
Abstract
ADHD is among the most commonly occurring psychiatric disorders of childhood (e.g., Spencer, Biederman, & Mick, 2007). ADHD frequently persists into adolescence and adulthood and is associated with multiple functional impairments. Of the impairments associated with ADHD, social impairment is particularly pervasive and intractable (Hoza, 2007). Findings of prior studies indicate that externalizing behavior problems and social impairment are partly attributable to emotion dysregulation (ED) among children with ADHD (Maedgen & Carlson, 2000; Melnick & Hinshaw, 2000; Parker, Majeski, & Collin, 2004). ED, when associated with ADHD, involves two primary deficits. These are an inhibitory deficit, which manifests in socially inappropriate behavioral responses to strong emotion, and a self-regulatory deficit, which manifests in an inability to (a) self-soothe physiologic arousal that strong emotion induces, (b) refocus attention, and (c) organize the self for coordinated action in the service of an external goal (Barkley, 2010). 1
Although the association between ADHD and ED as well as between ED and externalizing behavior problems and social impairment has been established (e.g., Maedgen & Carlson, 2000; Melnick & Hinshaw, 2000), some limitations to the available literature are worthy of note. First, ED encompasses impairments in a broad set of processes (Gratz & Roemer, 2004) and it is unclear which aspects thereof are most relevant to ADHD. Second, the association between ED and ADHD has been typically examined with child samples, leaving questions of generalizability across development unaddressed. Third, although prior findings indicate that ADHD subtype and comorbid conditions may affect the association between ED and ADHD (Maedgen & Carlson, 2000; Melnick & Hinshaw, 2000), only a few studies considered the effects of subtype or comorbidity on ED. Finally, ED has been typically measured in the context of experimental laboratory tasks (for exception, see Seymour et al., 2012). Thus, the ecological validity of prior findings as well as the impact of ED on the externalizing behavior problems and everyday social impairment of young adolescents with ADHD remains unclear.
In this study, our first aim was to examine which aspects of ED are associated with ADHD among young adolescents, taking into account ADHD subtype and comorbid oppositional defiant disorder (ODD). Our second aim was to evaluate the relationship between ED and externalizing behaviors (i.e., aggression and rule-breaking) as well as between ED and social impairment.
Youth With ADHD Exhibit Behavior Problems and Experience Social Impairment to Which ED May Contribute
Children with ADHD exhibit high rates of aggressive behaviors and rule-breaking, relative to typically developing peers (e.g., Buhrmester, Whalen, Henker, MacDonald, & Hinshaw, 1992; Cunningham & Siegel, 1987; Erhardt & Hinshaw, 1994; Grenell, Glass, & Katz, 1987; Guevremont & Dumas, 1994; Pelham & Bender, 1982). In turn, aggression and rule-breaking contribute to peer rejection (Guevremont & Dumas, 1994; Hoza et al., 2005) and social impairment (Biederman, Faraone, & Monuteaux, 2002; Cunningham & Barkley, 1979; Hoza, 2007). There is reason to believe that ED may contribute to aggression and rule-breaking 2 as well as to social impairment among children with ADHD.
Empirical findings indicate that children with ADHD exhibit physiological and observable behaviors consistent with ED (Musser et al., 2011; Musser, Galloway-Long, Frick, & Nigg, 2013; Seymour et al., 2012; Walcott & Landau, 2004). One manifestation of ED, slow return to emotional baseline, has been shown to be associated with aggression and predict social impairment among boys with ADHD (Melnick & Hinshaw, 2000). Other manifestations of ED, such as over-reactivity to positive and negative emotions (Barkley, 2010; Martel & Nigg, 2006), poor control of emotions (Erhardt & Hinshaw, 1994; Saunders & Chambers, 1996), and impatience likely contribute to peer perceptions of youth with ADHD as overly-exuberant, boisterous, disruptive, or intrusive in their social interactions (Henker & Whalen, 1989; Landau & Moore, 1991). It is thus likely that various manifestations of ED alienate peers, contribute to rejection, and thereby interfere with the social functioning of youth with ADHD. Yet, the association between ED and externalizing behavior problems and social impairment may be further complicated across ADHD subtypes and by comorbidities, such as ODD, and may vary across development.
Some research indicates that ED may vary as a function of ADHD subtype. One observational study found that children with the combined subtype of ADHD, but not children with the inattentive subtype, exhibit ED characterized by heightened emotional intensity and increased frequency and intensity of behaviors of emotional display (Maedgen & Carlson, 2000). In addition, negative emotionality is part of the diagnostic criteria for ODD (i.e., loses temper, touchy or easily annoyed, angry and resentful; Barkley, 2010), which co-occurs in preschool children with ADHD at a rate of 30% to 50% (Biederman, Newcorn, & Sprich, 1991). Although negative emotionality is not synonymous with ED, it is a risk-factor for ED (Belsky, Friedman, & Hsieh, 2001) and is closely linked to risk for developing ODD in children with ADHD (Martel & Nigg, 2006). Of note, by the time children reach school age, ODD in the absence of ADHD becomes less common (Lavigne et al., 2001; Maughan, Rowe, Messer, Goodman, & Meltzer, 2004), and half or more of ODD cases co-occur with ADHD. First, these data indicate that the temporal persistence of ODD may be linked to ADHD and that it may be beneficial to consider the role of ODD in functional outcomes of adolescents with ADHD. Second, these data also indicate that to ensure that any association between ADHD and ED are not merely an artifact of comorbidity, it is important to account for the effects of ODD when considering the association between ADHD and ED. Finally, with regard to development, adolescents with or without ADHD experience more intense and frequent emotions than younger or older persons (Silk, Steinberg, & Morris, 2003) and they are doing this in the context of increased environmental demands for behavioral and affect regulation (Steinberg, 2005). Normal adolescent development is thus characterized by improved coordination of behaviors, cognitions, and emotions and therefore by improved emotion regulation (Kopp, 1992; Southam-Gerow & Kendall, 2002). ED may thus be particularly debilitating for the social functioning of adolescents with ADHD.
In sum, ADHD is associated with ED and impairments in emotion regulation may be linked to externalizing behaviors, such as aggression and rule-breaking, as well as to social impairment. However, limitations to the literature, such as a relative lack of specificity on which aspects of ED are most relevant to ADHD, a paucity of studies with adolescents or that take into account ADHD subtype and ODD, and a focus on laboratory-based measurement of ED highlight the need for additional research. An enhanced understanding of the relationship among these constructs may help further clarify the debilitating social impairment of adolescents with ADHD and inform treatment development research.
Present Study
We conducted a study to investigate which subscales of ED differ between young adolescents with ADHD and a community sample and whether ED in young adolescents with ADHD varies as a function of ADHD subtype or comorbid ODD. We also conducted analyses of the relationship between various subscales of ED and aggression and rule-breaking, and between various subscales of ED and social impairment.
Method
Overview
The data analyzed for this study were collected in the context of a randomized controlled trial. Our sample was representative of youth with ADHD in this age-group with regard to comorbidity status, such as ODD (Biederman et al., 1991), any mood disorder (Biederman et al., 1992), and any anxiety disorder (Wilens et al., 2002). Our sample was also representative of our state census with regard to household income and parental education (U. S. Census Bureau, 2011).
Participants
Participants were 180 adolescents (75.7% males) who were recruited at two sites and from seven public middle schools in central and southern Ohio. One third of the participants were randomized to a community care condition and the other two thirds were randomly assigned to one of two treatment conditions. Participants were between the ages of 12 and 16 years (Mage = 13.5, SD = .91) and the majority of the sample was Caucasian (77.2%), followed by African Americans (11.7%), Hispanics (3.4%), and Other ethnicities (7.7%). The inclusionary criteria for the study were (a) attendance at one of the participating middle schools; (b) meet diagnostic criteria for at least one subtype of ADHD, (c) demonstrate academic or social impairment, (d) demonstrate an IQ of 80 or above on the Wechsler Abbreviated Scale of Intelligence (Wechsler, 1991), and (e) not meet diagnostic criteria for pervasive developmental disorder, bipolar disorder, psychosis, substance dependence other than tobacco, or obsessive-compulsive disorder.
