
Abstract
Keywords
Anecdotal reports have indicated a sharp increase in the number of college students with ADHD (Gaddy, 2008); these students rank second behind students with learning disabilities (LDs) as the largest group of postsecondary students served by offices for students with disabilities (Harbour, 2004). In a review of the literature, Advokat, Lane, and Luo (2011) reported that students with ADHD fail more grades, have lower report card scores, have worse scores on standardized achievement tests, take more years to complete high school, and have lower rates of college graduation. As adults, they are less likely to have finished or obtained a degree from a postsecondary school. Interventions for college students with ADHD are important in preventing these negative outcomes. The National Institute of Mental Health (NIMH) Multimodal Treatment of ADHD Study (MTA Cooperative Group, 1999) found that psychosocial treatments in combination with medication resulted in the best outcomes for individuals with ADHD. Among the psychosocial treatments, positive results have been found for cognitive-behavior therapy (CBT)–oriented treatment in adults with regard to attention and related functions of time management, organization, and planning (Mongia & Hechtman, 2012; Ramsay & Rostain, 2006; Safren, Perlman, Sprich, & Otto, 2005; Solanto et al., 2010; Torrente et al., 2014).
An intervention for ADHD that is closely aligned with CBT is ADHD coaching. Despite limited scientific study on ADHD coaching as an intervention for adults and college students with ADHD, this approach has grown significantly and gained popularity in recent years (Dupaul, Weyandt, O’Dell, & Varejao, 2009; Murphy, 2005; Murphy, Ratey, Maynard, Sussman, & Wright, 2010; Prevatt & Lee, 2009; Quinn, 2001). However, the research in this area is quite limited (Murphy et al., 2010). Goldstein (2005) has lamented the lack of empirical research regarding ADHD coaching; he concludes that a critical examination of ADHD coaching is needed that evaluates theoretical underpinnings, definition of basic tenets, efficacy of treatments, and an analysis of costs and side effects.
Review of Empirical Studies of ADHD Coaching
There are limited empirical studies of ADHD coaching in adults and college students. Swartz, Prevatt, and Proctor (2005) presented a single case study of a college student engaged in a structured 8-week coaching program. Results indicated improvements on study skills and learning strategies, increased study time, and achievement of personal course-related goals. In a qualitative study of executive functioning (EF) coaching for 54 college students, Parker and Boutelle (2009) reported that coaching led to more positive thoughts and behaviors, such as taking greater responsibility for one’s actions, utilizing goal attainment skills, modulating emotions, and increasing positive expectations for performance. In a pilot study of seven undergraduates, Parker, Hoffman, Sawilowsky, and Rolands (2011) showed effectiveness for a semester-long individualized coaching program that involved phone calls, email, and text messages. Their participants showed improvements in study skills and learning strategies. Prevatt, Lampropoulos, Bowles, and Garrett (2011) found positive results with a sample of 13 college students utilizing between-session assignments (BSAs) in their coaching program. Wentz, Nyden, and Krevers (2012) used 8-week (twice per week) Internet “chat” sessions plus instant messaging with a group of ten 15- to 26-year-olds diagnosed with either ADHD or Autism Spectrum Disorder. They found positive results for the participants’ sense of coherence, self-esteem, and subjective quality of life.
Other studies have evaluated coaching conducted in a group format. Bloemen, Verbeeck, and Tuinier (2007) studied ten 25- to 61-year-olds who took part in an 8-week structured group coaching program. Results showed no significant self-report of improvement for self-esteem, quality of life, or symptom impairment. However, raters noted significant improvement in daily life functioning. Kubik (2010) found positive results with a six-session group coaching intervention for 45 adults aged 40 to 59 that focused on education, anxiety, homework, interpersonal interactions, planning, organization, and assertiveness. Zwart and Kallemeyn (2001) used peers to do group coaching of college students with ADHD and/or LDs. Although they utilized a control group, the control group was not randomly assigned and was composed of significantly more students with LDs than in the coaching group. Gains were found after 2 to 10 sessions of group coaching on self-efficacy, motivation, time management, anxiety, and test-taking strategies. In summary, the empirical studies of ADHD coaching have been positive, yet sample sizes are small and outcome measures limited.
Theoretical Underpinnings
The studies of ADHD coaching reviewed above tend to use two primary theories to guide their coaching programs, CBT and psychoeducation. In addition, newer work utilizes EF as a way of understanding client difficulties and formulating coaching goals. EF is becoming increasingly more popular in the literature as a way of describing the etiology of and the deficits associated with ADHD. Brown (2008) concluded that ADHD is not a behavioral disorder but rather a cognitive disorder due to developmental impairment of executive functions. Barkley (2011; Barkley & Murphy, 2010) has proposed a new schema of EF that uses behavioral ratings of impairment and has published the Barkley Deficits in Executive Functioning Scale (BDEFS), which categorizes EF into the following five domains: Self-Organization/Problem Solving, Self-Management to Time, Self-Restraint or Inhibition, Self-Regulation of Emotion, and Self-Motivation. The schema developed by Barkley for categorizing EF domains is a useful platform for developing and evaluating a coaching program. The behaviors that underlie the BDEFS items are areas of impairment commonly targeted in work with individuals with ADHD.
