
Abstract
Until recently, ADHD had been diagnosed and treated primarily as a childhood condition (Kooij et al., 2010). Research from a variety of disciplines has examined the impact of childhood ADHD on subsequent social, emotional, and functional outcomes for this population (Kerig & Wenar, 2006). Studies have invariably concluded that ADHD places children at significant risk for several negative outcomes across a variety of domains. Children with ADHD are at increased risk for developing comorbid psychological disorders, most frequently oppositional defiant disorder (ODD) and conduct disorder (CD; Fischer, Barkley, Smallish, & Fletcher, 2002), as well as anxiety (Milich, Balentine, & Lynam, 2001; Tannock, 2000) and depression (Faraone et al., 2005). Youth affected by ADHD are also more likely to experience functional impairments, such as poor academic achievement (Coie, Dodge, & Coppotelli, 1982; Hoza et al., 2005; MTA Cooperative Group, 1999a) and impaired peer relationships (MTA Cooperative Group, 1999b).
Given that children and adolescents with ADHD constitute a remarkably high-risk group, researchers have directed much effort toward understanding how ADHD exerts a negative influence on affected youth. Given the complexity of the disorder, Johnston and Mash (2001), in their seminal review of the empirical studies on parent-related variables and the development of children with ADHD, examined such relationships through a developmental psychopathology lens. From a developmental psychology perspective, child development unfolds through interactions between individual-level variables (i.e., temperament, behavior) and environmental contexts (i.e., family, school). In examining the development of youth with ADHD, research has emphasized interactions between parent-related factors (i.e., parenting style) and child ADHD symptoms in particular, given the tremendous impact that parents often have on the development of their children. Causal relationships between specific parenting styles and differential outcomes for children with ADHD have yet to be established; however, research has identified strong and consistent correlations between certain parenting practices and child outcomes (Hinshaw et al., 2000; Wells et al., 2000).
Parenting and Academic Outcomes in Children and Adolescents With ADHD
Research on parenting practices in relation to childhood ADHD has tended to focus on the development and treatment of comorbid childhood psychopathology. Less research has explored relationships between parenting practices, child ADHD symptoms, and corresponding functional impairments, such as academic underachievement and compromised peer relationships (Deault, 2010). However, several studies have linked parental involvement in particular to children’s academic outcomes (Fan & Chen, 2001; Pomerantz, Moorman, & Litwack, 2007). More specifically, two forms of parental involvement have been identified in relation to a child’s academic sphere: (a) supportive involvement and (b) controlling involvement. Supportive involvement is characterized by parental interest, praise, and reinforcement, and fosters self-efficacy and initiative in the child regarding his or her scholastic endeavors. Controlling involvement by contrast is marked by harsh commands, punishment, criticism, and intrusiveness. This type of involvement is linked to poorer academic achievement among children. The literature suggests that parents of children with ADHD are more likely to adopt the latter style of involvement with regard to their child’s schooling and make greater use of negative parenting strategies, such as harsh and controlling discipline combined with low levels of emotional support and responsiveness (Johnston, Murray, Hinshaw, Pelham, & Hoza, 2002; Khamis, 2006; Woodward, Taylor, & Dowdney, 1998). Not surprisingly, this style of parenting is associated with increases in the severity of inattention and hyperactivity in children (McLaughlin & Harrison, 2006).
Examining parenting-related correlates of functional impairment among children with ADHD is of great importance, given the far-reaching implications that such impairments have on developmental trajectories throughout an individual’s life. For instance, as compared with nonaffected controls, youth with ADHD complete on average 2.5 fewer years of schooling. Furthermore, among adolescents with ADHD, nearly one quarter fail to complete high school (Mannuzza, Klein, Bessler, Malloy, & LaPadula, 1993). Heading into young adulthood, less than 12% of individuals with ADHD complete a bachelor’s degree or higher (Barkley, Fischer, Edelbrock, & Smallish, 1990; Murphy, Barkley, & Bush, 2002), in contrast to the 30% of Americans who earn a bachelor’s degree or higher (U.S. Census Bureau, 2012). Similar long-term consequences have been observed in the social realm. Thirty to fifty percent of individuals with ADHD who experienced social difficulties in childhood continue to experience such problems in adulthood (Jackson & Farrugia, 1997).
ADHD Symptoms in College Students
Recently, researchers and practitioners have begun to direct efforts toward understanding how ADHD symptoms might affect adult populations. Examining the impact of ADHD symptoms on outcomes in college students is of particular importance, given the high rates of self-reported ADHD symptoms among this age group and corresponding impairment. Estimates suggest that approximately 2% to 8% of college students report clinically significant levels of ADHD symptomatology and comprise about 25% of students receiving disability services (Wolf, 2001).
