
Abstract
In recent years, the diagnosis of ADHD and its subtypes has been much discussed. The Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) classifies ADHD into three subtypes: the predominantly inattentive subtype (ADHD-I), the hyperactive subtype (ADHD-H), and the combined subtype (ADHD-C). The latter includes people with high symptoms of both subtypes (ADHD-I and ADHD-H; APA, 2000).
The current controversy among researchers refers to the conceptualization of ADHD-I (Milich, Balentine, & Lynam, 2001; Barkley, 2001b). Some authors have found that children with ADHD-I may have some traits of hyperactivity (Carlson & Mann, 2002; Derefinko et al., 2008), but they did not fit the criteria to be a combined subtype. However, it is possible to find children with ADHD-I who do not have hyperactivity, but often show behaviors such as drowsiness, sluggishness, lack energy or low physical activity, daydreaming, high levels of internalizing behaviors, decreased alert and orientation (Barkley, 2001b; Carlson & Mann, 2002; Derefinko et al., 2008; Desman, Petermann, & Hampel, 2008; Garner, Marceaux, Mrug, Patterson, & Hodgens, 2010; Harrington & Waldman, 2010; McBurnett, Pfiffner, & Frick, 2001). This set of behaviors forms a new construct called Sluggish Cognitive Tempo (SCT; Barkley, 2001b; Carlson & Mann, 2002; Garner et al., 2010; Hartman, Willcutt, Rhee, & Pennington, 2004; McBurnett et al., 2001).
Currently, researchers are discussing the conceptualization of this construct. It is not yet possible to define whether SCT symptoms occur only in the ADHD-I, or whether the ADHD-I could be divided into two groups: a group with SCT and other one without SCT but with a low level of hyperactivity. Another alternative would be that the SCT were considered as a new diagnostic group distinct and separate from ADHD (Derefinko et al., 2008; Garner et al., 2010; Hartman et al., 2004; McBurnett et al., 2001; Todd, Rasmussen, Wood, Levy, & Hay, 2004). Some authors as Barkley (2001a) and Garner et al. (2010) ensure that the SCT is an attention disorder that does not correspond to the subtypes of ADHD. On the other hand, Milich et al. (2001) and McBurnett et al. (2001) state that SCT symptoms are part of the inattentive subtype. In the same rationale, Carlson and Mann (2002) suggest that it is important to study SCT in children with ADHD-I because it improves the validity of this subtype through the development of diagnostic criteria. They propose further studies of ADHD-I with SCT to clarify the definition of this category. Other studies suggest that SCT symptoms do not define a separate type of clinically relevant ADHD-I (Harrington & Waldman, 2010; Ludwig, Matte, Katz, & Rohde, 2009; Todd et al., 2004), as SCT is associated not only with ADHD-I, but also with a whole dimension of inattentiveness, as it is also associated with ADHD-C (Hartman et al., 2004; Hurtig et al., 2007; Todd et al., 2004). In addition, some authors (Harrington & Waldman, 2010; Mayes, Calhoun, Chase, Mink, & Stagg, 2009; Milich et al., 2001; Penny, Waschbusch, Klein, Corkum, & Eskes, 2009) mention that it is not possible to ensure that the SCT only occurs with ADHD-I, but that these are traits or behavioral symptoms associated with various pathologies of internalizing nature.
Thus, to better understand the nosology of the SCT, the above-mentioned studies indicate the need for clearly defining what children we are referring to when we use this diagnostic category. Considering that the SCT is strongly associated with ADHD-I, studying neuropsychological functioning is of great importance, as recent studies show that ADHD is associated with deficits in executive function (EF; Barkley, 2001a; Sergeant, Geurts, & Oosterlaan, 2002; Sonuga-Barke, Dalen, Daley, & Remington, 2002). This function allows the individual to lead and guide the behavior to reach a goal, and regulate it against possible changes in his or her immediate context (Luria, 1966, in Goldberg, 2002). This function also regulates the cognitive, emotional, and social behavior of individuals (Anderson, 2002; Barkley, 2000; Goldberg, 2002; Senn, Espy, & Kaufmann, 2004). Inhibition, planning and organization of a task, working memory, emotional control, monitoring, flexibility to switch strategies and initiative are some of the areas that compose the EF. These are the areas in which children with ADHD are affected (Barkley, 2001a; Brocki, Eninger, Thorell, & Bohlin, 2010; Holmes et al., 2010; Re, De Franchis, & Cornoldi, 2010; Willcutt, Pennington, Olson, Chhabildas, & Hulslander, 2005). Studies that have been interested in distinguishing the neuropsychological profile in the SCT are few. Barkley (2001b), Derefinko et al. (2008), and Wåhlstedt and Bohlin (2010)) claim that the SCT is not accompanied by deficits in inhibition. This statement has great significance if we consider that children with ADHD-I in most studies have shown deficits in this area (Brocki et al., 2010; Mullane, Corkum, Klein, McLaughlin, & Lawrence, 2011).