Psychoeducational strategies focus on educating patients with ADHD about the disorder (e.g., Fields & Hale, 2011), and multimodal approaches to treating ADHD often include psychoeducation (Levrini & Prevatt, 2012; Murphy et al., 2010). For example, it is helpful for those with ADHD to understand the hypothesized biological underpinnings of ADHD; how diet, sleep, and exercise can affect functioning; the importance of medication management; and how to self-advocate for accommodations. It is believed that a combination of cognitive-behavioral and psychoeducational strategies to target the areas of EF impairment outlined in the BDEFS can provide a theoretical and content base to guide ADHD coaching.
The Process of ADHD Coaching
Some authors have suggested that ADHD coaching refers primarily to academic support (Ramsay & Rostain, 2006). However, coaching has evolved to encompass a wide range of CBT techniques that focus on ADHD symptoms that interfere with academic performance and coping with difficulties such as procrastination, lack of concentration, ineffective self-regulation, poor planning, anxiety, social incompetence, or time management (Levrini & Prevatt, 2012). Kubik (2010) described coaching as focusing on behavioral, emotional, and cognitive outcomes and building life skills to change negative outcomes and beliefs. She stated that ADHD coaching “educates adults with ADHD on the outcomes of living with ADHD over a lifetime, making a logical connection to their current cognitive, emotional, and behavioral responses” (p. 443).
The description of ADHD coaching presented by Swartz et al. (2005) describes an eight-session program. Initial sessions include symptom clarification, education, goal setting, establishing the length and type of meetings and between-session communications, and rewards and consequences. Subsequent sessions explore weekly objectives, completion of assignments, obstacles, and problem solving. BSAs are routinely used as a means of accomplishing weekly objectives, which are ultimately tied to long-term goals. Cognitive changes are thought to occur as the result of behavioral interventions brought about by questioning, problem solving, modeling, and practicing (Reaser, 2008). Appendix A gives a list of topics routinely covered in ADHD coaching, with specific content dictated by client and coach collaboration. Each of these elements would be expected to change if they were chosen by the client as his or her specific goals.
BSAs
BSAs, or homework assignments, although most typically associated with CBT, are commonly used by therapists of various theoretical orientations and for a variety of clinical problems (Kazantzis, Lampropoulos, & Deane, 2005). BSAs aim to maximize benefit from treatment by asking clients to engage in self-help tasks between sessions. They typically include assignments that facilitate different change processes, such as gaining awareness and insight into thought patterns and behavioral difficulties, as well as exploring, rehearsing, and implementing solutions to problems. Meta-analytic research has shown that the use of BSAs improves treatment outcome and that client compliance with BSAs is also related to benefits from treatment (Kazantzis, Deane, & Ronan, 2000).
The present study is an evaluation of an ADHD coaching program implemented at a large public university. The theoretical orientation combined CBT with psychoeducational techniques. EF impairment served as a way of viewing both initial problem areas and outcomes. The coaching was a structured 8-week program modeled after Swartz et al. (2005), and BSAs were a core component of the program. Because no control group was utilized, this was considered an exploratory study that can give some preliminary evidence about ADHD coaching structure, processes, efficacy, and correlates of positive outcomes.
Method
Participants
ADHD coaching participants (N = 148) were seen at a psychoeducational training clinic at the campus of a large public university in the Southeast. The study has been in progress for 5 years, with about 10 clients per semester (fall, spring, and summer). With regard to demographics, 49% of the clients were female, and they ranged in age from 17 to 60 (M = 24.6, SD = 9.36). For class year, 13% of the participants were freshmen, 18% sophomores, 19% juniors, 10% seniors, 16% were graduate students, and 5% were not currently enrolled. In terms of ethnicity, 73% of the clients were Caucasian, 8% African American, 2% Asian American, 8% Hispanic, 2% multiracial, and 7% were unknown. Mean grade point average (GPA) was 3.08 (SD = 0.59) on a 4.0 scale, with a range of 1.5 to 4.0. Participants were asked if they had a current diagnosis of ADHD or LDs, and this information was obtained by self-report: 80% reported a diagnosis of ADHD; of those, 55% were inattentive type, 43% were combined type, and 2% were hyperactive/impulsive type. There was a comorbid diagnosis of a specific LD in 28% of the participants. Diagnoses varied, having been provided by medical doctors, psychologists, or as part of a K-12 school-based evaluation. We did not ask for verification of these diagnoses. About half of the clients were self-referred, while half were referred by parents, professors, or other university personnel. The ADHD coaching was an eight-session program, and although some clients missed sessions, the modal number of sessions missed was zero. A total of 26 coaches provided services; 21 were female; 22 were Caucasian, 2 were African American, 1 was Asian, and 1 was Hispanic. All were doctoral-level practicum students who were enrolled in an American Psychological Association–approved, combined PhD program in counseling psychology and school psychology.
