
Abstract
Introduction
Injuries are one of the major public health problems. Among children and adolescents in the United States, they are the leading cause of deaths (Miniño, 2010). In Europe, injuries represent 23% of all-cause deaths and 19% of all-cause DALYs (i.e., disability-adjusted life years) among these age groups (Valent, Little, Tamburini, & Barbone, 2004). Thus, investigation of the underlying factors and identifying groups of children prone to injuries are needed for injury prevention. One of the risk groups might be those suffering from ADHD. Specifically, its symptoms of hyperactivity-impulsivity may be related to risk-taking behaviors and reduced parental supervision. However, in spite of a body of literature linking injury risk and inattention/hyperactivity symptoms together, findings are still controversial.
Cross-sectionally, children with ADHD had injuries more often than those without it in clinical (Hoare & Beattie, 2003) and epidemiological samples (Lee, Harrington, Chang, & Connors, 2008). The latter study adjusted the association for gender, age, race, number of children in family, and family poverty (Lee et al., 2008). Hoare and Beattie (2003) also found that children with ADHD attended emergency department more frequently—indicating recurrent injuries—than other children. Also, significant cross-sectional associations between ADHD and the risk of injury (Pastor & Reuben, 2006), and specifically between ADHD and the risk of fracture (Rowe, Maughan, & Goodman, 2004), have been found in children. These two studies adjusted the risk for several psychosocial factors such as age and gender as well as for other psychopathology, but relied on parental information on injuries, which may result in recall bias, and the severity of injury may also remain unclear.
However, among school-aged pediatric patients, parental information on inattention and/or hyperactive-impulsive symptoms was cross-sectionally more often linked with hospital-treated injury than with appendicitis (Maxson, Lawson, Pop, Yuma-Guerrero, & Johnson, 2009) and more often with extremity fracture than with other orthopedic conditions (Uslu, Uslu, Eksioglu, & Ozen, 2007). On the other hand, clinically unrecognized symptoms of ADHD in children and adolescents were not associated with injuries treated in emergency department (Pittsenbarger, Grupp-Phelan, & Phelan, 2008). Even if neither ADHD nor oppositional defiant disorder (ODD) was separately associated with emergency department–treated injuries among preschoolers, the combination of these two conditions was associated with injury-risk-taking behaviors (Garzon, Huang, & Todd, 2008).
Longitudinally, severe injuries—especially intracranial injuries and skull fractures—as well as recurrent injuries have been linked with ADHD in a retrospective cohort study examining medical claims to an insurance company (Merrill, Lyon, Baker, & Gren, 2009) among participants aged 0 to 64. Rowe, Simonoff, and Silberg (2007) reported cross-sectional and longitudinal data revealing a significant association between impulsivity and anxiety symptoms and the risk of injury. According to the review of Fritz and Butz (2007), ADHD and behavioral disorders together increase the risk of subsequent burn morbidity in children. Thus, they suggested prevention programs including increased supervision of children with these problems.
In addition to controversies in previous studies, medication for ADHD or psychosocial factors was not adjusted in many of them. Furthermore, a congruent diagnosis of ADHD is not necessarily warranted due to the use of different screens or data sources. The same applies to injuries if research relies on parental recall of injuries. Also, the severity of injury may remain unclear. In the present study, we utilized data from a large unselected prospective birth cohort and studied the risk of hospital-treated injuries related to the symptoms/diagnosis of ADHD by adjusting several contributing factors. We also studied whether the symptoms or diagnosis of ADHD are related to injuries and whether the types of injuries vary by symptoms or diagnosis of ADHD during childhood and adolescence.
Method
Study Sample and Procedure
The study population was composed of the population-based Northern Finland Birth Cohort (NFBC) 1986, collected from the two northernmost provinces in Finland (Oulu and Lapland). It comprises 9,432 live-born infants (and 47 stillbirths) whose expected date of birth fell between July 1, 1985, and June 30, 1986 (Järvelin, Hartikainen-Sorri, & Rantakallio, 1993). Mothers (99% of all pregnant women in the area) were recruited via the national Well Baby Clinics at their first prenatal visit, which usually took place by the 12th gestational week. The cohort members have been prospectively followed since the prenatal period, with follow-ups at birth and at ages 7 to 8, 15, and 16 to 18 years.
