
Abstract
Models of help-seeking behavior for mental disorders depict four core stages: problem recognition, the decision to seek help, service selection, and service utilization (Andersen, 1995; Eiraldi, Mazzuca, Clarke, & Power, 2006). These four help-seeking stages are interrelated, and families generally transition through them in a linear fashion. This process can be interrupted at any stage and therefore many children do not receive adequate care (Power, Eiraldi, Clarke, Mazzuca, & Krain, 2005). A number of factors, occurring within and outside the individual, have been hypothesized to impact the transition through each help-seeking stage (Cauce et al., 2002; Eiraldi et al., 2006). Parental cognitions (e.g., knowledge, attitudes toward treatments) are one factor that may predict when (or if) families enroll in treatment, which types of treatments are considered, and ultimately whether the treatments are completed (Hoza, Johnston, Pillow, & Ascough, 2006). The present study examines the relationship of ADHD knowledge and misconceptions with perceptions of treatment acceptability for medication and dietary interventions.
Treatment Acceptability
Kazdin (1980) originally conceptualized treatment acceptability as a “judgment of a treatment by nonprofessionals, lay persons, clients, and other potential consumers of a treatment” (p. 259). Treatment acceptability can be influenced by a variety of factors including problem severity, type of treatment, side effects, efficacy, and costs (Reimers, Wacker, & Koeppl, 1987). Parental cognitions such as knowledge and beliefs about ADHD and its treatment may also play a role in the acceptability of a given treatment. Johnston, Seipp, Hommersen, Hoza, and Fine (2005) found that parents with more reasonable beliefs about ADHD and its treatment showed greater acceptance and utilization of both behavioral and medication treatments for ADHD. Those with false beliefs about ADHD were more likely to find alternative interventions (e.g., diet) as more acceptable (Johnston et al., 2005). Although some research has linked broader knowledge of ADHD to treatment acceptability (Bennett, Power, Rostain, & Carr, 1996; Ohan, Cormier, Hepp, Visser, & Strain, 2008), research on the link between knowledge and treatment acceptability has been inconsistent (Carter, 2007). It may be that knowledge or misconceptions of specific principles or concepts (e.g., whether stimulants are addictive), rather than the overall level of knowledge (i.e., number of correct answers), is a better predictor of treatment acceptability. It is reasonable to assume that not all misconceptions are equally important; having correct or incorrect knowledge of specific content may be more important than overall levels of knowledge when it comes to predicting perceptions of treatments. Specific misconceptions about dietary interventions, ADHD etiology, and medication treatment have been well documented in studies of parents and teachers (Akram, Thomson, Boyter, & McLarty, 2009; Bussing et al., 2012; dosReis et al., 2003; Sciutto, Terjesen, & Bender Frank, 2000). The present study examines how specific misconceptions and the strength with which they are held are related to the perceptions of interventions that are either “directly” (e.g., misconceptions about stimulants predict acceptability of stimulants) or “indirectly” (e.g., misconceptions about stimulants predict acceptability of alternatives like diet) related to the content of the misconception. For instance, a parent who believes that stimulant medication leads to later substance abuse is likely to find stimulant medications as less acceptable in the treatment of ADHD. However, there may also be a “collateral” effect. In other words, does that misconception also make alternatives like diet seem more acceptable?
