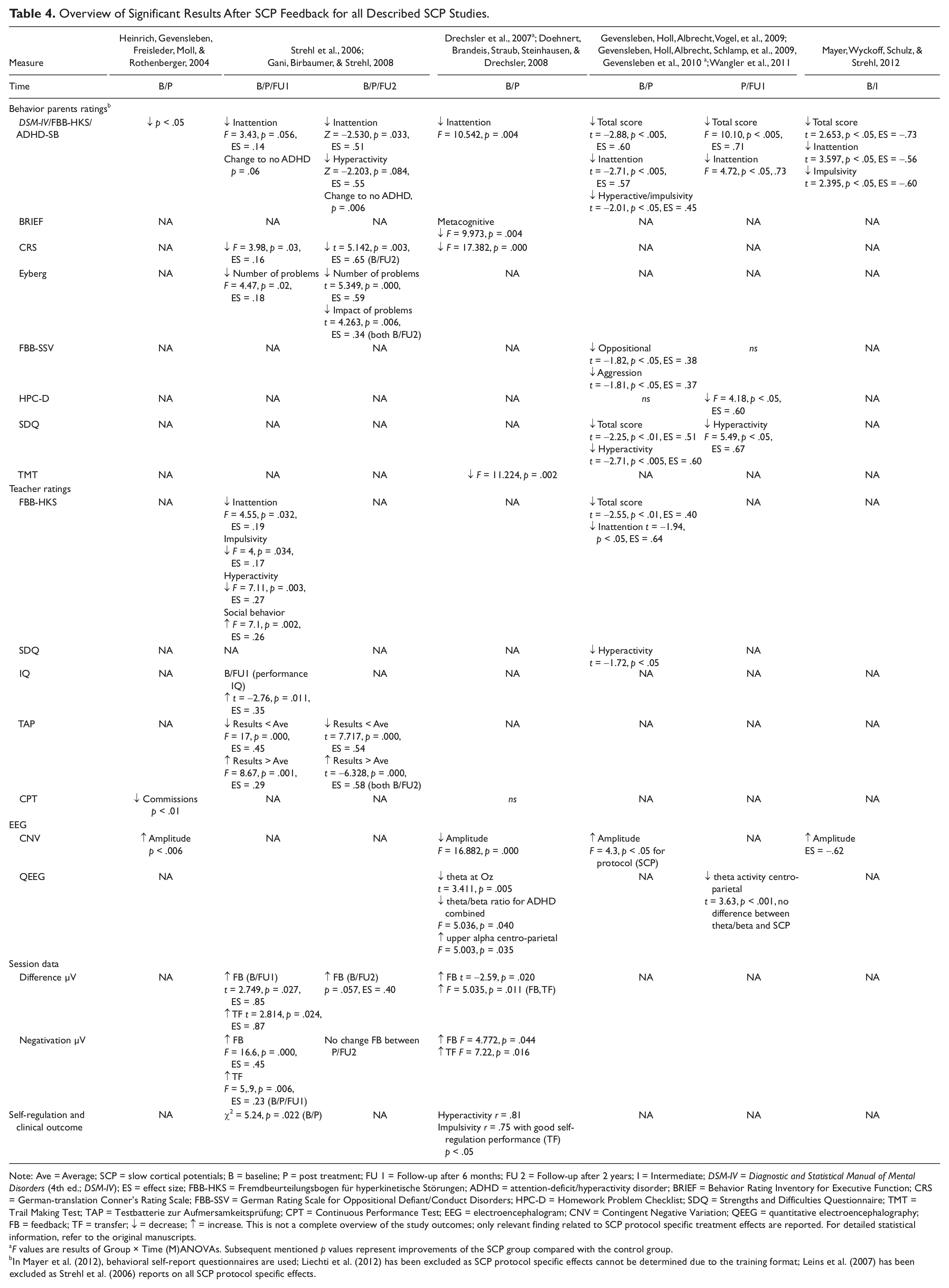
Note: Ave = Average; SCP = slow cortical potentials; B = baseline; P = post treatment; FU 1 = Follow-up after 6 months; FU 2 = Follow-up after 2 years; I = Intermediate; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV); ES = effect size; FBB-HKS = Fremdbeurteilungsbogen für hyperkinetische Störungen; ADHD = attention-deficit/hyperactivity disorder; BRIEF = Behavior Rating Inventory for Executive Function; CRS = German-translation Conner’s Rating Scale; FBB-SSV = German Rating Scale for Oppositional Defiant/Conduct Disorders; HPC-D = Homework Problem Checklist; SDQ = Strengths and Difficulties Questionnaire; TMT = Trail Making Test; TAP = Testbatterie zur Aufmersamkeitsprüfung; CPT = Continuous Performance Test; EEG = electroencephalogram; CNV = Contingent Negative Variation; QEEG = quantitative electroencephalography; FB = feedback; TF = transfer; ↓ = decrease; ↑ = increase. This is not a complete overview of the study outcomes; only relevant finding related to SCP protocol specific treatment effects are reported. For detailed statistical information, refer to the original manuscripts.
F values are results of Group × Time (M)ANOVAs. Subsequent mentioned p values represent improvements of the SCP group compared with the control group.
In Mayer et al. (2012), behavioral self-report questionnaires are used; Liechti et al. (2012) has been excluded as SCP protocol specific effects cannot be determined due to the training format; Leins et al. (2007) has been excluded as Strehl et al. (2006) reports on all SCP protocol specific effects.
