
Abstract
Hyperactivity is a key symptom for ADHD subtype classification, and is a primary reason for clinical referral due to the often disruptive nature of hyperactive behaviors (Sayal, Taylor, Beecham, & Byrne, 2002). Furthermore, the presence of hyperactive/impulsive symptoms is associated with the most severe impairment (Gaub & Carlson, 1997; Hinshaw, 2002) and is predictive of criminal activity in adulthood (Babinski, Hartsough, & Lambert, 1999). While some findings suggest that symptoms of hyperactivity remediate during adulthood (Biederman, Mick, & Faraone, 2000; Faraone, Biederman, & Mick, 2006), opposing findings suggest that adults diagnosed with ADHD in childhood continue to exhibit increased motor movement relative to same-aged peers, regardless of whether they continue to meet diagnostic criteria for ADHD (Halperin, Trampush, Miller, Marks, & Newcorn, 2008).
The functional working memory (WM) model of ADHD (Rapport, Chung, Shore, & Isaacs, 2001) hypothesizes that excessive motor activity acts as a compensatory mechanism that improves WM performance to meet the increasing environmental demands on central executive (CE) functioning (Rapport et al., 2009). WM involves the temporary storage and active manipulation of internal information and comprises a domain-general CE and two subservient subsystems—the phonological loop (PH; associated with storage and rehearsal of verbal information) and the visuospatial sketchpad (VS; associated with storage and rehearsal of visual and spatial information; Baddeley, 2007). WM deficits, particularly in the domain-general CE, are hypothesized to serve as a core feature that underlies characteristics of the ADHD phenotype (Rapport et al., 2008). Specifically, the WM model posits that biological influences (e.g., genetics, prenatal factors) contribute to alterations of neurobiological systems (e.g., dopamine dysregulation, cortical underarousal) that result in the observed deficits in WM processes. Increased motor activity is believed to compensate for deficient neurobiological systems by increasing cortical arousal as demands on the WM system increase.
Efforts to examine Rapport et al.’s (2001) model and explicate ADHD-related activity have been predominantly confined to studies of children. For example, Rapport and colleagues (2009) identified a functional relationship between motor activity and WM, such that increased ADHD-related motor activity was functionally related to increased demands on the WM system, particularly the CE. A more recent study found that motor activity in children with ADHD disproportionately increased relative to typically developing children during tasks that placed greater demands on CE-mediated attentional processes, rather than inhibitory processes (Alderson, Rapport, Kasper, Sarver, & Kofler, 2012). A comprehensive model of ADHD, however, must adequately account for ontological variation in the ADHD phenotype and relate changes to potential underlying neurocognitive deficits (i.e., WM) across the life span. That is, examination of the association between WM and hyperactivity in adults with ADHD is particularly important because the presence of hyperactive symptoms appears to decrease in adulthood (Biederman et al., 2000; Faraone et al., 2006) while WM deficits persist (Alderson, Hudec, Patros, & Kasper, 2013; Alderson, Kasper, Hudec, & Patros, 2013; Schweitzer, Hanford, & Medoff, 2006).
Only one study to date has investigated the relationship between WM and objectively measured ADHD-related motor activity in adults. Lis and colleagues (2010) examined motor activity during an n-back WM task in adults with ADHD and healthy controls (HCs) and demonstrated that impaired task performance was significantly associated with an increase in objectively measured activity level for adults with ADHD, but not for HC adults. The authors’ conclusion that increased motor activity is associated with cognitive impairments in adults with ADHD may be premature, however, and should be tempered given several limitations. For example, Lis and colleagues measured motor activity by assessing displacement from a center point at regular intervals with an infrared motion analysis detector attached to participants’ heads. This assessment of motor activity may underestimate activity by discounting movements limited to extremities (i.e., not necessarily associated with head movement; Teicher, Ito, Glod, & Barber, 1996). In addition, the VS n-back task used by Lis and colleagues does not allow for examination of PH WM processes or cross-modality (e.g., PH and VS) comparisons. This is important as recent meta-analytic (Alderson, Kasper, et al., 2013) and experimental (Alderson, Hudec, et al., 2013) findings suggest that adults with ADHD, relative to HC adults, exhibit greater deficits associated with the PH system compared with the VS system. Even more, the exclusive use of a 1-back task does not allow for examination of performance differences across varying WM loads, and consequently precludes conclusions about potential between-group differences in storage/rehearsal capacity (e.g., administering 1-, 2-, and 3-back loads). Lis and colleagues also did not examine the contribution of specific component processes (e.g., storage/rehearsal and CE) that may be differentially associated with activity changes, as suggested by previous findings in children with ADHD (Alderson et al., 2012; Rapport et al., 2009). Finally, Lis and colleagues (2010) did not include a control condition, which limits conclusions regarding the nature of hyperactivity in ADHD as persistent across all conditions (regardless of WM demands) or dependent on situational demands (related to WM demands).
The current study is the first to utilize actigraphy to examine the relationship between activity level and PH and VS WM demands. Furthermore, the current study is the first to statistically isolate and examine the independent contributions of the domain-general CE and PH/VS storage/rehearsal processes to ADHD-related motor activity in adults. Consistent with the WM model of ADHD (Rapport et al., 2001), young adults in both groups were expected to exhibit higher levels of activity during WM tasks, relative to control conditions, and participants with ADHD were expected to exhibit disproportionately greater activity during WM conditions. Furthermore, the activity level was expected to be higher for all participants during tasks that place demands on the PH rather than the VS system. This prediction was based on previous findings that suggest larger deficits are observed in the PH system, compared with the VS system, in adults with ADHD (Alderson, Hudec, et al., 2013; Alderson, Kasper, et al., 2013). Finally, based on findings in children with ADHD (Rapport et al., 2009), the CE was predicted to provide the greatest contribution to the activity level, while the PH and VS storage/rehearsal subsystems were not expected to contribute to activity level in either group after controlling for the CE.