Measuring ADHD Knowledge and Misconceptions
Many studies examining knowledge of ADHD have used dichotomous scoring (true/false or correct/incorrect) to estimate knowledge. Using this method, an incorrect answer on a true/false item may be the result of a strongly held misconception, a weakly held belief, or simply a consequence of guessing. Therefore, this method does not directly identify misconceptions and gives little information about the strength of people’s confidence in the accuracy of their knowledge. The strength of beliefs may be clinically important to the study of help seeking because strongly held, but incorrect, beliefs are harder to change and may adversely affect the interpretation of new information (Anderson, Watt, Noble, & Shanley, 2012; Dole & Sinatra, 1998; Taylor & Kowalski, 2004). Thus, a strong belief in inaccurate knowledge may serve as a barrier to seeking help or pursuing a specific form of treatment for ADHD. For example, parents who hold strong misconceptions about the use of stimulant medication for ADHD (e.g., that they lead to greater substance abuse) may be reluctant to consider this treatment option for their child or they may delay seeking help in the first place if medication is perceived to be the first-line intervention. Those parents, in turn, may find less established treatments more acceptable. Other parents may hold the same misconception but not as strongly. These parents may be more receptive to new information and may be open to changing their cognitions over time. Changes in parental cognitions may play an important role in the improvement and maintenance of progress over the course of treatment (Hoza et al., 2006). In this study, ADHD knowledge was measured using the Strength of Belief in ADHD Knowledge Scale (SBAKS), which has been designed to (a) distinguish guessing from misconceptions and (b) reflect the strength of participants’ belief in the accuracy of their knowledge.
Sources of Information and ADHD Knowledge
Relatively little is known about the sources that contribute to people’s knowledge of ADHD. Some studies have examined the types of sources that parents have used or prefer for information about ADHD (Bussing, Gary, Mills, & Wilson Garvan, 2007; Bussing et al., 2012). In general, parents of children with ADHD tend to seek information from a variety of sources, including healthcare professionals, school personnel, social networks, the Internet, and other media sources. While some studies have linked information sources to stigma experiences (dosReis, Barksdale, Sherman, Maloney, & Charach, 2010), it is less clear how the use of specific sources of information is related to misconceptions or perceptions of treatment alternatives. One particularly important source may be the Internet because many individuals use the Internet as a source of information about ADHD (Akram et al., 2009; Bussing et al., 2012). Although there are many credible, informative sites, the Internet may also be a source of misinformation about ADHD and other health-related conditions (Akram, Thomson, Boyter, & Morton, 2008; Kisely, Ong, & Takyar, 2003; Reavley & Jorm, 2011). This study will examine the relationships among information sources, ADHD knowledge/misconceptions, and treatment acceptability.
Method
Participants
In this study, 196 participants (21% male, 75% female, 4% other/no response) with an average age of 25.97 (SD = 10.52) years completed an online survey measuring ADHD knowledge and the acceptability of interventions for ADHD. Participants were recruited from two different sources. Seventy-two (37%) participants were college students from an introductory psychology class who participated for course credit. The remaining 63% (n = 124) accessed the study through an Internet site that posts online psychological experiments (http://psych.hanover.edu/research/exponnet.html). The majority (85%) of the sample self-identified as White/Caucasian, with the next largest racial group being Black/African American (4%). With regard to participants’ highest level of education, 27% of those who responded had a college degree (bachelor’s or above) and 17% had not completed any college work. Forty-seven (24%) of the participants were parents and 75 (38%) indicated that they worked regularly with children or adolescents. The majority (84%) of participants indicated that they knew someone who had been diagnosed with ADHD.
Measures and Procedure
Strength of Belief in ADHD Knowledge Scale
The SBAKS is a 9-item scale designed to measure participants’ knowledge and misconceptions of interventions for ADHD. Items were derived from the content of existing measures (Power, Hess, & Bennett, 1995; Sciutto et al., 2000) and modified based on feedback from five experts in the field of ADHD and qualitative feedback from a sample of 20 parents who were seeking treatment for their child with ADHD. Based on the assumption that not all misconceptions are held with equal conviction, the SBAKS is constructed to reflect the strength of confidence in a person’s knowledge or misconceptions rather than a sum of correct or incorrect responses. For each item, the participant indicates (a) whether he or she believes the statement is true or false and (b) his or her level of confidence in that response on a 4-point scale (0 = just a guess; 3 = I am certain). The SBAKS generates two total scores: strength of misconceptions and strength of knowledge. When measuring knowledge, correct true/false responses are coded as 1 and incorrect answers as 0. Alternatively, when measuring misconceptions, incorrect responses are coded as 1. For each item, the strength of belief was computed by multiplying the true/false score by the confidence level. A guess (i.e., a confidence level of 0) does not contribute to the knowledge or misconceptions score. For instance, an incorrect answer to a question for which the person was very confident would get a 3 toward the strength of misconceptions score and a 0 toward the strength of knowledge score. Scores on each of the items are summed to compute total scores ranging from 0 to 27. Descriptive statistics and reliability estimates for the SBAKS are presented in Table 1.