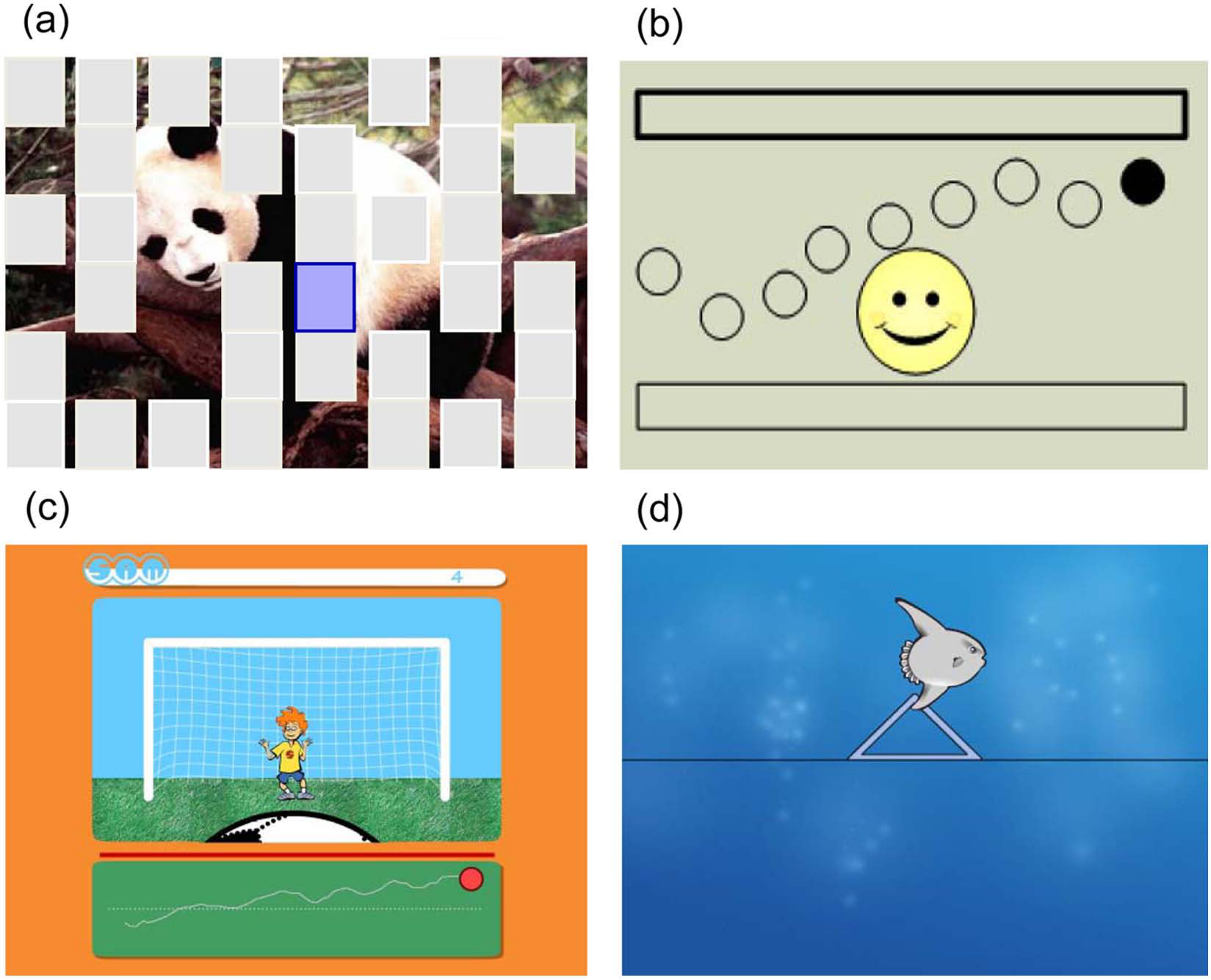
Examples from the different neurofeedback screens used in each program: (a) Neurofeedback program GÖFI—A puzzle piece lights up in white and must be changed to the indicated color (blue for deactivation and red for activation). With successful regulation, the puzzle piece changes to reveal the picture (with kind permission of the Department of Child and Adolescent Mental Health, University Hospital of Erlangen and Studio FILM BILDER, Stuttgart). (b) Neurofeedback program Thought Translation Device—A ball has to be directed to the light up frame, up for activation and down for deactivation. With successful regulation, a smiley face appears. (c) Neurofeedback program SAM—A ball has to be directed to a cued direction, up for activation and down for deactivation. With successful regulation, an animation is played (with kind permission of the Department of Child and Adolescent Mental Health, University Hospital of Erlangen and Studio FILM BILDER, Stuttgart). (d) Neurofeedback program THERA PRAX®—An object has to be directed to the direction the triangle is pointing, up for activation (negative shift of slow cortical potential) and down for deactivation (positive shift of slow cortical potential). With successful regulation, a picture of a sun appears (with kind permission of neuroConn GmbH, Ilmenau).
In a preliminary investigation of SCP feedback, Rockstroh et al. (1990) compared children with and without attention problems on their ability to self-regulate SCP activity. The findings demonstrated that children with attention problems (not ADHD) could learn to self-regulate SCPs during active feedback trials but displayed performance difficulties during transfer trials without continuous feedback, whereas children without attention problems were able to regulate during both conditions. In addition, a global reduction of cortical negativity in anticipation of a task stimulus was observed in children with attention problems, suggesting that performance decrements are related to disengagement of specific cortical networks. Based on these findings, researchers at the University of Göttingen conducted the first investigation of the behavioral and neurophysiological effects of SCP feedback for the treatment of childhood ADHD.