All diagnoses were determined by the Children’s Interview for Psychiatric Syndromes–Parent version (P-ChIPS). With regard to ADHD diagnoses, to supplement parent interview data and confirm or disconfirm the presence of symptoms and impairment, parent- and teacher-reported data from the Disruptive Behavior Disorders Rating Scale (DBD) and parent- and teacher-administered Impairment Rating Scale (IRS) were also considered. For a diagnosis of ADHD, adolescents had to meet a total of six (or more) of the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) inattention or hyperactivity/impulsivity symptoms endorsed by either parents or teachers. At least four of the six endorsed symptoms had to be reported by parents. Unanimous agreement by two licensed psychologists on ADHD diagnoses was required before determining eligibility. For a summary of participants’ estimated IQ, diagnoses including comorbid ODD and subtype, grade level, and family income, see Table 1. For a summary of key demographic variables across ADHD subtypes and comorbid ODD, see Table 2.
Demographics.
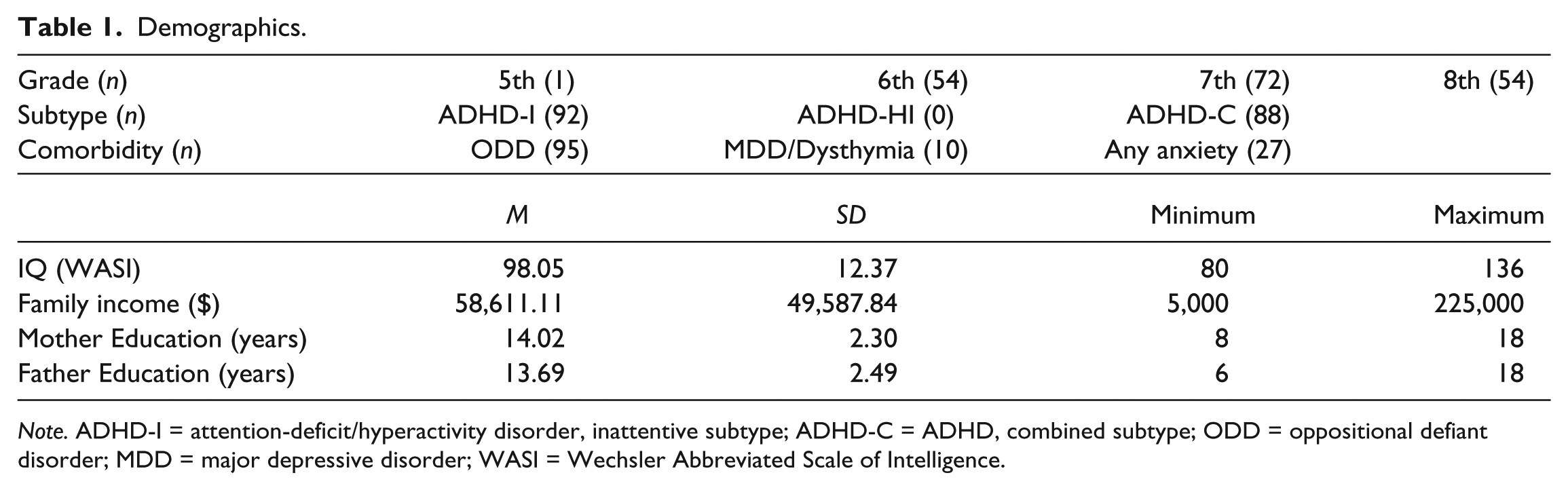
Note. ADHD-I = attention-deficit/hyperactivity disorder, inattentive subtype; ADHD-C = ADHD, combined subtype; ODD = oppositional defiant disorder; MDD = major depressive disorder; WASI = Wechsler Abbreviated Scale of Intelligence.
Descriptive Statistics on Key Demographic and Outcome Variables Across Subtypes and Comorbid ODD.
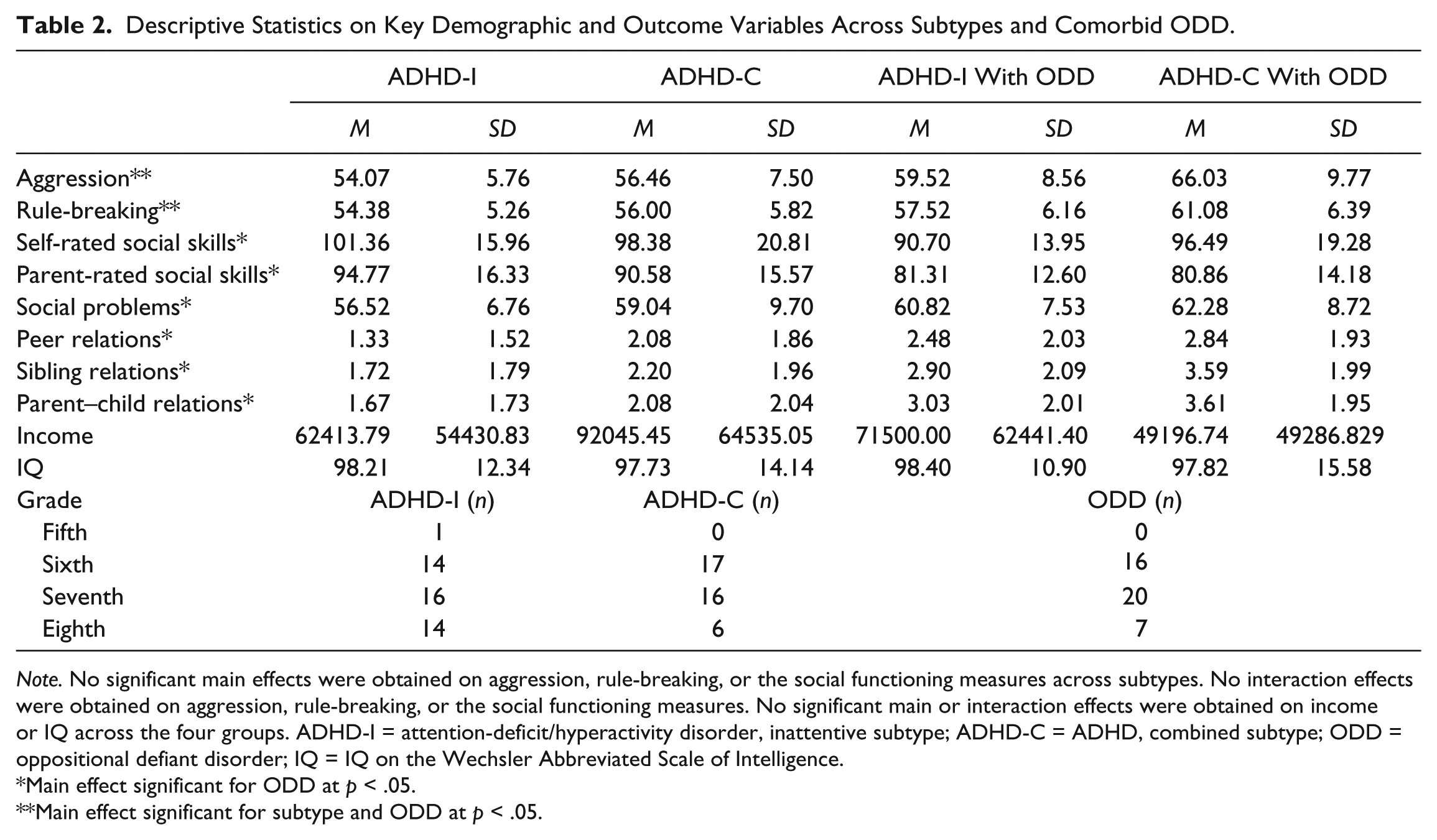
Note. No significant main effects were obtained on aggression, rule-breaking, or the social functioning measures across subtypes. No interaction effects were obtained on aggression, rule-breaking, or the social functioning measures. No significant main or interaction effects were obtained on income or IQ across the four groups. ADHD-I = attention-deficit/hyperactivity disorder, inattentive subtype; ADHD-C = ADHD, combined subtype; ODD = oppositional defiant disorder; IQ = IQ on the Wechsler Abbreviated Scale of Intelligence.