Method
Participants
The sample consisted of 35 undergraduate students between the ages of 18 and 24 years who completed the study to fulfill a research requirement for a university course. All participants gave their informed consent to participate in the study, and the university’s Institutional Review Board approved the study prior to the onset of data collection. Twenty (10 male) participants comprised the ADHD group and had an average age of 19.57 (SD = 1.91) years. The HC group included 15 (9 male) participants with an average age of 19.44 (SD = 1.09) years. The sample comprised 85.7% Caucasian, 5.7% Native American, 2.9% African American, 2.9% Hispanic, and 2.9% biracial participants. All self-report and collateral behavior rating scale scores were significantly higher for the ADHD group relative to the HC group (see Table 1). A Pearson chi-square indicated no between-group differences in gender, χ2(1) = .345, p = .557, or racial composition, χ2(4) = 4.92, p = .296. Independent samples t tests indicated no group differences in age, t(33) = .575, p = .569, intellectual functioning, t(33) = .090, p = .929, or socioeconomic status, t(32) = .160, p = .874; therefore, these variables were not included as covariates in any of the Tier I, II, III, or IV analyses described below.
Sample and Demographic Variables.

Note. HC = healthy control; KBIT-2 = Kaufman Brief Intelligence Test–2.
Scores are based on the Four Factor Index of Social Status (Hollingshead, 1975).
p < .001.
Group Assignment
Participants in the ADHD group met all of the following criteria: (a) diagnosis by the directing clinical psychologist using Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) criteria for ADHD based on a Kiddie Schedule for Affective Disorders and Schizophrenia–Present and Lifetime Version (K-SADS-PL; J. Kaufman et al., 1997) semistructured clinical interview with the participant and a mental health history questionnaire; (b) symptom count of at least four on the Barkley ADHD Current Symptoms Scale–Self-Report (Barkley & Murphy, 2006); (c) symptom count of at least six on the Barkley ADHD Childhood Symptoms Scale–Other Report (Barkley & Murphy, 2006) completed by a parent/guardian (i.e., collateral rating; Kooij et al., 2008); and (d) no indication of current comorbid conditions based on supplemental ratings scales, a mental health history questionnaire, and K-SADS-PL clinical interview. A criterion count of four (rather than six) on the Current Symptoms Scale was utilized based on literature suggesting childhood cutoffs may be too restrictive for adults (Barkley & Murphy, 2006; Simon, Czobor, Bálint, Mészáros, & Bitter, 2009).
Participants included in the HC group met all of the following criteria: (a) normal developmental history and no evidence of any clinical disorder based on supplemental ratings scales, mental health history questionnaire, and participant K-SADS-PL interview; (b) symptom count score less than four on the Barkley ADHD Current Symptoms Scale–Self-Report; (c) symptom count on collateral ratings within the nonclinical range (less than six) on the Barkley ADHD Childhood Symptoms Scale–Other Report.
Participants that presented with gross neurological, sensory, or motor impairment, history of a seizure disorder, psychosis, or Full Scale IQ score less than 85 were excluded from the study. Participants with ADHD that were currently prescribed psychostimulant medication (n = 12) were asked to discontinue use of the medication for 24 hours prior to the laboratory-based session.
Measures
Clinical interview
All participants were administered the K-SADS-PL semistructured clinical interview (J. Kaufman et al., 1997). Although the K-SADS-PL was originally developed for use with children, it has been successfully adapted for use with adults to measure past and present symptoms of psychopathology by reframing probes in the past tense and using age-appropriate behavior examples (Belendiuk, Clarke, Chronis, & Raggi, 2007), and has demonstrated strong construct and criterion validity and reliability ranging from 0.70 to 0.90 (Ambrosini, 2000; Belendiuk et al., 2007).
ADHD Ratings Scales
The Barkley (Barkley & Murphy, 2006) report forms (Current Symptoms Scale–Self-Report and Childhood Symptoms Scale–Other Report) are widely used to assess ADHD psychopathology, have internal reliability coefficients ranging from .84 to .95 (Katz, Petscher, & Welles, 2009; Zucker, Morris, Ingram, Morris, & Bakeman, 2002), and have strong discriminant validity (Barkley, Murphy, DuPaul, & Bush, 2002).
Intellectual functioning
All participants were administered the Kaufman Brief Intelligence Test–second edition (KBIT-2; A. S. Kaufman & Kaufman, 2004) to obtain an overall estimate of intellectual functioning. The KBIT-2 has strong psychometric properties with internal-consistency reliability that ranges from .89 to .96, and test–retest reliability that ranges from .76 to .93 (A. S. Kaufman & Kaufman, 2004).
Background/psychosocial history
A series of questionnaires designed to assess psychosocial history in adults obtained information such as developmental history, medical and mental health history, social history, and work history. This information was gathered to further rule out potential competing etiologies for ADHD symptoms, and was supplemented by a brief psychosocial interview conducted prior to administration of the K-SADS-PL.