Heinrich et al. (2004) hypothesized that an extended course of SCP feedback would enhance ERP amplitudes, reflecting the build-up of attentional resources, resulting in a reduction of core ADHD behavioral symptoms and improvements on a cued continuous performance test (CPT). To test this theory, 22 children aged 7 to 13 years diagnosed with ADHD (Diagnostic and Statistical Manual of Mental Disorders [4th ed.; DSM-IV; American Psychiatric Association, 1994]) were randomly assigned to a wait-list control group (n = 9) or 25 sessions of SCP feedback (n = 13; see Tables 1-3). The SCP and wait-list group were comparable on all measures pretreatment. The SCP neurofeedback group demonstrated a significant reduction in parent-rated ADHD behavioral symptoms, fewer impulsivity errors on the CPT, and increased CNV activity post-treatment, whereas the wait-list control group did not differ across the treatment period (see Table 4). Heinrich and colleagues concluded that behavioral and neurophysiological improvements were the result of newly acquired SCP self-regulation skills rather than practice effects.
Expanding on the hypotheses and study outcomes of Heinrich et al. (2004), Gevensleben, Holl, Albrecht, Vogel, et al. (2009) investigated the efficacy of neurofeedback (combined: SCP and theta/beta protocols) compared with computerized attention skills training (AST). With a primary goal of controlling for unspecific effects and confounding variables, 102 children aged 8 to 12 years diagnosed with ADHD (DSM-IV) were randomly assigned to 35 sessions of neurofeedback (n = 59) or AST (n = 35). No significant pretreatment differences were observed for age, sex, IQ, ADHD subtype, medication, or comorbid disorders. Parents were blind to treatment group assignment. The treatment protocol for both groups consisted of two treatment phases of nine double sessions. For the neurofeedback group, treatment consisted of balanced phases of SCP and theta/beta protocols, whereas the control group completed two phases of the AST protocol. All participants were required to practice protocol specific strategies for improving focus and attention at home and during different cognitive tasks (see Table 2). Treatment outcomes were assessed through behavioral questionnaires and neurophysiological testing (EEG, ERP) collected pre-treatment, mid-treatment, and post-treatment. In general, the results indicated that neurofeedback and AST had positive effects on parent- and teacher reports Gevensleben, Holl, Albrecht, Vogel, et al. (2009). However, neurofeedback had statistically significant superior improvements on the German ADHD behavioral parent-rating scale (Fremdbeurteilungsbogen für hyperkinetische Störungen [FBB-HKS]) total score, inattention, and hyperactivity/impulsivity as well as significant reductions in oppositional behavior, delinquent and physical aggression, and the strength and difficulties questionnaire (SDQ) total score and hyperactivity (see Table 4). Treatment response was defined as a 25% reduction in the primary outcome measure (FBB-HKS total score). Analysis indicated that children in the neurofeedback group (51.7%) had a superior response rate as compared with children in the AST group (28.6%). Investigations of differences in behavioral outcomes for SCP and theta/beta protocols indicated comparable improvements in the FBB-HKS total score and subscales for inattention and hyperactivity/impulsivity.
The stability of behavioral improvement was assessed at a 6-month follow-up for neurofeedback (n = 38) and control (n = 23) participants (Gevensleben et al., 2010). Overall, behavioral outcomes persisted or incurred additional gains for both groups. At follow-up, 50% of children in the neurofeedback groups were identified as treatment responders, whereas 30.4% of AST participants met this criterion (see Table 4). Improvements on the ADHD-related behavior remained superior for the neurofeedback group.
To assess the impact of neurofeedback (n = 46) and AST (n = 26) on resting state EEG, Gevensleben, Holl, Albrecht, Schlamp, et al. (2009) analyzed 3 min of data collected during an eyes-open condition recorded from 23 electrode sites pre-treatment, mid-treatment, and post-treatment. No significant differences in frequency band activity or theta/beta ratio were observed between the neurofeedback and AST control group pre-treatment. Pre–post changes indicated a significantly larger reduction of centro-parietal theta activity in the neurofeedback group compared with AST. No significant differences in frequency activity were found between the SCP and theta/beta protocols.
EEG predictors of behavioral outcome were assessed using linear regression analysis, indicating no significant predictor variables for combined neurofeedback but several predictors for theta/beta, SCP, and AST protocols independently. For example, following the SCP protocol, changes in the FBB-HKS total score were predicted by lower pre-treatment left-parietal alpha, whereas improvements on the hyperactivity/impulsivity subscale of the FBB-HKS were predicted by lower pre-treatment left-parietal alpha activity and greater posttreatment increases of central-midline alpha. For the AST group, improvements on the hyperactivity/impulsivity subscale of the FBB-HKS were correlated with increased beta activity over parietal-midline electrode sites.
The effects of neurofeedback (n = 59) and AST (n = 35) interventions on cognitive processing were investigated by Wangler et al. (2011) using the Attention Network Test (ANT; Neurobehavioral Systems, Albany, CA, USA) to elicit CNV and P3 activity for analysis (see Table 3). Following treatment, all performance measures improved significantly; however, no significant Time × Group effects were observed (see Table 4). In line with the study hypothesis, ERP analysis indicated that the neurofeedback group had a significant posttreatment increase in CNV activity at Cz compared with AST. Analysis of individual protocols indicated the CNV increase because of the SCP protocol, as amplitudes did not change following the theta/beta protocol. For the cue-P3 activity at Pz, a Group × Cue × Time interaction was observed, indicating that the neurofeedback group had a significantly increased activity during neutral cues but decreased during special cues, compared with AST; however, no neurofeedback protocol specific effects were observed. Finally, for the SCP protocol, pretreatment CNV activity during special cue trials was predictive of improvements on the FBB-HKS.
