
Abstract
As the second leading cause of death among individuals aged 18 to 25 years (Centers for Disease Control and Prevention, 2011), suicide represents a significant public health problem. In a national survey, 6.4% of college students reported past year suicidal ideation (SI; American College Health Association [ACHA], 2009), a strong predictor of attempt (Borges et al., 2010). Although Major Depressive Disorder (MDD) symptoms predict SI (Cavanagh, Carson, Sharpe, & Lawrie, 2003), impulsive disorders, (e.g., ADHD) not only increase SI risk (Chronis-Tuscano et al., 2010), but also more strongly predict progression from ideation to attempt than depression (Nock et al., 2013).
Given that ADHD increases risk for depressive symptoms (Angold, Costello, & Erkanli, 1999; Chronis-Tuscano et al., 2010) and the strong link between depression and SI, depressive symptoms may mediate the link between ADHD and SI. Little research explains why ADHD increases risk for SI, demonstrating the need to evaluate possible mechanisms. Emotion regulation (ER) deficits are frequently associated with negative emotionality for those with ADHD (Marx et al., 2011), suggesting that ER deficits may amplify risk for depressive symptoms and SI for college students with ADHD symptoms (Seymour et al., 2011). Thus, we evaluated the mediating role of depressive symptoms in the link between ADHD and SI and the extent to which ER moderates these associations.
ADHD, Depression, and Suicide Risk
Although research suggests that ADHD may increase risk of SI (Hinshaw et al., 2012; James, Lai, & Dahl, 2004), little research has evaluated potential mechanisms. In a meta-analysis on the link between ADHD and suicide, individuals with ADHD displayed 2.91 times the risk of attempting suicide than controls (James et al., 2004). Individuals with a childhood ADHD diagnosis were almost twice as likely to consider suicide and 7 times as likely to attempt suicide in high school compared with those without ADHD in a longitudinal follow-up study (Barkley & Fischer, 2005). By young adulthood, those with a previous ADHD diagnosis were still 2.6 times more likely to have considered suicide than controls.
Depressive symptoms, which are frequently associated with suicidal behavior, may underlie the link between suicide risk and ADHD. However, results regarding the link between ADHD and depressive symptoms have yielded both positive (Biederman, Petty, Evans, Small, & Faraone, 2010; Chronis-Tuscano et al., 2010) and negative findings (Hinshaw et al., 2012), and only one study has explored the relation among ADHD, depression, and suicide risk. In that longitudinal study, Barkley and Fischer (2005) found that children who had both a childhood diagnosis of ADHD and considered suicide in high school were much more likely to have MDD (49%), compared with children with a childhood diagnosis of ADHD and no SI (10%). Results also extended to SI in young adulthood (63% vs. 15%). These results suggest that depressive symptoms may mediate the link between ADHD and SI. Identifying mediating factors for SI in individuals with ADHD may help develop effective prevention strategies to reduce negative outcomes for this population.
ER Deficits: Moderator of Suicide Risk for ADHD and Depressive Symptoms
ER occurs in the context of emotion; emotion occurs in a situation, directs attention, derives meaning, and influences a multi-system response (Gross & Thompson, 2010). Thus, ER is defined herein as internal and external strategies that modulate the magnitude and/or type of emotion experienced. These strategies include attention to and appraisal of emotion, the clarity of that appraisal, the quantity and quality of coping strategies, and employing these strategies to achieve a goal. Although distinct from ER, emotional reactivity—the sensitivity, intensity, and persistence of an emotion—may predispose individuals to ER deficits (Nock, Wedig, Holmberg, & Hooley, 2008). Given that suicidal behaviors may represent an attempt to cope with emotional distress for which adaptive coping strategies are inaccessible (Baumeister, 1990), reactivity and deficits regulating emotions may link ADHD and depressive symptoms to SI.
While the literature is sparse, evidence suggests that difficulty coping with negative emotions significantly contributes to the link between ADHD and depression. Individuals with ADHD experience more distress from negative emotions and behave more impulsively when distressed. Barkley and Fischer (2010) found that young adults with persistent ADHD were more likely to report being impatient, quick tempered, frustrated, and emotionally over-reactive than controls. The few studies that have evaluated ER deficits for adults with ADHD also indicate that ADHD is associated with less effective management of emotional distress (Marx et al., 2011), difficulties with identifying and accepting emotions, as well as difficulties acting with self-control (Edel et al., 2010). Negative emotionality has mediated the link between ADHD symptoms and the urge to act impulsively when distressed (i.e., negative urgency) for college students (Mitchell, Robertson, Anastopolous, Nelson-Gray, & Kollins, 2012). Thus, ADHD has been linked with decreased capacity to regulate emotions in young adulthood, which has implications for suicidal thoughts and behaviors.
ER deficits are also associated with depressive symptoms and SI. In an adolescent sample, depression and SI were linked to deficits in accepting negative emotions, identifying emotions (i.e., emotional clarity), being goal-oriented, and being impulsive when distressed (Weinberg & Klonsky, 2009). Rajappa, Gallagher, and Miranda (2012) also found that not accepting negative emotions was associated with previous suicide attempts in college students. Among adolescents, deficits in emotional clarity partially mediated the link between depression and SI (Jacobson, Marrocco, Kleinman, & Gould, 2011). Understanding how ER, depression, and SI are related can guide risk assessments and treatment targets for college students with ADHD.