Activity
MicroMini-Motionlogger® (Ambulatory Monitoring, 2010) actigraphs are wristwatch-like devices that measure motor activity by recording frequency, intensity, and duration of movement 16 times per second. Actigraphs have been used as an objective measure of activity in studies examining children with ADHD (Rapport et al., 2009), adolescents with chronic pain (Long, Palermo, & Manees, 2008), and adult ADHD smokers (Gehricke, Hong, Whalen, Steinhoff, & Wigal, 2009). The actigraphs were attached with a Velcro strap immediately above the participant’s left and right ankles and onto his or her nondominant wrist. An actigraph was not placed on the dominant hand to exclude activity associated with task response. Participants were informed that the actigraphs’ purpose is to record physiological data but no additional explanation was provided. All actigraphs were set on the Proportional Integrating Measure (loPIM) mode, which provides a measure of the participant’s movement intensity (i.e., gross activity level). Recorded movement was aggregated into 1-min epochs for analyses using the Action4 software program (Ambulatory Monitoring, 2010). For each participant, activity rates were calculated for each task by summing data from all three actigraphs. Live observation software (The Observer XT; Noldus Information Technology, 2008) was used to record time stamps for each task that was then matched to corresponding time stamps within the actigraph data.
PH WM task
The PH WM task was programmed using SuperLab 4.0 (Abboud, Schultz, & Zeitlin, 2008) and is similar to the Letter-Number Sequencing subtest in the Wechsler series of intelligence tests (Wechsler, 2008). The task is a modified version of a measure developed by Rapport and colleagues (2008) and is designed to assess PH WM based on Baddeley’s (2007) model. Participants heard a series of single digit numbers and one letter taken from a prerecorded stimulus bank. No number was presented twice in the same trial. The serial position of the letter in the sequence of stimuli (i.e., position 2, 3, 4, 5, or 6) was counterbalanced across trials to occur equally, but the letter never appeared in the first or last position of the sequence to reduce potential primacy or recency effects. Each number or letter was followed by a 200 ms interstimulus interval, and each trial was followed by a click and the appearance of a green traffic light to signal the participant should give his or her verbal response. Participants were instructed to recall the numbers aloud from smallest to largest followed by the letter. After verbally responding, participants touched the computer screen to advance to the next trial. Trials also advanced if participants failed to touch the screen after a delay commensurate with the number of stimuli presented in the trial (e.g., 40 s during trials of 4 stimuli, 50 s during trials of 5 stimuli). The responses were followed by an intertrial interval of 1,000 ms and an auditory click to signify the beginning of a new trial. A trial comprised four to seven stimuli (i.e., set sizes 4, 5, 6, and 7), and each set size block consisted of 24 trials (96 total trials). The presentation order of set size blocks was counterbalanced across participants. Figure 1 provides a visual schematic of the PH task. Five practice trials were administered prior to the experimental trials, and participants were required to respond correctly to 80% of the practice trials to proceed.
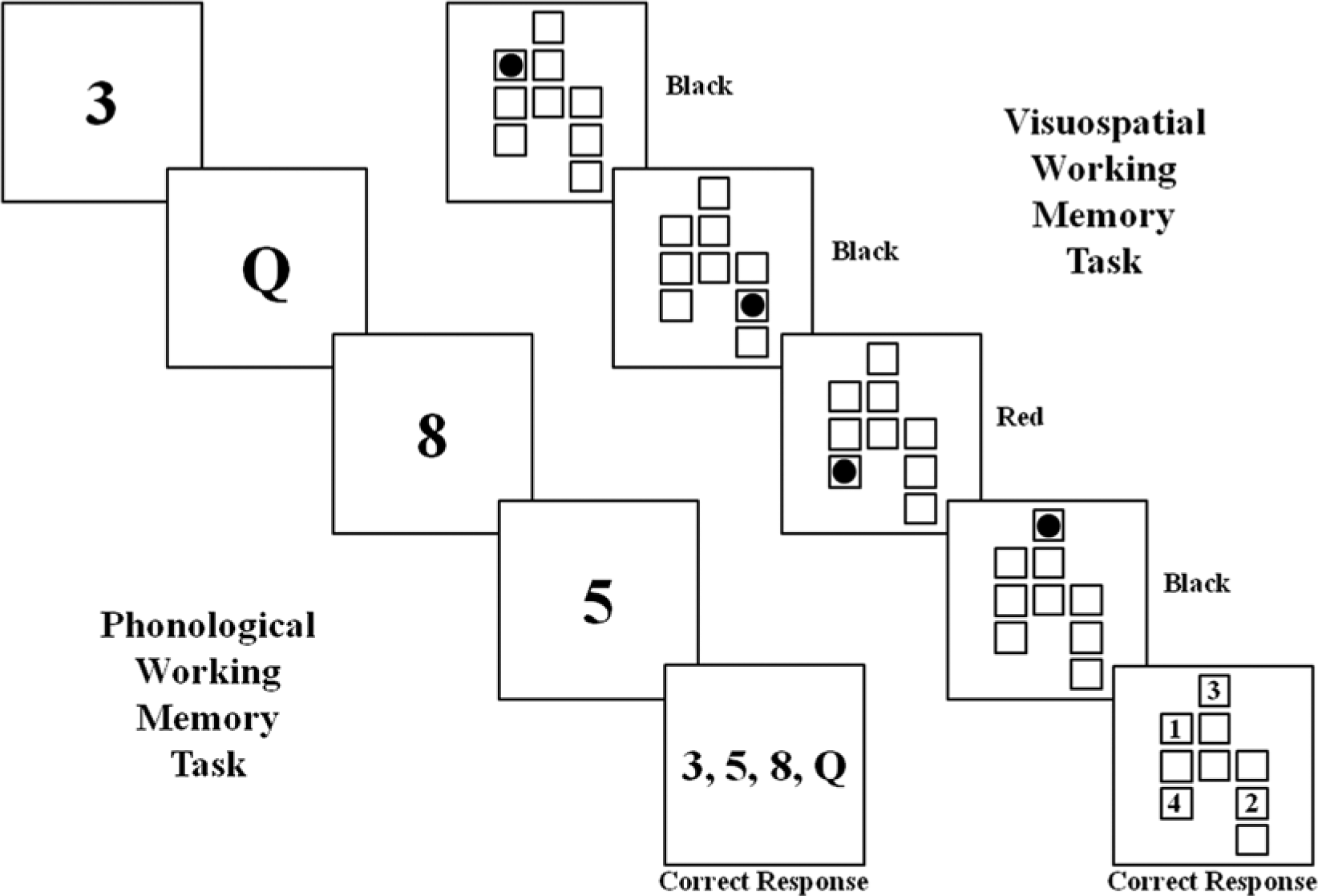
Visual schematic of the phonological and visuospatial working memory tasks.
