
Abstract
Introduction
ADHD in adults is a complex condition which sparks particular interest in different medical, social, academic, cultural, and economic areas given its impact during patient’s life (Gibbins & Weiss, 2007; Klein et al., 2012; Kooij et al., 2010; Laufkötter, Eichhammer, & Hajak, 2004; Matheson et al., 2013; Waite, 2010). Quality of life in these patients is affected by the impact of this condition on family, education, and employment, as well as a higher rate of accidents and forensic or criminal issues (Goksøyr & Nøttestad, 2008; Ramos-Quiroga et al., 2006; Weiss, Hetchman, Milroy, & Perlman, 2003). The negative impact of ADHD on quality of life and functioning persists into middle to late adulthood (Das, Cherbuin, Butterworth, Anstey, & Easteal, 2012; Gjervan, Torgersen, Nordahl, & Rasmussen, 2012; Lensing, Zeiner, Sandvik, & Opjordsmoen, 2015). Moreover, the burden of illness is similarly relevant across several Western countries (Brod, Pohlman, Lasser, & Hodgkins, 2012). All these factors mean that ADHD in adult patients results in a high costs to economy and health (Bernfort, Nordfeldt, & Persson, 2008; Hodgkins, Montejano, Sasané, & Huse, 2011; Kessler et al., 2005, Kessler, Lane, Stang, & Van Brunt, 2009).
Although some adults with ADHD were diagnosed during childhood, for many others, the condition may not be detected until adulthood (Gibbins & Weiss, 2007), and this delay in diagnosis and access to treatment is thought to worsen the outcomes. According to available studies, it is known that only 25% of adults referred with possible ADHD were diagnosed during childhood or adolescence (Faraone, Spencer, Montano, & Biederman, 2004). In this regard, there is a high genetic factor involved in ADHD, and its heritability has been estimated to be around 0.76 (Faraone, Perlis, et al., 2005). In fact, some adults with ADHD are referred for the first time after their children has been diagnosed with ADHD (Harvey, Danforth, McKee, Ulaszek, & Friedman, 2003). Therefore, ADHD may currently be considered an underdiagnosed and undertreated disorder in adults (Aragonès, Cañisá, Caballero, & Piñol-Moreso, 2013; Faraone et al., 2004; Rostain & Ramsay, 2006). For instance, the results of the National Comorbidity Survey Replication (NCS-R) showed that only 11% of cases of ADHD in adults were treated (Kessler et al., 2006).
One of the main reasons for this underdiagnosis in adults may be the high rate of psychiatric comorbidity associated with the condition, which may mask the main symptoms (Kooij et al., 2012). An estimated 70% to 75% of adults with ADHD present at least one concomitant psychiatric diagnosis (Biederman et al., 1993; Cumyn, French, & Hechtman, 2009; Kooij et al., 2010; Sobanski et al., 2007). Furthermore, patients with ADHD present a poorer prognosis for the comorbidity (Diler et al., 2007; Klassen, Katzman, & Chokka, 2010). According to the literature, the most common comorbidities are anxiety disorders, mood disorders, and substance use disorders (SUDs), with a highly variable percentage of comorbidity ranging between 15% and 45% (Biederman et al., 1993; Kessler et al., 2006; Park et al., 2011).
The prevalence of ADHD in the adult general population has been estimated at around 2.5% to 3.4% (Fayyad et al., 2007; Simon, Czobor, Bálint, Mészáros, & Bitter, 2009). While a number of different studies on the prevalence and incidence of ADHD in adults exist in different countries (de Zwaan et al., 2012; McCarthy et al., 2012; Montejano et al., 2012) and information on ADHD adult patients in primary care in Catalonia has been collected (Aragonès et al., 2013; Aragonès et al., 2010), as yet no nationwide study has been completed in Spain. Similarly, despite the frequency of psychiatric comorbidity in adults with ADHD, and the fact that it is usually the initial reason for referral, few studies have focused on this issue. As far as we know, no multicenter studies on the prevalence and the nature of psychiatric comorbidity in adult ADHD have been performed. For this reason, the aim of this study was to establish the prevalence, nature, and number of and risk factors associated with psychiatric comorbidities in ADHD patients diagnosed for the first time in adulthood.
Method
The CAT (Comorbilidad en Adultos con TDAH) study was designed as an observational, cross-sectional, multicenter patient register. The study was approved by the Ethics Committee at the Clínic I Provincial Hospital in Barcelona (2011/6367) and classified by the Spanish Medicines Agency as an observational non-postauthorization study. All participants agreed to be included in the study and signed an informed consent document.