To demonstrate whether children with ADHD could learn self-regulation of neurofeedback parameters, researchers at the University of Tübingen (Leins et al., 2007; Strehl et al., 2006) for the first time analyzed session data to investigate differences in signal amplitude for task (activation/deactivation), condition (feedback/transfer), and time (baseline/post-treatment/follow-up) in a design with two active treatments. Children aged 8 to 13 years diagnosed with ADHD (DSM-IV) were randomly assigned to 30 sessions of SCP (n = 19) or modified theta/beta (n = 19) neurofeedback. To allow a blind design, theta/beta feedback was scheduled according to the SCP protocol. In addition to increasing beta and inhibiting theta, the children had to regulate the opposite—inhibiting beta and increasing theta—and the trial duration was only 10 s. Another new component of treatment was the introduction of a 4- to 6-week treatment break with “homework” sessions. Homework sessions required participants to practice self-regulation strategies used to produce activation in problematic situations and on a daily basis using a “transfer card” (laminated card of the protocol screen) to help generalize treatment effects (see Table 2). Participants, parents, and teacher were blind (in the sense of not being informed by the investigator) to group assignments and matched for age, sex, IQ, diagnosis, and medication. The results indicate that SCP and theta/beta neurofeedback groups had significant cognitive and behavioral improvements following treatment and demonstrated that children were able to learn self-regulation of protocol specific components (see Table 4). Therefore, only changes observed in the SCP feedback group will be discussed in detail.
The neurophysiological and psychometric outcome data for the SCP group presented by Leins et al. (2007) was already reported by Strehl et al. (2006) with the addition of four participants (n = 23). Throughout treatment, participants developed the ability to produce SCP shifts in the desired direction during feedback and transfer trials. The increased ability to produce SCP shifts in the negative direction during transfer trials significantly correlated with symptom reduction post-treatment. Parents’ ratings indicated significant improvements for behavioral problems and ADHD symptoms, and teacher rated reduced inattention, hyperactivity, impulsivity, and improved social behavior on DSM-IV questionnaires (see Table 4). In addition, enhanced performance IQ scores, as well as improved performance on subtests of the attention test “Testbatterie zur Aufmersamkeitsprüfung” (TAP) were reported. The within ESs reported for behavior, attention, and IQ changes were moderate to high and were stable 6 months after the end of treatment.
Finally, the Tübingen group was the first (and until now the only) group who investigated the stability of self-regulation skills, as well as behavioral and attentional improvements 2 years after the end of treatment (Gani, Birbaumer, & Strehl, 2008). Of the 23 SCP participants included in the initial study, 11 children participated in a follow-up investigation that included three additional SCP feedback sessions, parent ratings, and completion of the TAP (see Table 3). “Lack of time” was reported by parents as the main factor for nonparticipation. Results indicated that differences between activation and deactivation tasks increased over time during the feedback condition. A significant interaction of Time × Task for the feedback condition was observed. The amplitude gains in negativity observed post-treatment were maintained at 2-year follow-up. Parent ratings indicated significant improvements in ADHD symptoms below cutoff values as well as decreased frequency and impact of behavioral problems from baseline to follow-up. Performance on the TAP subscales indicates additional significant improvements. As TAP raw scores are transformed to age corrected percentiles all gains cannot be explained by maturation.
Two current projects at the University of Tübingen focus on the comparison of SCP feedback with other treatment modalities and for application with individuals in an expanded age range. In collaboration with research teams in Göttingen, Frankfurt, Mannheim, and Hamm, a multicenter randomized controlled clinical trial (ISRCTN76187185) is underway to examine the efficacy of SCP feedback compared with electromyogram (EMG) feedback. In total, 144 children aged 7 to 9 years diagnosed with ADHD (DSM-IV) will be randomly assigned to a treatment condition. Parents are blind to group assignment in terms of not informed. Cognitive and neuropsychological pre-testing is conducted without medication, including acquisition of resting state EEG, ERP, and CPT data. Once medication is resumed (2-4 week titration), participants will complete 25 sessions of assigned feedback within a 3-month period (see Table 1). Following completion of the SCP sessions, a posttreatment assessment will be conducted under medication and repeated again following a 2- to 4-week medication washout. After this evaluation, patients are allowed to reduce or stay without medication if they want to. Finally, following a 5-month break, stability of treatment effects (self-regulation skills, behavioral changes, EEG/ERP/CPT changes) will be reassessed.
In the second investigation, the efficacy of SCP feedback as a treatment for adults with ADHD is under examination. In total, 21 participants aged 22 to 66 years diagnosed with ADHD (DSM-IV) will complete 30 sessions of SCP feedback. For protocol and design details, see Tables 1 and 2. Assessment points are conducted pre-treatment, mid-treatment, post-treatment, and at 6-month follow-up. Planned analyses include investigation of IQ matched healthy controls. Mayer et al. (2012) reported preliminary results of this investigation following 15 SCP sessions. The results indicated significantly reduced CNV amplitudes for adults with ADHD compared with healthy control participants at baseline (see Table 4). Following the initial 15 SCP sessions, significant improvements on the ADHD questionnaire total score and the inattention and impulsivity subscales were reported, as well as trends toward CNV amplitude increase after 15 sessions.