Descriptive Statistics for Measures of ADHD Knowledge, Misconceptions, and Treatment Acceptability.
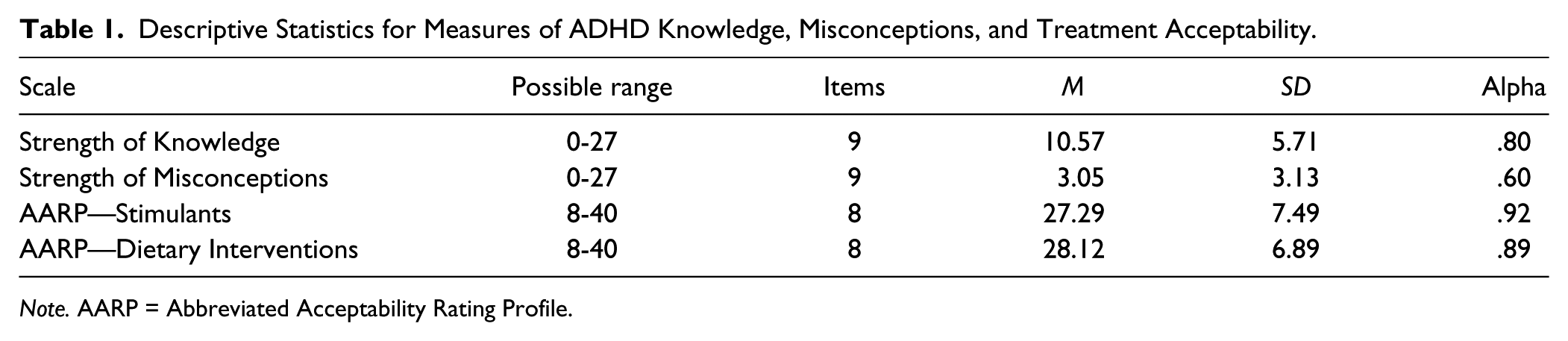
Note. AARP = Abbreviated Acceptability Rating Profile.
Treatment acceptability
The Abbreviated Acceptability Rating Profile (AARP; Tarnowski & Simonian, 1992) is designed to provide a brief measure of the acceptability of interventions. In this study, participants read a brief vignette designed to meet the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria for ADHD Combined Type (adapted from Pisecco, Huzinec, & Curtis, 2001). After reading the vignette, participants read a brief description of two interventions for ADHD: dietary restrictions and stimulant medications. These two interventions were chosen for analysis in this study because they have been well documented as areas of misconception and concern among parents of children with ADHD (Bussing et al., 2007, 2012). The order of the treatment descriptions was counterbalanced and randomly assigned to participants. Below are the descriptions of each treatment: Stimulant medications are commonly used to treat the symptoms of attention-deficit/hyperactivity disorder (ADHD) in children and adolescents. Ritalin is one of the most commonly used stimulants. These medications have been found to improve symptoms in the majority of children who have the condition by stimulating chemicals in the brain that help a person inhibit or restrain behaviors. Side effects may include loss of appetite, nervousness, tics or twitches, and problems sleeping. These side effects usually decrease after a few weeks on the medication, or the dosage can be lowered to offset them. Children should be closely monitored after they start medications to assess whether they are receiving the correct dose. Dietary restrictions are commonly used to treat the symptoms of attention-deficit/hyperactivity disorder (ADHD) in children and adolescents. Eliminating sugar is the most commonly used method. Parents have reported that this strategy leads to a reduction in hyperactive behavior. Although there are generally no physical side effects, children should be closely monitored after they start dieting to assess whether they are receiving adequate nutrition. Parents also report that these changes in diet are often time consuming. Changes should be made gradually in order to test whether the change helped or not.