The participating sites were National Health Services, mental health centers or Outpatient clinics (OC), and private practices interested in the study. The project was publicized through the retail network of the sponsor pharmaceutical company, JUSTE S.A.Q.F.
The patients included were those receiving a first time diagnosis of ADHD, as per Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) criteria. Patients were consecutively recruited from those attending appointments at the sites, between April and November 2011. The inclusion criteria were as follows: patients above 18 receiving a first diagnosis of ADHD who provided a minimum set of data: date of first ADHD diagnosis, date of birth, and gender. No exclusion criteria were established. We did not consider lifelong comorbidity because detailed psychiatric history during childhood was not available in all cases, and we aimed to avoid overweighting the prevalence rate of comorbidities.
The patient data were taken from their medical records and included on a restricted-access electronic database. To calculate the proportion of new cases of ADHD in adults attending appointments involved in the study, we used the register of the number of patients treated during the study period and the start and finish dates for patient inclusion.
Clinical records included data regarding psychiatric comorbidities, together with those present at the time the diagnosis was made. Demographic and social information was recorded, including birth date, sex, marital status, family composition, educational and employment status, and employment skills and economic level. Moreover, history of tobacco, alcohol and substance use, family history of psychiatric conditions, and personal history of self-injury were also recorded. Treatments were classified in three groups: medications for ADHD, medications for psychiatric comorbidities, and nonpharmacological treatments.
The study did not require specific pharmacological treatments; the patients selected for the study received treatment and/or medical care as deemed necessary by their doctors, for example, under naturalistic conditions.
No formal calculation of sample size was completed. We summarize qualitative variables by using a frequency distribution. Data were expressed through mean and confidence intervals of 95%—For categorical variables, the exact Fisher test or the chi-square test (χ2) was used. For quantitative variables, the Student’s t test and single factor analyses of variance were used, with Bonferroni or Games–Howell corrections. The statistically significant criterion was established at p < .05. For all the statistical analysis, the SPSS program was used (Version 14.0, SPSS Inc., Chicago, IL, USA).
Results
Seventy-six researchers took part in the CAT study. Of them, 14 (18.4%) enrolled patients from outpatient clinics at hospitals, 44 (57.9%) from mental health centers, and 18 (23.7%) from private practices. The participating sites enrolled a mean of 6 patients (range = 2-11).
Description of the Sample
Of the total number of patients included in the study (n = 416), 49 cases were excluded, as the diagnosis of ADHD was made prior to the start of the study. The final sample size was therefore 367 patients. The data collected showed a proportion of 12.8% of adult ADHD for every 100 patients attending practice. The greatest percentage of ADHD diagnoses were found in hospitals (25.7%, 95% confidence interval [95% CI] = [3.3, 48.2]) although there were no statistically significant differences with the other sites (SC: 9.5%, 95% CI = [3.5, 15.5]; P: 12.6%, 95% CI = [0.7, 24.6]). The study involved a predominantly male sample (n = 265; 72.6%). The mean age at the time of diagnosis was 32.7 (95% CI = [31.6, 33.8]) with a median of 31.8 years (18-65). No differences in age by gender or ADHD subtype were observed.
The most common ADHD subtype was the combined (ADHD-C; n = 152, 42.1%), followed by the hyperactive-impulsive (ADHD-H; n = 112; 31%) and the inattentive (ADHD-I; n = 97; 26.9%) subtypes. No specific subtype could be established at the time the diagnosis in 6 cases (1.6%). Compared with men, women presented predominantly ADHD-I (38% vs. 2.8%, respectively, p = .014). There were no differences in the gender ratios of the other two subtypes (Table 1).
Sociodemographic Description of the Sample According to ADHD Subtypes (n = 367 Patients).