On the other hand, Capdevila-Brophy, Artigas-Pallarés, and Obiols-Llandrich (2006), in a case study, found deficits in children’s metacognition. The latter represents the ability to initiate, plan, organize, and maintain the solution of a problem in working memory and monitoring one’s behavior. With regard to regulation and emotional control, these authors found that they were present in a normal way. On their part, Skirbekk, Hansen, Oerbeck, and Kristensen (2011) and Wåhlstedt and Bohlin (2010) did not find deficits in working memory.
Studies comparing the subtypes of ADHD with the SCT also have varied results. Hinshaw, Carte, Sami, Treuting, and Zupan (2002) found no differences in executive functioning among girls with ADHD-I-SCT and girls with ADHD-I or ADHD-C. In contrast, others argue that the combination of ADHD-I and SCT involves neuropsychological problems different from those that occur with ADHD-I only (Carlson & Mann, 2002; Milich et al., 2001).
Based on the literature review, our research aims to study the relationship between SCT symptoms and ADHD-I symptomatology with executive functioning. The objectives are to see whether the presence of symptoms of SCT impact directly on EF; to observe whether the presence of symptoms of ADHD-I has a greater weight on the EF deficits than the symptoms of SCT; and finally, to determine whether there are EF deficits associated only with ADHD-I and not with SCT symptoms. As a hypothesis, we hope to find that the symptoms of ADHD-I have more weight on the EF deficits than the SCT symptoms, not implying the presence of these executive dysfunction on their own.
Method
Participants
This study involved 76 participants 6 to 17 years of age. They were being treated for ADHD in a Mental Health Centre for Children and Youth of the Vic’s Health Corporation (Osona County, Barcelona, Spain). 84.2% were male and 15.8% female, all with average IQ and middle socioeconomic status (see Table 1).
Sociodemographic Data.
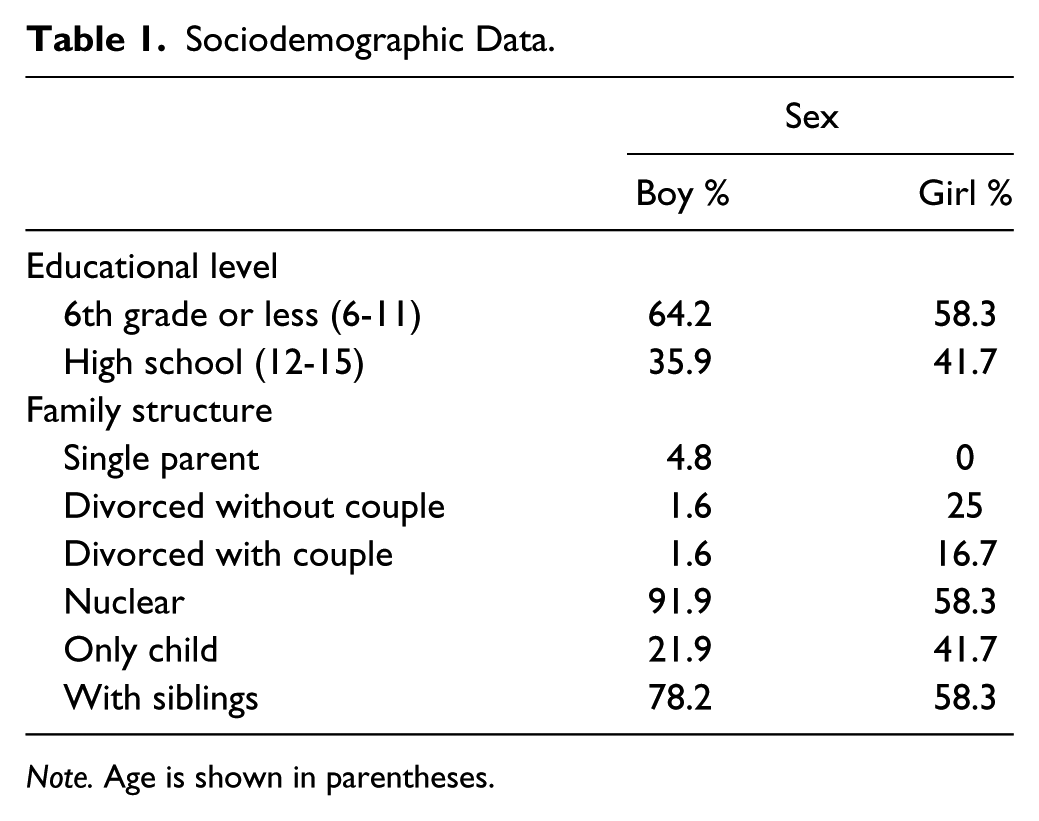
Note. Age is shown in parentheses.