After reading these descriptions, participants completed each of the eight AARP items using a 6-point scale. Scores on the eight items were summed to provide a total acceptability score for each intervention. The total scores could range from 8 to 48 with higher scores reflecting a greater level of acceptability for that intervention (see Table 1 for descriptive statistics)
Background characteristics
In addition to providing information about demographic characteristics, participants completed a brief survey about their background related to ADHD. Specifically, participants provided information about whether they knew someone personally (including self) who had been diagnosed with ADHD (yes or no) and the extent to which they believed ADHD is overdiagnosed (1 = strongly disagree; 5 = strongly agree). Participants also indicated any sources from which they had obtained information about ADHD and the source they considered to be their primary source of information. The possible sources were the Internet, professionals (e.g., medical/healthcare), social networks (e.g., family, friends, coworkers), media (e.g., TV, newspaper, radio), professional literature (e.g., research articles), and formal education (e.g., learned about it in a class).
Results
All statistical analyses were evaluated using an alpha level of .05.
Sample and Order Effects
I conducted a series of analyses to examine whether the college sample differed from the online sample on any of the primary measures. Fisher’s z transformations were used to compare the strength of the relationships between knowledge and acceptability measures across samples. The magnitude of these correlations did not differ significantly across samples (p > .05). However, the two samples did differ significantly on some background characteristics. The online sample (M = 30.43, SD = 11.08) was significantly older than the college sample (M = 18.45, SD = 0.65), t(120.38) = 11.80, p < .001, η2 = .54. Age, however, was not significantly related to any of the measures of knowledge/misconceptions or treatment acceptability (p > .05). Not surprisingly given the age difference, a higher percentage of participants from the online sample (48%) had worked regularly with children and adolescents than those in the college sample (24%), χ2(1, N = 191) = 11.13, p = .001. With regard to gender, the college sample had a higher proportion of male participants, χ2(1, N = 194) = 4.65, p = .031. However, males and females differed only on one of the primary measures; females had higher acceptability scores than males for dietary interventions, t(187) = 2.16, p = .032, η2 = .02. The two samples did not differ significantly with regard to personally knowing someone with ADHD, χ2(1, N = 192) = 0.14, p = .708, or in their belief that ADHD is overdiagnosed, t(178.17) = 0.49, p = .626, η2 = .001.
There were no significant effects of the order of the treatment descriptions (i.e., stimulants or diet first) on any measures or acceptability or belief that ADHD is overdiagnosed (p > .05). There were also no order effects for strength of knowledge scores, but there was a tendency for those who read dietary modifications first to report stronger misconceptions, t(183.63) = 2.26, p = .025, η2 = .03. However, the knowledge/misconceptions measure preceded the information on interventions. Therefore, this is not likely an effect of the order of presentation, but a random variation.
Relationship of Overall Knowledge and Misconceptions With Treatment Acceptability
In general, knowledge and misconceptions were stronger predictors of acceptability of medication than dietary interventions. Higher strength of knowledge about ADHD was associated with more positive levels of acceptability for medication, r(194) = .45, p < .001, but was not significantly related to views of dietary interventions (p > .05). Conversely, stronger misconceptions about ADHD were associated with more positive attitudes toward dietary interventions, r(194) = .23, p = .001, and more negative attitudes toward stimulant medications, r(194) = −.33, p < .001.
Relationship of Specific Misconceptions With Treatment Acceptability
Although the total strength of knowledge/misconceptions scores from the SBAKS were related to acceptability, it may be clinically useful to identify specific misconceptions that predict acceptability. Table 2 presents correlations of specific items on the SBAKS that differentially predicted the acceptability of medication compared with dietary interventions. Fisher’s z transformations were used to compare the magnitude of each item’s correlation with the acceptability of medication to its correlation with the acceptability of dietary interventions. In general, misconceptions about dietary interventions were significantly related to the treatment acceptability of dietary interventions but not to the acceptability of stimulant medications. For instance, participants who more strongly believed that sugar elimination diets or other restrictive diets (e.g., Feingold diet) were effective for most children with ADHD were more likely to find dietary interventions acceptable. However, these beliefs were not significantly related to their perceptions of the acceptability of stimulant medications. Likewise, more strongly held misconceptions about serious side effects or the effects of stimulants on later abuse were associated with lower treatment acceptability of medication but not consistently with more favorable views toward dietary interventions.