Information about sociodemographic factors was collected from the parents at all follow-ups. At the age of 16 to 18, clinical examination with a psychiatric interview was conducted among a subpopulation (n = 457) of the adolescents. The study was approved by the Ethical Committee of the Northern Ostrobothnia Hospital District, and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the parents and the adolescents.
Assessment of Hyperactivity Symptoms in Childhood
Teachers (N = 8,525) provided information on emotional, behavioral, and hyperactivity problems of the children aged 8 with the 26-item Rutter Children’s Behaviour Questionnaire for Teachers (RB2; Rutter, 1967). Symptoms of hyperactivity were assessed with the RB2 Hyperactivity subscale of 3 items (i.e., restlessness/difficulty staying seated, fidgety, short concentration ability) rated as “certainly applies,” “applies somewhat,” or “does not apply” with scores of 2, 1, and 0, respectively. The RB2 has shown good validity in a Finnish epidemiological sample of 8-year-old children (Kresanov, Tuominen, Piha, & Almqvist, 1998). In the present study, a cutoff of 3 (the 90th percentile of the distribution of scores) in the Hyperactivity scale was used to define those with problems.
Assessment of Inattention and Hyperactivity Symptoms in Adolescence
At the age of 15, parents (N = 6,985) provided information on inattention and hyperactivity symptoms of the adolescents using the Strengths and Weaknesses of ADHD symptoms and Normal Behavior questionnaire (SWAN; Swanson et al., 2001). The 18 ADHD items in SWAN correspond identically to the 18 ADHD symptoms described in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) compiling the Inattentive (Items 1-9), Hyperactive-Impulsive (Items 10-18), and Combined (Items 1-18) subscales. These symptoms are translated into a 7-point statement scale, where average behavior is rated as 0. SWAN measures problems lasting for at least 1 month with a continuum from skills to problems, unlike most ADHD symptom rating scales. It is well applicable in community samples, where it is found to be normally distributed (Hay, Bennett, Levy, Sergeant, & Swanson, 2007; Polderman et al., 2007; Swanson et al., 2001). In the present study, Swanson’s recommendation of the 95th percentile as a cutoff point for problems was followed in each subscale (Swanson et al., 2001). One missing item in each subscale was allowed and replaced with the mean of that subscale for the adolescent. After excluding nonvalid questionnaires and those who refused the use of their data, SWAN from 6,111 participants was available.
Assessment of the Diagnosis of ADHD in Adolescence
For setting the diagnosis of ADHD, all adolescents exceeding the 95% cutoff in any of the three ADHD subscales in SWAN and living in the Northern Finland (n = 487, cases) and a random sample of those scoring up to the 90th percentile (n = 315, controls) were invited to take part in a clinical examination at the ages of 16 to 18. After exclusion of those with a genetic syndrome or mild mental retardation, the subpopulation was formed of the participants including altogether 457 adolescents. They comprised the study population when the diagnosis of ADHD was studied. During the day of clinical examination, first the parents and then the adolescents were interviewed using the Finnish translation of the semistructured Schedule for Affective Disorders and Schizophrenia for School-Age Children, Present and Lifetime Version (Kiddie-SADS-PL; Kaufman et al., 1997) by master-level interviewers blind to the adolescents’ screening status. These interviews provided clinical DSM-IV (APA, 1994) diagnoses. Altogether, 105 adolescents met current diagnosis of ADHD. More information about the ADHD study is reported elsewhere (Smalley et al., 2007).
Assessment of Injury
Information on injuries of the cohort members between years 1985 and 2001 (i.e., between ages 0 and 15) was obtained from the Finnish Hospital Discharge Register (FHDR). It includes information on all admissions to hospitals, emergency departments, and public health care centers with discharge dates and diagnoses. The following International Classification of Diseases (ICD)–8 codes were used: 800 to 989; the following ICD-9 codes were used: 800 to 999; and the following ICD-10 codes were used: S00-T98 and V01-Y98 (World Health Organization, 1993). Only the first hospital visit of an individual with the same diagnosis code was examined, as several visits under the same diagnosis code could be due to the same injury that we were not able to detect.