Setting
Clients were seen in a university-based training clinic that specializes in assessment and intervention for college students who have academic difficulties. Coaching was provided in the context of a semester-long practicum, with 2 to 3 coaches per semester cosupervised by a doctoral-level licensed psychologist and a master’s-level licensed school psychologist. Prior to beginning the program, coaches completed general coursework and practica in counseling, and did extensive reading and received training regarding the ADHD coaching intervention. A training manual provided specific directions, forms, support materials, and samples of activities and requirements. Each case was discussed each week in supervision, and coaches received continual support and guidance to ensure that they were following the proscribed program.
Procedure
Clients were seen individually, once-per-week, for an 8-week period. The cost of coaching varied slightly over the course of the 5 years, but averaged US$100 for the entire 8-week session. To facilitate attendance, clients were required to pay in advance and were not refunded money if they missed sessions without medical or other necessity. At the beginning of the coaching process, the client completed the Coaching Topics Survey (see “Measures” section), and based on this survey, the coach and client established 2 to 3 long-term goals. The long-term goals were broken down into 3 to 4 short-term, weekly goals. BSAs were written down and utilized to help implement weekly goals. During weekly sessions, the coach and client did regular monitoring for mastery of BSAs and short-term goals, reflected on the attainment of goals, discussed successes and barriers, did problem solving if necessary, and set new or modified goals and BSAs for the coming week. To encourage completion of BSAs, clients were encouraged to use self-rewards, negative consequences, or rewards imposed by the coach or others. Immediately after each session, the coach wrote up case notes and emailed those to the client to facilitate memory of BSAs and help with reflection and mastery (see Appendix B for sample case notes). Between sessions, coaches used prearranged text messages, emails, or phone calls, as needed, to facilitate goal attainment. The use of reminders was gradually faded as clients learned to rely on daily planners instead. Treatment integrity was maintained by utilizing a coaching manual, weekly supervision of all cases, and review of videotapes of coaching.
Measures
New measures were added over the 5 years as the research team determined that additional data would be efficacious. As such, not all instruments described below were utilized for the entire 5-year period. The year in which each measure was implemented is listed in parentheses after each title.
BSA Survey (Year 2)
The BSA Survey (Prevatt et al., 2011) has two forms, one for coaches and one for clients. The coach form contains twelve, 7-point Likert-type scale items regarding the use of BSAs. It is filled out by the coach at the completion of the coaching program and includes items querying for the following: types of BSA used, how assignments were determined, how often written directions were given, usefulness of BSA, and barriers to using BSA. In addition, the survey asks the coach to rate client quality, compliance, time per week, and attitude in completing the BSA. The client form contains six, 5-point Likert-type scale items that query for willingness to utilize the BSAs, difficulty of the BSAs, degree to which BSAs matched weekly goals, specificity and clarity of the BSAs, and usefulness of the BSAs.
Client Symptom Checklist (CSC; Year 2)
The CSC asked respondents to rate symptoms of general anxiety, panic, depression, and ADHD, based on Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) criteria. This checklist was developed by the clinic where ADHD participants were recruited and was given to all clients seen in the clinic. Items depicting generalized anxiety disorder included six items: feeling anxious or worried, difficulty concentrating, restlessness, irritability, sleep disturbance, and being easily fatigued. Items depicting a panic attack included five items: nausea or abdominal distress, fear of losing control, palpitations or accelerated heart rate, trembling or shaking, and shortness of breath or dizziness. Items depicting depression included six items: depressed mood, poor concentration, feeling hopeless, irritable, difficulty sleeping, and feeling sluggish or low energy or fatigued. Items depicting ADHD included 12 items: difficulty following instructions, easily distracted, careless, poor concentration, cannot sit still, poor organization skills, driven by a motor, forgetful, acts without thinking, fails to finish tasks, talks excessively, and difficulty sustaining attention. Clients gave either a 1 (yes, generally experience this symptom) or a 2 (no, do not generally experience this symptom). Lower scores indicate more symptoms. Cronbach’s alpha for the scales were Generalized Anxiety = .70; Panic Attacks = .71; Depression = .78; ADHD = .83.
Coach’s Rating of Motivation and Progress (Year 2)
Within the first 2 weeks of coaching, the coach rated the client on a single-item, 1 to 7 Likert-type scale indicating the motivation of the client. After the eighth and final session, the coach rated the client on a single-item, 1 to 7 Likert-type scale indicating the progress of the client in coaching.
Coaching Topics Survey (Year 1)
The Coaching Topics Survey (Swartz et al., 2005) asked participants what areas they needed to work on, with responses ranging from 1 (definitely need to work on) to 5 (don’t need to work on). There were 27 total items; a partial list of these are improving time management, establishing routines, organizing schoolwork, organizing personal space, getting to class on time, paying attention in class, studying, scheduling classes, managing long-term assignments, planning and prioritizing, doing laundry, exercising, healthy eating, waking up, getting to bed, taking medication, making and keeping friends, getting along with roommates, establishing realistic goals, decreasing negative self-talk, managing stress or anxiety, understanding ADHD, and explaining ADHD to professors.
