
Abstract
Introduction
The definition of a therapeutic goal for any given medical condition is largely a function of the clinical course of that condition, the efficacy of evidence-based treatments for the condition, and the treatment objectives of patients and their families. For acute conditions, therapeutic goals often involve resolution of the condition (i.e., treating an infection to resolution or eliminating acute psychotic symptoms). Clinical goals for chronic conditions are often more modest than those for acute conditions and involve management of the disease to reduce morbidity and mortality over the patient’s life span. For certain chronic conditions, defining appropriate therapeutic goals is more complicated. Therapeutic goals for patients with chronic physical conditions like hyperlipidemia, hypertension, and asthma are largely defined by evaluating laboratory values, assessing findings on physical examinations, and evaluating clinical status, and these goals evolve as the clinical course of patients’ medical conditions change and the implications of the laboratory values have become better understood (National Institutes of Health, 2007; Pearson et al., 2002).
Therapeutic goals for chronic mental disorders such as major depressive disorder (MDD) and schizophrenia have evolved in parallel with the expanding medical knowledge regarding these disorders. Within the past 2 decades, therapeutic goals for MDD and schizophrenia have come to include the concept of remission and recovery, as well as freedom from impairment using well-defined criteria from diagnostic tools (American Psychiatric Association [APA], 1993; APA, 2000b; Andreasen et al., 2005; Depression Guideline Panel, 1993a, 1993b; Frank et al., 1991). Although ADHD was initially thought to be a self-limiting childhood disorder, a meta-analysis of prospective follow-up studies found that in two thirds of cases, ADHD is a chronic psychiatric disorder that often persists through adolescence and adulthood (Faraone, Biederman, & Mick, 2006), and studies of adults show that the disorder is associated with serious impairments in adulthood, including traffic accidents, occupational failure, substance abuse problems, and occupational difficulties (Barkley, Murphy, & Fischer, 2008; Biederman & Faraone, 2006; Faraone et al., 2007; Mick, Faraone, Spencer, Zhang, & Biederman, 2008). This would suggest that it is important to develop long-term objectives for the treatment of ADHD.
In defining a primary outcome for treatment response, clinical trials of medications for the U.S. Food and Drug Administration (FDA) have used ADHD symptom reduction as the primary outcome measure as this is a therapeutic goal clearly related to the disorder being treated (Findling, Childress, Krishnan, & McGough, 2008; Findling et al., 2009; Hoare et al., 2005; McGough et al., 2005; Sallee, Lyne, Wigal, & McGough, 2009; Wilens, Newcorn et al., 2006). The knowledge base regarding the clinical course of ADHD has evolved past symptomatic treatment response; however, long-term goals, such as remission and optimization of functioning, have not yet been clearly defined. Present ADHD guidelines from the American Academy of Pediatrics refer to developing “targeted outcomes” as long-term therapeutic goals; however, these guidelines refer only to an undefined “treatment response” in the treatment algorithm (American Academy of Pediatrics, 2001). Present ADHD guidelines from the American Academy of Child and Adolescent Psychiatry mention “optimal response,” “normative functioning,” and “remission,” but do not offer criteria to define these therapeutic goals (Pliszka, 2007).
The lack of well-defined, long-term treatment goals has implications for patients, families, and clinicians. The multisite National Institute of Mental Health (NIMH) Multimodal Treatment Study of Children With ADHD (MTA study) compared intensive treatment versus community treatment strategies (Conners et al., 2001; Jensen, 1999; Jensen, Hinshaw, Kraemer et al., 2001; Jensen, Hinshaw, Swanson et al., 2001; NIMH, 1999a, 1999b; Swanson et al., 2001). Children were randomly assigned to behavioral treatment, medical management, combined (behavioral and medical management) treatment, or community treatment groups. Children in the first three groups received intensive treatment for 14 months that was delivered by staff specifically trained for this study and monitored by the MTA investigators (Conners et al., 2001; Jensen, 1999; Jensen, Hinshaw, Kraemer et al., 2001; Jensen, Hinshaw, Swanson et al., 2001; NIMH, 1999a, 1999b; Swanson et al., 2001). Clinical success, or remission, as defined by a mean item score <1 on the Swanson, Nolan, and Pelham Questionnaire–Fourth Revision (SNAP-IV), was achieved by 34%, 56%, 68%, and 25% of patients in the behavioral treatment, medical management, combined treatment, and community treatment groups, respectively (Swanson et al., 2001). The study demonstrated that combined treatment represented a 21.4% increase in the rate of remission compared with either behavioral treatment or medical management alone (Swanson et al., 2001). For some children with ADHD, the failure to achieve remission may have been related to the need for further optimization of available treatments (behavioral treatment, medical management, or combined treatment) based on the individual needs of each patient (Swanson et al., 2001).