Main effect significant for ODD at p < .05.
Main effect significant for subtype and ODD at p < .05.
Procedures
Recruitment flyers were mailed to all families with children attending the middle schools participating in this study during 2 consecutive school years. Primary caregivers (79% mothers) who responded to the flyers participated in a telephone screen to assess the likelihood of child eligibility. If the parent reported that the child had a prior diagnosis of ADHD or endorsed four or more symptoms of inattention, parents and their children were scheduled for a session to complete informed consent procedures and an evaluation. Participating families were involved with the study for 1 academic year and 6 months, with all interventions taking place during the first year. In the larger study, participating families completed measures at the initial evaluation, three times during the school year, at the end of the academic year (post-treatment), and at a 6-month follow-up point. Participants and their parents completed the ED, aggression, rule-breaking, and social functioning measures for the present study during the post-treatment evaluations in May or June, right after treatment ended. Measures of ED, aggression, rule-breaking, and social functioning were administered to parents and adolescents. Similar to the completion of all other measures, parents and adolescents were in different rooms while completing the measures and did not have access to each other’s responses.
Measures
Measures used in this study were those used in diagnostic decisions (i.e., P-ChIPS, DBD, and IRS) and two self-report questionnaires on ED, a parent-report questionnaire on aggression and rule-breaking and parent- and self-report questionnaires on social functioning. For descriptive statistics on the outcome variables across ADHD subtypes and comorbid ODD, see Table 2.
P-ChIPS
The P-ChIPS (Weller, Weller, Rooney, & Fristad, 1999) is a structured parent interview of 20 DSM-IV-TR (APA, 2000) mental health disorders in youth aged 6 to18 years. Adequate psychometric properties have been reported for the PChIPS (Weller, Weller, Fristad, Rooney, & Schecter, 2000).
DBD
The DBD (Pelham, Gnagy, Greenslade, & Milich, 1992) is a 45-item parent- and teacher-report measure of the presence and severity of DSM-IV symptoms of ADHD, ODD, and conduct disorder (CD). Parents and teachers rate items on a four-point scale ranging from 0 (“not at all” present) to 3 (“very much” present) with higher scores indicating more severe symptoms. Scores for the entire measure range from 0 to 135, for the ADHD subscale from 0 to 54, for the ODD subscale from 0 to 24, and for the CD subscale from 0 to 84. The DBD has well-established reliability and validity (Pelham et al., 1992). In the present study, parents and teachers completed the DBD for diagnostic purposes.
IRS
The IRS (Fabiano et al., 2006) is a parent- and teacher-report measure of areas of functioning in which children with ADHD are typically impaired (Fabiano et al., 2006). The parent version contains seven items (relationship with peers, relationship with siblings, relationship with parents, academic progress, self-esteem, influence on family functioning, and overall impairment), and the teacher version contains six items (relationship with peers, relationship with teacher, academic progress, self-esteem, influence on classroom functioning, and overall impairment). Parents and teachers rate items on a visual analogue scale by placing an “X” on a line that represents a continuum of impairment and ranges from 0 (“no problem/definitely does not need treatment or special services”) to 6 (“extreme problem/definitely needs treatment or special services”). As each item represents a unique domain of impairment, scores range from 0 to 6. The IRS demonstrated excellent temporal stability and convergent and discriminant validity (Fabiano et al., 2006) as well as effectiveness in discriminating between children whose parent and teacher ratings of ADHD symptoms are consistent with a diagnosis of ADHD and children whose ratings of symptoms is below the DSM-IV threshold (Fabiano et al., 2006). In the present study, parents and teachers completed the IRS for diagnostic purposes and items from the parent-report measure were used as an index of social impairment in the analyses.
Difficulties in Emotion Regulation Scale (DERS)
The DERS (Gratz & Roemer, 2004) is a 36-item self-report measure of ED. Items are rated on a five-point scale (1 = Almost Never, 5 = Almost Always), with higher scores indicating greater difficulty with emotion regulation. Subscales of the DERS are as follows: Nonacceptance of Emotional Responses (Nonacceptance), Difficulties Engaging in Goal-Directed Behavior (Goals), Impulse Control Difficulties (Impulse), Lack of Emotional Awareness (Awareness), Limited Access to Emotion Regulation Strategies (Strategies), and Lack of Emotional Clarity (Clarity). Scores for the total DERS range from 36 to 180. The DERS demonstrated good internal consistency, good test–retest reliability, and adequate construct and predictive validity in multiple adolescent samples (Adrian et al., 2009; Vasilev, Crowell, Beauchaine, Mead, & Gatzke-Kopp, 2009; Weinberg & Klonsky, 2009). In addition, the DERS exhibited robust correlations with psychological problems reflecting ED (Weinberg & Klonsky, 2009) and physiological measures of ED (Vasilev et al., 2009). In the present study the DERS demonstrated excellent internal consistency (α = .912). Means and standard deviations have been reported elsewhere (13- to 17-year-olds: Weinberg & Klonsky, 2009) and were used for the statistical analyses addressing the first research aim of this study.
Emotion Regulation Index for Children and Adolescents (ERICA)
The ERICA (MacDermott, Gullone, & Allen, 2010) is a 16-item self-report measure of emotion regulation in children and adolescents. Items are rated on a five-point scale (1 = Strongly Disagree to 5 = Strongly Agree), with higher scores indicating better regulation of emotions. Subscales of the ERICA are as follows: Emotional Control (Emotional Control), Emotional Self-Awareness (Self-Awareness), and Situational Responsiveness (Situational Responsiveness). Scores for the total ERICA range from 16 to 80. The ERICA has demonstrated good internal consistency, good test–retest reliability, and good convergent and construct validity in a sample of 9- to 16-year olds (MacDermott et al., 2010). In the present study the ERICA demonstrated good internal consistency (α = .801). Means and standard deviations are reported elsewhere (MacDermott et al., 2010) and were used for the statistical analyses addressing the first research aim.
Child Behavior Checklist (CBCL)
The CBCL (Achenbach, 1991) is 113-item parent- and teacher-report measure of children’s aggressive behavior, rule-breaking, and social problems. Items are rated on a 3-point scale (0 = Not True to 2 = Very True of Often True). Internal consistency and test–retest reliability are good, with test–retest coefficients ranging from .78 to .88 for the subscales. There is also evidence for the convergent and discriminative validity of the CBCL and the measure has demonstrated utility in distinguishing between referred and nonreferred populations (Achenbach, 1991; Drotar, Stein, & Perrin, 1995). For the present study, we used scores from the aggressive behaviors and rule-breaking subscales as representing behaviors that may be associated with ED, for two reasons. First, manifestations of ED for youth with ADHD are frequently characterized as verbal and physical aggression (Guevremont & Dumas, 1994; Henker & Whalen, 1989; Landau & Moore, 1991) and as a tendency to violate rules (Guevremont & Dumas, 1994). Furthermore, aggression and rule-breaking are behaviors associated with ODD. We used the social problems subscale as an index of social impairment. In the present study, parents completed the CBCL.