The third work group at the University of Zürich, Drechsler et al. (2007) for the first time investigated the efficacy of SCP feedback compared with a behavioral group therapy program. Children aged 8 to 13 years diagnosed with ADHD (DSM-IV) were assigned to either thirty 45-min SCP sessions (n = 17) or fourteen to fifteen 90-min sessions of cognitive-behavioral-based group therapy (n = 13). The groups were not randomly assigned but showed no significant differences related to gender, age, IQ, ADHD diagnosis, medication, or symptoms of the Child Behavior Checklist were reported pre-treatment. However, participants of the SCP group turned out to be more impaired on the Behavioral Index of the Behavior Rating Inventory for Executive Functions (BRIEF) according to teacher ratings.
For the SCP protocol, electrode placement and positivation/negativation task randomization was similar to the procedure described above by Heinrich et al. (2004). However, the treatment protocol detailed by Drechsler et al. (2007) was designed more intensive and included more transfer tasks (Tables 1 and 2). Unlike other SCP studies, parental involvement and compliance with homework session supervision were explicitly asked for and assessed via phone/email contact. The group therapy sessions were conducted 1 to 2 days a week in small groups of five to six children. The therapy program focused on self-management, enhanced self-awareness, and development of social and meta-cognitive skills. Parent involvement of children assigned to the group therapy condition was assessed based on the frequency of participation in treatments, but was not comparable with the SCP group, as home support could not be assessed.
Outcome variables included baseline and post-treatment behavioral assessments, measures of attention and neurophysiologic recordings (see Table 3). Drechsler et al. (2007) reported that the SCP group improved significantly on inattention scores of the FBB-HKS and Metacognitive Index of the BRIEF, whereas participants in group therapy did not show significant improvements (see Table 4). Assessment of teacher ratings indicated that children in the SCP group had significantly greater impairment before and after treatment, but reported improvements in cognitive performance as more pronounced following neurofeedback compared with group therapy. Both groups showed improvement in attention variables over time (see Table 4). Group differences revealed that although commission errors reduced over the course of treatment, the SCP group made significantly more commission errors than the group therapy participants did pre-treatment and post-treatment. The overall within-group ESs of the attention parameters revealed moderate to large ESs for neurofeedback and small to moderate effects for group therapy. Finally, high level of parental support during the homework phase with the transfer card exercises was significantly correlated with the reduction of inattention scales of the FBB-HKS (parent ratings) and the Conners’s Rating Scale (CRS) Global Index (teacher ratings).
Investigation of session data for the SCP group revealed a significant increase in the mean amplitude of negativity trials during feedback and transfer trials, as well as increased task differentiation during feedback sessions over the course of treatment. In a secondary investigation of this sample, Doehnert, Brandeis, Straub, Steinhausen, and Drechsler (2008) analyzed pre- and posttreatment EEG data collected from participants in the SCP group (n = 14) and the group therapy treatment (n = 12). EEG data were collected from 46 electrodes during a 3-min eyes-closed resting state condition and CPT (Heinrich et al., 2004) with flanker task variation.
Analysis indicated no pretreatment group differences and no significant changes in resting state EEG activity (Doehnert et al., 2008). No Group × Time interactions were observed for theta/beta ratio or theta band activity at Cz (see Table 4). Post-training, participants in the SCP subgroup with combined type ADHD showed significant reductions in theta/beta ratio, and explorative analysis indicated a significant reduction of core theta power (4-6 Hz) at Oz and increase of upper alpha (10-12 Hz) band activity over central and parietal sites for the overall SCP group. Against expectations, significant CNV amplitude reductions were observed in both CPT variations and treatment groups. Doehnert et al. (2008) reported only minor changes in CPT performance. No significant interactions or correlations were observed between parental support and changes in EEG, CNV, or CPT measures. Several correlations between resting state EEG changes and improvements on behavioral questionnaires were reported for the participants in the SCP group.
The most recent study conducted by researchers at the University of Zürich focused on the effects of tomographic neurofeedback (tNF) as a treatment for childhood ADHD (Liechti et al., 2012). The assumption was that a direct control of structures, like the anterior cingulate cortex (ACC), which are related to the symptoms of ADHD, could be achieved. In a blind pre–post design randomized controlled clinical trial, children aged 8.5 to 13 years with diagnosed ADHD (DSM-IV) were assigned to one of three treatment groups using tNF, standard NF, or EMG biofeedback. The tNF protocol focused on regulation of bidirectional SCP and theta/beta-ratio activity in the ACC and included activation/deactivation trials, feedback, delayed feedback, and transfer conditions. For both tNF protocols, feedback parameters were acquired from a voxel of the ACC computed using the inverse solution (sLORETA) of 30 channels of scalp EEG activity. Pre- and posttreatment evaluations were conducted, including resting state EEG (eyes-open, eyes-closed), cued CPT flanker tasks (CNV, P3a, P3b), and psychometric testing. Liechti et al. (2012) concluded that behavioral improvements after the tNF seem to be comparable with improvements after previously reported classical neurofeedback. Analysis of pre–post changes in ERP parameters indicated significant increases in posterior cuedP3b and NoGo P3a activity, global field power, and CNV negativity of right frontal electrodes. No changes specific to the ACC were observed. However, normalization of ACC activity toward the group mean was significant for theta and beta activity at the participant level. Analysis of resting state EEG activity pre- and post-treatment did not reveal any significant changes to the target frequency parameters. The performance data during the tNF showed that participants scarcely learned to control their ACC activity through SCP and theta/beta tNF. Some learning in subgroups and subcomponents was observed but will not be described further. In summary, after 36 sessions of tNF of the ACC, Liechti et al. (2012) found clinical improvement of ADHD symptoms as well as changes in the resting EEG and ERP without substantial learning of cortical control.