The potential consequences of not treating patients with ADHD to predefined remission criteria have been widely published. Research studies indicate that patients with ADHD who received pharmacological treatment may have a reduced risk of developing substance use disorder, MDD, anxiety disorders, and disruptive behavior disorders compared with those who did not (Biederman, Monuteaux et al., 2008; Biederman, Monuteaux, Spencer, Wilens, & Faraone, 2009; Biederman, Wilens, Mick, Spencer, & Faraone, 1999; Wilens, Biederman, & Mick, 1998; Wilens, Faraone, Biederman, & Gunawardene, 2003). Untreated or inadequately treated patients with ADHD are at greater risk for other adverse outcomes, such as driving accidents, teen pregnancy, and sexually transmitted diseases (Barkley, Fischer, Edelbrock, & Smallish, 1990; Barkley, Fischer, Smallish, & Fletcher, 2006; Barkley, Guevremont, Anastopoulos, DuPaul, & Shelton, 1993; Fischer, Barkley, Smallish, & Fletcher, 2002; Mannuzza, Klein, Bessler, Malloy, & Hynes, 1997; Mitchell, Aman, Turbott, & Manku, 1987; Murphy & Barkley, 1996; Satterfield & Schell, 1997; G. Weiss, Hechtman, Milroy, & Perlman, 1985).
Through our review of the literature, long-term goals are proposed for the treatment of ADHD in children, and practical, clinically relevant criteria are provided to help clinicians and researchers define these long-term goals.
Method
Literature Search
We conducted a PubMed literature search to investigate the therapeutic goals referenced in the literature from January 1998 through February 2010 to capture the advent of the long-acting stimulants used to treat ADHD. Search terms included ADHD and the following commonly used ADHD treatments: amphetamine, methylphenidate, atomoxetine, lisdexamfetamine, guanfacine, and clonidine. This search was then combined with an additional search that included the outcome terms remission, relapse, remit, response, normal, normalization, recovery, and effectiveness. The search was limited to publications in the English language and those involving human subjects.
Results
Literature Review
The literature search resulted in 524 ADHD publications (articles and abstracts), of which 102 had predefined criteria for determining “treatment response,” “normalization,” and “remission” and/or “relapse.” As expected based on available guidelines, the majority 88.2% (90/102) of the publications contained predefined criteria for “treatment response” (see Appendix A for list of references cited). Predefined criteria for “normalization” were presented in only 4.9% (5/102) of publications (Table 1; Biederman, Mick, & Faraone, 1998; Gualtieri & Johnson, 2008; Stein et al., 2003; M. Weiss et al., 2007; Zeiner, Bryhn, Bjercke, Truyen, & Strand, 1999), criteria for “remission” in 12.7% (13/102) of publications (Table 2; see Appendix B for list of references cited), and criteria for “relapse” in 3.9% (4/102) of publications (Table 3; Buitelaar et al., 2007; Cheng, Chen, Ko, & Ng, 2007; Michelson et al., 2004; Newcorn et al., 2006).
Publications With Predefined Criteria for “Normalization” of ADHD Outcomes in Children and Adolescents.