Not surprisingly, college students with significant ADHD symptoms may experience difficulty adjusting to the new academic and social environments of college. Results from several studies have linked ADHD symptoms to academic difficulty. Specifically, college students with significant ADHD symptoms report lower grades (Blase et al., 2009; Heiligenstein, Guenther, Levy, Savino, & Fulwiler, 1999; Norwalk, Norvilitis, & MacLean, 2009; Rabiner, Anastopoulos, Costello, Hoyle, & Swartzwelder, 2008; Shaw-Zirt, Popali-Lehane, Chaplin, & Bergman, 2005) and less self-efficacy in selecting career paths (Norvilitis, Sun, & Zhang, 2010; Norwalk et al., 2009). College students affected by ADHD also report higher rates of mental health concerns, particularly depression (Blase et al., 2009; Rabiner et al., 2008), which, in and of itself, consistently predicts academic underachievement among college students (Haines, Norris, & Kashy, 1996; Heiligenstein, Guenther, Hsu, & Herman, 1996).
Parenting and Academic Outcomes in Non-Clinical College Student Samples
In light of the difficulties that college students with significant ADHD symptoms face throughout college, researchers have attempted to understand variables, both proximal and distal, that might relate to success during college. In nonclinical samples, one distal variable that has been explored to understand college students’ success is student report of their parents’ parenting style. Several studies provide evidence for a positive relationship between parenting style and academic achievement among college students. One study found that students who reported their parents to be a combination of autonomy granting, demanding, and supportive were more likely to be academically successful in college as compared with students who did not endorse such parenting styles (Strage & Brandt, 1999). Other studies have replicated these results, linking authoritative parenting to increased academic adjustment among college students (Hickman, Bartholomae, & McKenry, 2000; Silva, Dorso, Azhar, & Renk, 2007; Turner, Chandler, & Heffer, 2009).
As discussed previously, research has examined relationships among parenting, ADHD symptoms, and academic outcomes in children and adolescents. Such studies have generally found strong and consistent links between certain parenting practices and academic outcomes in youth. To our knowledge, no studies to date have explored relationships among ADHD symptoms, parenting style, and adjustment in college students. The relative dearth of research in this area may reflect the diminished influence that parents may have on the adjustment of their offspring as they enter young adulthood (Laible, Carlo, & Raffaelli, 2000). However, given the established relationships among parenting styles and ADHD symptoms in children, as well as the relationships between parenting and academic achievement in nonclinical college student samples, it is important to examine these variables and their interrelationships in college students. Also of interest is whether parenting practices continue to play a role in the academic adjustment of college students with ADHD symptoms. Establishing continuity of the relationship between parenting style and academic adjustment among individuals affected by ADHD from early childhood through college might enable researchers to better understand the unique challenges faced by this population and to clearly define targets for intervention.
The Present Study
The primary aim of this study was to identify relationships among college student report of their parents’ parenting style (hereafter referred to as “parenting style”), ADHD symptoms, and academic adjustment to college. Specifically, we examined whether parenting style moderated the relationship between ADHD symptoms and academic adjustment. For instance, for students with high ADHD symptoms, would certain parenting styles (i.e., authoritative) buffer against the documented negative relationship between ADHD symptoms and academic adjustment resulting in no difference in academic adjustment between those with high and low ADHD symptom levels when authoritative parenting was high?
Method
Participants