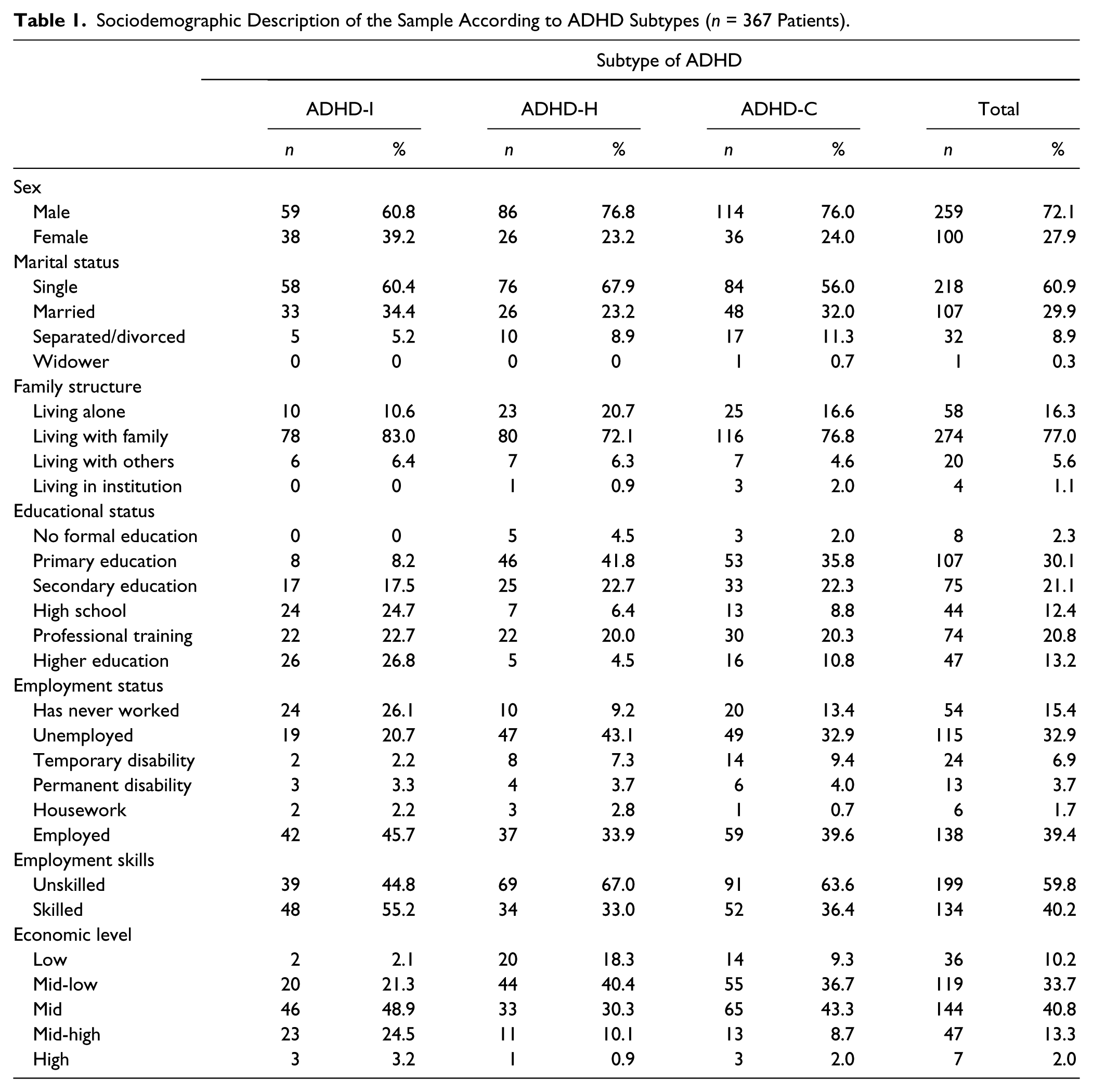
Primary education was the academic level reached by most of the patients with ADHD-C and ADHD-H, versus ADHD-I (p < .001). A greater proportion of patients with ADHD-I tended to complete secondary and higher education than patients with the other two subtypes of ADHD (p < .0001). A higher proportion of patients with ADHD-I had never worked (p = .004), compared with the other two subtypes. A greater proportion of patients with ADHD-H were unemployed compared with those with ADHD-I (p < .05).
Patients with ADHD-I were better qualified for employment (p = .004) than patients with the other two subtypes. Low and mid-low economic levels were less common in patients with ADHD-I versus the other two subtypes (p < .0001); whereas mid level was more frequent in ADHD-H (p < .0001), mid-high level was more common among patients with the other two subtypes of ADHD (p < .0001) (Table 1).
Prevalence of Psychiatric Comorbidity at the Time of Diagnosis
The type of psychiatric disorder diagnosed prior to the first appointment was recorded, together with the date of detection. Most patients (n = 243; 66.2%) had at least one comorbid psychiatric condition. The frequency of psychiatric comorbidity was similarly distributed by gender (65.7% males vs. 67% females). The group of patients with ADHD-C presented psychiatric comorbidity at the time of diagnosis (72.4%) in a greater proportion (p = .006) than patients with ADHD-I (53.6%), with no difference versus patients with ADHD-H (69.6%).