All new cases over 6 years of age presented in the course of 2 years were invited to participate in the study. We interviewed the children or adolescents and their parents.
Instruments
ADHD symptomatology
We used the diagnostic interview “Schedule for Affective Disorders and Schizophrenia for School-Age Children Present and Lifetime version” (K-SADS-PL; Kaufman et al., 1997). This is a semi-structured interview to collect information from children or adolescents and their parents. It includes diagnoses according to DSM-IV-TR. It consists of 82 symptoms related to 20 diagnostic areas and 5 diagnostic supplements (emotional disorders, psychotic disorders, anxiety disorders, disruptive behavior disorders, and a final one consisting of substance abuse, tic disorders, eating disorders, and elimination disorders). They are coded in absent, probable, or present. The interview was conducted separately for parents and children or adolescents. The following variables were created: ADHD-I, ADHD-H, making a sum of the severity of symptoms.
Executive function assessment
We used the Behavior Rating Inventory of Executive Function (BRIEF; Gioia, Isquith, Guy, & Kenworthy, 2000, translated and adapted by Capdevila-Brophy et al., 2006). It consists of a self-report for parents and another for teachers. In this study, we used only the parent version. This questionnaire assesses executive function in children and adolescents between 5 and 18 years of age. The BRIEF contains 86 items, rated on a three-point scale, where 1 = Never, 2 = Sometimes, 3 = Often. The items form eight clinical scales (and two validity scales), which in turn form three broader indexes: conduct regulation, metacognition, and a score of global executive composite. The eight scales correspond to: Inhibition, Shift, Emotional Control, Initiate, Working Memory, Plan/Organize, Organization of Materials, and Monitor. High scores on any scale indicate poor executive functioning. They can be calculated from the sum of the items or the mean of the items. Like other authors, we use the second option because it keeps the same metric at all scales, regardless of the number of items they have (Bonillo, Araujo Jiménez, Jané Ballabriga, Capdevila, & Riera, 2011).
In this study, we only use the BRIEF to assess the EF as, based on the study by Barkley and Fischer (2011), self-reports of EF are capable of measuring deficits in daily activities and occupational functioning of children and adolescents. These authors state that these problems are not evident in laboratory tests, as they “have little ecological validity” (p. 155; e.g., Digit Span from the Wechsler Adult Intelligence Scale, 3rd ed. [Wechsler, 1997] or the Tower of London Test [Shallice & Burgess, 1991], both in Barkley & Fischer, 2011).
Symptoms of sluggish cognitive tempo
Parents and adolescents (older than 13 years) answered the Child Behavior Checklist (CBCL, Achenbach, 1991). It is a self-report that assesses behavioral problems and social skills. It consists of 113 items based on a three-point scale, where 0 = Not true, 1 = sometimes true, and 2 = true, very often or quite often. For the SCT construct, we used four items associated according to the literature (Carlson & Mann, 2002; Garner et al., 2010; Ludwig et al., 2009): “He is confused and looks like he’s in the clouds”; “he daydreams, he is lost in thought,”; “he stares into the void”; and “he is very inactive, slow, or lacking energy.” Higher values indicate problems in the symptoms of SCT. As the study of Garner et al. (2010), the item “very active” was excluded from the analysis as it did not show a strong correlation with other items of SCT. The value of Cronbach’s alpha was .584.
We used the family data questionnaire (Domènech-Llaberia, Canals, Viñas, & Jané, 1998) to collect sociodemographic data.
Procedure
To carry out the evaluations, we asked permission from the Ethics Committee of the Mental Health Services for Children and Youth of the Vic Health Consortium. We asked parents and children and adolescents to sign an informed consent to participate in the study. We asked for contact details to make appointments for interviews. Interviews were conducted with parents and children and adolescents in the facilities of the Hospital.
