
Abstract
Keywords
Introduction
Pharmacotherapy, mainly with central stimulant medication, is considered to be the cornerstone of treatment for ADHD across the life span (Elia, Ambrosini, & Rapoport, 1999; Rosler, Casas, Konofal, & Buitelaar, 2010; Swanson et al., 1998). Its efficacy in treating the core symptoms of the disorder (i.e., hyperactivity, impulsivity, and inattention) in younger age groups is well documented (National Institute for Health and Clinical Excellence, 2008; E. Taylor et al., 2004). Research on drug treatment in adults aged 50 years and older with ADHD is sparse (Wilens, Morrison, & Prince, 2011). However, studies in this area are warranted, as the estimated prevalence of ADHD in older adults (2.8%) is in line with results from studies of younger adults with the disorder (Michielsen et al., 2012; Simon, Czobor, Balint, Meszaros, & Bitter, 2009).
Assessing pharmacotherapy in adults aged 50+ with ADHD raises at least two important clinical questions. First, how well does it work for this group of adults, many of whom have lived their lives undiagnosed and untreated for the condition (Asherson et al., 2012; Turgay et al., 2012), and second, can adults aged 50+ tolerate pharmacotherapy?
The benefits of pharmacotherapy beyond addressing the core symptoms of ADHD (e.g., academic performance, acquisition of new information, cognitive plasticity) have been questioned (Advokat, 2010; Barkley & Cunningham, 1978). Follow-up studies of children with ADHD have shown no clear relationship between long-term outcomes and the type of drug used, the treatment modality, or treatment duration (Molina et al., 2009; G. Weiss, Minde, Werry, Douglas, & Nemeth, 1971). However, when treated and untreated samples with ADHD were compared, improved long-term outcomes were reported for those who had been treated (Shaw et al., 2012). Researchers have also suggested that the timing of treatment onset is related to outcomes (Barkley & Cunningham, 1978). For example, research in younger adults with ADHD showed that diagnosis and psychopharmacological treatment in childhood or adolescence were associated with better outcomes than diagnosis and treatment in adulthood (Halmoy, Fasmer, Gillberg, & Haavik, 2009). Besides this, one has to consider that the dopaminergic system is one of the more age-sensitive neurotransmitter systems (Volkow et al., 1996). Age-related decreases in dopamine transporter capacity and dopamine receptor density (and concomitant declines in motor and cognitive functioning) have been reported (Volkow et al., 1996; Volkow et al., 1998). This may be important, as stimulant medication is found to increase intrasynaptic concentrations of dopamine and norepinephrine (Wilens et al., 2011).
The second clinical question about pharmacotherapy for adults aged 50+ with ADHD concerns the side effects of treatment. Increasing cardiovascular problems with age, potentially higher doses of therapeutic drugs needed, and slower drug elimination are some of the concerns that have been raised about using stimulant medications in older adults (Retz, Retz-Junginger, Thome, & Rosler, 2011; M. Weiss, Hechtman, & Weiss, 2001; Westover & Halm, 2012). One recently published study on the use of stimulant medication in adults found that a short median exposure of 0.33 years did not lead to an increased risk of serious cardiovascular events when current use was compared with nonuse (Habel et al., 2011). However, others have reported increased risks for transient ischemic attacks, sudden death, and ventricular arrhythmia among users of stimulant medications (Holick et al., 2009; Schelleman et al., 2012). In a recent systematic review of research on stimulant medications and cardiovascular disease, the authors concluded that the association between use of stimulant medications and cardiovascular disease in adults is still uncertain (Westover & Halm, 2012).
To the best of our knowledge, only one study has examined adults 50 years of age or older with ADHD, an open-label pilot study of 11 adults newly diagnosed with ADHD (Manor, Rozen, Zemishlani, Weizman, & Zalsman, 2011). In that study, subjects were treated mainly with stimulant medication and the follow-up duration was at least 2 months. Treatment outcomes were similar to what has been found with younger adults. The sample was small, however, and the follow-up was short. With an increasing awareness that ADHD can persist into middle age and late adulthood, we studied a comparatively large sample of adults (≥50 years old) with ADHD with the following aims:
To investigate the use and persistence of psychopharmacological treatment for ADHD.
To explore the association between current psychopharmacological treatment for ADHD and ADHD symptoms, life satisfaction, and psychosocial factors.