Differences in Correlations Between the Strength of Specific Misconceptions and Treatment Acceptability.

Source of Information, Knowledge, and Acceptability
Although Internet sources were used by most participants (58%), relatively few people cited it as a primary source of information about ADHD (14%). Overall, the most common primary sources of information for this sample about ADHD were social networks (30%) followed by medical/healthcare professionals (29%). A series of independent samples t tests were conducted to evaluate whether knowledge and acceptability measures differed for participants who used a given primary source (e.g., Internet) compared with those who relied on other primary sources (e.g., not the Internet). Participants whose primary source was the Internet or social networks were not significantly different in their acceptability toward stimulants or dietary interventions (p > .05). However, participants whose primary source was healthcare professionals had significantly higher acceptability scores (compared with those whose primary source was not a healthcare professional) for stimulants, t(186) = 3.25, p = .001, η2 = .05, but they did not differ for dietary interventions, t(186) = 0.29, p = .776, η2 = .001. With regard to ADHD knowledge, participants whose primary source was healthcare professionals had significantly higher strength of knowledge scores than those who used other primary sources, t(186) = 4.42, p < .001, η2 = .10. Participants whose primary source was social networks had significantly lower strength of knowledge scores, t(173.58) = 4.62, p < .001, η2 = .11, than those who used other sources. Participants whose primary source was the Internet were not significantly different in their knowledge (p >.05). Strength of misconception scores were not significantly related to the participants’ primary source of information about ADHD (p > .05).
Background Characteristics
Participants who knew someone with ADHD scored significantly higher on the strength of knowledge scale than participants who did not know anyone with ADHD, t(189) = 4.07, p < .001, η2 = .08, but did not differ on measures of acceptability or strength of misconceptions (p > .05). Surprisingly, those participants who worked regularly with children or adolescents scored significantly higher on the strength of misconceptions scale, t(188) = 2.17, p = .031, η2 = .02, but did not differ on measures of acceptability or strength of knowledge (p > .05). Participants who believed that ADHD was overdiagnosed found medication less acceptable, r(189) = −.26, p < .01. Perceptions of overdiagnosis were not related to the acceptability of dietary interventions, r(189) = −.003, p = .968.
Discussion
In this study, the overall strength of knowledge and strength of misconceptions were moderately related to perceptions of treatment acceptability. In general, more positive attitudes toward stimulants were associated with higher levels of knowledge and lower levels of misconceptions. However, examination of specific misconceptions suggests that the acceptability of a given treatment is likely related primarily to misconceptions about that treatment only. There was not a corollary relationship between misconceptions about stimulants and perceptions of alternative treatments like diet. For example, believing that stimulant medications were likely to lead to future substance abuse predicted a more negative response toward stimulants as a treatment for ADHD, but it did not appear to cast dietary interventions in a more positive light. This finding has implications for the service-selection stage of help-seeking models for ADHD (Eiraldi et al., 2006). Addressing misconceptions about dietary interventions, for example, may not be sufficient to have parents consider more empirically supported interventions. Prior research has found that these misconceptions are prominent among parents who are reluctant to consider medication use and that this reluctance may account for racial or ethnic disparities in help-seeking attitudes and behavior (Bussing et al., 2012).