The Current Study: Research Questions
Research shows that ADHD confers increased risk for depression and suicide attempt. However, less research has evaluated links between ADHD and SI or ADHD, depression, and SI. We sought to fill this gap by examining the degree to which depression mediated the association between ADHD and SI. As ER deficits are associated with ADHD, depressive symptoms, and SI, we examined the degree to which ER deficits magnified risk for depression and SI for those with ADHD as well as the indirect effect of ADHD on ideation through depression. Given previous research, we predicted that depressive symptoms mediated the link between ADHD and SI and that ER deficits amplified the risk for both depression and SI for those with ADHD.
Method
Participants and Procedure
Participants were 627 college students ages 18 to 25 years (M = 20.23, SD = 1.40; 60% female) enrolled at a large, public, Southeastern university. Many students were in their first year in school (43%). Nearly half (47%) identified as European American, 12% as African American, 3% as Asian, and 3% as Latino. About 4% did not specify race/ethnicity; 31% identified as multi-racial. Moreover, 14% of participants had a childhood household income of <US$40,000/year, compared with 48% of participants with a childhood household income of >US$100,000/year. About 41% of mothers of participants had taken some college courses. Recruited via announcements in undergraduate psychology courses, participants completed an online survey in one sitting. Items with similar content showed no significant inconsistencies when compared. Participants received extra course credit; the university Institutional Review Board approved all procedures.
Measures
The Current Symptoms Scale–Self-Report Form (CSS)
The 36 self-reported items on the CSS (Barkley, Murphy, & Fischer, 2008) have a 4-point scale (0 = never or rarely to 3 = very often) and correspond to the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) criteria for ADHD. Eighteen items asked about current symptoms, and eighteen items assessed childhood symptoms. Validity concerns about retrospective self-report (Mannuzza, 1993) led us to use only current symptoms. Items were summed for a total scale score, given the multicollinearity between inattention and hyperactivity (r = .78, p < .05). Reliability for this sample was strong (α = .92). Self-report is correlated with parent and spousal report (Barkley et al., 2008). The CSS is often used to identify diagnostic levels of ADHD symptoms in research and clinical practice (e.g., Covey, Manubay, Jiang, Nortick, & Palumbo, 2008).
Research with a normative sample indicates that a CSS total score ≥ 27.8 is the clinical cutoff for ADHD for those 17 to 29 years old (Barkley et al., 2008). Analyses included ADHD as a dichotomous variable with 0 for symptoms below the diagnostic cutoff and 1 for those above the cutoff, who are referred to as having ADHD in this study. Childhood and current ADHD symptoms were highly correlated (r = .63, p < .001); rates of diagnosis were comparable between childhood and current ADHD symptoms.
Emotion Regulation Difficulties Scale (DERS)
The 36 items assessed emotion regulation across six domains: non-acceptance of negative emotions (6 items; α = .90; e.g., “When I’m upset, I become angry with myself for feeling that way”), inability to engage in goal-directed behaviors when distressed (5 items; α = .87; e.g., “When I’m upset, I have difficulty focusing on other things”), difficulties controlling impulsive behaviors when distressed (6 items; α = .85; e.g., “When I’m upset, I become out of control”), limited access to effective ER strategies (8 items; α = .90; e.g., “When I’m upset, I believe that there is nothing I can do to make myself feel better”), lack of emotional awareness (6 items; α = .84; e.g., “When I’m upset, I acknowledge my emotions”), and lack of emotional clarity (5 items; α = .83; e.g., “I have difficulty making sense out of my feelings”). The response scale had five options from almost never to almost always. The DERS has acceptable validity (Gratz & Roemer, 2004).
Brief Symptoms Inventory (BSI)
The 53 self-reported items on the BSI (Derogatis & Coons, 1993) measure constructs related to psychological adjustment using a 5-point scale (1 = almost never to 5 = almost always). Analyses included only the depressive symptoms subscale (6 items), which includes one item that assesses SI. We excluded that item to reduce collinearity between depressive symptoms and SI. Reliability for this scale without the SI item was strong (α = .89) with responses ranging from 6 to 29. The depression subscale has strong construct validity (Schwannauer & Chetwynd, 2007) and discriminates between those with and without MDD (Johnson, Chipp, Brems, & Neal, 2008).
SI was assessed on the BSI with one question (“How often do you have thoughts of ending your life?”). The item displayed significant positive skew and responses ranged from 1 to 4. Thus, we recoded the item so that responses of “sometimes” or above were rated as a 1 (“yes”) and a response of “almost never” was coded as 0 (“no”).
Analytic Procedures
Model description
Mplus v.7.1 (Muthén & Muthén, 2010) was used for mediation analyses; SPSS v.19 (IBM Company, 2010) was used for remaining analyses. We estimated a moderated mediation model to test the degree to which depressive symptoms mediated the associations among ADHD diagnosis and SI and the degree to which ER moderated the association ADHD diagnosis had with depressive symptoms and SI, including the indirect and direct effect of ADHD diagnosis on SI (see Figure 1). Using path analysis in a structure equation model framework, multiple regression analyses were simultaneously generated for all paths of the mediation model. Analyses evaluated the effects of ADHD diagnosis, ER, and their interaction on depressive symptoms (path a), the effect of depressive symptoms on SI (path b), and the direct effects of ADHD diagnosis, ER, and their interaction on SI (path c’). The effect of ADHD diagnosis was first evaluated without ER constructs included in the mediation model. Given the strong association among ER subscales, the moderation of ER subscales was considered in independent models for a total of seven models. To aid interpretation and reduce multicollinearity, all variables were mean centered (Cohen, Cohen, West, & Aiken, 2003).