VS WM task
The VS WM task was programmed using SuperLab 4.0 (Abboud et al., 2008) and presented to participants on a 17 × 14 inch touch-screen monitor. The task is designed to assess VS WM based on Baddeley’s (2007) model and is a modified version of the task developed by Rapport and colleagues (2008). A series of 2.5 cm diameter dots (4, 5, 6, or 7) were presented to participants sequentially for 800 ms each, in one of nine 3.2 cm squares arranged in three offset columns. The columns were offset to reduce the potential for PH coding by assigning numeric values to the square locations. One dot was red, but the rest were black. No two dots appeared in the same square during a trial and the location of the red dot was counterbalanced to appear in each of the squares an equal number of times across trials. However, the red dot was never presented first or last in the sequence to minimize potential primacy or recency effects. The presentation of each dot was followed by a 200 ms interstimulus interval, and each trial was followed by an auditory click and the appearance of a blank grid of boxes. Participants responded by touching the boxes on the screen in the same order and location in which the black dots appeared, followed by the location of the red dot. Participants were allowed to respond for a maximum of 10 s per stimulus (e.g., 40 s maximum for set size 4). The responses were followed by an intertrial interval of 1,000 ms and an auditory click to signify a new trial. A trial comprised four to seven stimuli (i.e., set sizes 4, 5, 6, and 7), and each set size block consisted of 24 trials (96 total trials). The presentation order of set size blocks was counterbalanced across participants. Figure 1 provides a visual schematic of the VS task. Five practice trials were administered prior to the experimental trials, and participants were required to respond correctly to 80% of the practice trials to proceed.
Control (C) condition
The control condition is based on previously established protocols by Rapport and colleagues (2009). Measurements of participants’ motor activity were collected while they used the Microsoft Paint program to draw or paint anything of their choice. This computer-based task is expected to place minimal WM demands on participants because they are not required to temporarily store, rehearse, or recall information. Five consecutive minutes of control condition activity were collected prior to the participant completing the WM tasks (C1) and after completing the WM tasks (C2). The use of two control condition activity measurements allowed for examination of potential fatigue effects.
Procedure
Participants first completed an online screening questionnaire that included the Current Symptoms Scale–Self-Report and a supplementary question that asked whether they had been previously diagnosed with ADHD. The initial screening questionnaire was completed by 9,133 adults. Participants who self-reported at least four inattention or hyperactivity/impulsivity problems were notified via email of their eligibility to participate in the study. Participants with no psychiatric history and less than four self-reported ADHD symptoms were also invited to participate as potential members of the HC group. A total of 1,100 individuals completed the entire questionnaire, provided contact information, met initial eligibility requirements, and were recruited via email. Seventy-eight participants responded to the recruitment email, were available during the limited weekday timeslots to complete the laboratory-based session, and were subsequently asked to complete additional online questionnaires that inquired about their social development, health history, and employment history. The online questionnaires required approximately 30 min to complete. Forty-one participants were not included in the final analyses, however, because they did not meet inclusion criteria for the ADHD or HC group after their ratings scales and clinical interviews were examined. That is, they comprised a heterogeneous group with psychiatric symptoms and disorders that were not due to ADHD (e.g., generalized anxiety disorder, dysthymic disorder, and adjustment disorder). The final sample (N = 35) consisted of 20 adults with ADHD and 15 HC adults.
Each participant completed one laboratory-based session. On arrival, the session administrator reviewed an informed consent with each participant and obtained their consent to participate. The K-SADS-PL was administered followed by a short break (3-5 min) and administration of the KBIT-2. The session was video-recorded to allow two coders to review the clinical interview for interrater agreement of diagnoses, and agreement of diagnosis/group assignment was 100%.
Participants completed PH and VS experimental tasks seated alone on a swivel chair approximately 0.70 m from a computer monitor in the testing room. Each participant completed two control conditions (C1 and C2), four PH conditions (set sizes 4, 5, 6, 7) and four VS conditions (set sizes 4, 5, 6, 7). Set size and WM modality (PH or VS) were counterbalanced to control for order and carryover effects, but the control conditions always occurred first (C1) and last (C2). All participants were offered breaks (2-3 min) between tasks or as needed. The entire laboratory-based session lasted approximately 2.5 hours.
Dependent Variable
A total extremity score (TES; Rapport et al., 2009) was calculated for each of the 10 conditions (C1, PH set sizes 4-7, VS set sizes 4-7, C2) by summing activity level (gathered from Action4 as described above) from each actigraph site (two ankles, one nondominant wrist). Summed TESs are preferred to other aggregate measures and single extremity scores, as total scores can account for individual differences in localization of movement and provide a more comprehensive sample of participants’ overall activity level (Eaton, McKeen, & Saudino, 1996). Composite TES scores for each modality (PH, VS) were computed by averaging TES across PH and VS set sizes, respectively.