Data Analysis
We used the SPSS software Version 20.0 for Windows, with which we analyzed the statistical relation between the symptoms of ADHD-I, ADHD-H and SCT (independent variables), and the BRIEF scales (Inhibit, Shift, Emotional Control, Initiate, Working Memory, Plan/Organize, Organization of Materials, and Monitor; dependent variables), using the statistical general model of multiple linear regressions. We conducted two hierarchical linear regression models: one that examined the independent relationship between SCT and each of the scales of the BRIEF (to see whether the presence of symptoms of SCT impact directly on EF), and then a second model that added the symptomatology of ADHD-I and ADHD-H. This strategy aims to observe whether the presence of symptoms of ADHD-I influences the relationship of SCT and the EF. It also helps to determine whether there are EF deficits associated only with ADHD-I and not with SCT symptoms.
We used standardized coefficients (or beta—β) of the multiple linear regressions to determine the relative importance of the symptomatology studied (in standard deviation units) on each EF. The adjustment variables used were sex and age (full year). We controlled their effect by incorporating them into the calculation of the multiple regressions regardless of statistical significance (Kleinbaum, 1982).
In addition, we observed the correlations between ADHD-I, ADHD-H, SCT, and the BRIEF scales to confirm the association between these symptomatologies.
For beta coefficients and Pearson correlations, we considered a significance <.10 in some cases, as mentioned by other authors (Lopez et al., 2008). Both were seen as effect size measures, because they are standardized and do not depend on the measurement unit (Kelley, 2007).
The “Results” section shows the confidence intervals of associations that have a statistically significant result.
Results
Results obtained in Model 1 of the linear regressions will be discussed in the first paragraph: This model includes SCT, sex, and age variables. Starting from the second paragraph, Model 2 will be explained: including SCT, ADHD-I, ADHD-H, sex, and age variables. In both cases, associations that were statistically significant and 95% confidence interval (CI) will be discussed as a priority.
In the first model of the linear regressions, the results indicate that the SCT symptoms explain the high scores on emotional control rates β = .31, 95% CI [0.08, 0.54], plan/organize β = .39, 95% CI [0.08, 0.67], working memory β = .34, 95% CI [0.13, 0.55], organize material β = .26, 95% CI [0.03, 0.49], and monitor β = .24, 95% CI [0.01, 0.48] (see Table 2). Deficits in inhibition, initiative, and flexibility (Shift index) in children or adolescents are not significantly associated with SCT.