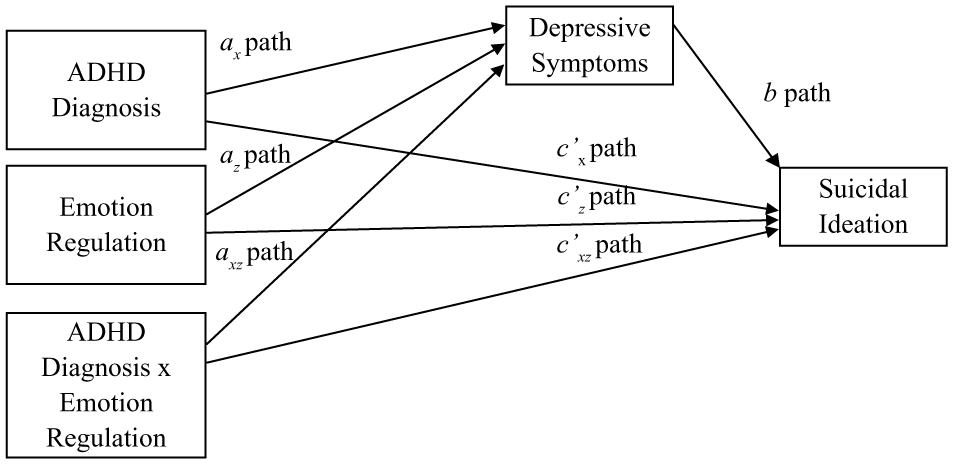
Conceptual moderated mediation model.
The model was tested using weighted least squares, means and variance adjusted chi-square (WLSMV) estimation, which provides robust estimation of standard errors for path coefficients using a probit link when the outcome variable is discrete (Asparouhov, 2005). Coefficients where SI was the outcome (path b and the indirect and direct effects) were probit regression estimates. Probit estimates represent the amount of z-score change in the outcome for every one unit change in the predictor. The indirect effect represents the product of a and b paths. Because the indirect effect (ab) is not likely to come from a normal distribution (MacKinnon, 2008), significance of the indirect effect was tested with bootstrapping using 5,000 generated samples, where 95% confidence intervals represented the range of the point estimates (Preacher & Hayes, 2008). Confidence intervals that do not include zero denote a significant indirect effect. Models were fully saturated, so fit statistics were not applicable.
Significant mediation would be indicated if the indirect effect of ADHD, ER, or the interaction of ADHD and ER reached statistical significance where bootstrapped confidence intervals did not include zero. Moderated mediation would be indicated only if the bootstrapped confidence intervals for the interaction of ADHD and ER did not include zero. This model also assessed the possibility that ER constructs may moderate the effect of ADHD diagnosis on depression symptoms (axz path) and on SI (c’ax path or direct effect).
Covariates
Covariates were selected based on research demonstrating their association with the mediator and outcome variables and based on associations among variables in these data. Covariates were participant sex (0 = “male”; 1 = “female”), race/ethnicity (0 = “European American”; 1 = “non–European American”), mother’s education, and household income.
Missing data
Only 4.4% of data were missing, which corresponded to 29 participants who chose not to disclose their race/ethnicity. Variables included in the study were not significantly different based on missingness, demonstrating that missing data were sufficiently missing at random (MAR). Missing data were managed in Mplus v.7.1 (Muthén & Muthén, 2010) with full information maximum likelihood (FIML), which generates accurate parameter estimates and standard errors when data are MAR.
Results
Descriptive Statistics
Descriptive statistics and correlations were assessed for continuous variables (see Table 1). Sixty-one participants (9.3%) had ADHD symptoms above the clinical cut-point, which is higher than prevalence rates of ADHD found in other studies with college students (2%-8%; see DuPaul, Weyandt, O’Dell, & Varejao, 2009). About 12% of participants reported thinking about ending their life “sometimes” or more often, which corresponds to prevalence rates of college student SI in other studies (12%; Wilcox et al., 2010). Although depressive symptoms and Emotional Impulsiveness were positively skewed, results did not differ in statistical significance or effect size based on log-transformed depressive symptoms and Emotional Impulsiveness; thus, we chose to report results with non-transformed variables.
Descriptive Statistics and Correlations Among Continuous Variables.