A regression approach described by Alderson, Hudec, et al. (2013) was used to create three dependent variables that reflect activity associated with the CE and separate PH and VS storage/rehearsal processes. Using response data 1 from each set size of the WM tasks, a CE performance variable was created that represents shared variability between the VS and PH systems and reflects CE processes. Shared variability between VS and PH systems, attributable to CE processes, was then statistically removed to create VS and PH performance variables that reflect separate VS and PH storage/rehearsal processes, respectively. 2 Next, the PH storage/rehearsal performance variable was regressed onto the TES for the associated PH condition at each set size (set sizes 4-7) to create new variables that reflect shared variance between PH storage/rehearsal performance and activity (i.e., activity associated with PH storage/rehearsal processes). The shared variance from each regression was subsequently averaged across set sizes to provide an overall measure of activity associated with the PH storage/rehearsal component. The same procedure was repeated using the VS storage/rehearsal performance variable to create a variable that reflects the contribution of VS storage/rehearsal processes to activity. Finally, the CE performance variable for each set size was regressed onto PH and VS TES at the same set size, and the shared variability scores from both regressions were averaged to create a variable that provides a measure of the overall contribution of the domain-general CE to activity level.
Results
Data Screening
Power analyses
G*Power software (v. 3.1.2; Faul, Erdfelder, Lang, & Buchner, 2007) was used to determine the number of participants required to reliably detect differences with a repeated measures ANOVA. Power was set to 0.80 based on Cohen’s (1992) recommendations and a Cohen’s d effect size of 1.40. This effect size (ES) was chosen for comparability with the most recent study examining executive functions and activity in adults (Lis et al., 2010), though this may result in an overestimate of the required sample size due to more sensitive measurement techniques (i.e., inclusion of collateral ratings for classification, use of actigraphy for activity scores) used in the current study. However, this ES was preferred to an ES from Rapport et al.’s (2009) more analogous child study, since effect sizes are expected to be larger in studies with children which would likely result in an underestimate of the required sample size and increase potential for Type II error. Based on a Cohen’s d of 1.40, alpha of 0.05, power equal to 0.80, two groups and six repetitions, four total participants are needed for a repeated measures ANOVA to reliably detect within-subject differences and interaction effects, and 12 total participants are needed to reliably detect between-subject differences. The current study included 35 total participants.
Outliers
TESs for each condition (C1, PH set sizes 4-7, VS set sizes 4-7, C2) were screened for univariate outliers (based on ≥3.29 SD above or below the group mean) that may skew group statistics during analyses (Tabachnick & Fidell, 2001). One HC participant’s score was identified as an outlier on C2, and one ADHD participant’s TES was an outlier on PH set size 5. Each TES was replaced with the activity value equal to 3.29 SD for the group.
Tier I (composite scores)
Tier I analyses examined differences in activity level between groups (ADHD, HC) and WM modalities (PH, VS). Using a 2 × 2 mixed-model ANOVA, a significant main effect for group, F(1, 33) = 4.92, p = .034, was found, suggesting greater overall activity in the ADHD group (see Figure 2). The main effect for WM modality, F(1, 33) = 3.72, p = .062, and the interaction effect were not significant (p = .941). Composite scores are provided in Table 2.
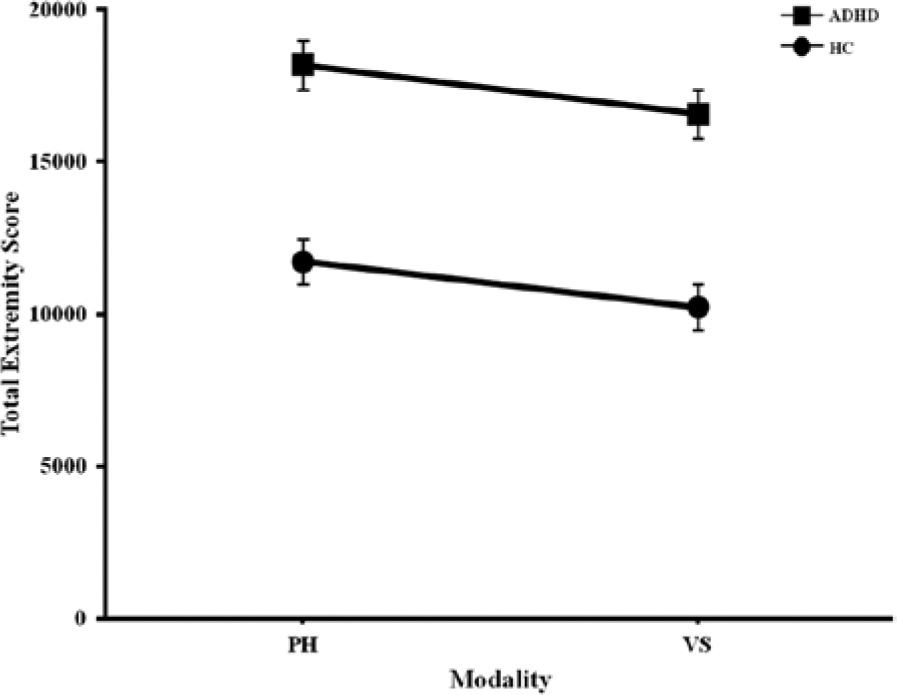
Composite total extremity scores for working memory modalities.