Material and Method
An anonymous survey of members of the national ADHD patient organization was conducted in 2010. Inclusion criteria for the study were diagnosis with ADHD (based on membership information and confirmed by self-reported year of diagnosis) and age of 50 years or older. According to national recommendations, the assessment and diagnosis of ADHD in adults must be performed by specialists, such as a psychiatrist or clinical psychologist (The Norwegian Directorate of Health, 2007). To secure anonymity, the questionnaire was sent three times to all included subjects. The data protection officer at the Oslo University Hospital approved the study after the Regional Ethic Committee for South-East Norway concluded that this was satisfactory.
Participants
Two hundred fifty-one subjects met the inclusion criteria, and 166 (66.1%) returned the questionnaire. Of these, 17 were excluded (12 because the diagnosis of ADHD could not be confirmed, and 5 because they failed to indicate their age). Thus, the study sample consisted of 149 participants. There were no statistically significant differences between the participants and the eligible sample with respect to gender distribution, age, and place of residence in the country. In five cases (3.4%), information on gender was not available. Eighty-nine participants (59.7%) were female. The mean age for the sample was 55.8 (SD = 4.4) years, and the mean age when ADHD was diagnosed was 50.3 (SD = 5.9) years. Ninety-one participants (61.6%) reported that a child had been diagnosed with ADHD, and 39 (26.2%) reported that a grandchild had been diagnosed with the disorder. Twenty-four participants (26.4%) had a child and a grandchild with ADHD.
Questionnaire
Participants reported whether they were receiving psychopharmacological treatment for ADHD, as well as whether they were receiving other (nonpharmacological) treatments such as psychoeducation or psychotherapy. Those who were currently receiving psychopharmacological treatment were asked to report which compound they were taking, the daily dosage, and who had prescribed the medication (e.g., psychiatrist, family doctor, or others). Participants also provided information about co-occurring medical disorders or injuries and any drugs they were taking for disorders other than ADHD.
Primary Outcome Measures
ADHD core symptoms were defined as the primary outcome. Current ADHD symptoms were measured with the Adult ADHD Self-Report Scale (ASRS V.1.1) screener (Kessler et al., 2005). This instrument consists of four items on inattention and two items on hyperactivity/impulsivity. Symptom frequency was rated on a 5-point scale that ranges from 0 (never) to 4 (very often), and the clinical cutoff score of 14 was applied (A. Taylor, Deb, & Unwin, 2011). In no cases were more than two items missing. The value of missing items was replaced by the mean of the available item values. Cronbach’s alpha for this scale was .80, which is in line with previous findings (Kessler et al., 2007). As recommended by others, we used an equally weighted sum of responses to create an Inattention Trait Score (ITS) and a Hyperactive/Impulsive Trait Score (HTS) to explore the two dimensions of the ASRS screener independently (Das, Cherbuin, Butterworth, Anstey, & Easteal, 2012).
Participants were asked to rate hyperactivity and impulsivity compared with 10 years ago on a 5-point response scale (1 to 5) from much more, somewhat more, unchanged, somewhat less to much less. Attention compared with 10 years ago was also rated on a 5-point response scale (1 to 5) from much worse, somewhat worse, unchanged, somewhat better to much better.
Secondary Outcome Measures
The Satisfaction With Life Scale (SWLS; Diener, Emmons, Larsen, & Griffin, 1985) is a five-item self-report instrument that measures satisfaction with one’s life as a whole. The five items are as follows: “In most ways my life is close to my ideal,” “The conditions of my life are excellent,” “I am satisfied with my life,” “So far I have gotten the important things I want in my life,” and “If I could live my life over, I would change almost nothing.” The original version of this instrument uses a 7-point response scale. We used a 5-point response scale that ranged from 1 (totally disagree) to 5 (totally agree), giving total scores that ranged from 5 (extremely dissatisfied) to 25 (highly satisfied). With the 7-point response scale, a total score of 20 is defined as neutral (Diener, 2012), whereas we set the equivalent score with the 5-point response scale at 15. The internal consistency of this instrument was 0.84 in this study, which is in line with previous findings (Diener et al., 1985).