Participants in this study were 200 college students (63.5% female) attending a large public university in the Midwestern United States, ages 18 to 42 years (M = 20.93, SD = 4.85). The university has a large commuter population, a 21:1 faculty: student ratio, and more than 25,000 students pursuing an undergraduate degree. The ethnic composition of the sample was primarily Caucasian (78.5%), which is representative of the geographic area. The majority of participants (60%) were in their freshmen year of study. Detailed participant demographic information is presented in Table 1.
Sample Characteristics.
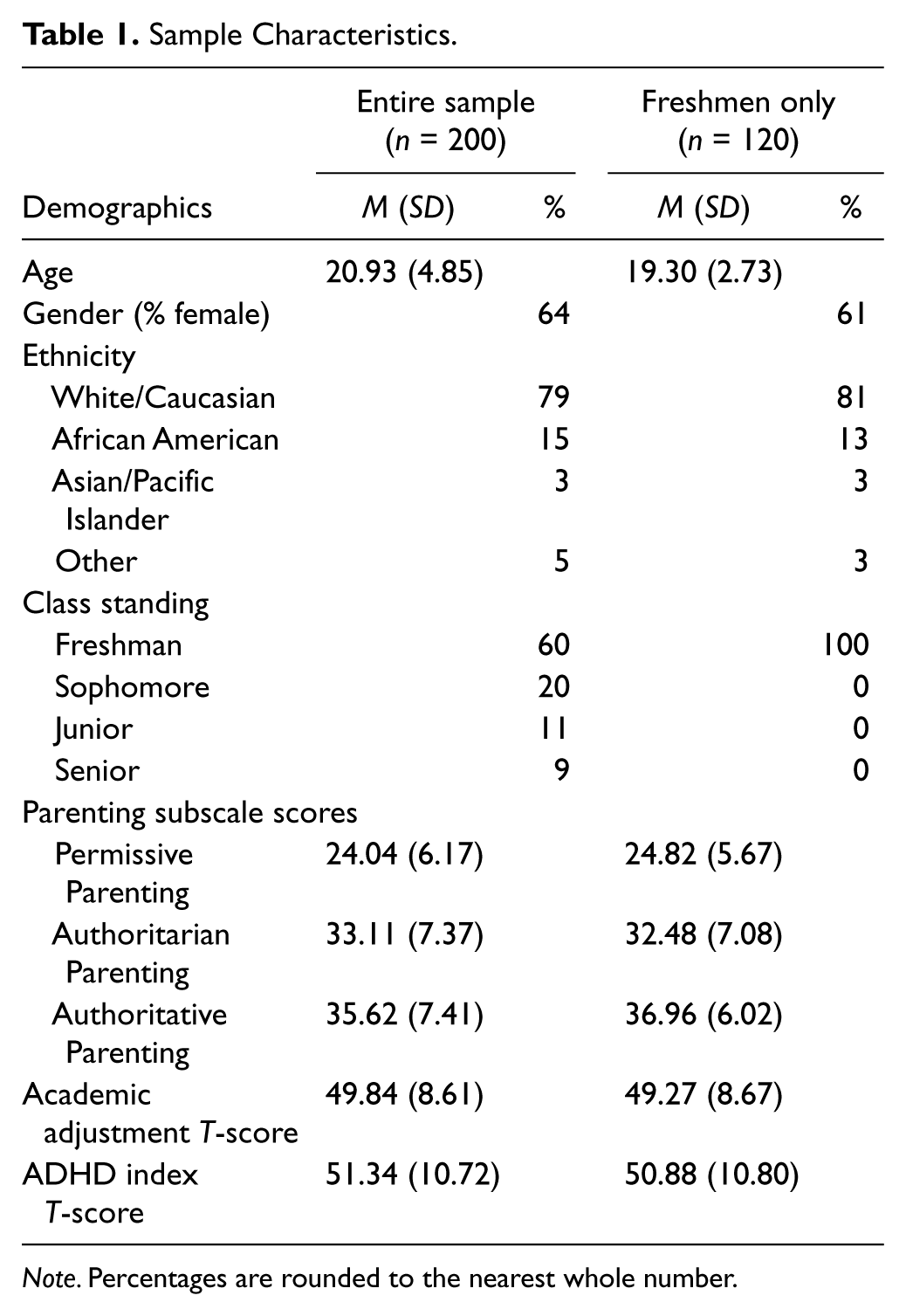
Note. Percentages are rounded to the nearest whole number.
Measures
Demographics
Each participant was asked to provide basic information about his or her age, ethnicity, class standing, and gender to ensure that a representative sample of the university population was selected.
ADHD Symptoms
The Conners’ Adult ADHD Rating Scale–Self-Report: Short Version (CAARS-S:S; Conners, Erhardt, & Sparrow, 1999) was used as a dimensional measure of current ADHD symptoms in a form suitable for adults. The CAARS-S:S is a 26-item, reliable and valid measure of ADHD symptoms that assesses the core features of ADHD as seen in children and adolescents, while adding content unique to adult expression of ADHD (Conners et al., 1999; Erhardt, Epstein, Conners, Parker, & Sitarenios, 1999). It was used to assess the presence and severity of Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) symptoms of ADHD and associated impairment on a 4-point Likert-type scale (not at all/never, just a little/once in a while, pretty much/often, very much/very frequently). In this study, the overall ADHD Index T-score was used as the measure of ADHD symptoms and evidenced excellent internal consistency (α = .92).
Parenting
To assess the parenting style used by their primary caregiver during their childhood, participants completed the Parental Authority Questionnaire (PAQ; Buri, 1991). With 30 Likert-type scale (strongly agree to strongly disagree) items measuring parenting behavior, this measure produced scores for each participant on three different subscales: Permissive Parenting, Authoritarian Parenting, and Authoritative Parenting. This measure has demonstrated strong psychometric properties (Buri, 1991). In the current study, internal consistency, as measured by Cronbach’s alphas, was .78 for Permissive Parenting, .87 for Authoritarian Parenting, and .86 for Authoritative Parenting.
Academic Adjustment to College
The Student Adaptation to College Questionnaire (Baker & Siryk, 1986) is a 67-item self-report questionnaire which measures adjustment to college in four specific areas: academic adjustment, personal-emotional adjustment, social adjustment, and attachment to the institution. It has been standardized on more than 1,300 undergraduates and has good psychometric properties (Baker & Siryk, 1986). In this study, academic adjustment was of primary interest. The Academic Adjustment subscale demonstrated adequate internal consistency (α =.76).
Procedure
Study participants were recruited via the Human Subjects participation pool in the Department of Psychology at the university. Students who expressed interest in the study were contacted by a study research assistant and scheduled for an appointment. Upon arriving at their research appointment, informed consent was obtained, and participants completed measures assessing basic demographic information, ADHD symptoms, parenting style, and adjustment to college. This study was approved by the university’s institutional review board.
Data Analyses
Consistent with recommendations from Aiken and West (1991), hierarchical multiple regressions were used to explore the moderating effect of each of the three different parenting styles on the relationship between ADHD symptoms and academic adjustment in participants. The predictor and moderator variables were centered, and interaction terms were created by multiplying together the centered variables (Aiken & West, 1991). For each of the three types of parenting style, predictor variables were entered in the following order: (a) ADHD symptoms and the parenting style variable and (b) the interaction between ADHD symptoms and the parenting style variable. Significant interactions were identified by examining the beta weights in the final regression models. Individual slopes were also calculated and tested for significance.