Association of the Symptomatology of SCT, ADHD-I, and ADHD-H Versus EF. Standardized Regression Coefficients.
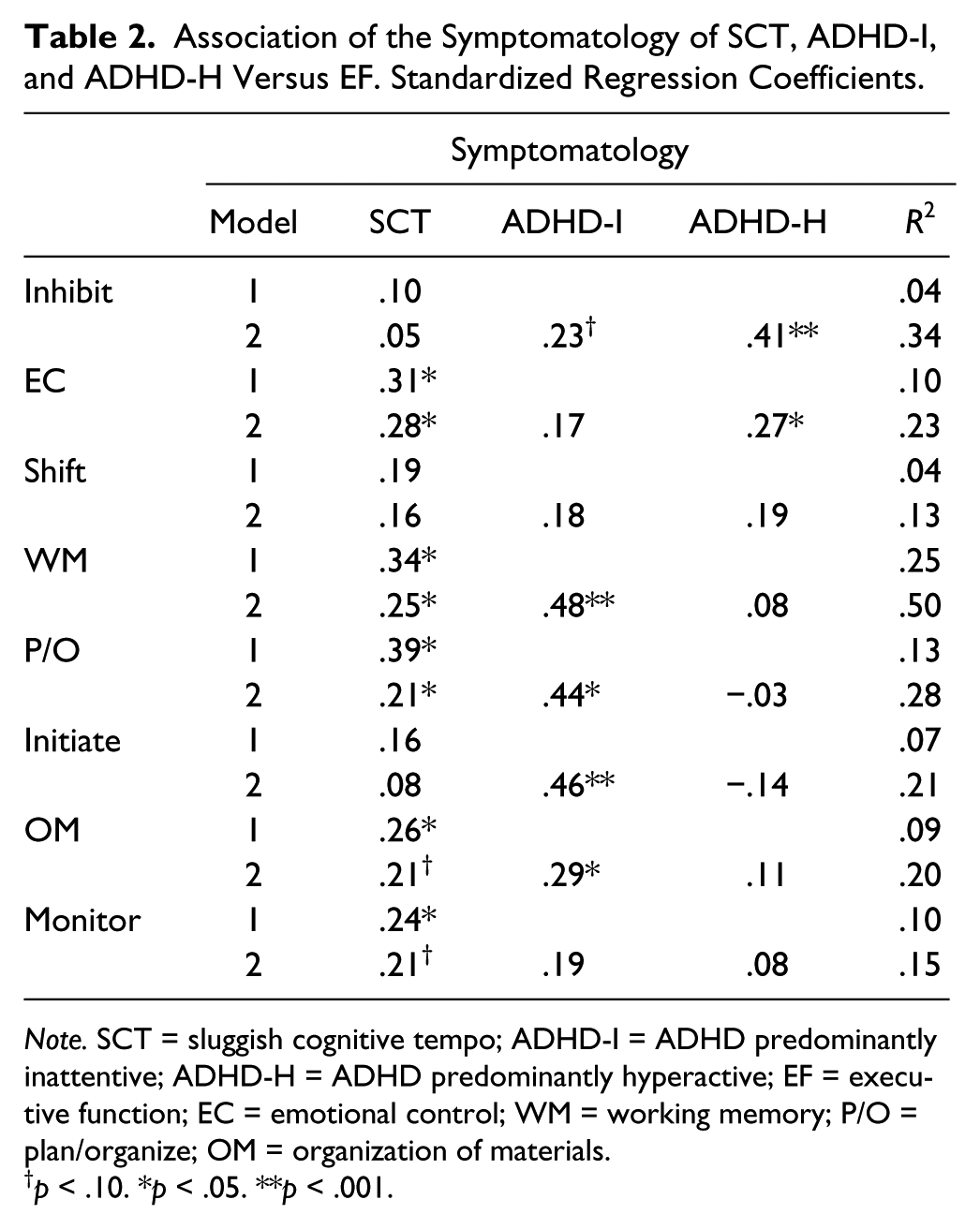
Note. SCT = sluggish cognitive tempo; ADHD-I = ADHD predominantly inattentive; ADHD-H = ADHD predominantly hyperactive; EF = executive function; EC = emotional control; WM = working memory; P/O = plan/organize; OM = organization of materials.
p < .10. *p < .05. **p < .001.
In the second model, we added as explanatory variables the symptomatology of ADHD, as well as SCT. It turned out that the presence of inattention and SCT explains the high rates of plan/organize (β = .21, 95% CI [−0.003, 0.42] for SCT; β = .44, 95% CI [0.18, 0.70] for ADHD-I), working memory (β = .25, 95% CI [0.07, 0.43] for SCT; β = .48, 95% CI [0.26, 0.70] for ADHD-I), and organization of material (β = .29, 95% CI [0.28, 0.137] for ADHD-I). The ADHD-I alone explains the presence of deficits in the initiative, β = .46, 95% CI [0.19, 0.74]. SCT symptoms do not explain the deficits in this index, so we decided to conduct a more detailed analysis of the BRIEF items corresponding to this scale. The literature shows that most children with SCT have difficulty initiating tasks (Capdevila-Brophy et al., 2006). Then, we separated the items into two groups: (a) those items measuring willingness to begin a task (“Is not a self-starter,” “Needs to be told to begin a task even when willing,” “Has trouble getting started on homework or chores,” and “Does not take initiative”) and (b) the items measuring the independent production of ideas (“Has trouble coming up with ideas for what to do in play or free time,” “Has trouble organizing activities with friends,” “complains there is nothing to do,” and “Lies around the house a lot”). However, the results indicated that the SCT symptoms do not explain the deficits of initiate and generate ideas.
In addition, high scores on the index of inhibition are explained by the presence of symptoms of ADHD-H, β = .41, 95% CI [0.16, 0.65], and ADHD-I, β = .23, 95% CI [−0.02, 0.48], and the rate of emotional control, which is explained in 23.4% by the symptomatology of ADHD-H, β = .27, 95% CI [0.01, 0.53], and the symptoms of SCT, β = .28, 95% CI [0.06, 0.50]. On the other hand, the symptoms of SCT also significantly explain slightly deficits in monitoring in the second linear regression model, β = .21. We found no significant relationship between Shift deficits and the studied symptomatology.
We observed significant correlations between SCT symptoms and the symptomatology of ADHD-I (r = .228, p = .048), and some BRIEF scales (emotional control, working memory, plan/organize, organization of material, and monitor; see Table 3).