Design Critique and Study Limitations
The body of research dedicated to investigating the clinical effects of SCP neurofeedback as a treatment for ADHD has developed over the last decade. From the exploratory investigations of SCP regulation in an “attention impaired” population (Rockstroh et al., 1990) to the current multicenter single-blind randomized controlled clinical trial (ISRCTN76187185) targeting SCP treatment effects in a DSM-IV diagnosed ADHD population, SCP investigations have utilized a variety of study designs and analysis methods. Although the majority of SCP research studies have been designed to circumvent weaknesses identified in early neurofeedback studies, limitations have been identified. Loo and Barkley (2005) updated and expanded on the methodological shortcomings of the first wave of neurofeedback studies, reporting flaws related to lack of control groups, limited placebo control, presence of confounding variables, small groups designs, inadequate diagnostics, no evaluator blinding, and lack of randomization have persisted.
As indicated in the research review, SCP studies have addressed a majority of the complaints highlighted by Loo and Barkley (2005). SCP research studies utilized passive or semi-active/active controls groups such as a wait-list control (Heinrich et al., 2004), EMG biofeedback (in progress: multi-center RCT [ISRCTN76187185]; Liechti et al., 2012), theta/beta neurofeedback (Gevensleben, Holl, Albrecht, Vogel, et al., 2009; Leins et al., 2007), cognitive training (Gevensleben, Holl, Albrecht, Vogel, et al., 2009), group therapy (Drechsler et al., 2007), as well as pre–post designs (Liechti et al., 2012; Mayer et al. 2012; Strehl et al., 2006) and long-term follow-up (Gani et al., 2008; Gevensleben et al., 2010; Leins et al., 2007). Blinding of participants and their parents was included in the design of most studies (see Table 3), but it remains unclear how well it could be maintained during the process of treatment. Evaluator blinding was used in a majority of the controlled SCP studies (Gevensleben, Holl, Albrecht, Vogel, et al., 2009; Leins et al., 2007; Liechti et al., 2012; in progress: multicenter RCT [ISRCTN76187185]), as well as parent (Drechsler et al., 2007; Gevensleben, Holl, Albrecht, Vogel, et al., 2009; Leins et al., 2007; in progress: multicenter RCT [ISRCTN76187185]), child (Liechti et al., 2012), self-report (Mayer et al., 2012), and spouse (Mayer et al., 2012) expectancy/satisfaction placebo control questionnaires. All investigations utilized a prospective research design, included research participants rather than private-pay clients, and required DSM-IV-based ADHD diagnosis and minimal comorbidities. In addition, care was taken to minimize confounding variables through randomization of participants (Gevensleben, Holl, Albrecht, Vogel, et al., 2009; Leins et al., 2007; Liechti et al., 2012; in progress: multicenter RCT [ISRCTN76187185]), use of matched healthy controls (Mayer et al., 2012), and baseline assessments to determine age, gender, IQ, medication, diagnostic, and performance differences between groups. Finally, study tasks were designed to limit differences in treatment duration, parent and therapist involvement, and research environment.
Despite these design improvements, recent studies continue to receive critical reviews. Lofthouse, Arnold, Hersch, Hurt, and DeBeus (2012) criticized Leins et al. (2007) for lack of therapist/evaluation blinding or sham control group. In addition, they were critical of further improvements observed from post-treatment to 6-month follow-up, citing a lack of control or measurement of potential confounds and the possibility of non-specific factors. In review of Gevensleben, Holl, Albrecht, Vogel, et al. (2009), Lofthouse et al. (2012) again cited lack of complete blinding and possible confounds related to the use of theta/beta and SCP protocols on the same participants. In review of neurofeedback RCT limitations, the author concluded that triple blinding was largely limited in previous studies, as neurofeedback technology required the oversight of a clinician to establish protocols and settings. They report advancement in the field has led to the development of systems that may be programmed to provide sham feedback contingent on a participants EEG, allowing trainer blinding. The standardized feedback, bidirectional relative baseline/threshold procedure, and discrete reward/reinforcement of SCP might permit treatment session to be completed without the constant adjustment of the feedback by the clinician. This feedback design could reasonably be applied to other frequency bands or frequency ratios (Leins et al., 2007; Liechti et al., 2012) allowing for a triple-blind design. However, it is of interest to note that Gevensleben, Holl, Albrecht, Vogel, et al. (2009) evaluated their double-blinding strategies and found that parents were able to determine treatment assignment of their children beyond chance level (neurofeedback: 58%, attention training: 63%). With regard to the issue of sham control, Lofthouse et al. (2012) again assert that technological limitations have made the development of a “true” and “valid” sham difficult and limit the ability of researchers to adequately control for all nonspecific effects. Conversely, Gevensleben, Rothenberger, Moll, and Heinrich (2012) assert that inclusion of a sham or placebo control group may lead to diminished effects, motivation reduction, and impaired outcomes, as the impression of “uncontrollability” during the initial learning phase of neurofeedback may be misattributed to placebo group assignment. Finally, possible confounds related to the assignment of multiple neurofeedback protocols to the same participant group by Gevensleben, Holl, Albrecht, Vogel, et al. (2009) were limited through the use of a counterbalanced cross-over design. The total neurofeedback group consisted of two thirds of the study population allowing for the investigation of a combined neurofeedback treatment, as well as investigation of protocol specific effects.