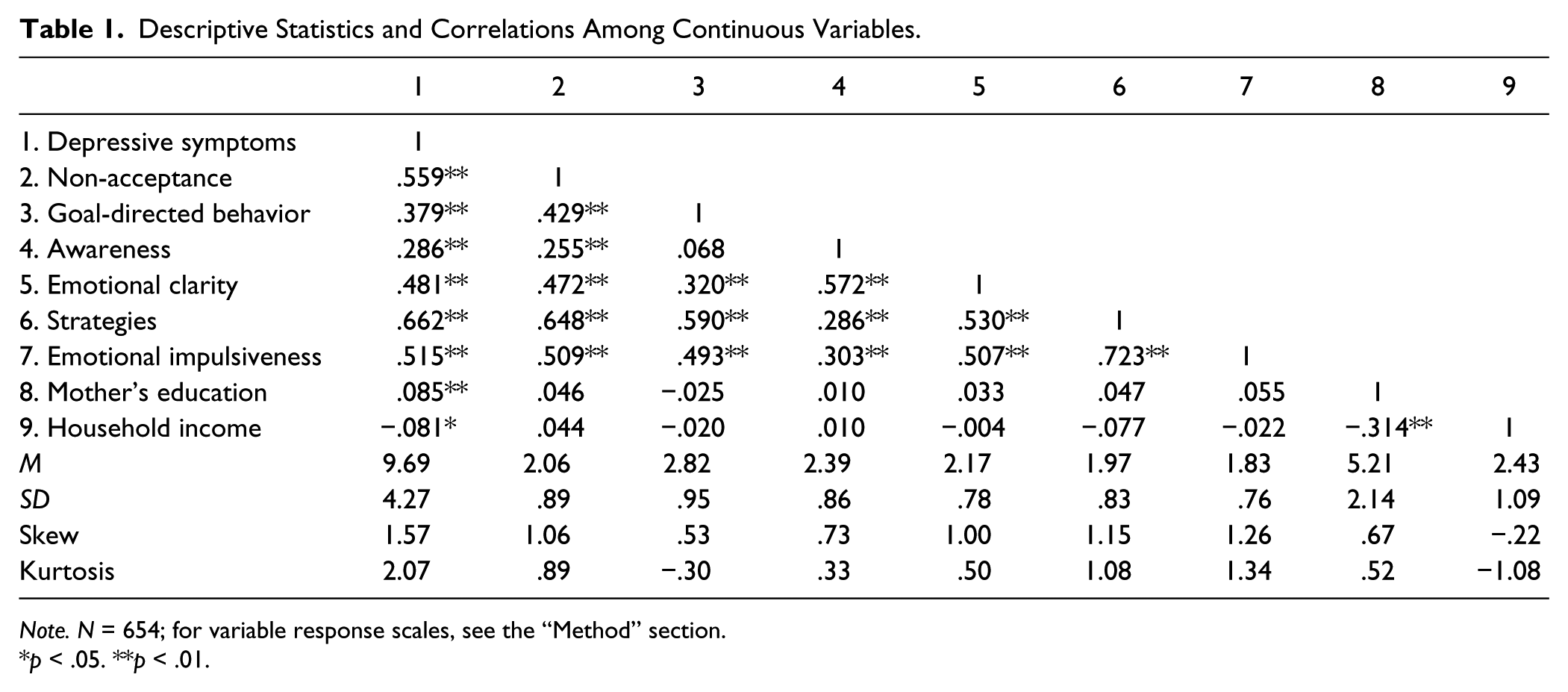
Note. N = 654; for variable response scales, see the “Method” section.
p < .05. **p < .01.
SI occurred more frequently for participants with clinical levels of ADHD symptoms. Twenty participants with ADHD reported SI (32.3%), compared with 62 participants without ADHD (10.5%). Those with ADHD were 3.08 times more likely to report SI than those without ADHD (χ2 = 24.29, p < .001). Men were 1.89 times more likely to report SI than women, with 18.7% of men reporting SI, compared with 9.9% of women (χ2 = 9.79, p < .002). Rates of ADHD diagnosis and SI did not differ according to household income or maternal education. t-test analyses indicated that those with ADHD symptoms and those who reported SI had significantly higher scores on ER constructs and depressive symptoms.
Depressive symptoms were positively associated with ER constructs with effect sizes ranging from small to large. All associations among ER constructs were significant and positive with effect sizes ranging from very small to large. The wide range of effect sizes for the association of ER constructs with depressive symptoms suggests that ER constructs may play different roles in the links between ADHD and SI as well as depression and SI. Thus, evaluating the role of each ER construct rather than the total score may provide meaningful findings. Furthermore, the significant collinearity among ER constructs supports evaluating the moderating effect of ER subscales in independent models.
Mediation Results
ADHD diagnosis
A mediation model with ADHD diagnosis and no ER constructs was evaluated to identify the independent effect of ADHD diagnosis in the model. Depressive symptoms significantly mediated the link between ADHD and SI (see Table 2), as indicated by confidence intervals that did not include zero. The direct and total effects of ADHD on SI were both positive and significant as was the association between ADHD and depressive symptoms (see Tables 3 and 2, respectively). The total effect represents the combined effect of the indirect and direct effect of ADHD on SI. The probit threshold or intercept for SI of 1.178 (see Table 3) can be interpreted as a z-score value and transformed into a probability, which in this case represents the probability of SI when all parameters are at their mean (p = .881). Using probit values for the direct effect and indirect effect, ADHD directly increases risk for SI above the threshold value by .178 z-score units and indirectly by .216 z-score units.
Indirect and Total Effects of ADHD and Emotion Regulation on Suicidal Ideation.