Correlations Between SCT, Symptomatology of ADHD, and the BRIEF Scales.
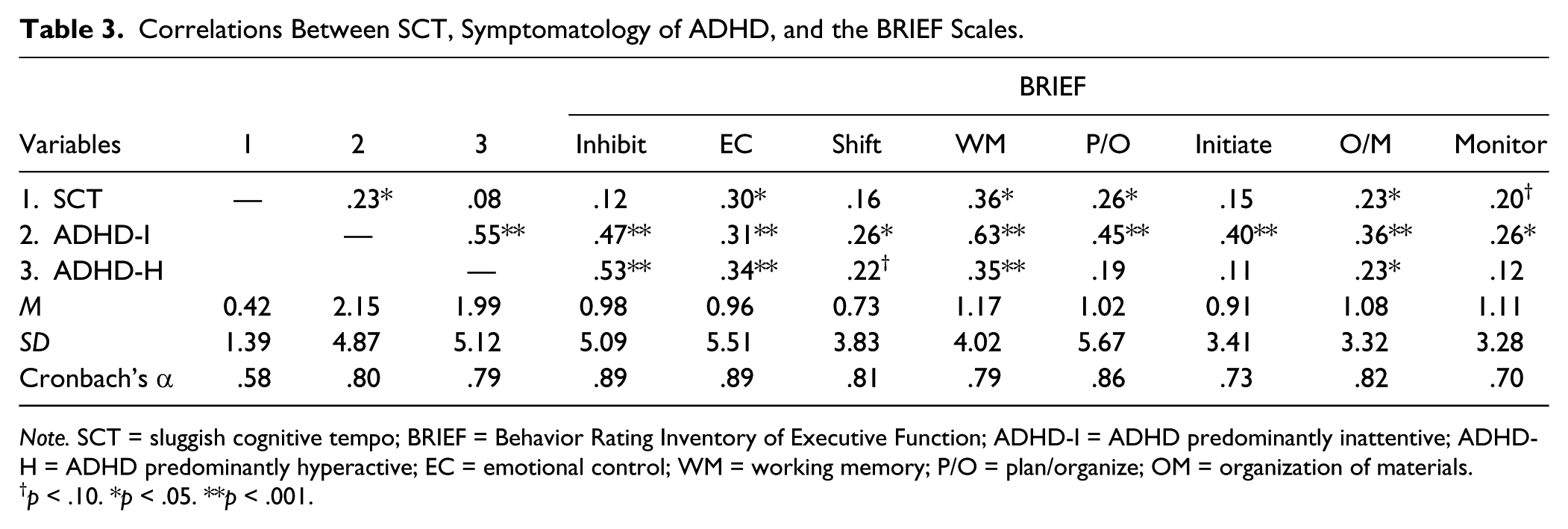
Note. SCT = sluggish cognitive tempo; BRIEF = Behavior Rating Inventory of Executive Function; ADHD-I = ADHD predominantly inattentive; ADHD-H = ADHD predominantly hyperactive; EC = emotional control; WM = working memory; P/O = plan/organize; OM = organization of materials.
p < .10. *p < .05. **p < .001.
Discussion
One of the objectives of this study was to observe whether the presence of symptoms of SCT directly impacts on the EF. In the analyzed linear regression models, we observed that the weight exerted by the symptoms of SCT on some EF deficits remain from one model to another. When we incorporated the ADHD-I into the analysis, we found that the presence of these symptoms involves more executive deficits in children than the SCT symptoms. However, it is interesting that these symptoms do not dispose of or remove from the model the weight of the SCT on some EF deficits. This may be related to the results obtained by Hurtig et al. (2007), which state that children with SCT and ADHD-I have the same problems organizing tasks, following directions, and avoiding tasks. Based on this, we would reject the hypothesis that SCT symptoms are not associated with executive deficits, and that these dysfunctions are explained only by the presence of symptoms of ADHD-I. In this study, we found that SCT symptoms and symptoms of ADHD-I independently promote executive deficits in children/adolescents. However, even if there is statistically significant association between these variables, it must be considered that the effect between some of them is still small, for example, in the association between SCT and emotional control rates, only 9.9% of the variance is explained.