Variables and Confounders
The outcome consists of hospital-treated injuries at ages 0 to 15 years. They were categorized into two by time of incident, that is, injuries between ages 0 and 6 and those between ages 7 and 15, and into four by their type, that is, intracranial injuries, fractures, intoxications (drug/drug-like or nonmedical substance), and other injuries. No information was available on the causes of different types of injury. Symptoms for hyperactivity measured with RB2 at age 7 were used as explanatory variable for injuries between ages 0 and 6 and symptoms of ADHD measured with SWAN at age 15 were used for injuries between ages 7 and 15, while the DSM-IV (APA, 1994) diagnosis of ADHD was investigated as explanatory variable for both of these time-related injury groups. To study confounding, we used several covariates, including gender, number of children in the family, family structure, and social status of the family, obtained from parents’ questionnaire (Table 1). According to earlier literature, these covariates were associated with the outcome and explanatory variables (Lee et al., 2008; Pastor & Reuben, 2006; Rowe et al., 2004). In addition, parents reported the use of any psychoactive medication in their offspring at the age of 15. Based on that information, none of the participants received stimulant medication for ADHD at that time.
Demographic Characteristics of the Sample (N = 6,111).
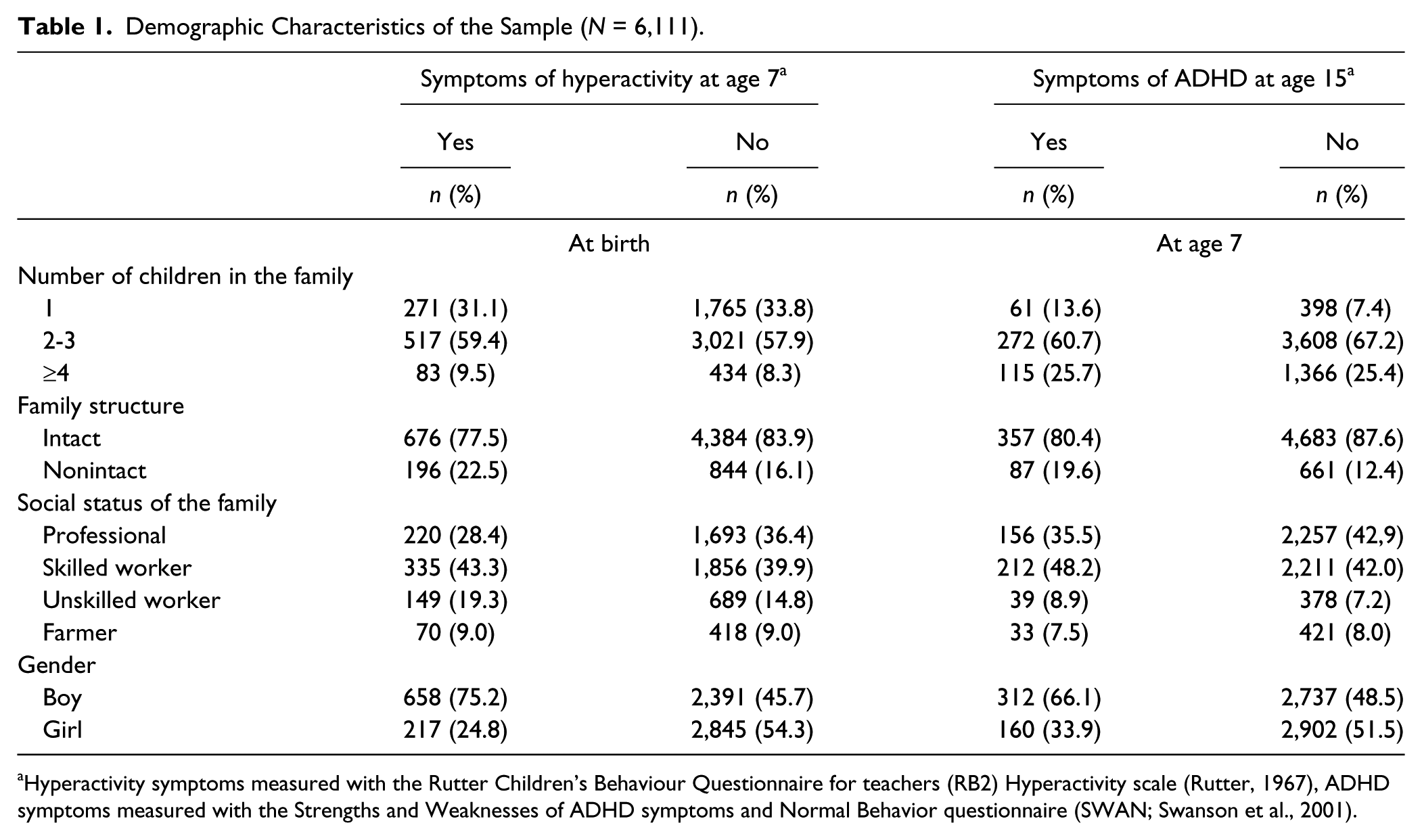
Hyperactivity symptoms measured with the Rutter Children’s Behaviour Questionnaire for teachers (RB2) Hyperactivity scale (Rutter, 1967), ADHD symptoms measured with the Strengths and Weaknesses of ADHD symptoms and Normal Behavior questionnaire (SWAN; Swanson et al., 2001).
Statistical Procedure
The Cox proportional hazard model with hazards ratios (HRs) and their 95% confidence intervals (CIs) was used when studying the injury risk related to the symptoms/diagnosis of ADHD. Crude and multiple-adjusted HRs were calculated. The analyses were performed using the SAS 9.2 TS for Windows (SAS Institute Inc., Cary, North Carolina, USA).