Composite and Set Size Comparisons of Total Extremity Scores. a
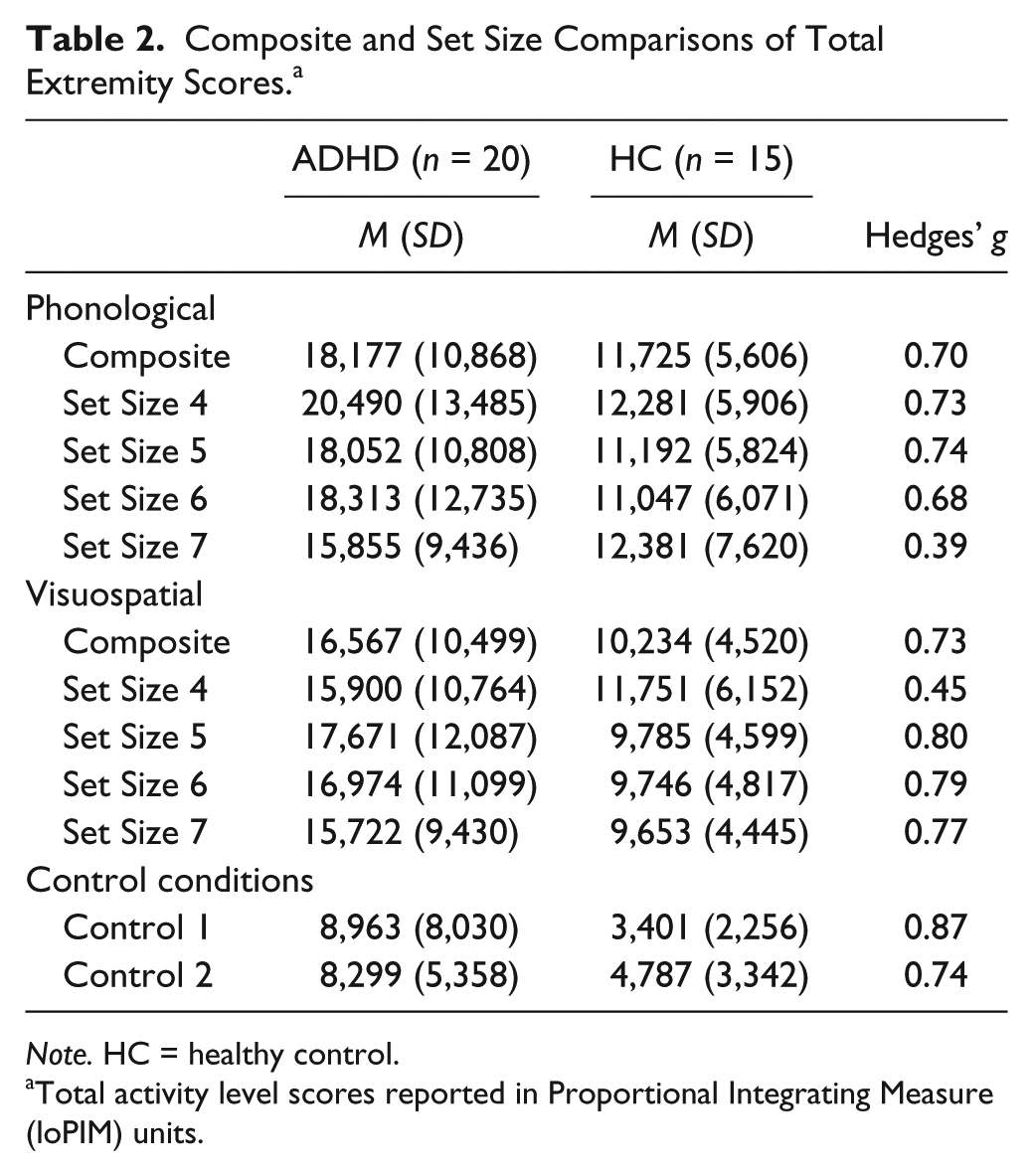
Note. HC = healthy control.
Total activity level scores reported in Proportional Integrating Measure (loPIM) units.
Tier II (WM components)
The contributions of CE and storage/rehearsal components of WM on motor activity were examined in Tier II. Three independent samples t tests were completed to examine between-group activity differences associated with each WM component (CE, PH storage/rehearsal, VS storage/rehearsal). TES associated with the CE were significantly greater in the ADHD group relative to the HC group, t(33) = 2.76, p = .009, Hedges’ g = .92. After controlling for the contribution of the CE, between-group activity level differences were significant for the PH storage/rehearsal component, t(33) = 2.50, p = .018, g = .84, but not significant for the VS storage/rehearsal component, t(33) = .116, p = .91, g = .04.
Tier III (set sizes)
Tier III analyses examined the effects of increased WM demands on total activity level. A 2 × 6 mixed-model ANOVA was conducted for each modality (PH, VS) to examine between and within-group differences in total activity across conditions (C1, four set sizes, C2).
For PH conditions, there were significant main effects for group, F(1, 33) = 5.56, p = .024, and for condition, F(5, 165) = 25.98, p < .001. The interaction between condition and group was nonsignificant, F(5, 165) = 1.27, p = .280. Results are shown in Figure 3a. Post hoc pairwise comparisons using Fisher’s least significant difference (LSD) indicated that activity level during all PH WM set sizes was significantly greater than during C1 (all p < .001) and C2 (all p < .001), but no differences were observed among PH WM set sizes (all p > .05). TES for all WM conditions are shown in Table 2.

Total extremity scores for phonological (a) and visuospatial (b) working memory and control conditions.
For VS conditions, there were significant main effects for group, F(1, 33) = 5.75, p = .022, and condition, F(5, 165) = 27.82, p < .001. The interaction between condition and group, however, was not significant, F(5, 165) = 1.50, p = .192. Post hoc pairwise comparisons using Fisher’s LSD indicated that activity level during all VS WM set sizes was significantly greater than during C1 (all p < .001) and C2 (all p < .001), but no differences were observed among VS WM set sizes (all p > .05). Figure 3b depicts TES for VS conditions.