We assessed current health status with a Euroqol Visual Analogue Scale or “thermometer” scale (EQ-VAS; The EuroQol Group, 1990) and one item from the Short Form Health Survey (SF-36; Ware, Kosinski, & Gandek, 1993/2000). The EQ-VAS is part of the EQ-5D that is a generic, standardized, health-related quality-of-life self-report instrument developed by the EuroQol Group (1990). On the EQ-VAS, subjects indicate their current health condition on a scale from 0 (worst imaginable health state) to 100 (best imaginable health state). On the SF-36 item, subjects are asked to compare their current health status with their status a year ago. The 5-point response scale (1 to 5) ranges from much worse, somewhat worse, unchanged, somewhat better to much better.
Finally, we measured self-efficacy with one item (“I’m able to manage daily demands well”), which has been used in a large survey of life course, aging, and generation (Solem, 2003). The 5-point response scale (1 to 5) ranged from strongly disagree, fairly disagree, neither disagree nor agree, fairly agree to strongly agree.
Statistics
Statistical analyses were performed with the predictive analytic software (PASW) Statistics 18.0 for Windows (IBM, Armonk, New York). Chi-square statistics were calculated to assess pair-wise associations between categorical variables. Associations between binary and continuous variables were analyzed with independent samples t test. One-way ANOVAs with Scheffé post hoc analysis were performed to assess group differences. Binary logistic regression analyses were performed to identify characteristics associated with less symptom severity and better outcomes. To increase the probability to report true findings, a significance level of 1% (p < .01) was used throughout the study.
Results
Characteristics of the study sample, divided into three groups (currently treated with medication for ADHD, stopped treatment with medication for ADHD, and never been treated with medication for ADHD) are presented in Table 1.
Characteristics of 149 Adults Aged 50+ With ADHD Separated by Status of Use of Medication for ADHD.
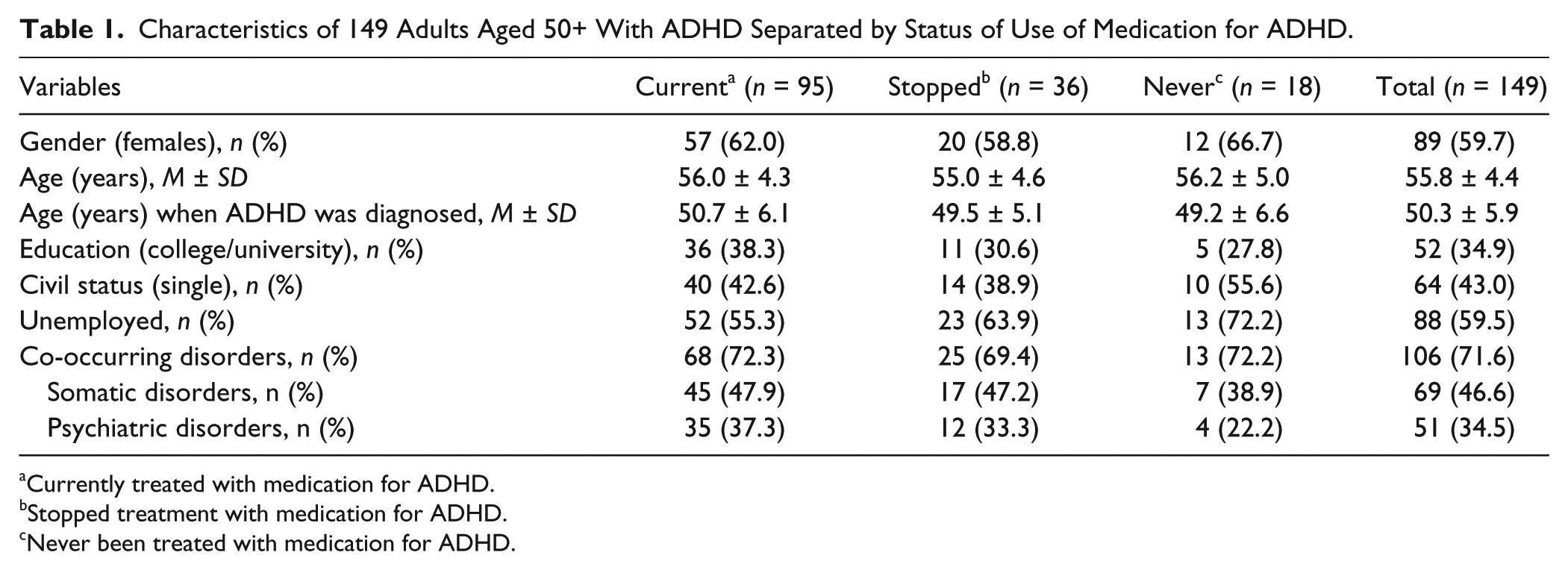
Currently treated with medication for ADHD.