Number of Psychiatric Comorbidities at the Time of Diagnosis
The study sample presented an average of 2.4 comorbidities (95% CI = [2.2, 2.5]) with a median of two comorbidities (ranging from 1 to 8). In the subsample of patients with psychiatric comorbidities, the mean number of comorbidities was significantly greater in males, 2.5 comorbidities (95% CI = [2.28, 2.7]), versus females, 2.0 (95% CI = [1.67, 2.33]); p = .014, as well as in patients with ADHD-H (2.4, 95% CI = [2.1, 2.8]; p = .021) and ADHD-C (2.6, 95% CI = [2.3, 2]; p < .001) versus patients with ADHD-I (1.8, 95% CI = [1.6, 2.1]; Figure 1).
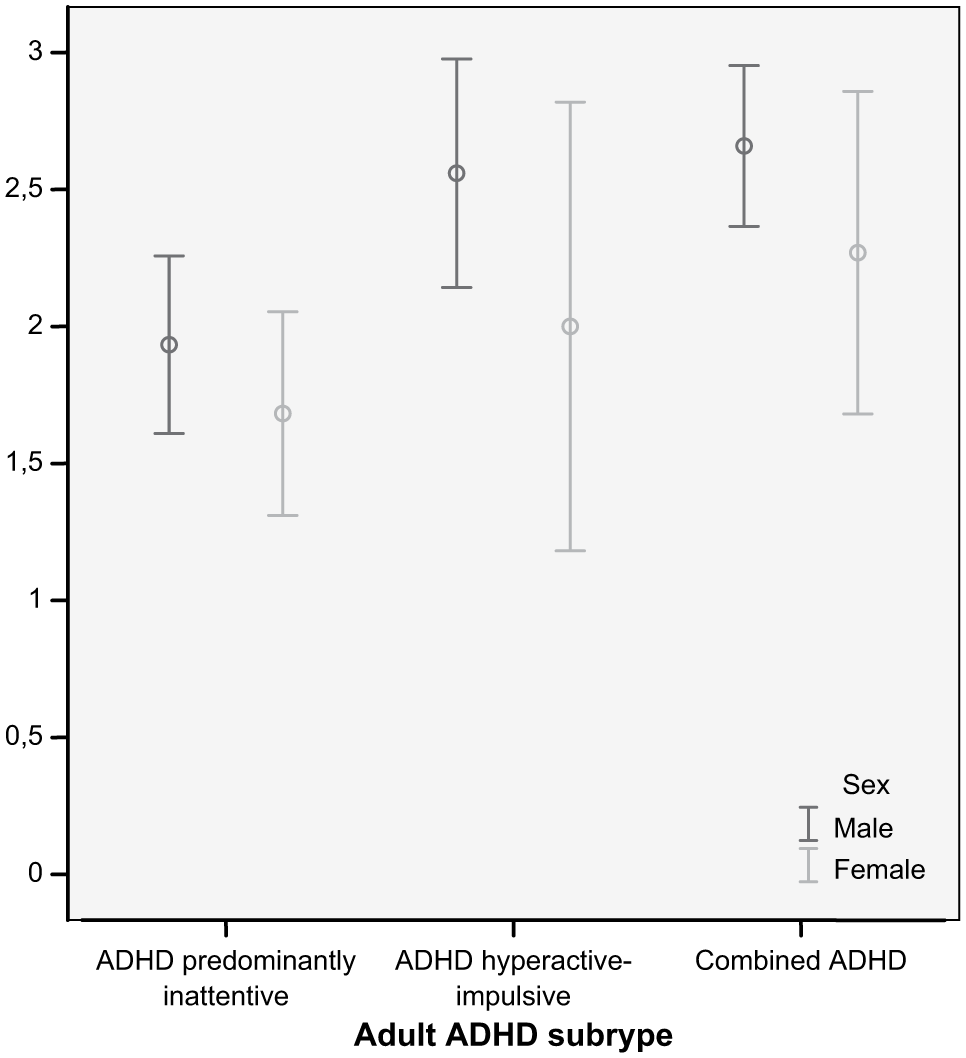
Number of comorbidities at the
Type of Psychiatric Comorbidities at the Time of Diagnosis
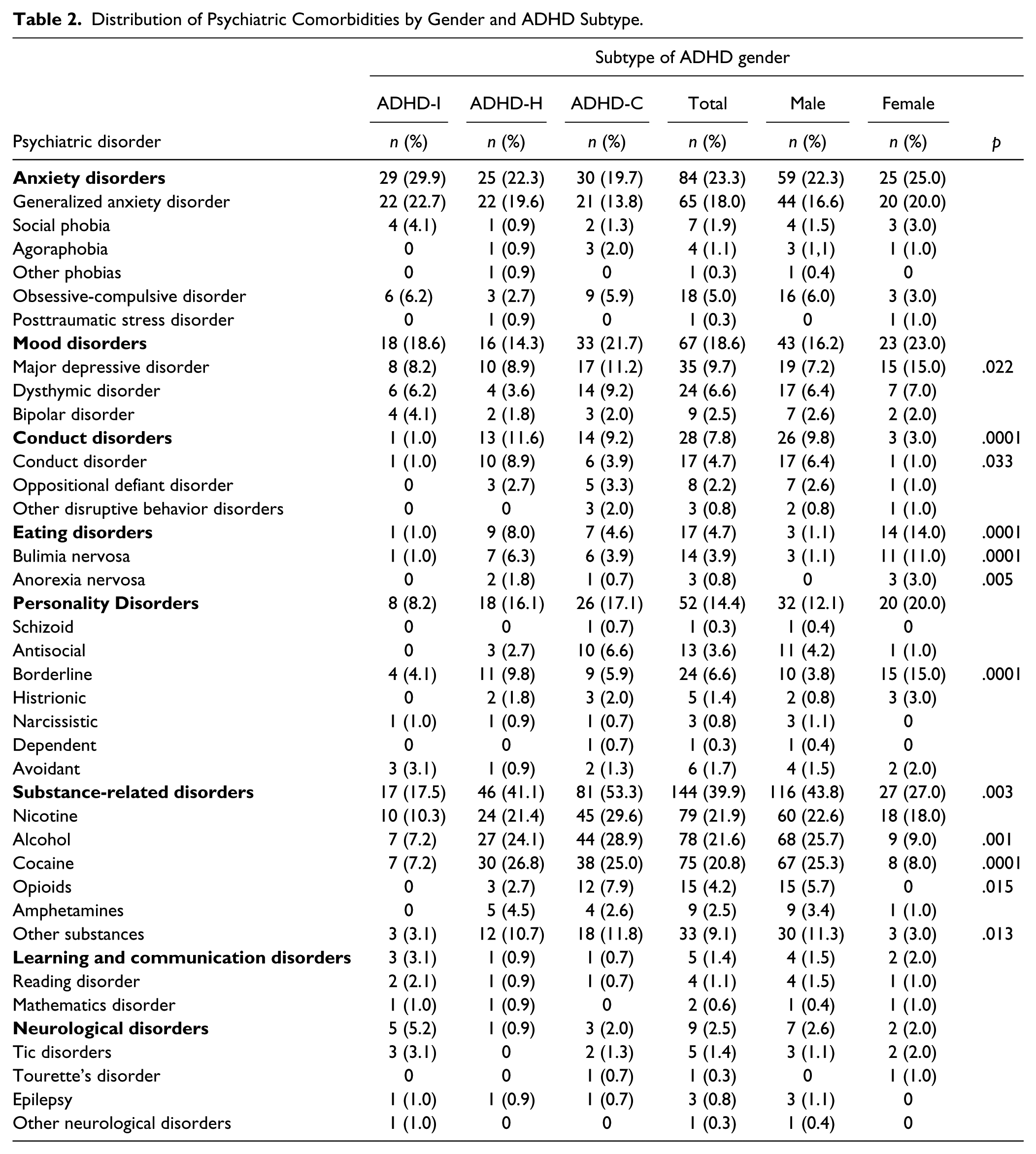
The presence of antisocial personality disorder was significantly more common in patients with ADHD-H in comparison with patients with ADHD-I (p = .023). SUDs, including nicotine, alcohol, cocaine, and others, were significantly more common in the ADHD-C compared with the other two ADHD subtypes (p < .05). Grouped by types of psychiatric disorders, it was observed that both conduct disorders (p = .012) and SUDs (p < .0001) were significantly more common in patients with ADHD-H and ADHD-C compared with patients with ADHD-I (Figure 2, Table 2).

Type of associated psychiatric illness at the time of diagnosis of ADHD in adult patients.
Distribution of Psychiatric Comorbidities by Gender and ADHD Subtype.
Comparison of Patients With and Without Psychiatric Comorbidity
The subsample with psychiatric comorbidities lived with family members (73.3% vs. 83.6%; p < .05) and had education levels up to the end of high school (9.2% vs. 17.9%; p < .05) less often than those without comorbidities.