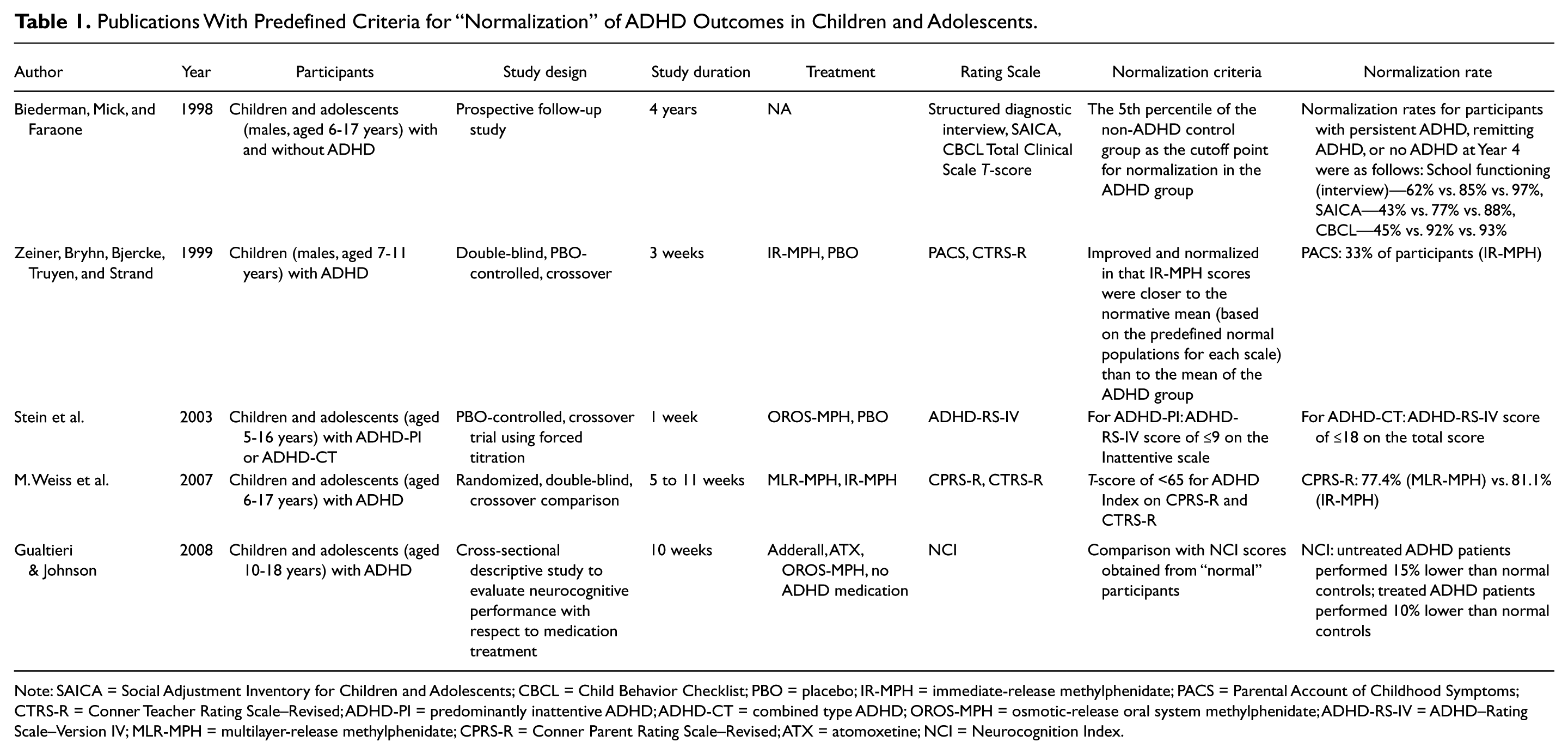
Note: SAICA = Social Adjustment Inventory for Children and Adolescents; CBCL = Child Behavior Checklist; PBO = placebo; IR-MPH = immediate-release methylphenidate; PACS = Parental Account of Childhood Symptoms; CTRS-R = Conner Teacher Rating Scale–Revised; ADHD-PI = predominantly inattentive ADHD; ADHD-CT = combined type ADHD; OROS-MPH = osmotic-release oral system methylphenidate; ADHD-RS-IV = ADHD–Rating Scale–Version IV; MLR-MPH = multilayer-release methylphenidate; CPRS-R = Conner Parent Rating Scale–Revised; ATX = atomoxetine; NCI = Neurocognition Index.