The results of this study suggest that assessing and targeting specific misconceptions may be a desirable strategy to consider as clinicians integrate educational components into treatment for ADHD. How to address misconceptions is complicated. Research on psychoeducational approaches in clinical practice may provide little insight. Although there does appear to be generally positive results, psychoeducation is a poorly defined treatment component (Montoya, Colom, & Ferrin, 2011). What is called “psychoeducation” may vary considerably from intervention to intervention or study to study. There is little systematic evidence related to the specific strategies for psychoeducation. Further complicating the matter is the fact that some misconceptions may influence the stages of help seeking that come before the clinician has an opportunity to intervene. However, even after parents make the decision to seek help, little is known about how providers address misconceptions in the context of treatment. Simply providing information that a form of treatment has not been supported by research may not be sufficient. In this regard, clinicians can benefit from the educational psychology literature on addressing misconceptions. Simple didactic interventions or textbook style readings are unlikely to be effective. Refutational texts have been researched extensively in education and may provide a helpful framework to address misconceptions in clinical settings. Refutational texts directly identify a misconception and provide scientific evidence that disputes it (Guzzetti, 2000). These texts are believed to create cognitive conflict in the reader that facilitates conceptual change. Research on refutational texts in education settings suggests that they are particularly effective when followed by discussion with an informed guide (Guzzetti, 2000).
The results of the current study also suggest a need for a deeper investigation about the sources of information that contribute to knowledge and misconceptions of ADHD. Past studies have pointed to clients’ preference to gather information from the Internet (Bussing et al., 2012). Even though participants in the current study did not report that the Internet was their primary source of information, a majority did report using it as a source of information about ADHD. It also appears that people whose primary source of information is a healthcare professional have higher levels of ADHD knowledge. Strength of misconceptions, however, was not related to participants’ primary source of information. It is possible that firmly held misconceptions are reinforced or diffused across multiple sources or that these misconceptions, once formed, serve as a filter for new information regardless of the source. One issue not addressed in the current study is how people process information available from a given source, especially Internet-based resources. Future research should examine how people respond to conflicting information about a given treatment. For instance, a simple search of “ADHD and sugar” quickly turns up several reputable sites that dispute the sugar-hyperactivity myth. However, paid ads alongside the search provide links to dietary interventions for ADHD. More research is needed on how people respond to this kind of conflicting information and how it influences their perceptions of treatment options. As access to health information on the Internet becomes more abundant, it will become particularly important for providers and researchers to identify credible information resources that are accessible to parents.
Finally, the current study is limited in several ways. The present study used a nonclinical, analogue population that may be different from the population of parents seeking treatment for a child with ADHD. Gage and Wilson (2000) found that there were differences between potential and actual consumers; that parents of children with ADHD differed in acceptability ratings from parents of children without ADHD. However, in other areas of healthcare research, findings based on analogue populations have been reliable and valid predictors of key elements in the help-seeking process (e.g., perceptions of patient–provider interactions; Blanch-Hartigan, Hall, Krupat, & Irish, 2013; van Vliet et al., 2012). Analogue methodologies, such as the one used in this study, may provide unique and important information about decision-making processes (Huebner, 1991), and may suggest hypotheses to be tested with clinical populations. Because of the apparent link between misconceptions and perceptions of acceptability in the present study, future research may need to examine the efficacy of specific strategies for refuting misconceptions. These strategies are likely to be evaluated using experimental methodologies, which may be prohibitive with clinical populations for practical and ethical reasons. Consequently, the use of analogue methodologies can play an important role in understanding the help-seeking process.
In addition, the current study only examined two specific intervention options, sugar elimination diets and stimulant medications. It is not clear whether these results are generalizable to other ADHD interventions. Of particular importance is how people’s knowledge and misconceptions relate to their perceptions of school-based interventions. Bussing and colleagues (2007) found that parents’ knowledge and awareness of school-based interventions were particularly low. Finally, the information about treatment options presented in this study was limited in scope. It is not clear whether the pattern of results in this study will generalize to situations in which parents encounter more extensive information on each of the treatment options.
Footnotes
Acknowledgements
The author would like to thank Thomas J. Power for his feedback during the development of the ADHD knowledge scale and Florencia Allegretti, Evelina Eyzerovich, Melanie Franklin, and Eric Hamilton for their assistance in the early stages of setting up the survey materials.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.