Results
Means and standard deviations for the independent and dependent measures are presented in Table 1. Variability in the primary predictor variable of the ADHD Index T-score was appropriate for the planned analyses (M = 51.34, SD = 10.72, range = 30-88, skewness = .705, kurtosis = .211). Given the large sample size in this study as well as the relatively low skewness and kurtosis, the ADHD Index T-score was reasonably normally distributed (Tabachnick & Fidell, 2001). Of note, 25 students in the overall sample (12.5%) had an ADHD Index T-score at 65 (clinical level) or above. Bivariate correlations were conducted to investigate relationships among ADHD symptoms, academic adjustment, and the three parenting style variables. Authoritarian parenting evidenced significant relationships with permissive parenting (r = −.49, p < .001), authoritative parenting (r = −.23, p = .001), academic adjustment (r = −.18, p = .01), and ADHD symptoms (r = .15, p < .05). Academic adjustment and ADHD symptoms were negatively correlated (r = −.44, p < .001). Neither ADHD symptoms nor academic adjustment were related to authoritative parenting (r = .12, p > .05 and r = −.12, p > .05, respectively).
Given that the majority of the sample was in the 1st year of university study (n = 120), independent t tests were conducted to identify differences between freshmen and nonfreshmen on variables of interest. There was no significant difference between freshmen and nonfreshmen on the ADHD Index T-score, t(199) = −.76, p = .45. Significant differences were found for Permissive Parenting, t(198) = 2.21, p < .05, and Authoritative Parenting, t(198) = 3.18, p < .01, with freshmen reporting higher scores on both parenting subscales. Thus, all moderation analyses were conducted with the entire sample and then repeated with data from freshmen only.
As noted above, a series of regressions and tests of slope, as recommended by Aiken and West (1991) were conducted for the entire sample and for freshmen only. In considering the full sample, permissive parenting did not moderate the relationship between ADHD symptoms and academic adjustment (β = .05, p > .05). Authoritarian parenting approached significance as a moderator (β = .12, p = .06). In the entire sample, only authoritative parenting emerged as significant moderator of the relationship between ADHD symptoms and academic adjustment (see Table 2 and Figure 1). At low levels of authoritative parenting, academic adjustment significantly decreased as ADHD symptoms increased, t(196) = −3.67, p < .001. At high levels of authoritative parenting, academic adjustment also significantly decreased as ADHD symptoms increased, but did so at a steeper decline than for low levels of authoritative parenting, t(196) = −6.86, p < .001.
Entire Sample Regression Analyses With ADHD Symptoms, Authoritative Parenting, and Their Interaction Predicting Academic Adjustment (n = 200).
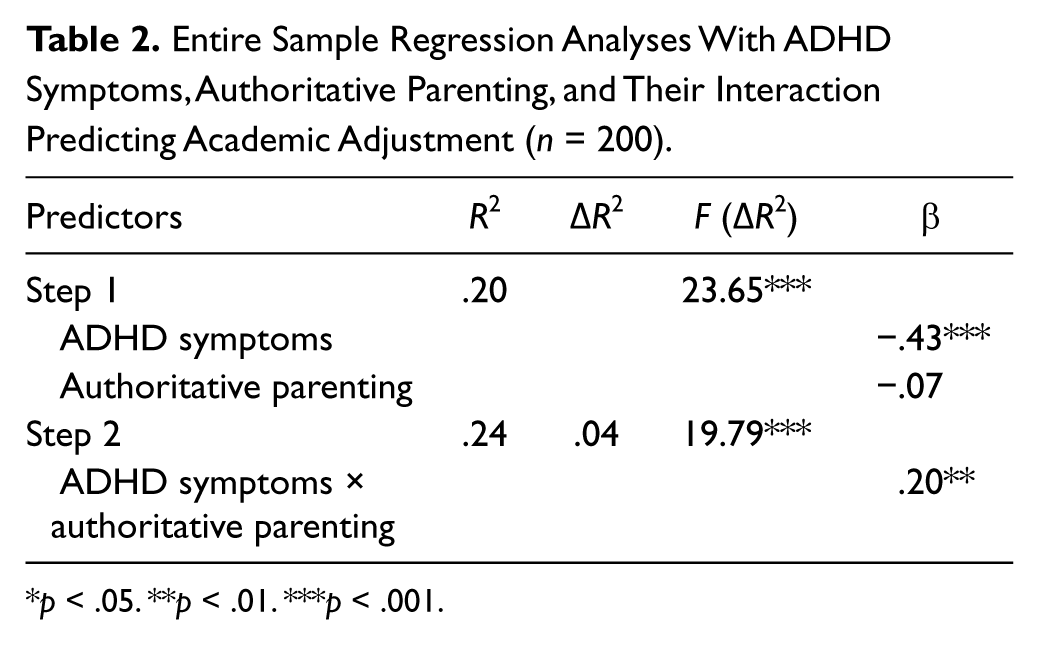
p < .05. **p < .01. ***p < .001.