Tier IV (control conditions)
The final step of analyses determined whether group differences in activity were present during control conditions, after controlling for activity associated with WM. That is, this step of analyses aimed to examine the extent to which observed group differences in activity level during control conditions (C1, C2) represent ubiquitous ADHD-related activity that occurs independently of WM task demands (Halperin et al., 2008; Porrino et al., 1983), or reflect the influence of WM-related attentional demands associated with the Paint program (Rapport et al., 2009). Performance variables for CE, PH storage/rehearsal, and VS storage/rehearsal were regressed onto both control conditions (C1, C2). Residual C1 and C2 scores represented activity during the control conditions that was unrelated to WM (i.e., variance associated with CE, PH storage/rehearsal, and VS storage/rehearsal removed). A mixed-model ANOVA examining group (ADHD, HC) differences in activity during control conditions (Residuals C1 and C2) resulted in a nonsignificant interaction effect (p = .174) and condition main effect (p = .844). The main effect for group was significant, F(1, 33) = 5.16, p = .030, g = .78, however, indicating that adults with ADHD were more active during control conditions than HC adults after controlling for WM.
Discussion
The current study examined the functional relationship between activity level and WM demands in adults with ADHD. Previous studies have suggested hyperactive symptoms associated with ADHD tend to remediate after adolescence (Biederman et al., 2000; Hill & Schoener, 1996; Kessler et al., 2010), while more recent studies suggest ADHD-related hyperactivity persists into adulthood (Halperin et al., 2008; Lis et al., 2010). Inconsistent findings in extant literature may be due to methodological differences in assessment procedures or task parameters. The current study improved on previous methodological procedures by requiring collateral ratings rather than relying solely on self-report measures for group classification and by using objective activity measurement techniques (e.g., actigraphy). The inclusion of collateral ratings and objective activity measures is particularly important for accurate group classification and detection of ADHD-related activity, given literature that suggests adults with ADHD tend to underreport symptom presence and severity due to poor insight and difficulty with retrospective recall (Kooij et al., 2008; McGough & Barkley, 2004). Collectively, the current results indicated that adults with ADHD were more active than HC, which provides support for the notion that excessive activity related to ADHD continues into adulthood.
A unique contribution of the current paper is the examination of activity level during discrete VS and PH WM tasks. A recent study by Rapport and colleagues (2009) demonstrated that children with ADHD were more active than typically developing peers across both modalities, and all children exhibited greater levels of activity during the PH task compared with the VS task. A similar pattern was anticipated in adults; as expected, adults with ADHD exhibited greater activity compared with HC during the PH and VS WM tasks. Unlike findings with children (Rapport et al., 2009), however, adults in the current study exhibited similar levels of activity for PH and VS modalities, as indicated by PH and VS composite scores that reflect the combined contribution of CE and storage/rehearsal processes. The discrepancy between the current study’s findings with adults and previous findings with children may be related to several ontological and methodological variables. For example, compared with typically developing peers, children with ADHD experience a delay in cortical maturation of neuroanatomical areas associated with WM, particularly areas typically associated with VS processing (Shaw et al., 2007). Examination of Shaw and colleague’s longitudinal findings, however, suggest that the cortical discrepancies between individuals with ADHD and nonaffected peers become less pronounced by adolescence, which may explicate the similar motor activity across WM modalities in the current adult sample. Differences in stimuli presentation may also account for the current results contradicting findings with children. Specifically, Rapport et al. (2009) examined WM with a PH task that presented numbers and letters visually, whereas the current study utilized an auditory presentation of stimuli. The latter approach is expected to provide a more pure measure of the contribution of PH processes as it does not require additional attentional control to inhibit the visual representation of the PH stimuli and allocate resources to articulatory rehearsal processes (Palmer, 2000), and/or PH information is given direct access to storage/rehearsal processes without the need for orthographic to PH conversion of visually presented numbers and letters (Baddeley, 2007).
Another unique contribution of the current study was its examination of discreet storage/rehearsal and CE processes. Storage/rehearsal processes (i.e., composite scores with CE variance removed) reflect the limited capacity system responsible for retaining information for brief periods (i.e., short-term memory), whereas CE processes (i.e., composite scores with storage/rehearsal processes removed) involve the controlled-attention component responsible for manipulating information (Engle, Tuholski, Laughlin, & Conway, 1999). Examination of the independent contribution of WM components indicated that the CE (.92) and PH storage/rehearsal subsystem (.84) were both associated with large-magnitude between-group differences in activity, while the VS storage/rehearsal subsystem did not significantly contribute to activity level after controlling for the contribution of the CE. Comparison of these findings with the findings of Rapport and colleagues’ (2009) similar study of children reveals a number of discrepancies. For example, the current study’s CE effect size is two standard deviations smaller than the effect size (g = 3.03) reported by Rapport and colleagues (2009), though this difference could be anticipated given that adults tend to exhibit less motor activity overall compared with children (Solanto, Wasserstein, Marks, & Mitchell, 2012). However, the current study’s finding of a significant large-magnitude between-group difference in activity associated with the PH storage/rehearsal subsystem, as well as the similarity of the PH storage/rehearsal and CE effect size magnitudes, was unlike previous findings with children (Rapport et al., 2009), but consistent with more recent findings from a study of adults with ADHD that reported larger WM deficits in the PH system compared with the VS system, and similar deficits in WM performance associated with the CE and the PH storage/rehearsal system (Alderson, Hudec, et al., 2013). Collectively, the findings appear to suggest improved CE functioning in adults with ADHD that corresponds with a reduction in overall motor activity.