Results
The Occurrence of Injuries
According to the information from the FHDR, there were 932 (15.3%) hospital admissions due to injuries among the cohort members having SWAN available (N = 6,111) by the end of the year 2001, that is, by the age of 15. The most common injuries were fractures (n = 377) and intracranial injuries (n = 127), followed by intoxications (n = 97, 18 of which were due to alcohol) and other injuries (n = 331). Altogether, 512 (73.6%) children had one hospital visit due to injury, 131 (18.8%) had two visits and 53 (7.6%) had three or more visits, the maximum visits per child being 6. There were no significant differences in the mean number of injuries (1.5, SD 0.8, vs. 1.3, SD 0.7, ns) or mean age at first injury (3.3, SD 2.0 years, vs. 3.5, SD 1.9 years, ns) between those with or without symptoms of ADHD at the age of 15.
The Association Between Injuries and Symptoms of ADHD
When injuries requiring a hospital visit from infancy to 6 years of age were the outcome, the risk of any injury was higher among those with symptoms of hyperactivity (RB2) at the age of 7 compared with others (crude HR 1.70, 95% CI = [1.28, 2.26]; adjusted HR 1.41, 95% CI = [1.03, 1.93]; Table 2). This was true for intoxications (crude HR 1.9, 95% CI = [1.04, 3.47]), other injuries (crude HR 2.06, 95% CI = [1.35, 3.14] and adjusted HR 1.61, 95% CI = [1.00, 2.61]), and for intracranial injuries (crude HR 2.4, 95% CI = [1.29, 4.46] and adjusted HR 2.1, 95% CI = [1.05, 4.15]), the latter remaining clearly significantly higher even after multiple adjustments. The risk of fractures did not differ by hyperactivity (Table 2).
Injury Risk (HR With 95% CI) According to the Type of Injury and Time of Incident With Respect to Symptoms of Hyperactivity or Symptoms of ADHD.