Publications With Predefined Criteria for “Remission” of ADHD Outcomes in Children and Adolescents.
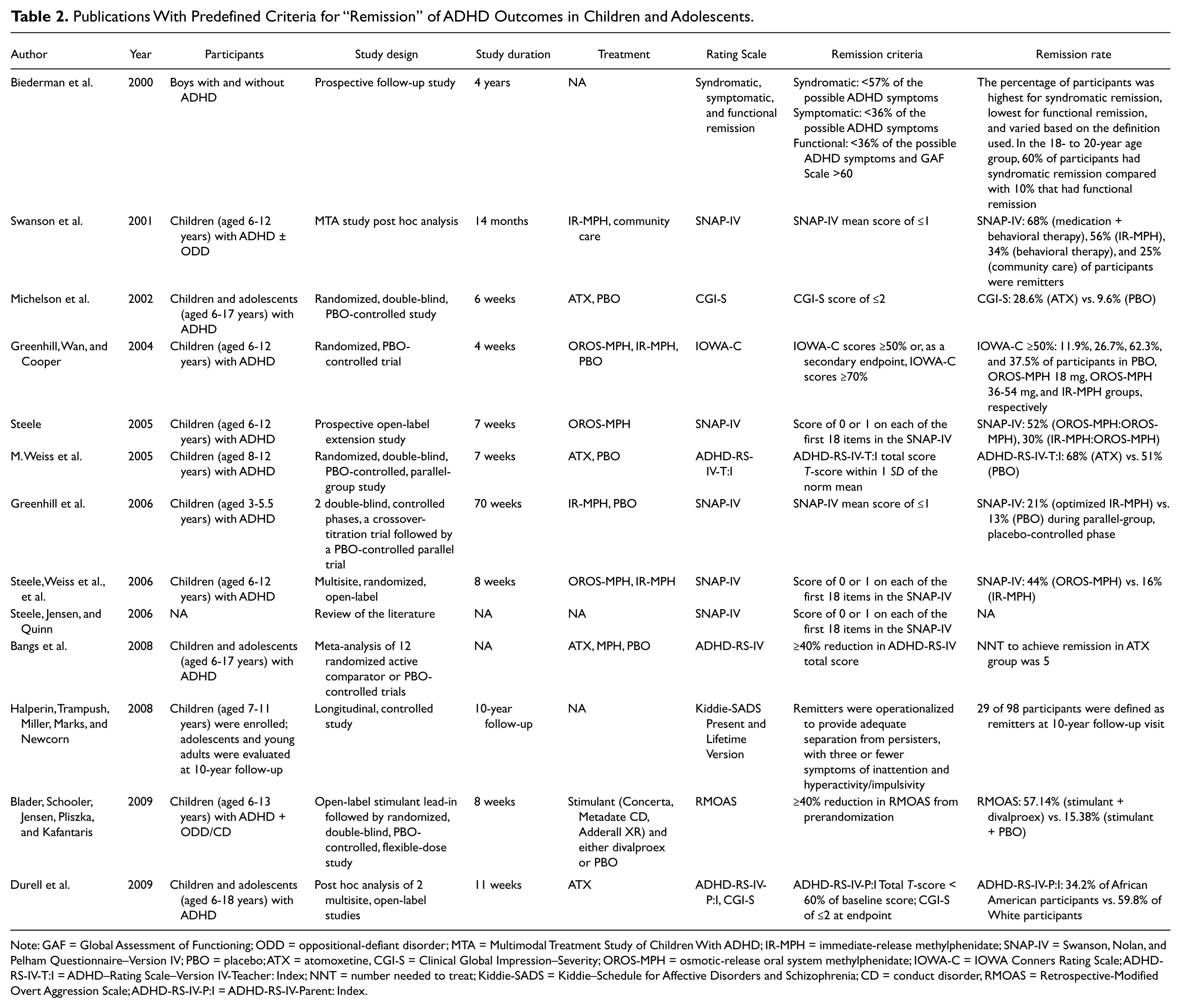
Note: GAF = Global Assessment of Functioning; ODD = oppositional-defiant disorder; MTA = Multimodal Treatment Study of Children With ADHD; IR-MPH = immediate-release methylphenidate; SNAP-IV = Swanson, Nolan, and Pelham Questionnaire–Version IV; PBO = placebo; ATX = atomoxetine, CGI-S = Clinical Global Impression–Severity; OROS-MPH = osmotic-release oral system methylphenidate; IOWA-C = IOWA Conners Rating Scale; ADHD-RS-IV-T:I = ADHD–Rating Scale–Version IV-Teacher: Index; NNT = number needed to treat; Kiddie-SADS = Kiddie–Schedule for Affective Disorders and Schizophrenia; CD = conduct disorder, RMOAS = Retrospective-Modified Overt Aggression Scale; ADHD-RS-IV-P:I = ADHD-RS-IV-Parent: Index.
Publications with Predefined Criteria for “Relapse” ADHD Outcomes in Children and Adolescents.
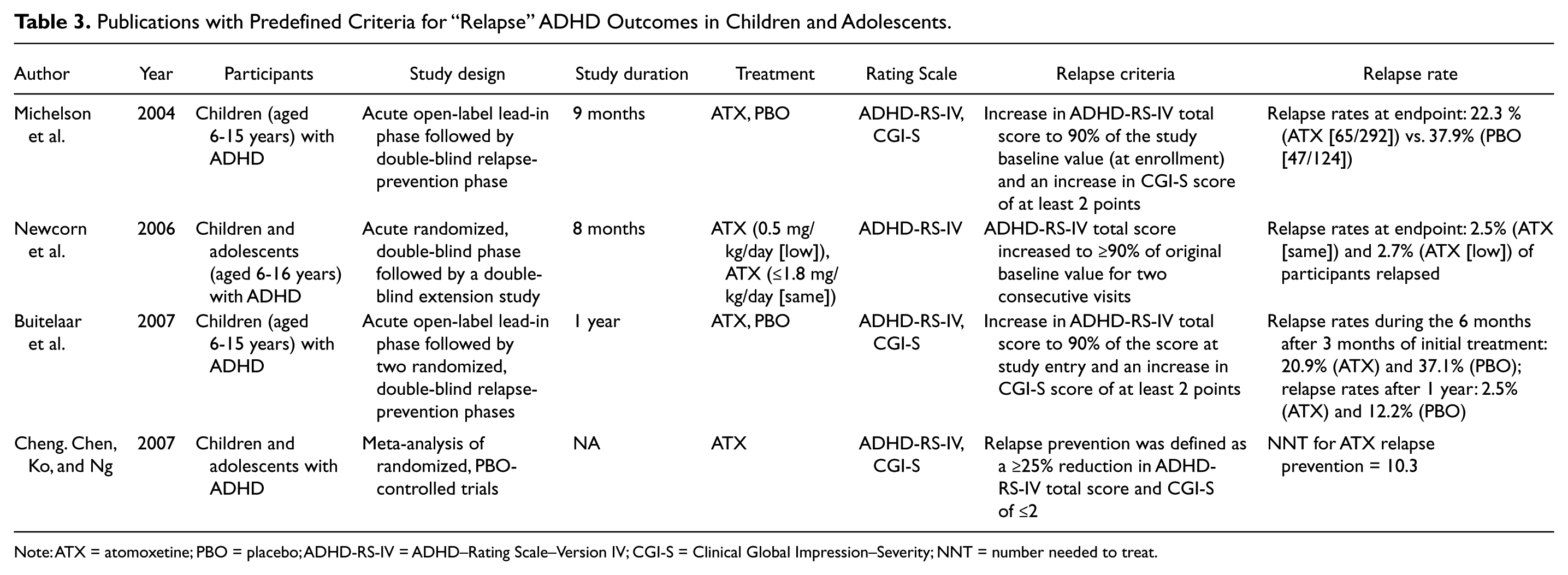
Note: ATX = atomoxetine; PBO = placebo; ADHD-RS-IV = ADHD–Rating Scale–Version IV; CGI-S = Clinical Global Impression–Severity; NNT = number needed to treat.