Stopped treatment with medication for ADHD.
Never been treated with medication for ADHD.
One hundred thirty-one participants (87.9%) reported psychopharmacological treatment for ADHD (95 who were currently treated and 36 who had stopped treatment), whereas 18 (12.1%) were not treated with medications. In the currently treated group, 77 (82.0%) reported using compounds containing methylphenidate, 10 (10.5%) were prescribed amphetamine, and 5 (5.3%) were using nonstimulant medications. The self-reported mean daily dosage was 54.1 ± 28.5 mg (range = 8-135 mg) for methylphenidate and 29.5 ± 14.5 mg (range = 4-50 mg) for amphetamine. In 58.9% of the cases, a family doctor prescribed the drugs for ADHD, psychiatrists prescribed the drugs in 35.8% of the cases, and in 5.3% of the cases, there was insufficient information about who prescribed the drugs.
There were no statistically significant differences between sexes or groups for the characteristics listed in Table 1 (age, education, civil status, employment, co-occurring disorders). In the unemployed group, 62 participants (70.5%) were on social security, whereas 7 (8.0%) were retired. Among those with self-reported co-occurring somatic disorders, hypothyroidism (20.6%), hypertension (19.1%), fibromyalgia (16.2%), and arthritis (16.2%) were the most common ones, whereas depression (40.0%), bipolar disorder (24.0%), and anxiety (20.0%) were the most frequently reported co-occurring psychiatric disorders. Twenty-one participants (14.1%) reported co-occurrence of at least one somatic and one psychiatric disorder.
The mean observation time, defined as the period of time from the year when ADHD was diagnosed to the year when the survey was performed, was 5.7 ± 5.5 years (range = 0-30 years). Observation time was not significantly different between groups (currently treated 5.4 ± 5.5 years, stopped treatment 5.7 ± 4.1 years, and never treated 7.0 ± 7.5 years; f = 0.7; df = 2, p = .5).
One hundred fourteen participants (76.5%) reported ongoing drug treatment (e.g., antihypertensives, analgesics, antidepressants, anxiolytics, anticonvulsants, antipsychotics) for co-occurring conditions. Drug treatment for co-occurring disorders did not differ statistically between groups.
Nonpharmacological Treatments for ADHD
For the whole sample, 35.6% of the participants reported receiving nonpharmacological treatments for ADHD. There were no statistically significant differences between the three groups on nonpharmacological treatments for ADHD.
Analyses of Primary and Secondary Outcome Measures
A comparison of primary and secondary outcome measures specified by groups is presented in Table 2. The mean score on the ASRS screener was above the cutoff of 14 in each of the three groups. Fifty-one participants (34.2%) had an ASRS screener score below the cutoff, and 54 (36.2%) had an SWLS score of 15 or above. Those who were currently being treated with medications for ADHD reported better attention (compared with 10 years ago) than the nonmedicated groups. Participants who had never been treated with drugs for ADHD indicated that their current health status was worse than that of participants in the two other groups, but Scheffé post hoc analyses revealed that the differences were not statistically significant. Those who were currently being treated with medications reported that their ability to manage daily demands (i.e., self-efficacy) was better than those who had stopped psychopharmacological treatment for ADHD.
Outcome Measures for 149 Adults Aged 50+ With ADHD Separated by Use of Medication for ADHD, Mean (SD).