Social Skills Improvement System–Rating Scales (SSIS-RS)
The SSIS-RS (Elliott & Gresham, 2008) is a parent- and self-report measure of two domains of social functioning: social skills and problem behaviors. The social skills domain is comprised of 46 items and the problem behaviors domain is comprised of 29 items, rated on a four-point scale (0 = Never to 3 = Almost Always). Scores on the social skills subscale range from 0 to 138, and on the problem behaviors from 0 to 87. Norms and standardization sample information reveal acceptable psychometric properties: median scale reliabilities of the Social Skills and Problem Behavior scales in the mid-to-upper .90s; median subscale reliabilities in the mid-.80s (Parent Form), and near .80 (Student Form); test–retest indices for Total Social Skills .84 (Parent Form), and .81 (Student Form); test–retest indices for Total Problem Behavior .87 (Parent Form), and .77 (Student Form) (Gresham, Elliott, Vance, & Cook, 2011). The SSIS-RS was completed by parents and adolescents.
Data Preparation and Preliminary Analyses
Eight participants failed to respond to one item each on the measures of ED. Mean-imputing based on participants’ average score on the subscale to which the item belongs was conducted. There was no pattern to missing data.
To examine whether being randomized to one of the three treatment conditions (i.e., a community care and two treatment conditions), whether key demographic variables such as gender and grade, or whether clinical diagnoses commonly comorbid with ADHD, such as CD, major depressive disorder, or generalized anxiety disorder had an effect on ED, a multivariate analysis of variance (MANOVA) was conducted to compare participants across these variables on measures of ED (on each ED subscale). In the presence of all other variables, the omnibus test of effects of condition, F(9, 154) = .791, p = .711; grade, F(9, 154) = .830, p = .713; CD, F(9, 154) = .679, p = .727; major depressive disorder, F(9, 154) = .590, p = .804; or generalized anxiety disorder, F(9, 154) = 1.280, p = .252 were nonsignificant. The omnibus test of gender was significant, F(9, 154) = 2.194, p = .025. This effect was due to a group difference on DERS Goals F(9, 154) = 4.754, p = .031 and a marginally significant group difference on ERICA Self-Awareness F(9, 154) = 3.766, p = .054. Follow-up analyses indicated that females (M = 15.07, SD = 5.40) exhibited higher ED than males (M = 13.55, SD = 4.86) on DERS Goals and females (M = 16.59, SD = 3.24) exhibited higher ED than males (M = 16.84, SD = 3.74) on ERICA Self-Awareness. Because of this gender difference, we entered gender as a covariate in all analyses. See Table 3 for bivariate correlations for all study variables.
Pearson Correlations Among All Study Variables.
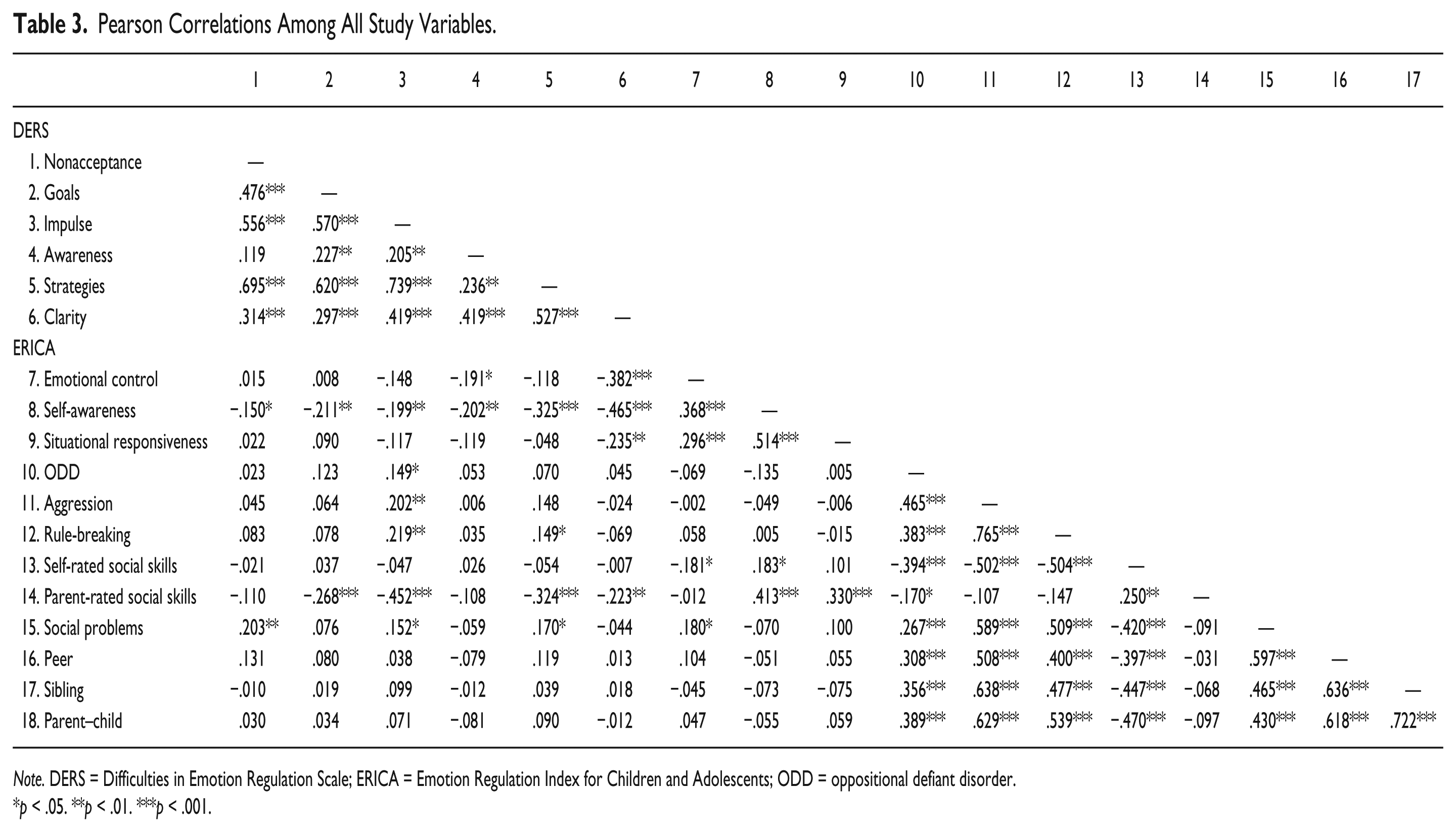
Note. DERS = Difficulties in Emotion Regulation Scale; ERICA = Emotion Regulation Index for Children and Adolescents; ODD = oppositional defiant disorder.
p < .05. **p < .01. ***p < .001.
Results
Nine (six DERS and three ERICA factors) one-sample t tests were used to compare our female sample means with data published elsewhere (MacDermott et al., 2010; Weinberg & Klonsky, 2009). Because of limitations to the size of the current sample (n = 44), an alpha correction for interpreting p values was not applied. 3 Our findings indicate that, compared to values obtained in a community sample of adolescent females, adolescent females with ADHD experience ED characterized by a lack of awareness and inattention to emotional responses (DERS Awareness, t(43) = 4.586, p < .001, d = .716, large), emotional inflexibility and a slow return to emotional baseline (ERICA Self-Awareness, t(43) = −3.973, p < .001, d = .603, large), difficulty in behavioral control when experiencing negative emotions (DERS Impulse, t(43) = 2.795, p = .008, d = .465, medium), difficulty exhibiting socially appropriate emotional responses (ERICA Situational Responsiveness, t(43) = −3.372, p = .002, d = .520, medium), and a lack of confidence in their ability to effectively regulate their emotions when upset (DERS Strategies, t(43) = 2.586, p = .013, d = .415, medium; see Table 4).
Adolescents’ Self-Ratings of Emotion Dysregulation by Sex.