The proportion of patients who had never worked was greater among those without psychiatric comorbidity (26.9% vs. 11%; p < .05). Temporary and permanent incapacity to work and a lower socioeconomic level were more common among patients with psychiatric comorbidity (8.9% vs. 2.5% and 5.1% vs. 0.8%, 13.1% vs. 5.7%, respectively; all p < .05). Current or past consumption of alcohol (21.9% vs. 12.5%, and 28.3% vs. 12.5%, p < .05) or substances (36.7% vs. 22% and 20.4% vs. 10.6%, p < .05) was significantly more common among patients with psychiatric comorbidity at the time of diagnosis. Current tobacco use was also more common among patients with a history of comorbidity (69.5% vs. 52.8%, p < .05).
History of Family Psychiatric Conditions and Self-Injury
On the other hand, 202 patients (56.6%) had a history of psychiatric illness among their first-degree relatives, with no significant gender differences, and 96 (26.9%) presented a first-degree family history of ADHD. Males had a greater proportion of family history of ADHD (29.8% vs. 19.4% females; p = .047). The rate of patients with family history of either psychiatric illness or ADHD did not significantly differ between the three ADHD subtypes. A subset (n = 38; 10.7%) of patients had shown prior suicidal attempts, with no gender differences (p = .062). Statistically significant differences were observed (p = .001) in the proportion of patients presenting suicide attempts, this being greater in patients with ADHD-H (n = 20; 18.3%) compared with 14 cases (9.7%) in the ADHD-C group.
Treatments
Regarding treatment, 50.4% (n = 185) of patients received treatment with behavioral therapy and/or psychological support, add-on to pharmacological treatment in all cases. Moreover, 358 patients (97.6%) received pharmacological treatments and 12.5% also received treatments for comorbid conditions. Most patients (n = 326; 88.8%) were receiving pharmacological treatment for ADHD, and most (n = 294; 90.2%) received just one medication. The most commonly prescribed drug for the treatment of ADHD was modified release methylphenidate capsules (n = 342; 93.4%), followed by atomoxetine (n = 12; 3.3%) and bupropion (n = 5; 1.4%). A total of 151 patients (41.1%) were receiving pharmacological treatment for psychiatric comorbidities. On average, 1.8 drugs (95% CI = [1.6, 1.9])—between 1 and 7 different ones—were administered.
Discussion
The main aim of the CAT study was to assess the frequency and type of psychiatric comorbidities observed in adults receiving a de novo diagnosis of ADHD. The percentage observed (66.2%) indicates a high proportion of concomitant psychiatric conditions, in line with the majority of data available in the literature (Biederman et al., 1993; Biederman, Newcorn, & Sprich, 1991; Kessler et al., 2006; Kooij et al., 2010; Sobanski et al., 2007) although lower than that observed in other studies (McGough et al., 2005).
The types of comorbidities observed, led by SUDs (39.2%) and followed by anxiety disorders (23%), mood disorders (18.1%), and personality disorders (14.2%), also converges with previous findings (Barkley & Brown, 2008). A possible explanation for the high rate of comorbid SUD may be the patients’ use of alcohol/substances as a means to relieve the symptoms of ADHD, that is, the self-medication hypothesis (Ohlmeier et al., 2007). However, causal inferences are precluded by the cross-sectional design of this study.
The prevalence of anxiety disorder and mood disorder in the CAT study is lower than that found previously, for instance 30% to 50% of anxiety disorder (Adler & Cohen, 2004) and 30% of mood disorder (Biederman, Faraone, Monuteaux, Bober, & Cadogen, 2004). The same holds true regarding comorbid major depressive disorder, which was observed in 9.7% of our sample, versus 18.6% (Kessler et al., 2006) or even 40.7% (Biederman et al., 2008). These differences might be explained by our study only considering comorbid disorders at the time the diagnosis of ADHD was made, whereas others involved lifelong comorbidity. The frequency of comorbidity with bipolar disorder (2.5%) was also lower than 10% to 14% reported in some (Biederman et al., 1994; Tamam, Karakus, & Ozpoyraz, 2008), but similar to other (Jaideep, Reddy, & Srinath, 2006) studies. Comorbidity with antisocial personality disorder in our study was 3.6%, slightly lower than that previously observed (Mannuzza & Klein, 2000). Borderline personality disorder, observed primarily in women (15%) presented a similar level of frequency to that found by other authors (14% in Fischer, Barkley, Smallish, & Fletcher, 2002). Collectively, the different methodologies used may explain the lower prevalence of the majority of common comorbidities in ours versus other studies; thus our study did not take into consideration childhood-related comorbidities such as oppositional defiant disorder (ODD) or conduct disorder. Furthermore, it only considers the conditions observed at the time of diagnosis and not during the course of their illness.