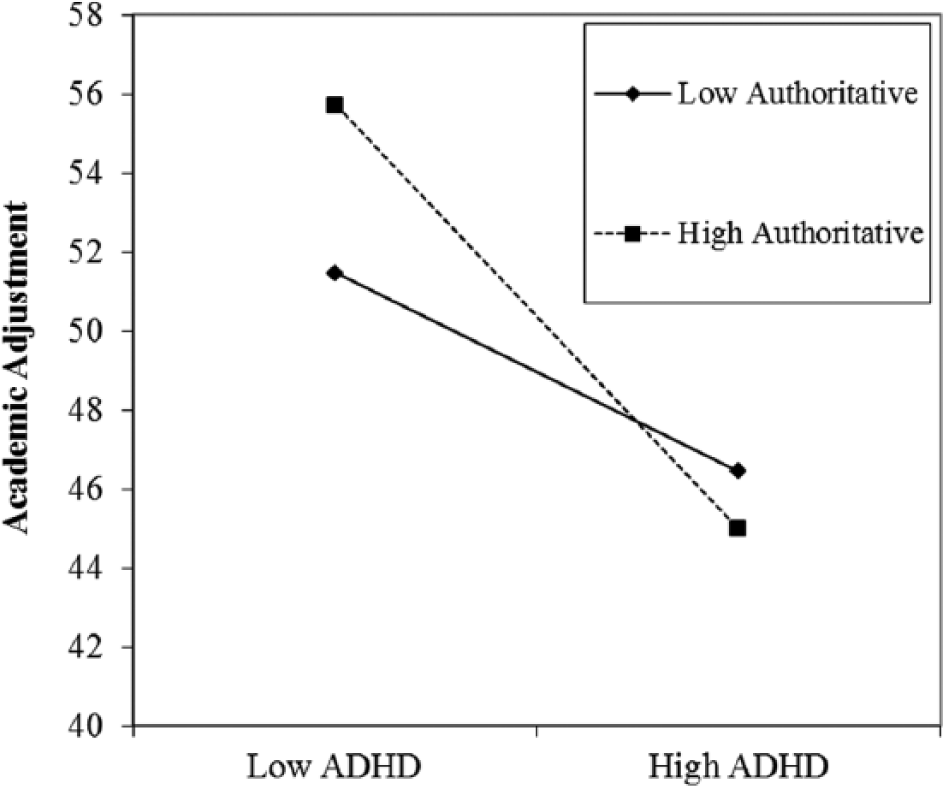
Significant interaction between ADHD symptoms and authoritative parenting using the entire sample.
When examining data from freshmen only, permissive parenting remained nonsignificant as a potential moderator (β = −.02, p > .05). However, analyses revealed that authoritarian parenting and authoritative parenting moderated the relationship between ADHD symptoms and academic adjustment. Table 3 and Figure 2 show the moderating effect of authoritarian parenting on ADHD symptoms and academic adjustment in college freshmen. At low levels of authoritarian parenting, academic adjustment significantly decreased as ADHD symptoms increased, t(116) = −5.19, p < .001; a similar pattern was detected at high levels of authoritarian parenting, only at less steep a slope than for low levels of authoritarian parenting, t(116) = −2.11, p < .001. Examining authoritative parenting as a moderator using data from freshmen only revealed similar findings to the analyses performed with the sample at large (see Table 4 and Figure 3): For low levels of authoritative parenting, academic adjustment significantly decreased as ADHD symptoms increased, t(116) = −2.60, p < .05, and for high levels of authoritative parenting, academic adjustment more steeply decreased as ADHD symptoms increased, t(116) = −5.50, p < .001.
Freshmen-Only Regression Analyses With ADHD Symptoms, Authoritarian Parenting, and Their Interaction Predicting Academic Adjustment (n = 120).
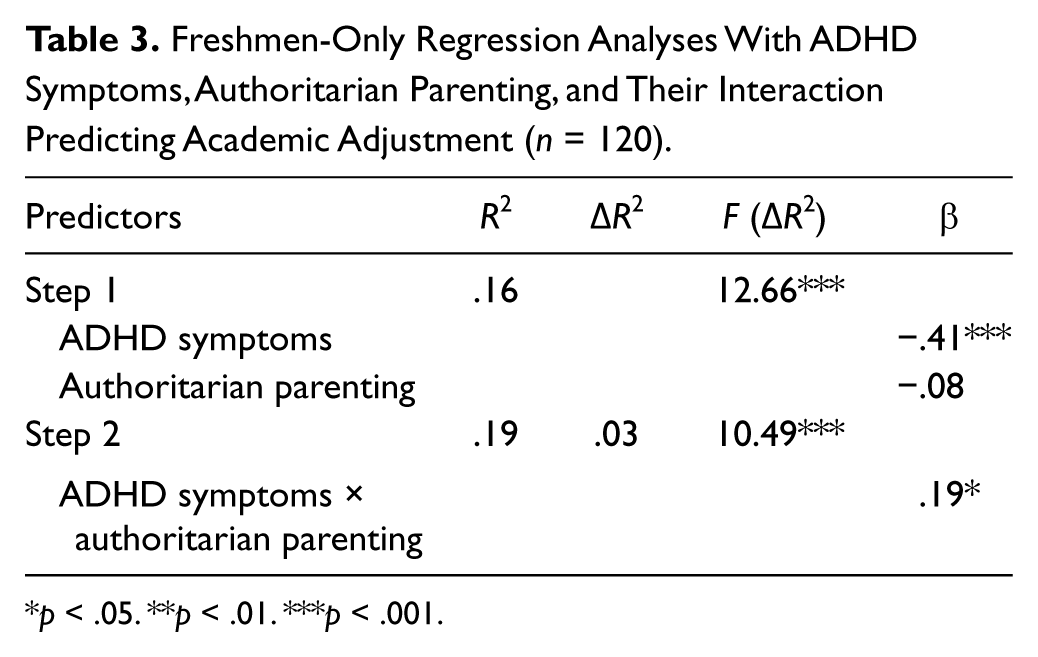
p < .05. **p < .01. ***p < .001.