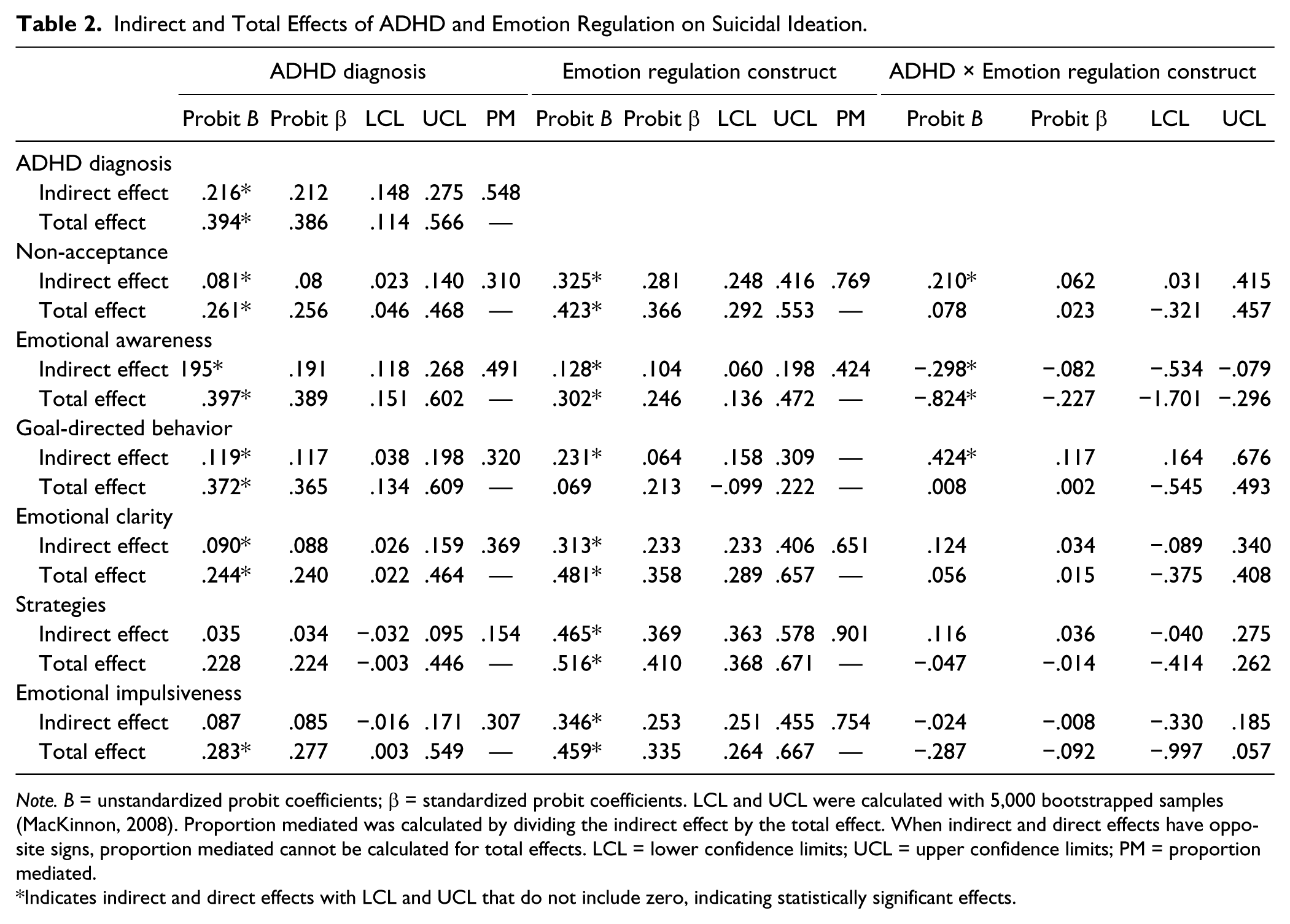
Note. B = unstandardized probit coefficients; β = standardized probit coefficients. LCL and UCL were calculated with 5,000 bootstrapped samples (MacKinnon, 2008). Proportion mediated was calculated by dividing the indirect effect by the total effect. When indirect and direct effects have opposite signs, proportion mediated cannot be calculated for total effects. LCL = lower confidence limits; UCL = upper confidence limits; PM = proportion mediated.
Indicates indirect and direct effects with LCL and UCL that do not include zero, indicating statistically significant effects.
Path Coefficients for Mediation Models.