As regards the comparison of ADHD subtypes, in consonance with other works, the frequency of psychiatric comorbidity was greater in ADHD-C and ADHD-H compared with ADHD-I, which may suggest greater disability and poorer functioning, quality of life, and prognosis (Barkley & Brown, 2008). Further supporting this data, history of suicide attempts was more common in ADHD-H than in ADHD-I. Our findings are also consistent with other studies reporting a tendency toward self-harm in ADHD patients (James, Lai, & Dahl, 2004).
In line with published data (Biederman et al., 2006), a greater prevalence of the condition was observed in men than in women, with a ratio of 2.7:1. Disproportioned gender ratios of 6:1 to 3:1 usually observed during childhood (Goodyear & Hynd, 1992; Taylor, Sandberg, Thorley, & Giles, 1991) virtually disappear in adulthood. As indicated by other authors, this is probably due to a bias in the assessment of symptoms according to gender, as girls more commonly present with ADHD-I which results in less disruptive behavior and means that the disorder is more easily left undetected and undiagnosed (Biederman et al., 2004; Quinn et al., 2008). Consistently, a significantly greater percentage of women than men in the ADHD-I group was found in our study. Since ADHD-I was associated with the lowest rate of comorbidities, it is likely that women with ADHD-I present less often to mental health services. Consequently, this may favor professionals’ impression that adult ADHD is far less prevalent among women.
Although the percentage of patients with comorbidity did not differ by gender, a higher number of comorbidities was observed in men compared with women, perhaps related to the predominant type of ADHD in each gender group. Moreover, the pattern of comorbidities observed by gender was different. Major depressive disorder was twice as common in women, and eating disorders were up to 13 times more common. Borderline personality disorder was also 4 times more common in women, similar to previous reports (Fischer et al., 2002; Sprafkin, Gadow, Weiss, Schneider, & Nolan, 2007). As expected, antisocial personality disorder was more common in men than in women (6.2% vs. 1%) although with lower percentages than in other studies (Biederman et al., 2004, 24% vs. 14%).
Overall, the distribution of comorbidities by gender in the CAT study concurs with those of previous studies, which also found that women with ADHD are more likely to present with comorbid eating and mood disorders, while men with ADHD are more prone to present with comorbid SUDs (Cumyn et al., 2009; Sobanski et al., 2007).
In our study, the proportion of patients with a de novo diagnosis was 12.8%, which is much higher than the prevalence in the adult general population (Faraone & Biederman, 2005; Fayyad et al., 2007; Kessler et al., 2006; Simon et al., 2009) but closer to that of studies based on clinical samples (18%, Almeida Montes, Hernández García, & Ricardo-Garcell, 2007; 21.6%, Nylander, Holmqvist, Gustafson, & Gillberg, 2009).
It should be noted that more than half of adult ADHD patients in the CAT study reported to have a positive family psychiatric history, with no difference between the genders, whereas a family history of ADHD was significantly more common in males. Bearing in mind the high level of heritability associated with ADHD (Faraone, Perlis, et al., 2005), professionals working with children and adolescents should consider an assessment of the disorder in their parents as part of integral therapy (Psychogiou, Daley, Thompson, & Sonuga-Barke, 2008) to maximize diagnoses of ADHD in adults.
Half of the adult patients in the CAT study received behavioral therapy and most (88.8%) received medications, primarily with methylphenidate, which was prescribed as monotherapy in 90.2% of the sample. This represents a very homogeneous prescription pattern, which is considerably higher than that obtained in recent studies (11% in Kessler et al., 2009), and may suggest a change in the treatment of adults with ADHD.
Nine psychiatric disease registers exist in Spain, yet none is ADHD specific (Imaz Iglesia, Aibar Remón, González Enríquez, Gol Freixa, & Gómez López, 2005). Until now, only three studies had focused on the prevalence of ADHD in psychiatric outpatient settings worldwide (Almeida et al., 2007; Lomas & Gartside, 1997; Nylander et al., 2009). Two of them were completed in a single mental health clinic, and the remaining study (Lomas & Gartside, 1997) was carried out in a veteran center. This means that the CAT study is the only multicenter, nationwide, ADHD-focused study, including a relatively large sample of psychiatric outpatients.
The limitations of our study include its cross-sectional design, the retrospective review of clinical records and the absence of limits in selection criteria. The participation of most Spanish regions makes it possible to estimate the results at a national level. However, future studies should cover the entire country to that end.