Of the publications mentioning “treatment response,” 74.4% (67/90) reported data for children and/or adolescents with ADHD (see Appendix C for list of references cited). The majority (73.1% [49/67]) of these studies used the ADHD–Rating Scale–Version IV (ADHD-RS-IV) and/or Clinical Global Impression (CGI) scale to assess treatment response (see Appendix D for list of references cited). However, the operational criteria for meeting response on these instruments were not consistent across studies. The majority of studies using the ADHD-RS-IV defined treatment response as a ≥25% reduction in ADHD-RS-IV score from baseline to study endpoint. The majority of studies using the CGI scale defined treatment response as a CGI score of 1 = very much improved or 2 = much improved.
Of the five ADHD studies in children and adolescents applying “normalization” criteria, each used different criteria definitions, usually by comparing scores from a predefined normative population against scores from patients diagnosed with ADHD. Specific scales used included the Social Adjustment Inventory for Children and Adolescents, the Child Behavior Checklist Total Clinical Scale T-score (Biederman et al., 1998), the Parental Account of Childhood Symptoms, the Conners Teacher Rating Scale–Revised (CTRS-R; Zeiner et al., 1999), ADHD-RS-IV scores based on ADHD subtype (Stein et al., 2003), T-scores for Conners Parent Rating Scale–Revised and CTRS-R (M. Weiss et al., 2007), and the Neurocognition Index (Gualtieri & Johnson, 2008). Table 1 presents the criteria used as cut points to define normalization for the comparisons listed above.
The 13 ADHD studies applying “remission” criteria used variable definitions (Table 2). Four studies used a mean score of ≤1 on the SNAP-IV as the predefined criteria for remission (Greenhill et al., 2006; Steele, 2005; Steele Weiss et al., 2006; Swanson et al., 2001). This score was equal to minimal or none on the individual items included in the symptom rating. Four studies used the ADHD-RS-IV and/or the Clinical Global Impression–Severity of Illness scale (CGI-S); however, the predefined criteria for remission varied among studies (Bangs et al., 2008; Durell et al., 2009; Michelson et al., 2002; M. Weiss et al., 2005). One study each used a score of ≤2 on the CGI-S (Michelson et al., 2002), ADHD-RS-IV Teacher Index total T-score within 1 standard deviation (SD) of the norm mean (M. Weiss et al., 2005), ≥40% reduction in ADHD-RS-IV total score (Bangs et al., 2008), and ADHD-RS-IV Total T-score <60% of baseline score with a CGI-S of ≤2 (Durell et al., 2009) as the predefined criteria for remission. Other remission criteria were a reduction in IOWA Conners scores of ≥50% or ≥70% compared with baseline (Greenhill, Wan, & Cooper, 2004), a comparison between ADHD persisters and remitters on the Kiddie–Schedule for Affective Disorders and Schizophrenia (K-SADS) interview (Cannon et al., 2009), and a ≥40% reduction in Retrospective-Modified Overt Aggression Scale (RMOAS) from prerandomization (Blader, Schooler, Jensen, Pliszka, & Kafantaris, 2009). One study proposed several degrees of remission defined as “syndromatic” (<57% of all possible Diagnostic and Statistical Manual of Mental Disorders [DSM] ADHD symptoms), “symptomatic” (<36% of all possible DSM ADHD symptoms), and “functional” (<36% of all possible DSM ADHD symptoms and a score on the Global Assessment of Functioning [GAF] Scale of >60; Biederman, Mick, & Faraone, 2000).