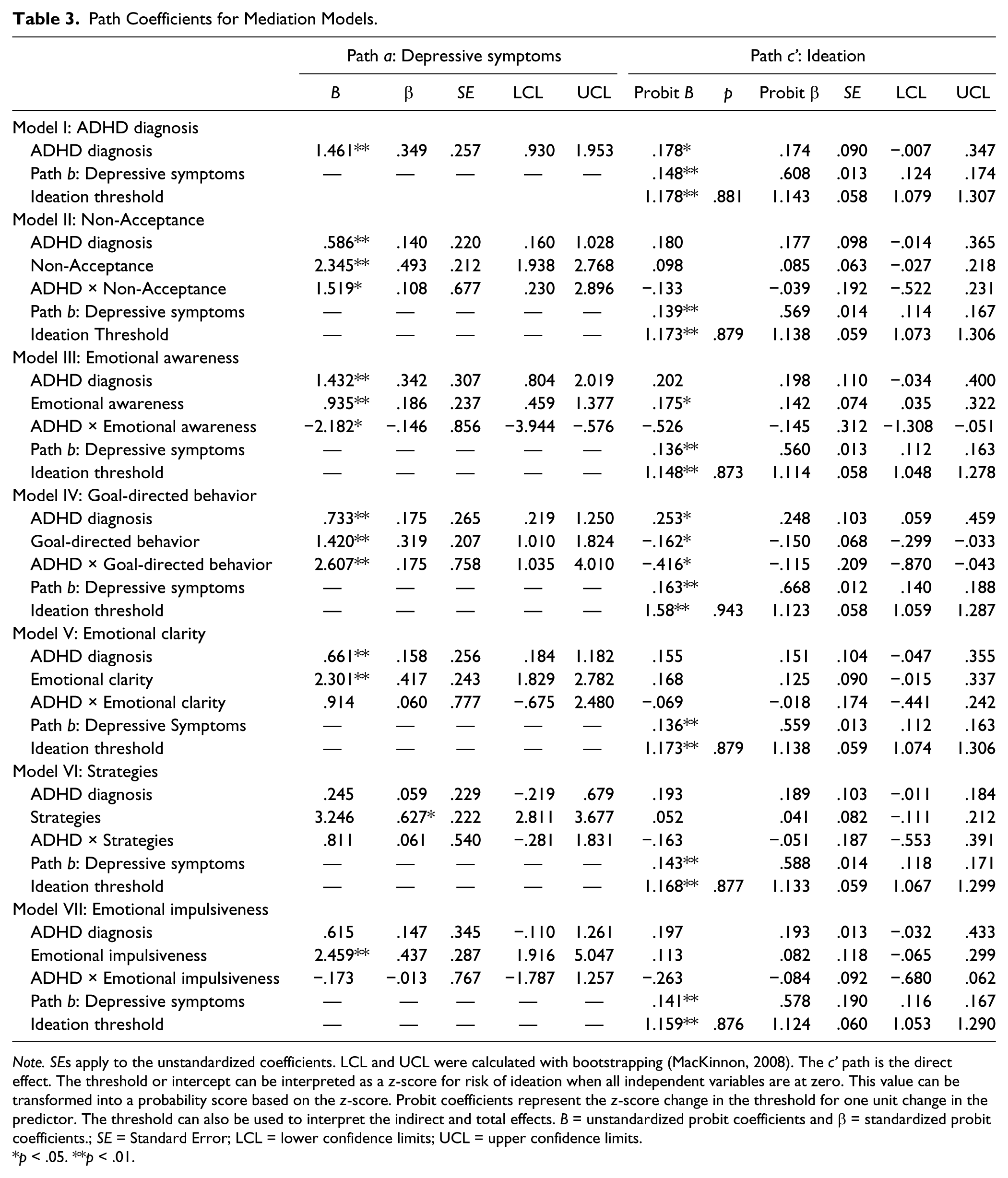
Note. SEs apply to the unstandardized coefficients. LCL and UCL were calculated with bootstrapping (MacKinnon, 2008). The c’ path is the direct effect. The threshold or intercept can be interpreted as a z-score for risk of ideation when all independent variables are at zero. This value can be transformed into a probability score based on the z-score. Probit coefficients represent the z-score change in the threshold for one unit change in the predictor. The threshold can also be used to interpret the indirect and total effects. B = unstandardized probit coefficients and β = standardized probit coefficients.; SE = Standard Error; LCL = lower confidence limits; UCL = upper confidence limits.
p < .05. **p < .01.
We then evaluated the role of ER by including in separate models each ER construct as a moderator of the link between ADHD and SI as well as ADHD and depressive symptoms. Results demonstrated that depressive symptoms mediated the association between ADHD and SI in all models except for models including Strategies and Emotional Impulsiveness as moderators (see Table 2). Strategies and Emotional Impulsiveness were strongly related to depressive symptoms allowing for little additional variance to be accounted for by other variables. The direct effect of ADHD on SI (c’ path) was positive and significant only in the model with Goal-Directed Behavior (see Table 3). The total effect of ADHD was similarly positive and statistically significant for all models except for the model with Strategies (Table 2).
Non-Acceptance
ADHD interacted with Non-Acceptance to indirectly affect SI (see Table 2), where confidence intervals did not include zero. The direct and total effects of the interaction term were not significant (Tables 3 and 2, respectively). The interaction of Non-Acceptance and ADHD was significantly associated with increased depressive symptoms, which significantly increased the risk of SI. According to simple slope evaluation, problems with accepting negative emotions were higher at diagnostic levels of ADHD symptoms, which corresponded to increased depressive symptoms and indirectly increased risk for SI (see Table 4; Figure 2). Interpreting the probit threshold (intercept) for SI of 1.173 (see Table 3) as a z-score indicates that the probability of SI when all parameters are at their mean was .879. Simple slope results indicated that at diagnostic levels of ADHD, one unit increase in problems with Non-Acceptance indirectly increased risk for SI by .269 z-score units above the SI threshold.
Simple Effects for the Interactions of ADHD and Emotion Regulation.

Note. B = unstandardized coefficients; Standard error for simple effects of the indirect effect used the following equation: √ (b2 × sa2 + a2 × sb2). High ADHD: ADHD symptoms above the diagnostic cutoff; Low ADHD: ADHD symptoms below the diagnostic cutoff. See Figures 1-3 for a visual representation of the interaction of ADHD and ER subscales on depressive symptoms and ideation. SE = Standard Error; ER = emotion regulation.

Interactions of emotion regulation constructs and ADHD predicting depressive symptoms.
Independent of ADHD, the indirect and total effects of Non-Acceptance on SI were positive and significant. Every one unit increase in Non-Acceptance indirectly increased the risk of SI by .325 z-score units above the SI threshold through the effects of depressive symptoms. The positive association between Non-Acceptance and depression indicated that, independent of ADHD, depressive symptoms increased as problems accepting negative emotions increased.