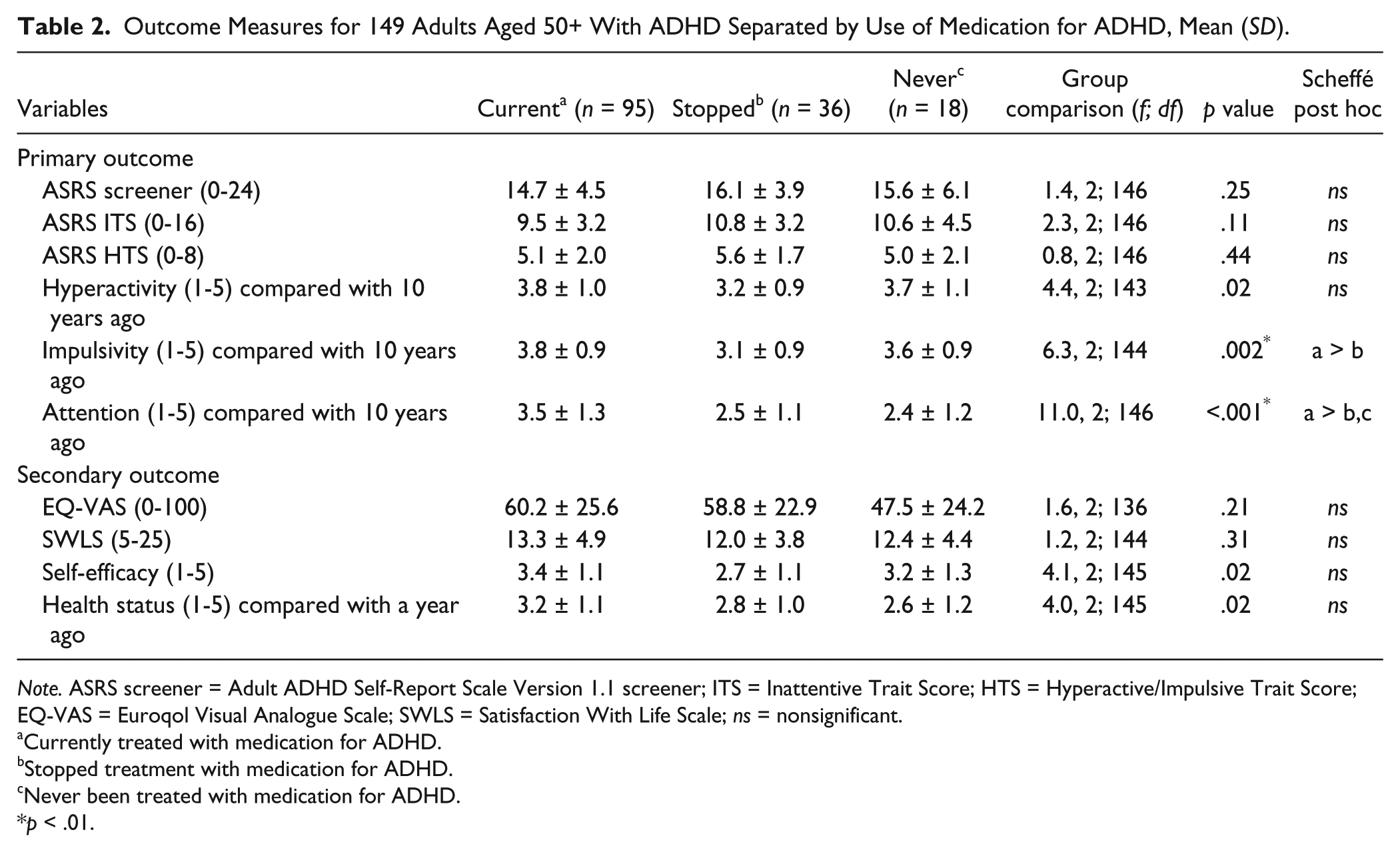
Note. ASRS screener = Adult ADHD Self-Report Scale Version 1.1 screener; ITS = Inattentive Trait Score; HTS = Hyperactive/Impulsive Trait Score; EQ-VAS = Euroqol Visual Analogue Scale; SWLS = Satisfaction With Life Scale; ns = nonsignificant.
Currently treated with medication for ADHD.
Stopped treatment with medication for ADHD.
Never been treated with medication for ADHD.
p < .01.
Favorable Outcome
A combined ASRS screener score below the cutoff of 14 and an SWLS score of 15 or above were defined as favorable outcomes. The comparisons of the favorable outcome group (n = 28) versus all others (n = 119) are presented in Table 3.
Favorable Outcome Group Compared With Others in Adults Aged 50+ With ADHD (n = 147 a ).