Learning and Study Strategies Inventory (LASSI), 2nd Edition (Year 2)
The LASSI (Weinstein & Palmer, 2002) asks college students to self-rate their thought processes and behaviors with regard to learning and study strategies. The 80-item test contains 10 eight-item scales (with Cronbach’s α): Anxiety (.87), Attitude (.77), Concentration (.86), Information Processing (.84), Motivation (.84), Self-Testing (.84), Selecting Main Ideas (.89), Study Aids (.73), Time Management (.85), and Test Strategies (.85). The LASSI has been shown to be positively correlated with GPA and is proposed to be an effective tool for predicting academic performance (Yip & Chung, 2002). For each of the 80 items, students are required to choose the letter on a 5-point Likert-type scale that corresponds best to how the statement describes them, from “not at all typical” to “very much typical.” The measure yields a raw score for each of the 10 subscales with higher scores indicating more positive functioning.
Outcome Questionnaire–45 (OQ-45; Year 3)
The OQ-45 (Lambert & Finch, 1999) is a 45-item self-report outcome instrument designed for repeated measurement of client progress through the course of therapy. The OQ-45 measures functioning in three domains: Symptom Distress (heavily loaded for depression and anxiety), Interpersonal Functioning (e.g., getting along with others, satisfaction with relationships) and Social Role (e.g., find school or work satisfying). It enables the clinician to assess functional level and change over time. Convergent validity has been established via correlations with standard measures of depression, anxiety, and interpersonal relations (e.g., Lambert et al., 1996; Umphress, Lambert, Smart, Barlow, & Clouse, 1997). Cronbach’s alpha for the scales are Symptom Distress = .93, Interpersonal Functioning = .80, and Social Role = .94. A higher score indicates more negative functioning.
Rosenberg Self-Esteem Inventory (RSE; Year 1)
The RSE (Rosenberg, 1965) is a 10-item scale that assesses global self-esteem. The RSE is one of the most widely used measures of global self-esteem in social science research today. This 10-item, Likert-type scale has been validated in many groups including college students and adults. The RSE has a 2-week, test–retest reliability in college students of .85 to .88. It also correlates significantly with other self-esteem measures such as the Coopersmith Self-Esteem Inventory and divergently with measures of depression and anxiety (Brown, Chopra, & Schiraldi, 2013; Owens, 2001; Sinclair et al., 2010). It is scored on a 4-point Likert-type scale (1 = strongly agree; 4 = strongly disagree). A higher score indicates higher self-esteem. Cronbach’s alpha for the scale was .89.
Results
Descriptive Analyses
Reasons for Being in Coaching
The Coaching Topics Survey asked participants what areas they needed to work on, with responses ranging from 1 (definitely need to work on) to 5 (don’t need to work on). Because this was a descriptive analysis, means for each of the 27 items were calculated and then rank ordered from low to high. Those areas rated as most needing work, as indicated by a mean of less than 3.0, were as follows: time management (M = 1.47), good habits and routines (M = 1.70), planning and prioritizing (M = 1.70), managing long-term assignments (M = 1.72), organizing schoolwork (M = 1.78), managing stress and anxiety (M = 2.19), establishing realistic goals (M = 2.21), keeping track of things (M = 2.22), organizing personal space (M = 2.30), paying attention and taking good notes (M = 2.43), making decisions and problem solving (M = 2.61), getting to bed (M = 2.69), waking up and staying up (M = 2.79), understanding ADHD (M = 2.88), and explaining ADHD to professors (M = 2.89). Alternately, those areas ranked as not needing work, as indicated by a mean of greater than 4.0, were making friends (M = 4.23) and getting along with roommates (M = 4.19).
BSAs
Coaches rated how frequently they used BSAs for different areas of functioning from 1 (never) to 7 (always). For this descriptive analysis, means were calculated for the six different areas of functioning and then rank ordered from high to low. BSAs were rated as being used “usually” or “always” for working on course homework (M = 5.03), studying for courses (M = 4.53), and time management (e.g., using a planner, making reminders, keeping appointments; M = 4.52). BSAs were used “sometimes” for organizational activities (e.g., putting things in folders, cleaning or organizing personal space; M = 3.26) and engaging in a healthy lifestyle (e.g., eating well, developing a sleep schedule, exercising, taking ADHD medication; M = 2.62). BSAs were almost “never’ used for social activities (working on friendships; M = 1.87).
Coaches also rated the five potential barriers to using BSAs on a 1 (never) to 7 (always) scale. Analysis of means, in order of frequency, showed that coaches gave the following reasons why clients did not complete BSAs: poor time management (M = 3.29), client forgot (M = 2.73), fear or avoidance of the BSA (M = 2.63), general unwillingness (M = 2.05), and lack of ability to complete the BSA (M = 1.66).