All four studies describing “relapse” in children and adolescents with ADHD used the ADHD-RS-IV and CGI scales, and the criteria for relapse were similar among studies (Table 3; Buitelaar et al., 2007; Cheng et al., 2007; Michelson et al., 2004; Newcorn et al., 2006). Three studies defined the primary criteria for relapse as an increase in the ADHD-RS-IV total score to 90% of the study baseline value (at enrollment) and an increase in CGI-S score of at least 2 points (Buitelaar et al., 2007; Michelson et al., 2004; Newcorn et al., 2006). One study described the criteria for relapse prevention as a ≥25% reduction in ADHD-RS total score and CGI-S of ≤2 (Cheng et al., 2007).
Discussion
On review of the literature search results, the use of the term normalization was considered by the authors to be too vague because normal is a relative term that means different things to clinicians and researchers, making it difficult to quantify as a treatment goal. The term itself may be stigmatizing to some people, as it implies that the patient with ADHD is abnormal. Therefore, the term normalization was discarded by author consensus as a term to describe the goals of ADHD treatment.
The majority of the publications, outside of those citing “treatment response,” utilized the term remission to describe the goals of ADHD treatment. Thus, a precedent within the published literature was set for the further use and refinement of the term. Furthermore, the term remission is also used in the description of other chronic mental health disorders such as major depression and schizophrenia. Authors proposed the following therapeutic goals to be considered in treating ADHD: short-term “treatment response” and long-term “syndromal remission,” “symptomatic remission,” and “functional remission,” a term that is identical to a definition of “no room for improvement.” For the purpose of this report, the definitions of “syndromal remission,” “symptomatic remission,” and “functional remission” have been described.
Biederman et al. (2000) suggest that the definition of syndromal remission should be based on the loss of diagnostic guidelines for the disorder. Thus, based on present Diagnostic and Statistical Manual of Mental Disorders (4th ed., text revision; DSM-IV-TR; APA, 2000a) guidelines, syndromal remission would be defined as “failing to meet the full diagnostic criteria for ADHD.” However, some patients who reach syndromatic remission may continue to exhibit clinically significant “subthreshold” symptoms of ADHD and functional impairments related to ADHD that would justify additional treatment.
The term symptomatic remission has been used in several ways. As presented in Table 2, there are a number of symptom scales that have been used to provide criteria for this definition. Guidelines from the American Academy of Child and Adolescent Psychiatry (2007) suggest that if a patient with ADHD has been symptom-free for at least 1 year while receiving medication, then inquiries should be made about whether the patient and family still think that the medication is warranted. Biederman et al. (2000) use the term to indicate that the patient has fewer than half the symptoms required for a diagnosis.
Functional and quality-of-life outcomes in children and adults with ADHD have been widely studied using both general assessment scales and disease-specific measures (see Appendix E for list of references cited). Studies have shown that reaching a symptomatic goal is associated with functional improvement (Buitelaar, Wilens, Zhang, Ning, & Feldman, 2009; Steele, 2005; Steele, Weiss et al., 2006; Steele, Jensen, & Quinn, 2006). Functional remission is a desired outcome for patients with ADHD, but it has been studied to a lesser extent. Functional remission means that the patient has achieved symptomatic remission and the individual also shows no functional impairments due to any residual symptoms that may remain. In the two studies identified in our literature search in which functional improvements were mentioned as criteria for remission, these functional improvements were defined using general assessment scales like the CGI or GAF (Biederman et al., 2000; Newcorn et al., 2006). An adaptation of the CGI-S using ADHD-specific criteria would be useful in clinical practice to assess functioning. Thus far, there is no ADHD-specific CGI scale to assess functioning and no CGI scale has been validated.