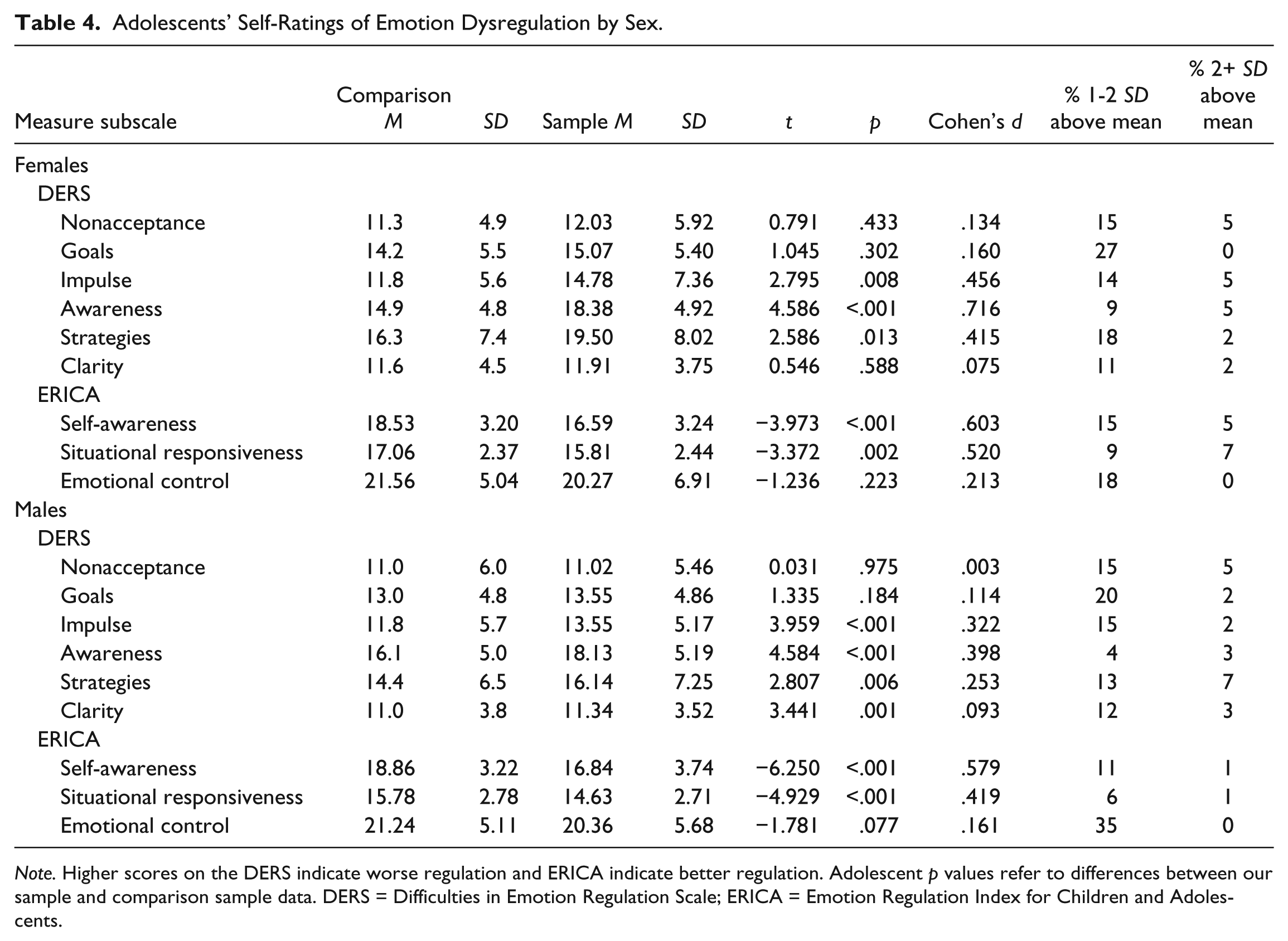
Note. Higher scores on the DERS indicate worse regulation and ERICA indicate better regulation. Adolescent p values refer to differences between our sample and comparison sample data. DERS = Difficulties in Emotion Regulation Scale; ERICA = Emotion Regulation Index for Children and Adolescents.
Nine (six DERS and three ERICA factors) one-sample t tests were used to compare our male sample means with data published elsewhere (MacDermott et al., 2010; Weinberg & Klonsky, 2009). A Bonferroni correction was applied as our sample of boys was adequately large (.05/9 = .006) to correct for family-wise error. Our findings indicate that, compared to values obtained in a community sample of adolescent males, adolescent males with ADHD experience ED characterized by emotional inflexibility and a slow return to emotional baseline (Self-Awareness t(136) = −6.250, p < .001, d = .579, large), difficulty exhibiting socially appropriate emotional responses (Situational Responsiveness t(136) = −4.929, p < .001, d = .419, medium), a lack of awareness and inattention to emotional responses (DERS Awareness t(136) = 4.584, p < .001, d = .398, medium), difficulty in behavioral control when experiencing negative emotions (DERS Impulse t(136) = 3.959, p < .001, d = .322, medium), and a lack of knowledge and clarity about the emotions they are experiencing (DERS Clarity t(136) = 3.441, p = .001, d = .253, small; see Table 4).
Because previous findings were mixed as to how those with ADHD, combined subtype (ADHD-C) differ from those with ADHD, inattentive subtype (ADHD-I) on indices of ED (Chhabildas, Pennington, & Willcutt, 2001; Maedgen & Carlson, 2000), we examined the difference between the two subtypes present in our sample (i.e., ADHD-C [n = 88] and ADHD-I [n = 92]) on ED subscales. A MANOVA was conducted to compare participants with ADHD-C to those with ADHD-I. Gender was a marginally statistically significant covariate, F(9, 165) = 1.929, p = .051. The omnibus test for subtype-based group differences was nonsignificant, F(9, 165) = 1.429, p = .179. Values for subtype-based comparisons on the individual ED subscales were Fs ranging from .001 to 3.345, ps ranging from .976 to .069.
In addition, because it has been argued that a failure to control for comorbid conditions may lead to the “erroneous conclusion that the deficits found in the ADD children are attributable to their ADD when, in fact, they are due to the overlap with other co-morbid disorders” (Barkley, Grodzinsky, & DuPaul, 1992, p. 184), we examined whether those with ADHD only, in comparison with those with comorbid ODD, differed on ED. Specifically, we examined the difference between those with ADHD only and those with ADHD and ODD, on all nine ED subscales in a manner similar to those used in previous studies with children (e.g., Melnick & Hinshaw, 2000). A MANOVA was conducted to compare participants with ADHD only (n = 86) with those with comorbid ODD (n = 94). Gender was a significant covariate, F(9, 165) = 2.021, p = .040. This effect was due to a gender difference on DERS Goals F(9, 165) = 4.035, p = .046; DERS Strategies F(9, 165) = 7.213, p = .008; and ERICA Situational Responsiveness F(9, 165) = 6.278, p = .013. The omnibus test for ODD-based group differences was nonsignificant, F(9, 165) = 1.531, p = .141. (See “Data Preparation and Preliminary Analyses” for gender-based differences when not accounting for ODD). Values for comorbidity-based comparisons on the individual ED subscales were Fs ranging from .101 to 5.312, ps ranging from .751 to .022.
In the absence of scales directly derived from theory about ED associated with ADHD as well as a lack of prior data on facets of ED that are associated with aggression, rule-breaking, or with social impairment in this population, we did not have a rationale for pre-selecting specific ED subscales as predictors. Thus, our analyses were exploratory and involved determining the extent to which self-reported ED is a predictor of aggression, rule-breaking, and social impairment. The independent variables in these analyses were the nine indices of ED as measured by the DERS and ERICA. To examine whether ED is associated with aggression or rule-breaking, a multivariate linear regression analysis was conducted and the dependent variables were parent ratings on the CBCL of adolescents’ (a) aggressive behaviors and (b) rule-breaking. To address whether ED is associated with social impairment, a second multivariate linear regression analysis was conducted and the dependent variables were indices of social impairment measured by adolescents’ (a) parent-reported social problems on the CBCL; (b) parent- and (c) self-reported social skills on the SSIS; and parent-reported (d) peer, (e) parent, and (f) sibling relationship problems on the IRS.