Emotional Awareness
ADHD interacted with Emotional Awareness to indirectly affect SI (see Table 2), indicated by bootstrapped confidence intervals not including zero. Evaluating the simple slopes (see Table 4) indicated that participants with ADHD and fewer problems being aware of negative emotions (i.e., low Emotional Awareness deficits) had the highest depressive symptoms; but, for participants without ADHD, problems with emotional awareness (i.e., high Emotional Awareness deficits) were associated with increased depressive symptoms (see Figure 2). For participants with ADHD, each unit increase in Emotion Awareness indirectly increased the risk for SI by .183 z-score units above the threshold for SI (probit B = 1.148).
Emotional Awareness demonstrated significant and positive indirect and direct effects on SI and a significant and positive association with depressive symptoms independent of ADHD. The main effect of Emotional Awareness indicated that depressive symptoms increased when difficulty being aware of negative emotions increased, which indirectly increased risk for SI by .128 z-score units above the SI threshold of 1.148. Similarly, increases in Emotional Awareness directly corresponded to a .175 z-score unit increase above the SI threshold.
Goal-Directed Behavior
ADHD interacted with Goal-Directed Behavior to indirectly and directly affect SI (see Tables 2 and 3). The interaction was significantly associated with increasing depressive symptoms, which significantly increased the risk of SI (see Table 3). For participants with ADHD, difficulty being goal-oriented when distressed (i.e., higher Goal-Directed Behavior deficits) was associated with increased depressive symptoms, which indirectly increased risk for SI by .521 z-score units above the SI threshold (probit B = 1.58; see Table 4 and Figure 2). However, the direct effect of the interaction had the opposite effect. When ADHD was not present, fewer problems with being goal-oriented when distressed (i.e., low Goal-Directed Behavior deficits) was associated with risk for SI (see Figure 3). That is, problems engaging in goal-directed behavior for those without ADHD directly decreased risk for SI by .140 z-score units below the SI threshold.

Interaction of lack of Goal-Directed Behavior and ADHD predicting suicidal ideation.
The indirect effect of Goal-Directed Behavior on SI independent of ADHD was also positive, but the direct effect was negative. Depressive symptoms increased as difficulty engaging in goal-directed behavior increased, which led to increased SI risk, but difficulty with goal-directed behavior decreased SI risk by .162 z-score units below the SI threshold.
Emotional clarity
Only the indirect and total effects of Emotional Clarity on SI were positive and significant (see Table 2). As problems with Emotional Clarity increased, depressive symptoms increased. Thus, Emotional Clarity indirectly increased risk for SI .313 z-score units above the SI threshold (probit B = 1.173).
Strategies
The indirect and total effects of Strategies on SI were significant (Table 2). As problems creating strategies to cope with distress increased, depressive symptoms increased. As a result, Strategies increased SI risk .465 z-score units above the SI threshold (probit B = 1.168).
Emotional impulsiveness
Only the indirect and total effects of Emotional Impulsiveness on SI were significant (see Table 2). As problems being impulsive when distressed increased, depressive symptoms increased. Thus, Emotional Impulsiveness indirectly increased risk for SI .465 z-score units above the SI threshold (probit B = 1.159).
Effect size
According to MacKinnon (2008), the proportion mediated indicates how the size of the indirect effect compares to the total effect and is calculated by dividing the indirect effect by the total effect. Given that the proportion mediated is not necessarily bounded by zero, caution is suggested in interpreting it as a strict proportion ranging from 0 to 1.0 (Preacher & Kelley, 2011). The proportion that depressive symptoms mediated of the association between ADHD and SI ranged from .154 to .491 (M = .332, SD = .101) across models. These results indicate that on average depressive symptoms mediated approximately 33.2% of the variance in the total effect of ADHD on risk for SI. Depressive symptoms mediated 76.9% of the association between Non-Acceptance and SI, 42.4% of the association between Emotional Awareness and SI, 65.1% of the association between Emotional Clarity and SI, 90.1% of the association between Strategies and SI, and 75.4% of the association between Emotional Impulsiveness and SI. Given the negative direct effects and positive indirect effect, it was not possible to calculate the proportion mediated for Goal-Directed Behavior. Standardized regression coefficients can also serve as effect sizes for path coefficients and indicate change in the outcome variable for every one standard deviation change in the predictor (MacKinnon, 2008; see Tables 2 and 3).
Additional analyses
To evaluate the assumption of mediation that the mediator is not better characterized as a moderator (VanderWeele & Vansteelandt, 2010), we analyzed alternate models that included the interaction of ER and depressive symptoms as well as ADHD and depressive symptoms for each ER subscale. Depressive symptoms did not function as a significant moderator of the link between ADHD and SI or any of the ER subscales and SI. Thus, we reported models without the interaction between independent variables and the mediator.
Discussion
The goals of this study were twofold. First, we evaluated the mediating role of depressive symptoms in the association between ADHD and SI. Second, we identified the degree to which ER moderated the association between ADHD and depressive symptoms as well as the direct and indirect effect of ADHD on SI. A unique contribution of this study is its evaluation of the role of both depression and ER in the association between ADHD and SI. ADHD diagnosis has been associated with suicide attempts (e.g., Chronis-Tuscano et al., 2010) and to a lesser extent, SI (Barkley & Fischer, 2005). Our findings suggest that depressive symptoms may be a possible mechanism for the association between ADHD and SI. Although SI is a Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) criterion for MDD, and depression increases the risk for SI (Nock et al., 2013), many individuals who think about suicide do not endorse depressive symptoms (Borges et al., 2010), and are not depressed at the time of their death by suicide (Arsenault-Lapierre, Kim, & Turecki, 2004). Thus, results suggest that depression in the context of ADHD may place individuals at particularly high risk for SI. Further work can evaluate whether findings extend to suicide attempts, death, and non-suicidal self-injury for those with ADHD.