Pre–Post Coaching Gains
General linear models (GLM) repeated-measures ANOVA was used to analyze the pre–post differences for the three dependent measures: LASSI (10 subscales), RSE (total score), and OQ-45 (total score and three subscales). The repeated measure was time, and thus the repeated measure procedure models the correlation between the pre- and post-tests. Three separate ANOVAs were chosen because not all participants had data for all three measures. There were significant pre- to posttreatment effects for all variables with the exception of the OQ-45 subscale for interpersonal relations. For example, Time Management increased from a mean of 17.26 to 24.30 (F = 38.94, p < .001, d = .89); Concentration increased from a mean of 18.46 to 23.50 (F = 20.96, p < .001, d = .76); and Social Role (e.g., finding school or work unsatisfying) decreased from a mean of 14.58 to 11.48 (F = 14.30, p < .01, d = .83). Full results can be seen in Table 1.
Pre–Post Group Effects for LASSI, Self-Esteem, and Overall Functioning.
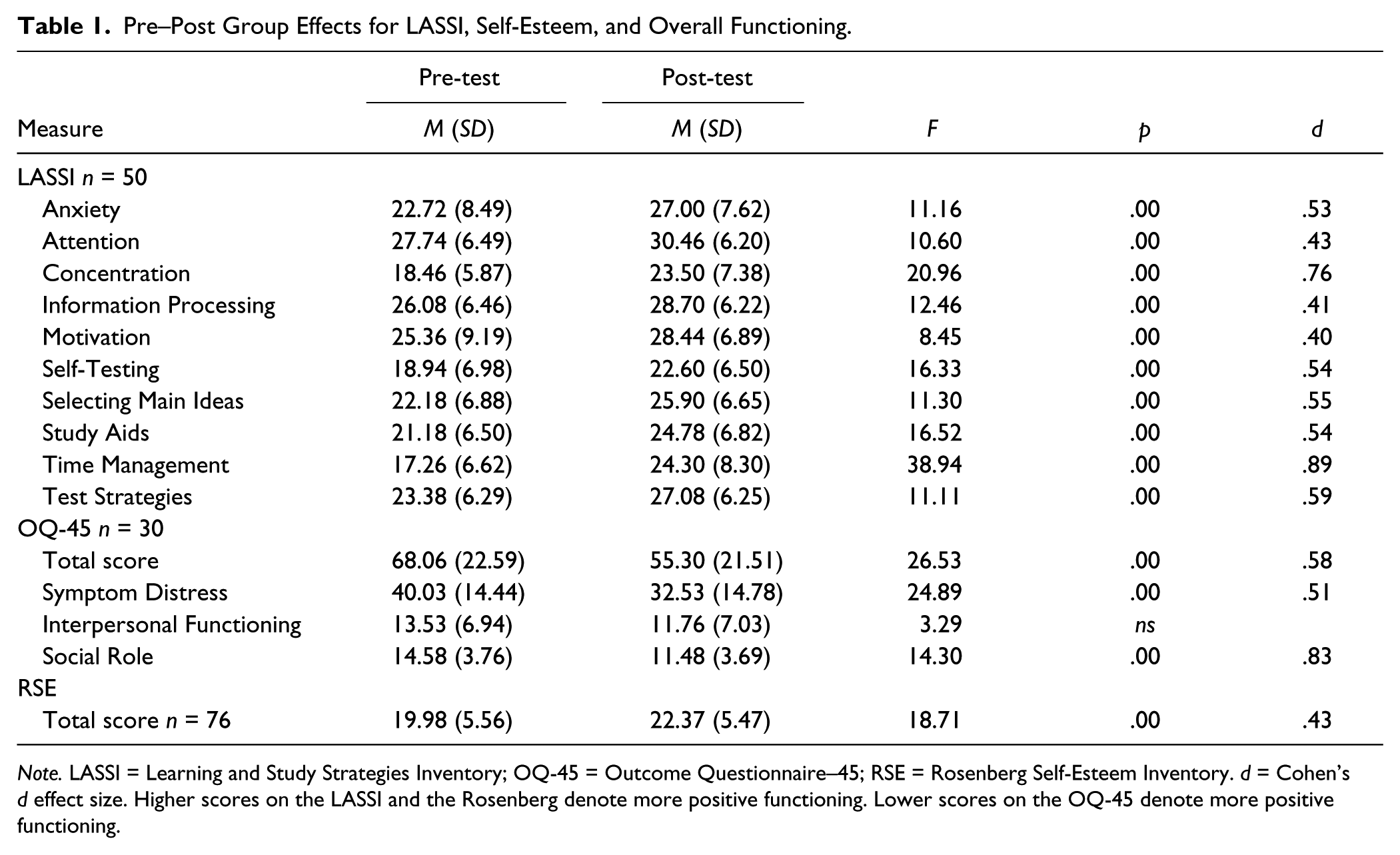
Note. LASSI = Learning and Study Strategies Inventory; OQ-45 = Outcome Questionnaire–45; RSE = Rosenberg Self-Esteem Inventory. d = Cohen’s d effect size. Higher scores on the LASSI and the Rosenberg denote more positive functioning. Lower scores on the OQ-45 denote more positive functioning.