A multivariate linear regression analysis was conducted, with all nine ED subscales as predictors and aggression and rule-breaking as outcome variables. Gender was not a significant covariate F(6, 162) = 2.285, p = .105. The omnibus test was significant for DERS Impulse F(9, 163) = 3.530, p = .032 and DERS Clarity F(9, 163) = 3.309, p = .039. This effect was due to DERS Impulse predicting parent-rated aggression F(1, 163) = 5.731, p = .018 and rule-breaking F(1, 163) = 6.674, p = .011 and DERS Clarity predicting parent-rated rule-breaking F(1, 163) = 6.493, p = .012. Follow-up simple linear regression analyses, with each significant predictor paired with each significant outcome variable, indicated that all predictors remained significant (see Table 5), with the exception of DERS Clarity predicting rule-breaking.
Follow-Up Simple Regression Models.
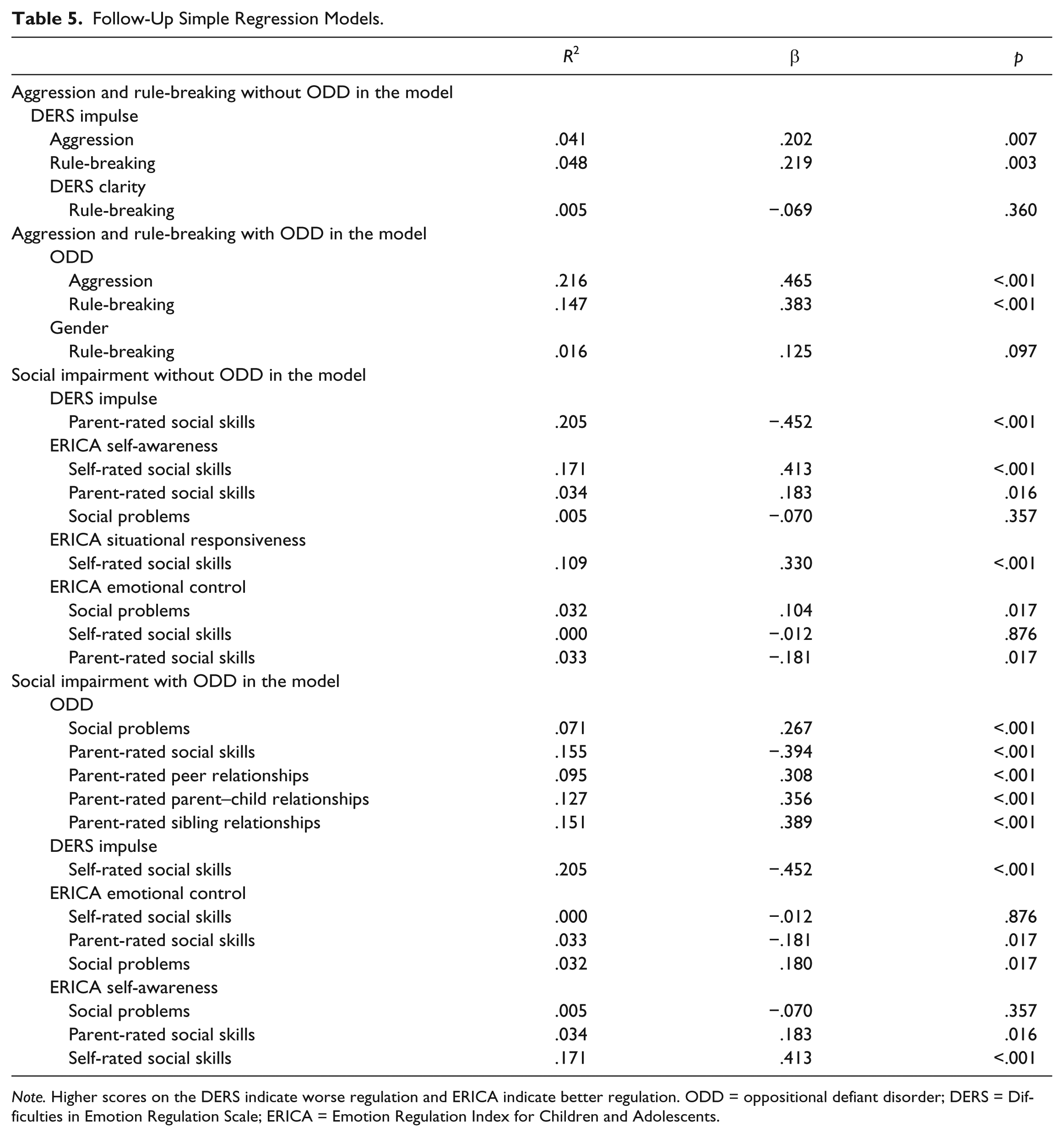
Note. Higher scores on the DERS indicate worse regulation and ERICA indicate better regulation. ODD = oppositional defiant disorder; DERS = Difficulties in Emotion Regulation Scale; ERICA = Emotion Regulation Index for Children and Adolescents.
Due to reasons outlined above, we replicated the first set of analyses controlling for ODD, by entering ODD into our model as an independent variable. A multivariate linear regression analysis was conducted, with ODD, all nine ED subscales as predictors and parent-reported aggression and rule-breaking as the outcome variables. Gender was a significant covariate F(2, 163) = 3.310, p = .039. Gender predicted rule-breaking F(2, 163) = 6.000, p = .015.
The omnibus test was also significant for ODD F(2, 163) = 21.374, p < .001. This effect was due to ODD predicting parent-rated aggression F(2, 163) = 41.241, p < .001 and rule-breaking F(1, 163) = 30.174, p < .001. Follow-up simple linear regression analyses, with each significant predictor paired with each significant outcome variable, indicated that ODD remained a significant predictor but gender did not (see Table 5).
A multivariate linear regression analysis was conducted, with all nine ED subscales as predictors and self-rated social skills, parent-rated social skills, parent-rated social problems, and parent-rated peer, parent, and sibling relationship problems as the outcome variables. Gender was not a significant covariate F(6, 135) = 1.911, p = .845.
The omnibus test was significant for DERS Impulse F(6, 132) = 6.368, p < .001; ERICA Self-Awareness F(6, 132) = 5.645, p < .001; ERICA Emotional Control F(6, 132) = 4.716, p < .001; and ERICA Situational Responsiveness F(6, 132) = 2.226, p = .044. This effect was due to DERS Impulse predicting self-rated social skills F(1, 132) = 32.318, p < .001; ERICA Self-Awareness predicting parent-rated social skills F(1, 132) = 15.345, p < .001, self-rated social skills F(1, 132) = 18.765, p < .001, and parent-rated social problems F(1, 132) = 6.606, p = .011; ERICA Emotional Control predicting parent-rated social skills F(1, 132) = 11.136, p = .001, self-rated social skills F(1, 132) = 15.827, p < .001, and parent-rated social problems F(1, 132) = 5.600, p = .019; and ERICA Situational Responsiveness predicting self-rated social skills F(1, 132) = 4.476, p = 0.36. ERICA Situational Responsiveness was also a marginally significant predictor of parent-rated social problems F(1, 132) = 3.671, p = .057. Follow-up simple linear regression analyses, with each significant predictor paired with each significant outcome variable, indicated that all predictors remained significant (see Table 5), with the exception of ERICA Self-Awareness predicting social problems, and ERICA Emotional Control predicting self-rated social skills.