Providing a definition of remission for patients with ADHD would allow for a description of symptoms beyond treatment response and would better align the clinical course with other chronic psychiatric disorders such as MDD and schizophrenia. Defining the full range of response and remission will help clinicians set goals for patient outcomes. Remission as a treatment goal would enable clinicians, patients, and families to advocate for comprehensive, longitudinal care using paradigms already developed for other chronic conditions. A recent publication by Ramos-Quiroga and Casas (2011) also communicates the importance of establishing remission as a routine goal of pharmacotherapy when treating patients with ADHD. In the absence of complete functional remission, clinicians should be identifying the areas of functional impairment and matching these to therapeutic approaches that will improve outcome (e.g., changing medications, increasing doses, and adding psychosocial, psychoeducational, and/or cognitive-behavioral therapies).
From a research perspective, more work is needed to develop reliable and valid definitions and criteria for the different levels of remission so that these may be implemented in clinical trials and in studies of clinical course and outcome. In addition, statistical tools, such as the Drug-Placebo Response Curve should be used to fully describe the effects of treatments throughout the range of measurement (Faraone, Biederman, Spencer, & Wilens, 2000; Faraone et al., 2002; Faraone et al., 2005). The development of useful tools to identify critical targets for clinical intervention, to track the impact of treatment over time, and to assess the impact of stopping treatment, would be greatly beneficial to practitioners and the patients and families who must make daily choices about how best to implement interventions.
In summary, based on a review of the published literature, the authors have proposed the following definitions for ADHD therapeutic goals. Syndromal remission is defined as “no longer meeting diagnostic criteria for ADHD.” Symptomatic remission is defined as “having symptom scores within the normal range with some remaining functional impairment.” Functional remission (i.e., recovery) is defined as “having both symptom scores and functioning within the normal ranges.”
Challenges/Limitations
Proposing these definitions is an attempt to extend therapeutic goals in ADHD beyond the presently described treatment response to account for the chronicity and long-term impact of the disorder. However, to be effective in changing how ADHD is treated in practice, these concepts and definitions need to be incorporated into treatment algorithms that can be easily adopted by clinicians caring for patients with ADHD. Future studies are needed to validate criteria for symptomatic and functional remission and to standardize and differentiate symptomatic and functional remission criteria.
Conclusion
The therapeutic goals of ADHD should include treatment response and remission. Definitions with specific criteria for syndromatic, symptomatic, and functional remission have been proposed to better characterize the long-term outcomes of ADHD treatment.
Footnotes
Appendix A
Appendix B
Appendix C
Appendix D
Appendix E
Acknowledgements
The authors acknowledge editorial assistance provided by The JB Ashtin Group, Inc. located in Plymouth, Michigan.
Authors’ Note
Dr. Rostain is presently an advisor and consultant to Shire Pharmaceuticals and Ortho-McNeil-Janssen-Pharmaceuticals. In previous years, he has participated in the speakers’ bureaus for these companies and the speakers’ bureau for Eli Lilly. He is also coauthor of Cognitive Therapy for Adult ADHD published by Routledge, Taylor & Francis Group. Dr. Jensen receives grant funding from National Institute of Mental Health (NIMH) and Agency for Healthcare Research and Quality (AHRQ), Casey Family Programs, and the Marriott Foundation. He is a consultant for Shire Pharmaceuticals and receives honoraria for books he has authored or edited from various publishing houses. Dr. Connor is a consultant for Supernus and Shire Pharmaceuticals. He receives grant support from Shire Pharmaceuticals and other support from NIMH and the State of Connecticut. Dr. Miesle is an employee of The JB Ashtin Group, Inc. Dr. Faraone has in the past year received consulting fees and has been on advisory boards for Eli Lilly, Ortho-McNeil, and Shire Development. He has also received research support from Shire and the National Institutes of Health. In previous years, he has received consulting fees or has been on advisory boards or has been a speaker for Shire, McNeil, Janssen, Novartis, Pfizer, Ortho-McNeil, and Eli Lilly. He has received research support from Eli Lilly, Shire, Pfizer, and the National Institutes of Health. He has published a book with Guilford Press, Straight Talk About Your Child’s Mental Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for manuscript development was provided by Shire Development, Inc to the JB Ashtin Group, Inc.