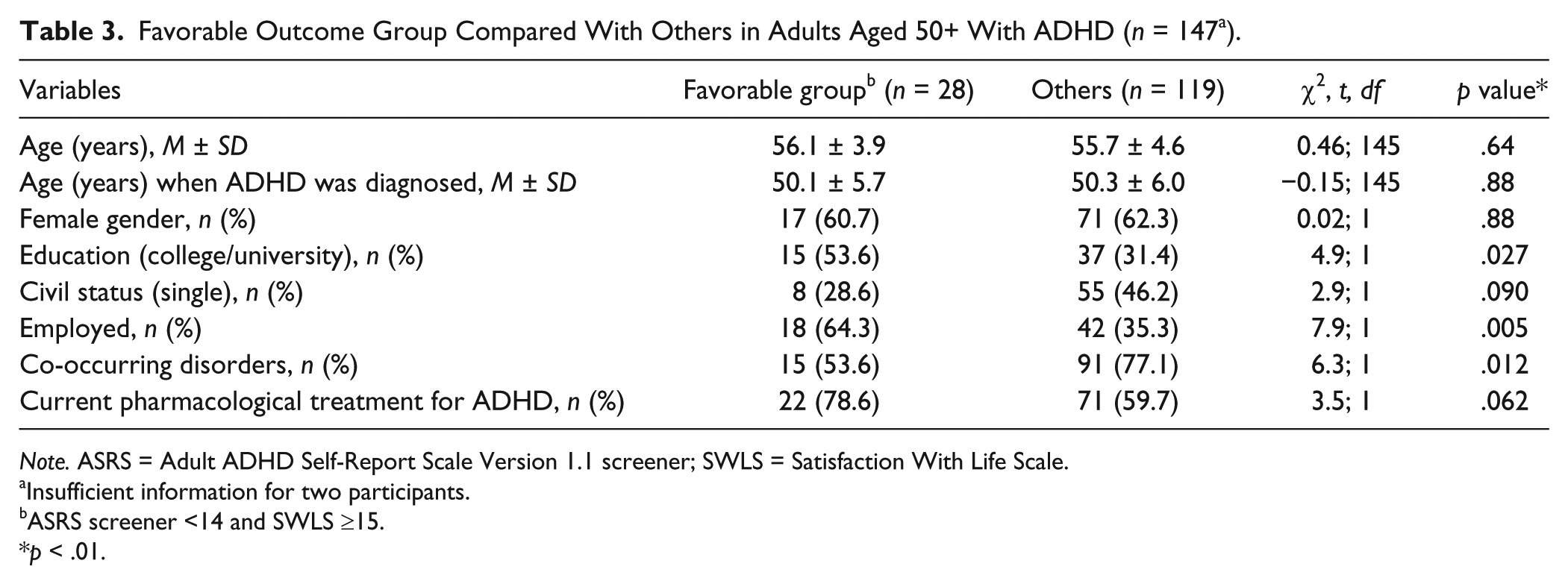
Note. ASRS = Adult ADHD Self-Report Scale Version 1.1 screener; SWLS = Satisfaction With Life Scale.
Insufficient information for two participants.
ASRS screener <14 and SWLS ≥15.
p < .01.
The mean ASRS screener and SWLS scores of the favorable outcome group were 9.1 ± 3.3 and 18.5 ± 2.5, respectively, whereas the corresponding mean scores for the others were 16.5 ± 3.7 and 11.6 ± 3.9, respectively. Observation time did not differ statistically significantly between the favorable outcome group and the rest of the sample (5.8 ± 5.8 years vs. 5.6 ± 5.5 years; t = 0.1, df = 145, p = .9). Furthermore, the three groups did not differ statistically significantly with respect to representation in the favorable outcome group (χ2 = 3.5; df = 2, p = .2). However, current health status (as measured by the EQ-VAS) was significantly better in the favorable outcome group compared with the rest of the sample (76.4 ± 18.0 vs. 54.7 ± 24.5; df = 136, t = 5.2, p < .001).
A stepwise backward binary logistic regression analysis was performed to identify characteristics associated with a better outcome. Outcome (favorable vs. others) was the dependent variable and the characteristics listed in Table 1 plus current pharmacological treatment for ADHD served as independent variables. Favorable outcome was significantly associated with employment only (odds ratio = 3.3; 99% confidence interval [CI] = 1.1, 10.2; p = .006).
Discussion
In this cross-sectional study of adults aged 50+ with ADHD, the majority (88%) had been treated with ADHD drugs, and 64% of the participants were currently receiving psychopharmacological treatment for ADHD. The mean observation time (from ADHD diagnosis to data collection) was more than 5 years. Those who were currently being treated with medication for ADHD reported improved attention compared with 10 years ago, whereas those who stopped taking (or had never had) ADHD medications did not. Employment was the only variable significantly associated with a favorable outcome when other variables were controlled.
With an increasing awareness that ADHD can persist into middle age and late adulthood, one can expect that pharmacotherapy will be considered for more cases in the future. In Norway, immediate-release methylphenidate (Ritalin IR) was approved for the treatment of ADHD in adults in 2000. Consequently, adults with ADHD could be treated with a labeled first-line drug, which has probably contributed to the increased number of adults aged 50+ being diagnosed with and treated for ADHD throughout the country.