Due to reasons outlined above, we replicated the first set of analyses controlling for ODD, by entering ODD into our model as an independent variable. A multivariate linear regression analysis was conducted, with ODD, all nine ED subscales as predictors, and self-rated social skills, parent-rated social skills, parent-rated social problems, and parent-rated peer, parent, and sibling relationship problems as the outcome variables. Gender was not a significant covariate F(6, 132) = .820, p = .556.
The omnibus test was significant for ODD F(6, 131) = 8.232, p < .001; DERS Impulse F(6, 131) = 5.659, p < .001; ERICA Emotional Control F(6, 131) = 5.260, p < .001; and ERICA Self-Awareness F(6, 131) = 4.182, p = .001. This effect was due to ODD predicting parent-rated social skills F(1, 131) = 31.671, p < .001, social problems F(1, 131) = 9.467, p = .003, peer relationship problems F(1, 131) = 15.925, p < .001, parent–child relationship problems F(1, 131) = 18.412, p < .001, and sibling relationship problems F(1, 131) = 36.883, p < .001; DERS Impulse predicting self-rated social skills F(1, 131) = 26.865, p < .001; ERICA Emotional Control predicting parent-rated social skills F(1, 131) = 13.878, p < .001, self-rated social skills F(1, 131) = 15.278, p < .001, and parent-rated social problems F(1, 131) = 6.550, p = .012; and ERICA Self-Awareness predicting parent-rated social skills F(1, 131) = 7.636, p = .007 and self-rated social skills F(1, 131) = 14.669, p < .001. ERICA Self-Awareness was also a marginally significant predictor of parent-rated social problems F(1, 131) = 3.052, p = .083. Follow-up simple linear regression analyses, with each significant predictor paired with each significant outcome variable, indicated that all predictors remained significant (see Table 5), with the exception of ERICA Emotional Control predicting self-rated social skills and ERICA Self-Awareness predicting parent-rated social problems.
Discussion
The purpose of this study was to evaluate aspects of ED that characterize young adolescents with ADHD, examine the effects of subtype and comorbidity, and determine the extent to which ED is related to aggression and rule-breaking and to social impairment. Analyses of self-report data obtained with young adolescent females and males with ADHD indicated that both females and males differed from a community sample of same-aged peers on four aspects of ED. These are on the DERS on Awareness (a lack of awareness and inattention to emotional responses) and Impulse (difficulty in behavioral control when experiencing emotions), and on the ERICA on Self-Awareness (emotional inflexibility and a slow return to emotional baseline) and Situational Responsiveness (exhibiting socially inappropriate emotional responses in social situations). In addition, young adolescent females with ADHD differed from a community sample of peers on the DERS on Strategies (a lack of confidence in their ability to effectively regulate their emotions when upset), and young adolescent males with ADHD differed from a community sample of peers on the DERS on Clarity (a lack of knowledge and clarity about the emotions they are experiencing). There were no differences in self-rated ED across ADHD subtypes or between youth with and without ODD. However, there were differences between females and males with ADHD, in that females reported higher ED on DERS Goals (difficulty with goal-directed behavior when experiencing negative emotions) and marginally higher ED on ERICA Self-Awareness (emotional inflexibility and a slow return to emotional baseline) than males.
Our not having obtained subtype-based differences is in contrast to prior research (Maedgen & Carlson, 2000). Specifically, Maedgen and Carlson (2000) reported that children with ADHD-C exhibited high emotional intensity and intensified behavioral expression of both positive and negative emotions, but those with ADHD-I did not. There are two likely explanations for the difference between these findings and the ones we obtained, and these explanations are interconnected. First, differences may be related to participants’ age. Participants in Maedgen and Carlson’s sample were between 8 and 11 years of age and our participants were between 12 and 16 years of age (see Note 1). It has been argued that changes in context, expectations, and maturation result in different presentation of ADHD among adolescents relative to school-aged children (Wolraich et al., 2005). In fact, symptoms of hyperactivity become more subtle during the teenage years (Langberg et al., 2008) and many youth who were diagnosed with Combined Type during childhood better fit the Inattentive Type during their teenage years (Wolraich et al., 2005). Because hyperactivity diminishes and subtype differences become more subtle during adolescence, the distinction between subtypes on manifestations of ED might also be less noticeable.
Furthermore, it may be that different situations elicit ED in the different subtypes and, when a larger number of situations are sampled (e.g., when using a rating scale), ED is detectable in more than one subtype. In contrast, the specific laboratory task used by Maedgen and Carlson might be such that it elicits ED, but not in a manner representative of the multiple contexts of a child’s day. This would be in line with recent proposals by Nigg (2010) who posits that ADHD is a combination of problems in both bottom up (e.g., emotion generation) and top down (e.g., emotion control) control systems with “distinct influences leading to their occasional convergence. What psychopathologists call attention problems reflects difficulty in regulation, constraint, and effortful control, whereas impulsivity and perhaps, hyperactivity are related to breakdown in incentive response systems” (p. 25). Thus, although the etiology and outward expression of ED across subtypes might differ, the relevant subjective experience and associated social impairments might not.
Results of exploratory analyses regarding aspects of ED that relate to aggression or rule-breaking indicated that DERS Impulse predicted parent-rated aggression and rule-breaking. The results of analyses regarding aspects of ED that relate to social impairment indicated that the ERICA Self-Awareness and Emotional Control subscales predicted parent- and self-ratings of social functioning on two of six indices of social impairment and the DERS Impulse and ERICA Situational Responsiveness subscales predicted social functioning on one of six indices of social impairment. In the presence of comorbid ODD, ED was not predictive of aggression or of rule-breaking. However, even in the presence of comorbid ODD, ERICA Self-Awareness and Emotional Control and DERS Impulse remained significant predictors of social functioning on three of six indices of social impairment. Specifically, ERICA Self-Awareness remained a significant predictor of parent- and self-rated social skills, ERICA Emotional Control remained a significant predictor of parent-rated social skills and social problems, and DERS Impulse remained a significant predictor of self-rated social skills. Our findings thus converge to indicate that the Self-Awareness and Emotional Control subscales of the ERICA and the Impulse subscale of the DERS differentiate young adolescents with ADHD from a community sample and are associated with social impairment, above and beyond comorbid ODD. Examining the items on these three subscales may help us understand the nature of the ED problems that characterize young adolescents with ADHD.
Items on the Self-Awareness subscale of the ERICA appear to be focused on flexible emotion management or adaptability (“I handle it well when things change or I have to try something new”) and a generally euthymic emotional style (“I am a happy person,” “I am a sad person,” “I am quiet and shy, and I don’t show my feelings”) to which the individual is able to return in a timely manner (“When I get upset, I can get over it quickly”). What appears to be an aspect of this subscale that may be unique to ADHD is its relevance for the individual’s ability to adjust to provocation and new situations or adaptability. Youth with ADHD cope less flexibly (i.e., adjust to, as opposed to change situations that become uncontrollable; Babb, Levine, & Arseneault, 2010), have more difficulty adapting to changes in routine, surroundings, or plans and recovering from setbacks in a timely manner (Jarratt, Riccio, & Siekierski, 2005; Manning & Miller, 2001).
The Emotional Control subscale of the ERICA is comprised of items that measure a low threshold for emotional excitability (“When things don’t go my way I get upset easily”), impatience (“I have trouble waiting for something I want”), socially inappropriate behaviors (“I can be disruptive at the wrong times,” “I annoy others by not minding my own business”), under-controlled anger (“I have angry outbursts”), and defiance (“I get angry when adults tell me what I can and cannot do”). In our experience, from the perspective of parents and teachers, low threshold for emotional excitability, impatience, and socially inappropriate behaviors are often characterized as “responding in an inappropriate manner at inappropriate times.” Empirical evidence related to such low threshold and impatience indicate that youth with ADHD may be more sensitive to external stimuli and, as a result, often respond instantly to provocation (Richardson, 2000). In addition, youth with ADHD have been characterized as exhibiting over-excitability and over-reaction to rewards or provocation (Firestone & Douglas, 1975).