The Process of Coaching
This series of analyses involved continuous variables that were hypothesized to be related to one another, and therefore Pearson correlations were utilized.
Coach Rating of Progress in Therapy
The coach rating of progress in therapy was significantly positively correlated with coach ratings of initial motivation to be in treatment (r = .53, p < .00), compliance with the BSAs (r = .65, p < .00), quality of the BSAs (r = .70, p < .00), and attitude toward the BSAs (r = .77, p < .00).
Correlates of Positive Change Related to BSA Use
Change scores were created by subtracting pre-test from post-test for the 10 subscales of the LASSI. These change scores were then analyzed using Pearson correlations with BSA client variables (willingness to use BSA, degree to which BSA matched weekly goals) and therapist variables (initial motivation to be in treatment, BSA compliance, BSA quality, and time per week spent doing BSA). As can be seen in Table 2, clients who rated the BSAs as being a better match with their personal coaching goals showed more positive changes on test strategies. Clients who were more willing to try the BSAs showed more positive changes on anxiety and attention. With regard to coach ratings, when coaches gave initial ratings of client motivation that were higher, the clients showed more positive changes on attention and time management. When coaches gave higher ratings of client compliance with the BSAs, the clients showed more positive changes on anxiety, concentration, and test strategies. When coaches gave higher ratings of client quality on the BSAs, the clients showed more positive changes on anxiety, concentration, selecting main ideas, and test strategies. When coaches gave higher ratings of time commitment per week to the BSA, the clients showed more positive changes on anxiety, selecting main ideas, and test strategies.
Pearson Correlations Among LASSI and Client and Coach Ratings of BSA.
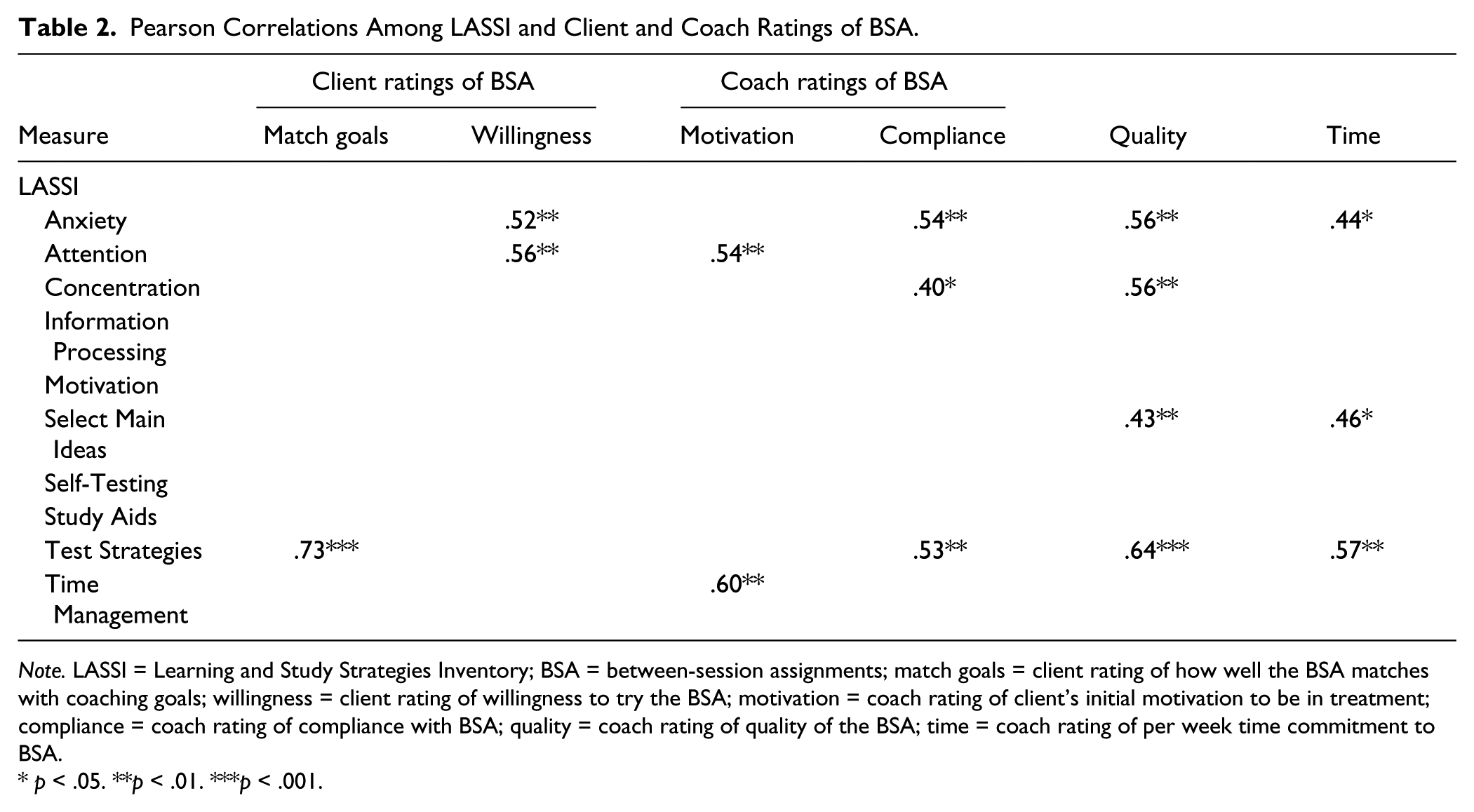
Note. LASSI = Learning and Study Strategies Inventory; BSA = between-session assignments; match goals = client rating of how well the BSA matches with coaching goals; willingness = client rating of willingness to try the BSA; motivation = coach rating of client’s initial motivation to be in treatment; compliance = coach rating of compliance with BSA; quality = coach rating of quality of the BSA; time = coach rating of per week time commitment to BSA.