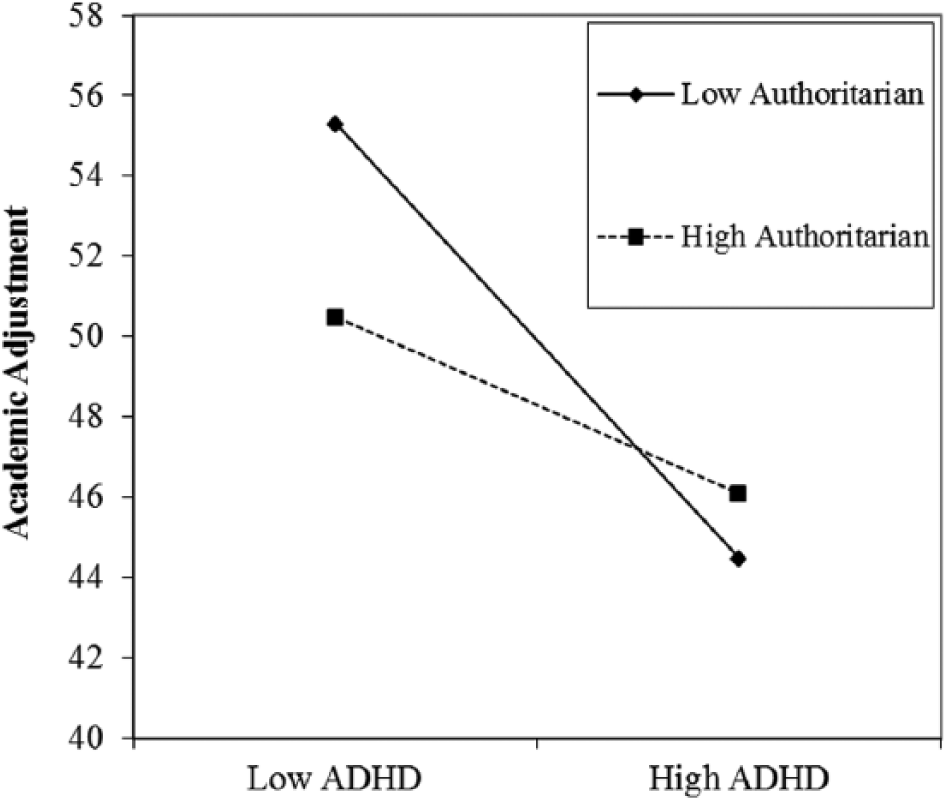
Significant interaction between ADHD symptoms and authoritarian parenting using the data from freshmen only.
Freshmen-Only Regression Analyses With ADHD Symptoms, Authoritative Parenting, and Their Interaction Predicting Academic Adjustment (n = 120).
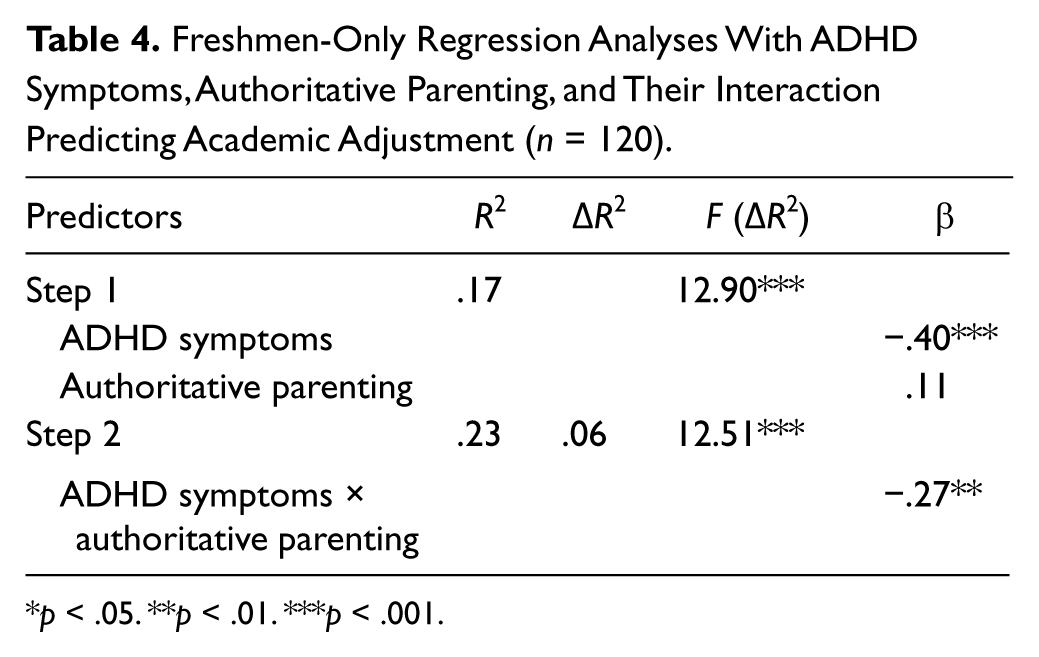
p < .05. **p < .01. ***p < .001.