Chart review studies (McCarthy et al., 2009; Olfson, Marcus, Zhang, & Wan, 2007; Perwien, Hall, Swensen, & Swindle, 2004) and open-label safety and efficacy studies (Adler et al., 2011; Adler, Spencer, Williams, Moore, & Michelson, 2008; Biederman et al., 2005) indicate that most adults diagnosed with ADHD use their ADHD medication for less than 6 months. Therefore, the high percentage of participants in this study who reported current pharmacological treatment for ADHD is striking. This result is strengthened by the fact that there was no significant difference in observation time (i.e., the period from when ADHD was diagnosed to when the survey was performed) between groups. Several factors may have contributed to this result. The increased use of extended-release formulations of methylphenidate has been found to predict longer treatment duration in adults with ADHD (Torgersen, Gjervan, Nordahl, & Rasmussen, 2012). Furthermore, Nordic welfare systems are characterized by access to equal treatment conditions, the availability of specialists throughout the country, and state payment for necessary medical treatments (Wahlbeck, Westman, Nordentoft, Gissler, & Laursen, 2011).
In our study, the majority of participants were treated with stimulant medication, most often methylphenidate, which is in line with national (The Norwegian Directorate of Health, 2007) and international (National Institute for Health and Clinical Excellence, 2008) guidelines for the treatment of ADHD. The means for the self-reported daily dosages of stimulant medications in this study (e.g., 54.1 mg/day for methylphenidate and 29.5 mg/day for amphetamine) were in line with the above-mentioned recommendations.
Adults with ADHD are found to report higher rates of inattention than hyperactivity/impulsivity. Problems with inattention are often described as difficulties with sustained attention, distractibility, daydreaming, forgetfulness, and sustained mental effort, which could subsequently lead to difficulties with planning, organizing, and finishing tasks in everyday life (Bramham et al., 2012; Wilens et al., 2009). Treatment of adults with ADHD with stimulant medication has been found to reduce symptoms of inattention (Faraone & Glatt, 2010). In our study, participants currently receiving ADHD medications reported significantly better attention (compared with 10 years ago) than those who were not being treated with medications. They also reported better self-efficacy than those who had stopped pharmacological treatment.
We did not find statistically significant differences between groups for hyperactivity and impulsivity compared with 10 years ago. Developmentally, it has been argued that symptoms of hyperactivity and impulsivity decline more rapidly from childhood to adulthood in those with ADHD than symptoms of inattention (Biederman, Mick, & Faraone, 2000; Wilens, Biederman, & Spencer, 2002; Willcutt et al., 2012).
However, in this study, the ASRS screener mean scores for all three groups were above the cutoff of 14, and no statistically significant differences were observed between groups. This is a somewhat surprising result, as it does not comport with a previous report of treatment outcomes on core symptoms being similar to those seen in younger adults with ADHD (Manor et al., 2011). One possible explanation for our findings could be related to the instrument itself. The ASRS screener was originally developed to detect symptoms of ADHD in adults aged 18 to 44 years (Kessler et al., 2005). To the best of our knowledge, the applicability of this instrument in adults older than 44 years of age has yet to be validated. Another explanation could be that there is no long-term advantage of pharmacotherapy for ADHD relative to other therapies. Thus, long-term follow up of children with ADHD showed improvement on ADHD and associated symptoms from baseline, with initial differences in outcomes between treatment strategies (such as pharmacotherapy and behavior modification) disappearing over time, as shown in the Multimodal Treatment Study of Children with ADHD (the MTA study; Molina et al., 2009). Furthermore, age-related changes in the dopaminergic system, such as the decreased availability of dopamine transporters and dopamine receptors, must also be seen as a possible explanation for our results. This downregulation of the dopamine system may reduce the efficacy of treatment with stimulant medications (Volkow & Swanson, 2003). Our sample of adults aged 50+ with ADHD consisted of more women than men. Research has shown that, after menopause, the availability of dopamine receptors in older women is higher than in older men (Kaasinen et al., 2002). If this is true, a more balanced gender distribution in our study probably would have revealed an even worse outcome for those currently receiving medication. The timing of treatment onset could be a possible explanation as well, as those who are diagnosed with ADHD later in life do not respond as strongly to pharmacological treatment as those who are diagnosed earlier (Gjervan, Torgersen, Nordahl, & Rasmussen, 2012). Finally, although available characteristics did not show differences between groups, those who were currently taking ADHD medications could have been more impaired in other important areas of life, and those symptoms might have been ameliorated by their psychopharmacological treatment.