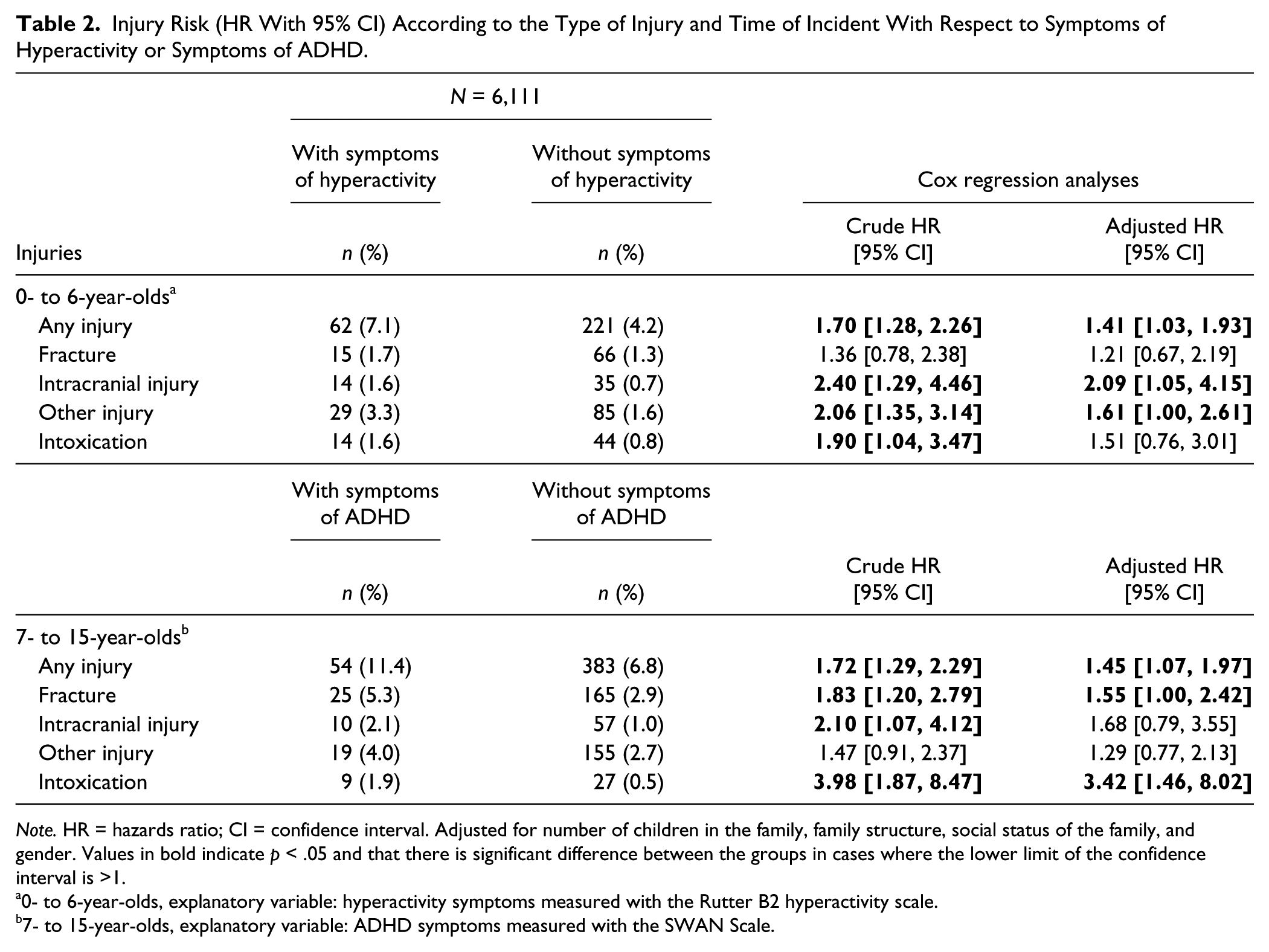
Note. HR = hazards ratio; CI = confidence interval. Adjusted for number of children in the family, family structure, social status of the family, and gender. Values in bold indicate p < .05 and that there is significant difference between the groups in cases where the lower limit of the confidence interval is >1.