Deficits in ER were directly related to change in SI, indirectly increased risk for SI through depressive symptoms, and moderated the indirect effect of ADHD on SI through depressive symptoms. Taken together, findings highlight the unique function of ER in ADHD, depression, and suicide risk. Because ER strategies can be learned, findings draw attention to potential avenues and modifiable risk factors for intervention.
One of the most surprising findings was the moderating role of goal-directed behavior in ADHD, depression, and SI. For individuals with ADHD, difficulty engaging in goal-directed behavior when distressed was associated with increased depression, which was then associated with increased SI. It is possible that difficulties engaging in goal-directed behavior can lead to increased frustration and/or negative self-cognitions, which are then associated with depressive symptoms (Mitchell, Benson, Knouse, Kimbrel, & Anastopolous, 2013). However, goal-oriented behavior moderated the direct effect of ADHD on SI, indicating that when those with ADHD experience more difficulty with goal-directed behavior, risk for SI decreases. Together, these findings suggest that in the context of depressive symptoms, difficulty with goal-directed behavior may increase SI risk. However, independent of depressive symptoms, problems with goal-directed behavior may be protective for individuals with ADHD in the context of SI. In general, individuals with ADHD have difficulty persisting with tasks when upset (Walcott & Landau, 2004), which has negative outcomes for schoolwork and coping strategies. However, struggling to persist when upset could be protective for SI, above and beyond the influence of depression on SI.
ADHD also interacted with awareness of emotions. For individuals without ADHD, difficulty with emotional awareness was associated with increased depressive symptoms and SI. For those with ADHD, difficulty with emotional awareness was associated with decreased depressive symptoms and SI, suggesting that increased emotional awareness was positively associated with depression and SI. Research on children, adolescents, and adults with ADHD has described the positive illusory bias, in which individuals with ADHD tend to over-report their competency, even in the presence of contradictory evidence (Owens, & Hoza, 2003, Prevatt, Proctor, Best, Baker, & Taylor, 2012). One possible function of the positive illusory bias is self-protection from negative emotions associated with failure (Hoza et al., 2010), which may be reduced in individuals with co-morbid depression (Owens & Hoza, 2003). Lack of awareness of negative emotions may have served a similar purpose to the positive illusory bias in this sample and may be protective for depressive symptoms, decreasing SI. Further investigation with young adults with ADHD is warranted. In addition, clinicians working to increase emotional awareness in patients with ADHD may benefit from carefully monitoring depressive symptoms and SI.
Non-acceptance of negative emotions targets frustration, guilt, and shame associated with experiencing intense negative emotions. Results indicated that those with ADHD and high non-acceptance of negative emotions had higher levels of depressive symptoms, leading to increased SI. Although difficulty accepting emotions has been associated with alexithymia—deficits in identifying and expressing emotional experience—in adults with ADHD (Edel et al., 2010), little research has linked non-acceptance of negative emotions to ADHD. While further investigation is needed, interventions that incorporate a non-judgmental stance on emotions or mindfulness (i.e., Acceptance and Commitment Therapy or DBT; Hayes, Luoma, Bond, Masuda, & Lillis, 2006; Linehan, 1993) may be effective with individuals with both ADHD and depression.
Emotional impulsivity, separate from ADHD diagnostic criteria, has been proposed as an important variable in the symptom persistence and impairment associated with ADHD (Barkley & Fischer, 2010). Although we found a main effect of emotional impulsiveness on depressive symptoms and SI, it did not function as a moderator. Instead, trait impulsiveness may impact depression and SI for those with ADHD rather than impulsiveness specific to emotional distress.
Problems with emotional coping strategies and emotional clarity did not interact with ADHD to predict depressive symptoms or SI, although they were independently associated with increases in both. Although these results underscore the importance of teaching coping skills and psycho-education around emotions in the treatment of depression, these deficits do not appear more problematic for those with ADHD than those without ADHD.
Limitations
Results are tempered by study limitations. Our sample was cross-sectional, which limits the evaluation of directional associations (MacKinnon, 2008; Maxwell & Cole, 2007). Very limited research has evaluated the role of ER deficits in the association between ADHD and depression, and no research has evaluated its role in the link between ADHD and SI. Thus, cross-sectional analyses provide an opportunity to consider a potentially important explanation for SI and its association with ADHD. However, this study should be replicated with longitudinal data to clarify the implied causal associations. Also, assessing a wider array of suicidal behavior and using methods that expand beyond self-report would clarify findings. Although multi-informant assessment is preferred, evidence suggests that self-report provides valid and reliable assessment of ADHD, depression, and suicidal behavior (Barkley et al., 2008; Kooij et al., 2008).
Summary and Conclusion
In sum, results indicated that specific ER deficits moderated the link between ADHD and depression and the indirect effect of ADHD on SI through depression. Findings suggest that individuals with ADHD may benefit from treatment that includes building effective ER competencies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.