p < .05. **p < .01. ***p < .001.
Correlates of Positive Change Related to Initial Symptoms
The 10 LASSI change scores were correlated with initial symptoms of anxiety, panic, depression, and ADHD (based on the CSC) to see whether level of initial functioning affected postcoaching changes in self-perceptions of learning and study strategies. Positive changes in the LASSI test strategies, time management, use of study aides, selecting main ideas, and anxiety were all associated with lower initial client self-ratings of symptoms of depression (rs = .40, .31, .37, .34, and .28, respectively) and lower initial client self-ratings symptoms of anxiety (rs = .31, .31, .46, .32, and .28, respectively). In addition, positive changes in the LASSI test strategies, use of study aides, and selecting main ideas were all associated with lower initial client self-ratings of symptoms of ADHD (rs = .39, .36, and .40, respectively).
Discussion
The present study was an evaluation of an ADHD coaching program for college students, implemented over a 5-year period. The theoretical orientation combined CBT with psychoeducational techniques. This was considered an exploratory study that could give some preliminary evidence about ADHD coaching structure, processes, efficacy, and correlates of positive outcomes. It was hypothesized that participants would show pre–post improvements in study and learning strategies, self-esteem, emotional distress, and satisfaction with school and work. All hypotheses were supported. Largest effect sizes were found for time management and concentration, two areas important for students with ADHD. These results were consistent across 5 years of coaching, across different semesters and time of semester, and with a variety of different coaches, all of whom were novice coaches. The learning and study strategies are important as they reflect critical skills for college students. The areas of functioning measured by the LASSI reflect behaviors, attitudes, motivations, and beliefs that relate to successful learning in postsecondary educational settings. According to Weinstein and Palmer (2002), three primary areas measured include skills (summarize assignments, identify key points, study for tests), the will to learn (lack of anxiety, positive attitude, perseverance and motivation in difficult classes), and self-regulation (concentration, attention, time management, and use of support techniques). Many studies have shown that these strategies predict success in college (Prus, Hatcher, Hope, & Grabiel, 1995; Schumacker, Sayler, & Bembry, 1995). We do not have postcoaching grades to confirm that changes in strategies are correlated with changes in grades; however, it is likely that the areas measured by the LASSI are important for students with ADHD. Prior research has found that college students with a diagnosis of ADHD show poorer performance in general on the LASSI (Reaser, Prevatt, Petscher, & Proctor, 2007), while other ADHD coaching studies have utilized the LASSI as a measure of EF (Parker & Boutelle, 2009).
Increases in self-esteem and decreases in symptoms of distress (anxiety and depression) are also important results, as research has shown the importance of both self-esteem and personal issues in college adjustment and performance (Pancer, Hunsberger, Pratt, & Alisat, 2000; Robbins, Allen, Casillas, Peterson, & Le, 2006). A large effect size was found for the OQ-45 measure of social role, which indicates satisfaction with work or school functioning. The only outcome variable not significantly changed after the 8 weeks of coaching was the OQ-45 measure of interpersonal relations. This is likely because peer relations were rarely the focus of coaching. Making friends and getting along with roommates were the two items on the Coaching Topics Survey rated by clients as least likely to need work. Also, friendships and social issues were rated by the coaches as least likely to be the focus of BSAs.
In addition to finding that coaching was associated with positive gains in symptoms of distress (as measured by the OQ-45), our results also revealed that those clients who gave higher precoaching ratings of depression or general anxiety (on the CSC) were less likely to make positive postcoaching gains on a variety of study strategies (e.g., test-taking strategies, time management, use of study aides, and selecting main ideas). We would hypothesize that this is partially due to the fact that time used in sessions to deal with issues of depression or anxiety took away from time spent on academic issues. The coach may have planned to spend a session working on organization or time management; however, if a client came in severely depressed or anxious, the session could be derailed until the current distress was dealt with. It has been well documented that ADHD is often comorbid with multiple psychiatric disorders, such as depression and anxiety (Schatz & Rostain, 2006). This is often an issue in our coaching clients, and we make it clear to them that coaching is not mental health counseling. We strongly encourage clients to seek counseling from the university student counseling center if needed. In summary, our results confirm that those clients with fewer issues of comorbid anxiety and depression will benefit more from the coaching, and that coaching is associated with reduced symptoms of psychological distress.