0- to 6-year-olds, explanatory variable: hyperactivity symptoms measured with the Rutter B2 hyperactivity scale.
7- to 15-year-olds, explanatory variable: ADHD symptoms measured with the SWAN Scale.
When injuries among 7- to 15-year-olds were investigated, the risks among those with symptoms of ADHD defined by SWAN were increased for any injuries (crude HR 1.72, 95% CI = [1.29, 2.29]), fractures (crude HR 1.83, 95% CI = [1.20, 2.79]), and intracranial injuries (crude HR 2.10, 95% CI = [1.07, 4.12]), but only HR for intoxication (crude HR 3.98, 95% CI = [1.87, 8.47]; adjusted HR 3.42, 95% CI = [1.46, 8.02]) remained clearly significant even after multiple adjustments. These results were similar for both genders and for both those with inattentive symptoms dominating and those with hyperactive-impulsive symptoms dominating. Our results were also similar for those with both hyperactivity symptoms at age 8 years and symptoms of ADHD at 15 years.
The Association Between Injuries and Diagnosis of ADHD
Further analyses were carried out using the data from the subpopulation, that is, those who participated in the clinical interviews focusing on ADHD at the ages of 16 to 18 (n = 457). During their first 6 years of life, those with a later diagnosis of ADHD did not differ from the others in terms of incidence of injuries during 0 to 6 years (5.2% vs. 5.6% for any injury; Table 3). However, from the age of 7 to the age of 15, those with a later diagnosis of ADHD had significantly more injuries than others (15.5% vs. 8.7% for any injury; crude HR 1.82, 95% CI = [0.97, 3.41]; adjusted HR 2.33, 95% CI = [1.20, 4.51]).
Injury Risk (HR and 95%CI) According to the Type of Injury and Time of Incident With Respect to Diagnosis of ADHD.
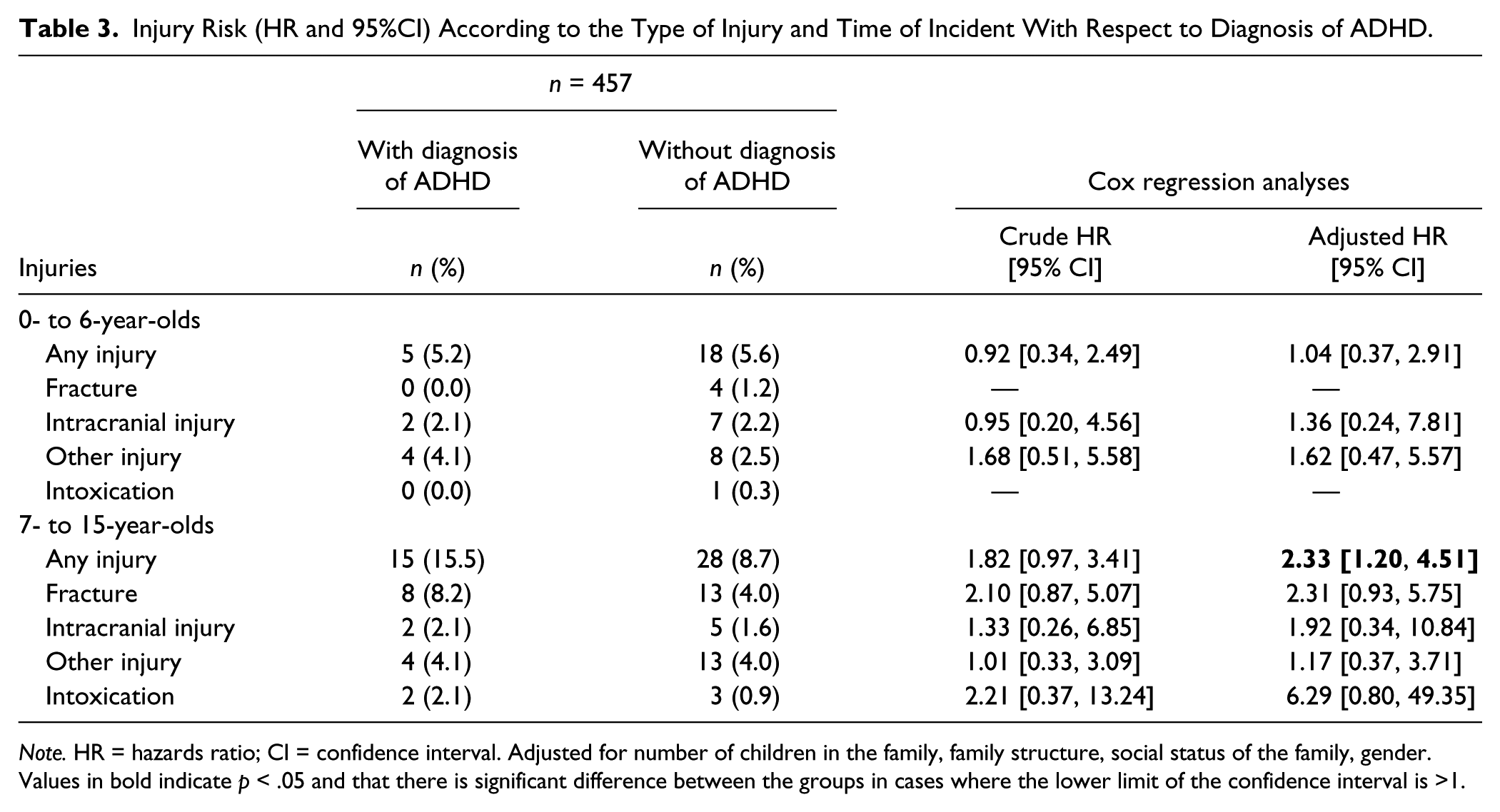
Note. HR = hazards ratio; CI = confidence interval. Adjusted for number of children in the family, family structure, social status of the family, gender. Values in bold indicate p < .05 and that there is significant difference between the groups in cases where the lower limit of the confidence interval is >1.
Discussion