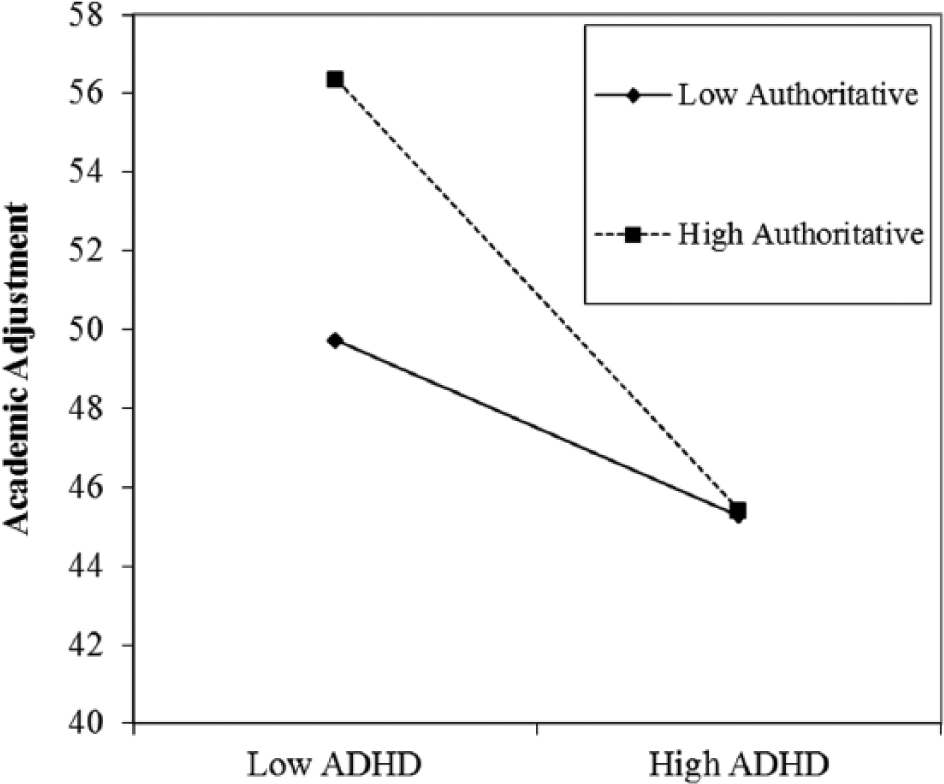
Significant interaction between ADHD symptoms and authoritative parenting using the data from freshmen only.
Conclusion
Overall, cross-sectional findings indicate that parenting (in particular authoritarian and authoritative parenting) relates to academic adjustment in college, but only if the student’s level of ADHD symptoms is low. Results from the bivariate correlational analyses were mostly consistent with the current literature, demonstrating significant negative correlations between academic adjustment and authoritarian parenting and ADHD symptoms. Our detection of a negative relationship between academic adjustment and authoritarian parenting is consistent with the literature on college student samples (Frazier, Youngstrom, Glutting, & Watkins, 2007; Strage & Brandt, 1999; Wintre & Yaffe, 2000). Also consistent with previous research (Barkley, Fischer, Smallish, & Fletcher, 2002), ADHD symptoms were negatively related to academic adjustment.
Given the breadth of literature documenting links between authoritative parenting and academic adjustment among normative child samples (Fan & Chen, 2001; Pomerantz et al., 2007), we expected to see this same trend in a college student sample, indicating that parenting may buffer against the negative impact of ADHD symptoms. Interestingly, in the simple correlational analyses, we did not find a relationship between authoritative parenting and academic adjustment for our sample. It may be that relative to school-age and adolescent populations, parenting has less of an impact on functional outcomes, such as academic adjustment among college students with significant ADHD symptoms. In addition, this finding may speak to the pervasive nature of ADHD symptoms and also the decreased relevance of parenting for college students. A study conducted by Parker, Majeski, and Collin (2004) found that personality type was the strongest predictor of academic success for this population. In a related vein, results from a separate study conducted by Kaminski, Turnock, Rosen, and Laster (2006) suggested that time-management skills and financial stability predicted academic success for college students with ADHD. Future research might examine relationships among ADHD symptoms, academic adjustment, and variables that are more salient for college students (e.g., organizational skills, coping strategies) or potentially have more stability over time (e.g., personality type). Finally, parenting may only be relevant for those students who still live at home or have their parents directly involved in their college education (e.g., allowing access to academic records, carrying a financial burden for their child’s college education); however, this is an empirical question that may be examined via future research.