The issue of specific and nonspecific effects of SCP feedback requires additional discussion. A recent meta-analysis (Arns et al., 2009) and review (Lofthouse et al., 2012) of neurofeedback (all protocols) for the treatment of childhood ADHD have discussed the guidelines for defining empirically supported therapies (Chambless & Hollon, 1998). Arns et al. (2009) assert that neurofeedback should be classified as “Efficacious and Specific” due to the series of randomized control trials and moderate to large ESs for reductions in core ADHD symptoms. However, Lofthouse et al. (2012) disagree with this evaluation and assert that neurofeedback should be regarded as “Efficacious” and is in need of additional randomized control trials, sham controls, and triple blinding. However, these guidelines have not been applied specifically to SCP neurofeedback. For the classification of an intervention as “Efficacious,” La Vaque et al. (2002) identified six key criteria, including (a) a randomized control trial comparison with a no-treatment control, alternative treatment group, sham condition that yields significantly superior/equivalent effects; (b) investigation of a specific (diagnosed) population; (c) use of validated measures; (d) appropriate data analysis; (e) study parameters are replicable; and (f) statistically superior/equivalent effects have been shown in two independent trials research settings.
In relation to variables (a) and (f), a variety of primary and secondary treatment effects has been reported following a course of SCP feedback, including moderate to large ESs for the reductions of core ADHD symptoms assessed by parents and teachers as compared with wait-list control (Heinrich et al., 2004), theta/beta feedback (Leins et al., 2007), AST (Gevensleben, Holl, Albrecht, Vogel, et al., 2009), and group therapy (Drechsler et al., 2007). In addition, superior effects have been observed in CPT (Heinrich et al., 2004), ERP (Heinrich et al., 2004; Wangler et al., 2011), and resting-state-EEG (Doehnert et al., 2008) analyses. Furthermore, SCP specific predictors have been identified and correlated with enhanced treatment outcome and symptom reduction (Gevensleben, Holl, Albrecht, Schlamp, et al., 2009; Leins et al., 2007; Strehl et al., 2006; Wangler et al., 2011). Variables (b) through (e) have also been met as all SCP studies have an identified study population, inclusion/exclusion criteria, valid diagnostic and assessment questionnaires, sound statistical analysis, and supplementary information detailing study parameters and procedures. To meet the criteria for an “Efficacious and Specific” classification, variables (a) through (f) need to be met, with the addition of the treatment showing statistically superior effects in two comparisons with a credible sham, medication, of bona fide alternative treatment. Based on these criteria, SCP feedback should be recognized as an “Efficacious” treatment for ADHD. To move toward classification as an “Efficacious and Specific” treatment, future studies should focus on the identification of a sensible sham control, as well as the comparison of SCP feedback to stimulant medication. Due to the mixed results related to parental support (Drechsler et al., 2007; Gevensleben, Holl, Albrecht, Vogel, et al., 2009; Leins et al., 2007), additional efforts should be made to control for parental expectancy/satisfaction via participant and examiner blinding and placebo questionnaires.
Discussion
Albeit the design and research discussions and shortcomings, all studies showed improvements after SCP feedback on behavioral outcome data with symptom reductions above 25%. Moderate to high within ESs were found on inattention, impulsivity, and on hyperactivity, in that order, measured with questionnaires and rating scales, as well as objective tests like TAP, CPT, or D2. Analysis of training data revealed advances in self-regulation of SCP, during feedback as well as during transfer trials. The outcome of the electrophysiological data was variable but also rather diverse, which highlights a need for more research to support results for EEG, ERPs, and EEG-session data.
All studies were designed to meet the majority of the standards required by the research community (Holtmann & Stadler, 2006; Loo & Barkley, 2005; Sherlin, Arns, Lubar, & Sokhadze, 2010) and used a similar almost standardized protocol for SCP feedback which will be discussed in the following. The protocols used a rather monotone feedback modality, which required bidirectional up or down movement of an object or an indicated change of color of an object. SCP feedback was discontinuous, recorded at Cz, referenced to one or both mastoids, and included transfer trials.
The study by Liechti et al. (2012) used tNF for the first time. They assumed that a direct control of structures, like the ACC, which are related to the symptoms of ADHD, could be achieved. There are still some difficulties in the realization of this approach. Therefore, no conclusions can be drawn if such a complex technique is profitable compared with the traditional treatment. Based on its novelty and difficulties, this study will not be included in the further discussion.
SCP Feedback Protocols
The SCP feedback protocols varied with regard to the neurofeedback system used, the number of trials, the density of treatment sessions, and the additional behavioral therapy components. The amount of trials during one session ranged from 70 to 160 and the density of treatment ranged from one to two sessions a week to five double sessions per week. At this point, it could only be speculated if one or another leads to better or worse effects.
Just looking at the neurofeedback component, SCP neurofeedback appears to be a standard “one size fits all” protocol unlike the variety of frequency feedback protocols, which differ in feedback frequency bands, definition of each frequency band, threshold setting, choice of electrode sites, and feedback modalities, which, depending on the used system, can be overwhelmingly diverse for the neurofeedback therapist and patient (Loo & Barkley, 2005). Usually, frequency neurofeedback is designed with more exciting feedback animations like video games, music, or movies compared with the rather monotone SCP animations (see Figure 1a-1d). In regard to learning principles, if a feedback animation is too exciting and thrilling, it might create a stimulus-reinforcer association instead of a response-reinforcer association, which means that the participants will associate the reinforcement with the stimulus rather than the desired brain activity (Sherlin et al., 2011). Another argument for the rather monotone SCP feedback protocol is the fact that people with ADHD often have the worst attention problems in situations, which are boring and monotone. If people with ADHD are highly interested in a task, the attention problem diminishes. Therefore, training in low-stimulus surrounding attacks their main area of difficulties and therefore neurofeedback should be rather monotone to train them in their problem situation. This can be achieved for SCP, as well as frequency neurofeedback. However, people with ADHD have a great need for motivation and reinforcement, which will be addressed later.