The percentage of participants who reported co-occurring disorders in this study is well in line with other studies of adults with ADHD (Sobanski et al., 2007). Co-occurring somatic disorders, however, were more often reported than co-occurring psychiatric disorders. Interestingly, Manor et al. (2011) also reported a high percentage of somatic disorders in their chart review of 11 middle-aged adults with ADHD (Manor et al., 2011).
A minority of participants in this study reported receiving nonpharmacological treatments for ADHD. Research has shown that pharmacotherapy alone is often not sufficient to treat adults with ADHD (Safren, 2006). Individualized and optimized treatments (Powell, Thomsen, Frydenberg, & Rasmussen, 2011), as well as treatment by specialists, have been suggested as important for optimal outcomes (Torgersen, Gjervan, & Rasmussen, 2008).
Only a minority of participants in this study had a favorable outcome, and the multivariate analysis indicated that a favorable outcome was only associated with employment. Employment has been identified as one of the several predictors of treatment response in adults with ADHD (Buitelaar et al., 2011), and in general, it has been found to be an important factor for quality of life (Aronson, 1997). However, ADHD research has also shown that outcomes are not associated with any particular variable alone but with the interaction of several variables (Hechtman, 1999). Furthermore, findings suggest that the remission of ADHD symptoms is not necessarily followed by functional recovery (Molina et al., 2009).
Strengths and Limitations
Our study has some limitations. Participants were recruited from the national patient organization, which is not necessarily a representative sample of all adults with ADHD. As membership of a patient organization may require personal engagement and continuity, more severely impaired adults with ADHD may have been underrepresented, which could limit the generalizability of our findings. Moreover, about one third of the eligible participants did not participate, and it is possible that this group may have comprised adults with more severe ADHD. A larger proportion of adults with more severe ADHD might have led to a greater proportion of participants with a better treatment outcome, as severe ADHD has been found to be a predictor of treatment response (Buitelaar et al., 2011).
We relied on self-report data that may have limited the information about impairment and ADHD symptom severity that we collected. Other studies have shown that the self-reports of adults with ADHD are fairly reliable and may even underestimate their own problems (Kooij et al., 2008; Manor et al., 2012; Murphy & Schachar, 2000).
Although baseline information for our sample was limited, other research indicates that the levels of functional and psychosocial impairments in undiagnosed adults with ADHD are quite similar to those in adults who have been diagnosed with ADHD (Able, Johnston, Adler, & Swindle, 2007; Biederman et al., 2006; Shekim, Asarnow, Hess, Zaucha, & Wheeler, 1990).
Our study sample consisted of more women than men. Findings by others, however, indicate that gender differences in the severity of symptoms and clinical presentations are limited in adults with ADHD (Biederman, Faraone, Monuteaux, Bober, & Cadogen, 2004; Rasmussen & Levander, 2009).
We were unable to control adherence to pharmacological treatments in this study, which is potentially important, as nonadherence to pharmacological treatment has been found to be quite common among adults with ADHD (Pappadopulos et al., 2009). In contrast, patients’ self-reports were found to be a fairly reliable method for measuring medication adherence in outpatients with severe mental disorders (Jonsdottir et al., 2010). Moreover, we recently reported in an adult sample with mean age 36.5 years that adults with ADHD who were treated with extended-release formulations of methylphenidate had a significantly better reported adherence to treatment than those treated with immediate-release formulations (Lensing, Zeiner, Sandvik, & Opjordsmoen, 2013).
Our results are strengthened by the large study sample and the length of observation. All data were gathered at one point in time, but the mean observation time (from ADHD diagnosis to when data were collected) was more than 5.5 years. With respect to treatment outcome, we recently reported that treatment for 2 years or more predicted a better outcome (Lensing et al., 2013).
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: From 2009 to 2011, M.B.L. was a member of the Scientific Committee of the Annual Nordic Psychiatric Academy ADHD meeting, which was organized and financially supported by Janssen Pharmaceutical Companies.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was financially supported by the Norwegian ExtraFoundation for Health and Rehabilitation through EXTRA funds (2009/1/0661).