Relevant to our primary aim, parenting did not buffer the effects of ADHD symptoms on academic adjustment. In other words, we found that those college students with high levels of ADHD symptoms and with parents who reportedly engaged in authoritative parenting still had decreased academic adjustment over those with low levels of symptoms, despite parenting style. Thus, parenting emerged as a moderator of the relationship between ADHD symptoms and academic adjustment. Specifically, lower levels of authoritarian parenting were associated with increased academic achievement at low levels of ADHD symptoms only and for freshmen only. This finding is consistent for previous studies cited above on college students’ academic adjustment and parenting style (e.g., Silva et al., 2007), as bivariate relationships between parenting and college student academic adjustment have been documented in the literature. However, when levels of ADHD symptoms are considered, the picture becomes more complicated as we found that, for authoritative parenting, higher levels of this parenting style were associated with increased academic adjustment at low levels of ADHD symptoms only. Once ADHD symptoms reached clinical levels, academic achievement dropped significantly, regardless of high versus low levels of authoritarian or authoritative parenting styles, thus indicating no buffering effect of parenting on the negative relationship between ADHD symptoms and academic adjustment.
One plausible explanation for this finding is that high levels of ADHD symptomology may mask some of the factors that may serve a protective function for students. It is also possible that the psychological comorbidities associated with clinical levels of adult ADHD symptoms negate the impact of parenting style on academic achievement. This particular interaction has neither been examined among college students with ADHD nor with younger populations. However, school-age children and adolescents with comorbid ADHD and ODD and/or CD consistently achieve lower academic success relative to youth with ADHD alone (Hinshaw, 1992; Kuhne, Schachar, & Tannock, 1992). Thus, it would be worthwhile to examine direct and indirect relationships between psychological comorbidity and academic adjustment among college students with clinically significant ADHD.
Findings from this study should be interpreted in the context of two primary limitations. First, the sample, although representative of the university, was relatively limited with regard to ethnic diversity. Research examining relationships between various parenting practices and subsequent child outcomes have indicated that culture-specific patterns exist. For instance, mothers’ use of physical discipline may be associated to greater externalizing behaviors in Caucasian as compared with African American children (Deater-Deckard, Dodge, Bates, & Pettit, 1996). Our sample was not large enough nor did it contain sufficient diversity to examine cultural differences in reported parenting and outcomes in college student participants. Future research should thus examine whether the relationships we found among parenting style, academic adjustment and ADHD symptoms in a primarily Caucasian sample exist in other, more diverse samples as well. Second, we did not query parents about their own parenting styles and instead relied upon college students’ retrospective reports, which may have been subject to recall biases (Yarrow, Campbell, & Burton, 1970). Replication of this study with student report of current parenting behavior (rather than past) as well as parent-report data would strengthen findings and reduce potential recall biases. In addition, the cross-sectional nature of our design prevents a determination of causality. Finally, we should caution that the sample in this study was not oversampled for college students with ADHD. Although we do feel that a significant number of students with clinical symptoms of ADHD participated, this study should be replicated with a clinical population to validate these findings with college students with ADHD.
As noted previously, this study was the first to investigate the role of parenting in the relationship between academic adjustment and ADHD symptoms in college students. This study carries with it several important clinical and research implications. First, given that academic adjustment declined as ADHD symptoms increased (regardless of parenting style) for those students with clinically significant ADHD symptomology, researchers should direct efforts toward developing specific interventions designed to improve academic functioning, specifically for college students with significant ADHD symptoms. Interventions might target variables that seem to be more salient predictors of academic adjustment for this population, including study habits and organizational and time-management skills. Furthermore, such interventions should be used to guide clinicians working with college students affected by ADHD to support and enhance learning for this population.
Second, clinicians working in university settings could help train other professionals (i.e., disseminate evidence-based practices) to meet the learning needs of students with ADHD. For example, staff members in academic support services on college campuses should be taught to include academic-specific learning strategies (e.g., note taking, the use of study aides) that might assist college students with ADHD symptoms. Given the high rates of psychological comorbidity among college students with significant ADHD symptoms, academic student support staff should be trained to recognize symptoms of ADHD and make referrals to psychological and psychiatric services for students with clinical levels of ADHD. To conclude, this study is the first to demonstrate that the strength of the relationship between ADHD symptoms and academic adjustment may vary by level of authoritative and authoritarian parenting. However, for those college students with high levels of ADHD, there is clear need for academic intervention irrespective of how they were parented as youth.
Footnotes
Acknowledgements
We would like to thank Martin Murphy for his assistance during the planning of this study and Joshua Langberg for his statistical consultation. We also acknowledge the undergraduate research assistants who worked on this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.