The current study also examined activity across control and WM conditions of increasing demands on storage/rehearsal processes (i.e., increasing set sizes), and found that both groups’ activity increased during all WM conditions relative to control conditions. Furthermore, adults with ADHD exhibited greater activity across all conditions, including control conditions, relative to adults in the HC group. Follow-up analyses indicated that between-group differences during control conditions were not solely related to WM demands associated with the control task. Collectively, these findings suggest that adults with ADHD, relative to HC adults, exhibit relatively ubiquitous hyperactivity that is exacerbated when demands on WM increase, and consequently provide partial support for Rapport et al.’s (2001) model. That is, these findings simultaneously corroborate the hypothesized functional relationship between WM and ADHD-related hyperactivity, while also indicating that some ADHD-related hyperactivity in adults may occur independently of situational WM demands, consistent with the early findings of Porrino et al. (1983). The current findings also contradict previous findings with children that indicated there were no group differences in activity during control conditions after controlling for the contribution of WM components (Rapport et al., 2009). The discord between control condition activity in the current study of adults and previous study of children was surprising, but may be related to several developmental factors. For example, typically developing children and children with psychiatric difficulties are expected to exhibit greater motor activity relative to adults (Miles, 2007), regardless of setting or situation-specific cognitive demands. This ubiquitous motor activity demonstrated by both groups in childhood may persist in adults with ADHD and become more apparent as HC adults become less active over time. Alternatively, the current findings may suggest that ontologically related differences in other neurocognitive variables that were not examined in the current study may also persist and contribute to motor activity in adults.
Finally, although both groups exhibited greater activity during WM conditions relative to control conditions, neither group exhibited significant changes in activity across the PH and VS set sizes. This finding is consistent with Rapport et al.’s (2009) study of children that reported significant activity increases from control to WM conditions, but nonsignificant variability in activity across WM set sizes. Consistent with the interpretation provided by Rapport and colleagues, the current findings may reflect the predominant role of CE processes in ADHD-related WM deficits. That is, potential set size differences only inform about differences in storage/rehearsal processes. In contrast, the CE does not have any storage/rehearsal processes associated with it (Baddeley, 2007), and consequently is not expected to evidence significant differences across set sizes. Alternatively, these findings may reflect a ceiling effect such that activity associated with storage-rehearsal demands may be more apparent at larger set sizes (e.g., 8, 9, or 10 stimuli) not included in the current study.
Findings from the current study provide important insight into the relationship between WM and motor activity in adults with ADHD, but a few potential limitations of the current study warrant consideration. The current sample was relatively small, which raises concern for potential Type II errors and limits the study’s ability to generalize to the larger population of adults with ADHD. However, a priori power analyses indicated the current sample was sufficient to detect within-group, between-group, and interaction effects for the planned analyses, and examination of effect sizes for nonsignificant effects suggests that additional participants would not likely change interpretations of the current findings. Regardless, findings from relatively small samples should be interpreted with caution, and future replication studies with larger samples are needed. Large-sample replication studies may also benefit from their ability to examine additional potential moderating variables. The composition of the current sample may also be considered a limitation. For example, the ADHD and HC groups included males and females, which may have confounded the current results, since previous findings from nonclinical samples have demonstrated that men, compared with females, perform worse on PH WM tasks and better on VS WM tasks (Schmidt et al., 2009). These concerns are limited, however, as sex-related WM differences do not appear to disproportionately affect ADHD or HC adults (Schweitzer et al., 2006). The current sample also included all ADHD subtypes. Inclusion of the Predominantly Inattentive type may have resulted in an underestimate of adult activity due to the presence of fewer hyperactive/impulsive symptoms; however, the current study reflects a preliminary examination of the association between motor activity and WM in adults with ADHD, and future studies that investigate the influence of gender and subtype on the relationship between WM and activity level in adults with the disorder would augment the current findings.
In summary, the current findings suggest that individuals with ADHD continue to exhibit significant levels of hyperactivity into adulthood. Current findings also suggest that a proportion of ADHD-related hyperactivity in adults is associated with increased demands on WM, especially the CE, consistent with predictions from Rapport et al.’s (2001) functional WM model. That is, increased demands on WM appear to result in increased motor activity (i.e., comparison of activity from control with WM conditions) in adults with ADHD and HC. In the context of real-life situations, these findings appear to suggest that healthy adults’ activity increases during conditions of high WM demands, but is not likely perceived as excessive or hyperactive as their baseline activity is very low (i.e., increased activity remains in the nonclinical/normal range). In contrast, what might have been perceived as minor fidgeting or restlessness by adults with ADHD during low WM demands becomes hyperactivity (and potentially impairing) during high WM demands.
Additional research is needed to determine if inconsistent findings, compared with other adult and child studies, are associated with methodological differences (i.e., diagnostic procedures, task parameters) or are representative of differences in the underlying causes of ADHD symptomology. Identifying specific underlying neurocognitive deficits associated with ADHD-related activity could greatly improve diagnostic accuracy and aid in development of treatment protocols if specific neurological deficits (i.e., WM, behavioral inhibition), rather than peripheral symptoms (e.g., impulsivity, inattention), were assessed and targeted. Even more, understanding that ADHD persists into adulthood and is associated with substantial lifelong difficulties increases the need to establish accurate diagnostic criteria, to develop appropriate interventions, and to implement treatment strategies early in development. Finally, as with any highly controlled lab-based experiment, ecological validity and generalizability of the current study’s findings to real-world situations are limited. Consequently, nonlaboratory studies that examine the relationship between objectively measured ADHD-related hyperactivity (e.g., actigraphy) and real-life situational changes in WM demands are needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.