As for problem solving and goal achievement, the objective of the EF is that the individual solve new and complex situations (cognitive or social-emotional) in an effective and acceptable way for him and society (Lezak, 1995). To do this, it takes into account the immediate consequences and results at mid and long term of the actions taken (Barkley, 2001a). It regulates the behavior and emotions so that the individual can be optimally adapted to his or her context (Anderson, 2002; Goldberg, 2002). It is a process that goes from presenting a problem to the solution of it (Anderson, 2002; Senn et al., 2004). Figure 1 shows the process of EF when the symptoms of SCT, ADHD-I, and ADHD-H occur. It is possible to note that the EF deficits associated with symptoms of ADHD-I are shown when children are not able to inhibit their own behaviors (Brocki et al., 2010; Mullane et al., 2011). Barkley (1997) states that problems in the inhibition of behavior can be generators of EF problems, such as working memory and emotional control. In addition, the current literature indicates that ADHD-I is associated with deficits in all areas of EF (Brocki et al., 2010; Holmes et al., 2010; Willcutt et al., 2005). In our study, children with ADHD-I showed deficits in most areas of the EF, but not in emotional control and flexibility to pursue new strategies. However, the analysis of correlations indicates that these two indices are correlated with ADHD-I. Therefore, in a school setting or in a family context, the inattention prevents the child with ADHD-I attend to what is asked. Even if he or she managed to address the problem that was posed, he or she would not be able to use his or her working memory in search of new solution strategies, due to deficits in this area, so he or she would not be able to plan and organize the required activities. Disinhibition would prevent the child to focus on the information stored, which he or she could use. Then, lack of motivation to start a task, lack of initiative, and difficulty in generating ideas would not let him or her to reach the goal. In addition to all this, children with inattention are disorganized (APA, 2000); this particular trait will cause many problems when carrying out an activity.
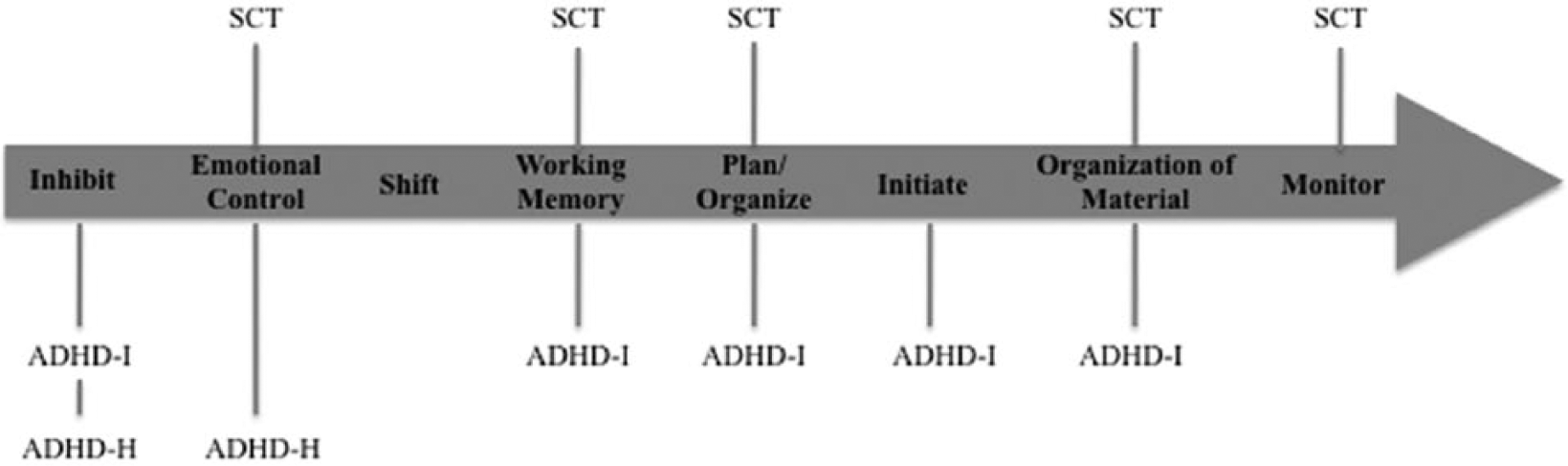
Problem solving and goal achievement.