The present study shows an association between injuries requiring hospital treatment and the symptoms or diagnosis of ADHD in a large epidemiological sample of children and adolescents. In a younger age group (0-6 years), the risks for having any injury or specifically intracranial injury were increased among those with hyperactivity symptoms. Similarly, in an older age group (7-15 years) the risks for having any injury, fracture, or intoxication were increased among those with the symptoms of ADHD. Getting a diagnosis of ADHD was associated with more than twofold increase of injury risk between ages 7 and 15.
The type of injury played a role with respect to ADHD symptoms in the present study. Previously, fractures and intracranial injuries have been associated with ADHD (Merrill et al., 2009; Rowe et al., 2004). These injuries may reflect “always-on-the-go” personality of a child, but they may also indicate poor attention skills to notice the hazards of environment or impulsivity to engage in dangerous activities. However, fractures and intracranial injuries among small children may also reflect poor parenting supervision, which may increase the risk of injury among children with behavioral disorder (Schwebel, Hodgens, & Sterling, 2006). It might be that due to considerable genetic etiology (e.g., Biederman & Faraone, 2002), parents of children with ADHD might have reduced supervision abilities because of their own problems in executive functions.
Among older children and adolescents, intoxication was common as well. The fact that intoxication among this population was partly due to alcohol overdose is in line with earlier findings in the Oulu University Hospital catchment area, reporting that more than 70% of hospital admissions due to self-poisoning among 12- to 18-year-old adolescents were due to ethanol poisoning (Liisanantti, Ala-Kokko, Dunder, & Ebeling, 2010). However, ADHD is linked with alcohol abuse in our area (Hurtig et al., 2007) as well as elsewhere (Angold et al., 1999). Presumably, inattention and impulsivity may lower the threshold to drink alcohol and increase the risk for overdose. It is also plausible that adolescents with ADHD are susceptible to peer influence in terms of heavy drinking. However, some cases of intoxication and injuries in the present study may also reflect suicidal behavior. In a clinical population sample, traumatic injuries, especially recurrent ones, were associated with subsequent psychiatric treatment and increased suicide rate among boys (Ebeling, Vuokko, & Moilanen, 2003). Suicidal behavior was also common among those with ADHD in the NFBC 1986 (Hurtig, Taanila, Moilanen, Nordström, & Ebeling, 2012).