The most diversity between the SCP protocols reviewed was observed in the additional behavioral therapy components implied in the sessions (see Table 2). The reviewed studies with children always implemented a token system and transfer to daily life situations. The study by Drechsler et al. (2007) used extended support from the parents for the daily transfer, all other studies kept the parents rather uninvolved. The transfer into daily life showed the most diversity. It ranged from only handing out transfer cards and the instruction to practice regulation at home, to sitting down and guiding the children into an activated state during their homework or other tasks. This component seems to be an important tool for application of the learned self-regulation into daily life, be it monitored by parents or by the children on their own.
A major difference in the study in adult ADHD by Mayer et al. (2012) is that they did not use any kind of token reinforcement system within or over all sessions. As Siniatchkin, Kropp, and Gerber (2000) described, reinforcement is less important for adults than for children. However, because ADHD is described as a motivation deficit disorder (Barkley, 2006) in which people with ADHD need a constant motivation from the therapist, reinforcement over the sessions should be considered. However, there were no dropouts in that study, which suggests a sufficient self-motivation in that group of adults with ADHD.
The motivating component of all protocols was the reward at the end of each trial, the verbal feedback from the therapist, and for all but the adult study, a token system. An advantage of SCP feedback over frequency feedback protocols might be the possibility to give verbal feedback and motivation from therapist after each 8- to 10-s trial. This might be better than irregular and less specific feedback during the continuous frequency feedback. The immediate reward creates a more consistent association between behavior (successful negativation or positivation) and reinforcement. This is also recommended by Sherlin et al. (2011) who stated that a discontinuous neurofeedback should achieve better results than continuous neurofeedback.
Electrophysiological Parameters
All studies found main or secondary effects of SCP neurofeedback on relevant EEG and ERP parameters. Changes were mainly observed on CNV, but also for EEG parameters that are primarily known to change with theta/beta feedback, such as P300 (Egner & Gruzelier, 2001, 2004; Lazzaro, Gordon, Whitmont, Meares, & Clarke, 2001) and theta/beta ratio (Monastra, Monastra, & George, 2002). In regard to the changes in the P300 after SCP feedback, a study by Ergenoglu et al. (1998) with healthy controls found a general relationship between negative SCP shifts and an increased P300 amplitude in an ERP experiment. This underlines that SCP feedback increases the ability to negativate in an attention-requiring task.
SCP feedback and frequency feedback may target the same attention network. Frequency feedback targets the tonic aspect of arousal, whereas SCP feedback targets the phasic regulation of excitability (Gevensleben et al., 2012; Rockstroh et al., 1990). It is likely that both treatments affect overlapping networks for activation and state regulation. Although SCP feedback seems to have a general influence on changes in brain activity, like CNV, P300, and alpha and theta/beta ratio, it could not be observed whether successful frequency feedback also improves SCP-related EEG markers of attention.
From early research on, SCPs have been described as a phasic tuning mechanism in the regulation of attention (Rockstroh et al., 1990). Recent research has extended this view as they found a relationship between the blood oxygen level dependency signal in functional magnetic resonance imagery research and SCPs (He, Snyder, Zempel, Smyth, & Raichle, 2008). In this context, the role of SCPs and consciousness has been discussed (He & Raichle, 2009). The relationship between SCPs and consciousness is currently not fully understood but interesting linkages were found. In an integrated information theory of consciousness, Tononi (2004) claims that integration of different information is essential for one’s own experience. Therefore, on a fundamental level, consciousness can be defined as integrated information. The main direct generators of SCPs are long-range intracortical and feedback cortico–cortico connections, as well as nonspecific thalamic inputs. All these different inputs present integration of information from different parts of the brain. It is concluded that SCPs might carry large-scale information integration in the brain that contribute directly to the emergence of conscious awareness (He & Raichle, 2009). Regarding the widespread generation of SCPs, it might be concluded that SCP feedback influences these inputs and therefore the underlying brain activities. This might be reflected in modified information integration and thereby influences consciousness. The relationship has not been investigated yet, but future research might yield interesting perspectives regarding the relevance of SCP feedback.
Conclusion
The results of the reviewed studies showed consistent behavioral improvements and with the exclusion of one study, also for electrophysiological outcomes after SCP feedback. Participants learned to self-regulate their brain activity and the ability to self-regulate served as a predictor of clinical outcome.
The “one size fits all” protocol has several advantages. First, it led to a consistent well-defined research protocol, making the reviewed studies and outcomes comparable and replicable for future research. Second, it is designed to optimize the principles of learning and operant conditioning. Finally, this type of protocol is easy to follow for practitioners in daily clinical application.
SCP feedback has an excellent chain of research that needs to be followed. Currently, the body of SCP feedback research lacks a medication or sham control comparison needed for classification as an “Efficacious and Specific” treatment modality. Additional investigations are needed to answer questions about the specificity of neurofeedback treatment, the number and frequency of sessions needed to maximize clinical effects, and in terms of clinical application, individualization of treatment regarding learners and non-learners. Some of these questions are currently under investigation, but future studies are still needed. In addition, an in-depth comparison between frequency and SCP neurofeedback should be addressed in future research studies and reviews.
Footnotes
Authors’ Note
Kerstin Mayer and Sarah N. Wyckoff contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deutsche Forschungsgemeinschaft (DFG HO2503 4/1) and Bundesministerium für Bildung und Forschung (BMBF01GQ0831).