If we compare the problem solving in ADHD-I and SCT, in the same figure we can see that deficits in inhibition and initiative are unique to inattention. However, the ability to inhibit behaviors of children with SCT occurs normally. This has also been found in other studies (Barkley, 2001b; Derefinko et al., 2008; Wåhlstedt & Bohlin, 2010). Perhaps the main difference between these two symptomatologies is precisely the absence of behavioral disinhibition in SCT symptoms. However, the child with SCT will inhibit his or her own behavior and that of others to reach the goal, but this does not guarantee that he or she reaches it optimally. This requires that the rest of EF occur efficiently. Yet, to our knowledge, there are few studies that analyze the association of SCT symptoms and all the areas of EF in detail. As shown in Figure 1, the problem-solving process does not occur normally in these children (as in children with symptomatology of ADHD-I). These are children who fail to achieve their goals properly. In the figure, we note that while they can inhibit their own behavior and/or external stimuli, they are unable to control their emotions. This lack of control accompanied by confusion (which is proper to the symptoms of SCT) causes them not to seek new solutions or strategies when a new problem arises. From here on, deficits in working memory and the inability to plan and organize prevent them to initiate their tasks properly (Capdevila-Brophy et al., 2006).
The results of our research are different from those found by Skirbekk et al. (2011) and Wåhlstedt and Bohlin (2010), who found no deficits in working memory in children with SCT. Furthermore, we disagree with Capdevila-Brophy et al. (2006) in that these children have trouble initiating a task. This can be explained considering that in the rest of the reviewed literature there is no mention of a lack of initiative to carry out tasks or to generate ideas, but rather a slower response time and an error-prone information-processing compared with other children (Barkley, 2001b). Once the child begins his or her task, all the mentioned executive deficits will be present as well as the lack of monitoring of activities. Thus, the child with symptoms of SCT will not achieve his or her objectives optimally. The slowness of the child or his or her tendency to daydreaming does not imply that the child does not initiate or carry out his or her tasks. What is interesting is how and the quality with which he or she carries them out, and the EF is responsible for this (Goldberg, 2002). These problems not only occur in school or family settings but are also present in social functioning, that is, in interpersonal relationships of these children/adolescents. The particular characteristics of SCT coupled with the presence of EF deficits prevent children to follow the same pace as their peers. They are quiet, shy, and inactive children (Barkley, 2001b). These characteristics may cause isolation or being ostracized by the rest. Within the family, parents may confuse these characteristics with behavioral problems. Parents can take the slowness with which they perform the activities as a breach of orders or rules.
On the other hand, we found that children with ADHD-H symptoms were only affected in inhibition and emotional control. These deficits can be explained by impulsivity, which is typical in these children/adolescents. Although no deficiencies were found in the rest of EF, we found that there is a high correlation with problems in flexibility, working memory, and organization of materials. We believe that the problems presented in the inhibition and emotional control prevent children with these symptoms to achieve their objectives effectively and efficiently (Barkley, 1997).
Thus, these results suggest that deficits in EF are given differently in different subtypes of ADHD, as mentioned by other authors (Brocki et al., 2010). In addition, the SCT symptoms were not correlated with hyperactivity (Carlson & Mann, 2002), so that deficits in the EF are given differently in these two clinical categories. However, in our study we could not observe the effect of hyperactivity on inattention as a unique category. Further research is needed to conduct structural equation modeling to analyze, separately, the direct and indirect effect of hyperactivity on inattention, and their respective associations with the EF.
Based on the results above, in this study we conclude that deficits in EF are associated with symptomatology of ADHD-I and symptoms of SCT. We consider that if these two symptomatologies occur together, this will involve greater cognitive impairment in children. Therefore, the study of EF is of great interest to obtain a better understanding of the characteristics of children that present the symptomatologies we studied. It is necessary to know this functioning to help children with academic, family, and social difficulties. In addition, we provide information to teacher and parents the way in which these symptomatologies are accompanied by cognitive deficits. Carlson and Mann (2002) suggest that more studies should be conducted on ADHD-I and SCT to define these clinical categories. Our results may facilitate the study of this new construct (SCT) in future research. However, a limitation of this study is the small sample size. We believe it is necessary to carry out further research with a larger number of clinical samples to study the EF deficits in children with ADHD-I and SCT, and with different informants. We also propose to study SCT symptoms in other diagnostic groups (depression, anxiety, autism), besides ADHD, for a better conceptual consolidation. We believe it is important to conduct studies to assess in detail the different areas of the EF, with ecological instruments (self-reports) and neuropsychological tests.
It is noteworthy that the K-SADS-PL interview was applied to children and parents. However, the results were based on information obtained from parents, as children/adolescents did not report about significant deficits in EF. This can be explained because these children/adolescents suffered symptomatologies that make it difficult to give correct information (Winsler & Wallace, 2002).
Footnotes
Acknowledgements
We appreciate the cooperation of Consorci Hospitalari de Vic (Health Corporation of Vic), Spain.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.