EF
The areas most commonly selected by clients to work on involved school functioning, which is not surprising for a college population. The specific areas selected to work on were consistent with Barkley’s five domains of EF. Appendix C illustrates how the five EF domains line up with the areas chosen by clients to work on, as well as CBT principles utilized in the coaching. EF is a useful paradigm for organizing ADHD coaching, as it aligns well with common areas of impairment as well as CBT techniques for intervention. Barkley (2010) suggested several intervention strategies for EF impairments that could be integrated into ADHD coaching. He advocates training in working memory with specific skill builders. Arranging someone’s setting so it boosts or facilitates EF can include activities such as writing notes and making to-do lists. These types of activities play a crucial role in facilitating self-regulation. Those with ADHD have limited capacity for EF and self-control; therefore, activities to replenish the EF “fuel tank” such as frequent breaks and regular exercise are important. Overall, according to Barkley, the key is to compensate for the EF impairment; the deficits will not go away, but individuals can be trained to cope with them. In the current study, EF measures were implemented in Year 4 of the 5-year project, making it premature to have sufficient outcome data; however, the BDEFS seems promising as a way of viewing EF and an efficient tool to measure pre–post coaching gains.
BSAs
The process of coaching was evaluated by examining correlates of BSA usage. BSAs are an integral part of the coaching. Some sample BSAs can be seen in Appendix D. Positive coaching outcomes were associated with numerous aspects of BSA use, indicated by both client and coach ratings. Clients who believed the BSAs to match well with their personal coaching goals showed improvement on test-taking strategies and clients who indicated willingness to try BSAs showed an improvement in attention and a decrease in anxiety. With regard to coach ratings, three different measures of BSA use (compliance, quality, and time commitment) were associated with client improvement on concentration and test-taking strategies, and a decrease in anxiety. These findings are consistent with prior work by Prevatt et al. (2011), who found that overall progress in ADHD coaching was significantly correlated with therapist ratings of BSA quality, usefulness, and client attitude. As seen in Appendix C, BSAs are thought to line up with two areas of EF, problem solving and motivation. BSAs are mutually decided upon by client and coach, and a standard problem-solving approach is utilized. The process of determining the BSA helps teach the client problem-solving skills, and engaging in the BSA with its associated rewards serves as motivation for the client.
Lessons Learned
Important information was learned from this 5-year development of a coaching program. Motivation is important to the success of coaching. Initially, we allowed students to sign up for coaching when a parent called to initiate their registration. We learned that the majority of these students were not themselves motivated, and they tended to miss sessions and failed to complete many of the BSAs. We began accepting clients only when they made the effort themselves to complete all registration activities. Payment also appeared to be tied to motivation. We tried to strike a balance between creating an incentive to attend versus not pricing the coaching out of the reach of students. It appeared that somewhere between US$75 and US$250 for the entire 8-week session was an optimal range. We learned that requiring students to pay up-front benefited attendance, as did not returning money if sessions were missed (except in documented medical or other emergencies). The use of BSAs appeared to facilitate compliance, increase motivation, and teach new skills. We learned that the BSA plan needed to be “owned” by the client. The coach might believe that a certain behavior would be beneficial, but unless it was the client’s plan, it was not likely to work. Finally, writing case notes and emailing them to clients after sessions also served as a motivator, and clients anecdotally told us that they valued these notes.
Limitations and Future Work
A primary limitation to the current study is the lack of a control group. However, uncontrolled studies can nonetheless demonstrate important information about efficacy, feasibility, and acceptability of CBT-oriented interventions (Mongia & Hechtman, 2012). Beginning in 2012, we implemented a new procedure whereby each semester is divided into two 8-week sessions. Coaching clients are identified at the beginning of the semester and randomly assigned to immediate versus wait-list coaching conditions. The wait-list clients serve as the control group and begin their coaching during the second half of the semester. This randomized controlled design will be an important next step in evaluating the efficacy of coaching. A second limitation is the generalizability of the sample. College students are a very selective group and are likely higher in certain characteristics than those individuals with ADHD who do not attend college (e.g., motivation, persistence, EF). Future studies need to replicate our findings with noncollege student adults with ADHD. We did not have a measure of medication status of the coaching client. This would be a possible confound if those students who showed more positive results were those who had also begun a medication regime. Future studies need to evaluate medication status. Other areas that were not measured in a structured way were whether participants used self-rewards, number of participants with diagnoses of anxiety and depression, and perceived usefulness of written notes given to clients.
Finally, the coaches in this study were all novice coaches, and due to the large number of coaches, it was not possible to determine how much variation in outcomes could be attributed to individual differences among coaches. On the positive side, if we were able to achieve positive results with graduate students who were novices to coaching, then it could be anticipated that more experienced coaches would have even greater success.
Footnotes
Appendix A
Appendix B
Appendix C
Appendix D
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.