To conclude, the use of patient records for the control and assessment of the prognosis for a condition that, like ADHD, may persist throughout the patient’s lifetime. The high level of psychiatric comorbidity in these patients means that appointments at mental health centers offer an excellent opportunity to diagnose cases of ADHD which would otherwise go undetected, thus negatively affecting patients’ outcomes and quality of life. Given the results of the CAT study, ADHD should be ruled out systematically in all patients attending psychiatric practices to offer improved access to the effective treatments currently available. This seems to be particularly relevant for women with eating and mood disorder and men with SUD.
Footnotes
Authors’ Note
In addition to the authors, the following researchers were members of the CAT Study Group: Moisés Aguilar Domingo; Jose David Albillo Labarra; Pablo Alvarez Lobato; Alejandro Amor Salamanca; Jesús Ayala Bes; Francisco Javier Barón Fernández; Rafael Benito Moraga; Javier Blanco Blanco; Antonio Briones Perona; Tulio Callorda Boniatti; Jose Miguel Cano Gras; Juan Manuel Cantos Martínez; Indalecio Carrera Machado; Mª Cristina Casal Pena; Carlos Castillo Flores; Carlos Castro Dono; Mª Teresa De Lucas Taracena; Begoña De Pablo García; Patricia Fadón Martín; Ernesto Ferrer Gómez Del Valle; Eva Fontova; Facund Fora Eroles; Rafael Forcada Chapa; Ignacio Gainza Tejedor; Araceli Gamez Palomares; Javier García Campayo; Jose Manuel García Moreno; Xavier Gastaminza Pérez; María Del Carmen Gimeno Escrig; Sara González Vives; Elisabet Gorgues Queralt; Alfredo Granell Gonochategui; Alfredo Gurrea Escajedo; Rosario Gutierrez Labrador; Ana Herrero Mendoza; Federico Guillermo Iglesias Lorenzo; Miguel Martín Iribarren; German Jurado De Flores Yepez; Miguel A Lanbadaso Vazquez; Jose Mª Lomba Borrajo; Sonia López Arribas; Jose Manuel Manso García; Antonio Marcos Flores; Daniel Martín Fernández-Mayoralas; Nicolás Martin Navarro; Luis Martín Recuero; Isabel Martínez Gras; Jose Martínez Raga; Pedro A Megia López; Jose Luis Montero Horche; Pablo Luis Moreno Flores; Emma Osejo Diago; Francesco Panicali; Francisco Pascual Pastor; Guillermo Ponce Alfaro; Santiago Posik Rosati; Marta Puig Sanz; Ana Mª Inés Queijero Presa; Carmen Ripoll Alandes; Jose Juan Rodriguez Solano; Juan Ramon Sambola Buguña; Gemma San Narciso Izquierdo; Milagros Sánchez García; Cesar Luis Sanz De La Garza; Olga Sanz Granado; Francesc Segarra Murla; Pedro Seijo Ceballos; Olga Sobrino Cabra; Pedro A Sopelana Rodríguez; Virgilio Traid Sender; Rosario Vacas Moreira; Miguel Angel Villalba Abarquero; Rosa Villanueva Peri; Laura Villar Mateo; Diana Zambrano; Jose Miguel Zoido Ramos.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Pilar García is contracted by the medical department of Juste S.A.Q.F. Begoña Soler completed the design, quality control, and statistical analysis of the study under contract with Juste S.A.Q.F. The remaining authors hereby declare that they have no conflicts of interest affecting the aims and results of the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Juste S.A.Q.F.
Author Biographies
![]() ). He works in acute psychiatric hospitalization in a General Hospital since 2002. He has more than 10 years of experience in diagnostic and treatment of adults with ADHD, and he was director and author of the online workshop “The attention deficit disorder (ADHD). Evolution throughout life and its comorbidities.”
). He works in acute psychiatric hospitalization in a General Hospital since 2002. He has more than 10 years of experience in diagnostic and treatment of adults with ADHD, and he was director and author of the online workshop “The attention deficit disorder (ADHD). Evolution throughout life and its comorbidities.”
![]() ). She founded the company in 1997. She is a senior medical adviser and statistician, with more than 20 years of experience in clinical research in different international companies and several therapeutical areas. Her research is focused in public health. She published 23 articles in journals indexed in PubMed.
). She founded the company in 1997. She is a senior medical adviser and statistician, with more than 20 years of experience in clinical research in different international companies and several therapeutical areas. Her research is focused in public health. She published 23 articles in journals indexed in PubMed.