The results of the present study were similar with respect to symptoms as well as diagnosis of ADHD, although the size of the latter study population was quite small and therefore had smaller study power. As hyperactivity measured with the RB2 Hyperactivity scale at the age of 8 years may not be a marker for adolescent diagnosis of ADHD, this indicates the need for studying hyperactivity symptoms separately from symptoms of ADHD. This was done in the present study, showing that both of them were related to proneness for injuries. Both the core components of ADHD, that is, inattentiveness and hyperactivity-impulsivity, seem to be related to injuries, although the mechanisms may differ.
The association between ADHD and subsequent injury needs a prospective and bidirectional approach. Our design, although longitudinal, was mainly retrospective, with the occurrence of lifetime childhood injuries studied among those with symptoms of ADHD at age 8 or 15. The associations could also occur the other way round. Brain injury in childhood preceded subsequent behavioral symptoms such as those of ADHD (Levin et al., 2007; Max et al., 2005; McKinlay, Grace, Horwood, Fergusson, & MacFarlane, 2010; Wassenberg, Max, Lindgren, & Schatz, 2004). Retrospectively, in a cohort of more than 60,000 children, a head or a burn injury before age 2 increased the risk of ADHD before age 10 (Keenan, Hall, & Marshall, 2008). The authors, however, concluded that an injury, but not specifically a head injury in early childhood, may be more of a marker than a causal factor for subsequent diagnosis of ADHD. Some studies have failed to find longitudinal associations of this kind, such as that of Rowe et al. (2007) which found no association between injury and later impulsivity and anxiety. However, preinjury behavioral and psychosocial characteristics of a child should be taken into account to seek out previously unnoticed symptoms (Levin et al., 2007; Wassenberg et al., 2004).
Strengths and Limitations
The main strength of the present study is a large, unselected, population-based sample with reliable measures on teacher-rated childhood hyperactivity, parent-rated adolescent symptoms of ADHD, and clinical diagnostic procedure. The outcome measure relying on register-based information in hospital-treated injuries is highly reliable, also in terms of severity. In terms of contributing factors, there is a suggestion that a high dose of stimulant medication for ADHD may decrease the risk for injuries (Marcus, Wan, Zhang, & Olfson, 2008). Our community sample is medication-naïve for ADHD, as stimulant treatment for ADHD was very rare in Finland at the time of data collection. Consequently, stimulant medication has no effect on our results.
Some limitations should be noted, however. First, childhood measure of hyperactivity may not tell only about ADHD. Although teachers are considered reliable informants on children’s behavioral problems, a 3-item measure of hyperactivity in the spring of children’s first school year may also be indicative of developmental issues. Similarly, the SWAN was completed by parents when their children were in the midst of adolescent turmoil (age 15), which may temporarily increase inattention and hyperactivity problems. Second, symptomatic information from teachers and parents at the ages of 8 and 15 would have strengthened our study, but this was not possible to obtain in our study design. However, the present study provided similar results for all cohort members as well as for a subpopulation assessed with extensive clinical procedure for ADHD. Thus, it is plausible that the found childhood hyperactivity symptoms and adolescent symptoms of inattention/hyperactivity were symptoms of the same entity. Nevertheless, further longitudinal research is needed with consistent approach assessing ADHD from childhood to adolescence. Therefore, our results can be considered as exploratory.
In sum, our results suggest that ADHD and its components of inattention and hyperactivity-impulsivity are associated with childhood unintentional hospital-treated injuries. Some types of injuries, such as intracranial injuries in childhood and fractures and intoxication in adolescence, are common among those with ADHD. This association should be noted in overall injury prevention and when guiding parents with a child with ADHD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Academy of Finland (grants to T. Hurtig, PhD, and Professor A. Taanila), the Emil Aaltonen Foundation, and Paulo Foundation (grants to T. Hurtig, PhD) are acknowledged for their support.