The Impulse subscale of the DERS comprises items that measure respondents perceiving their emotions as overwhelming (“I experience my emotions as overwhelming and out of control”) and experiencing difficulties with remaining in control (“When I’m upset, I have difficulty controlling my behaviors,” “When I’m upset, I feel like I can remain in control of my behaviors”) and ultimately losing control of their behavior when experiencing negative emotions (“When I’m upset, I become out of control,” “When I’m upset, I feel out of control,” “When I’m upset, I lose control over my behaviors”). These items tap into processes involved in the adaptation of the outward behavioral expression of emotional states in a manner that those are congruent with (social) situational demands. Those skilled in behavioral control while experiencing negative emotions engage in socially appropriate behaviors even in the face of confrontation, whereas those with poor behavioral control lose control of the manifest expression of emotions (Bickel, Jarmolowicz, Mueller, Gatchalian, & McClure, 2012). Our finding that young adolescents with ADHD have difficulty managing their behaviors in response to emotional arousal is consistent with theory (Barkley, 1997, 2010) and findings obtained in studies investigating relevant skills among young children (e.g., Walcott & Landau, 2004). Similar to the findings of Melnick and Hinshaw (2000), our results indicate that difficulty with behavioral management in the face of emotional arousal is associated with poor social functioning.
The Role of ODD
Our findings indicate that three aspects of ED, emotional inflexibility and a slow return to emotional baseline; a low threshold for emotional excitability, impatience, and socially inappropriate behaviors; and difficulty in behavioral control when experiencing negative emotions, differentiate youth with ADHD from a community sample and are associated with social impairment, even when accounting for comorbid ODD. However, other domains of ED, such as the extent to which youth experience difficulty exhibiting socially appropriate emotional responses, such as empathy and friendliness (ERICA Situational Responsiveness) may be associated with ODD (e.g., some items on this subscale measure empathy or callousness/unemotionality: “When others are upset, I become sad or concerned for them,” “I enjoy seeing others hurt or upset”). Indeed, ODD predicted areas of social impairment that had been accounted for by this subscale when ODD was not considered.
The predictive power of the ED subscales of externalizing behaviors that have been previously shown to be related to ODD, such as aggression and rule-breaking was nonsignificant when ODD was accounted for. Upon examination of these constructs, it is apparent that the aggression and rule-breaking subscales on the CBCL include a list of negative behaviors that are relatively close to symptoms of ODD. Similarly, only ODD predicted impairment in peer, sibling, and parent–child relationship items on the IRS. These items are also rated from the perspective of impairment and need for treatment, and therefore represent dysfunction. Thus, it appears that the unique variance accounted for by measures of ED used in this study may be more related to positive, prosocial behaviors measured by the SSIS-RS and social problems on the CBCL, than to the antisocial behavior measured by the aggression and rule-breaking subscales on the CBCL or the dysfunction measured by the IRS.
These findings are relevant to conceptualizing the clinical heterogeneity in ADHD as it relates to ED. Recently, Musser and colleagues (2013) found that, controlling for CD, children with ADHD and clinically low prosocial behavior (i.e., callous/unemotional traits) experienced difficulties with emotion regulation but relatively low arousal. 4 Conversely, youth with ADHD and normal-range prosocial behavior displayed elevated sympathetic activity, indicating they experienced high emotional arousal. In combination with our findings, it may be the case that youth with ADHD who experience difficulties with empathy, friendliness, or callousness/unemotionality comprise a group that is different with regard to ED from youth with ADHD but without such difficulties. In addition, it may be ODD that confers increased risk for youth with ADHD to experience impairments in their ability to exhibit difficulties with socially appropriate emotional responses, such as empathy and friendliness. Yet, regardless of symptoms of CD or ODD, the young adolescents with ADHD in our sample exhibited emotional inflexibility and a slow return to emotional baseline; a low threshold for emotional excitability, impatience, and socially inappropriate behaviors; and difficulty in behavioral control when experiencing negative emotions.
Treatment Implications
From a treatment perspective, one primary issue to consider is whether ED explains social impairment among young adolescents with ADHD above and beyond ODD. Current evidence-based treatments of ODD involve parent (and teacher) training (Eyberg, Nelson, & Boggs, 2008). If ED does not explain social impairment among those with ADHD above and beyond ODD, then such treatments may suffice to address associated impairment. However, if there are unique contributions of ED to social impairment, then treatment efforts may need to extend beyond addressing social impairment explained by ADHD alone or with comorbid ODD and incorporate a focus on ED. First, some of our findings indicate there is incremental utility in a focus on ED. Second, ODD is exclusive to negative emotionality (i.e., often loses temper, is often angry and resentful, is often spiteful or vindictive). Conversely, ED associated with ADHD may consist of two component processes including positive and negative emotionality and regulation (i.e., effortful and reactive forms of control; Martel, 2009). These involve problems both in the positive incentive approach and negative withdrawal systems (Martel & Nigg, 2006), and manifests in exuberant positive affect and fearful and angry negative affect (Nigg, Goldsmith, & Sachek, 2004). Thus, our findings and the previously established differences between ODD and ED indicate that if ED is not addressed in treatments targeting social impairment in ADHD, important contributors to problems in prosocial behavior may be missed. In fact, this argument combined with the absence of observable systematic associations between ED facets and ODD, indicate that while ED and ODD both explain social impairment, areas of non-overlap may provide important insights into our understanding of social impairment among young adolescents with ADHD. It may be the case that specific aspects of ED contribute to both the presence of negative social behaviors and the absence of positive social behaviors, but the presence of ODD compounds social impairment by increasing the likelihood of the negative social behaviors beyond what may simply be attributable to ED. Future studies that evaluate complex models of these relationships will be needed to address these questions to inform conceptualizations of possible causal pathways and treatment development.
Future Directions
The relationship between ADHD subtypes and ED certainly warrants additional investigation in light of the inconsistency across prior findings and the present study. Part of the problem may be that the validity of subtypes and the measurement of symptoms are in need of improvement for adolescents. Both the nature of ADHD subtypes and ED among adolescents may be areas in which we have a limited understanding, thus complicating the study of relationships between them. Relatedly, future research may focus on further examining the heterogeneity in ADHD as it relates to ED.
Our findings suggest that part of the reason why typical psychosocial interventions for social impairment fail with youth with ADHD (e.g., Hoza, 2007) may be due to a lack of a focus on ED. Techniques to improve the ability of individuals with ADHD to manage their emotional states during and after arousal may be a necessary addition to interventions targeting social impairment. Merging other treatments that directly target ED into interventions targeting social impairment may be beneficial. For example, mindfulness meditation may decrease emotional reactivity and improve emotion regulation (Teasdale, Segal, & Williams, 1995). In addition, dialectical behavior therapy (DBT) is a comprehensive treatment for ED (Linehan, Bohus, & Lynch, 2007) that has been successfully adapted for adolescents with bipolar disorder (e.g., Goldstein, Axelson, Birmaher, & Brent, 2007). Studies assessing the effectiveness of these or similar techniques in other populations have reported decreases in emotional reactivity (Linehan et al., 2007) and in impulsive and self-destructive behaviors during attempts to self-soothe (cf. Brown, Ryan, & Creswell, 2007). These changes, in turn, have measurable effects on ED (see Ivanovski & Malhi, 2007, for review). Some have applied these techniques to adults and adolescents with ADHD, although these investigators focused on symptom change without specifically addressing improvements in social functioning (Hesslinger et al., 2002; Zylowska et al., 2008). Although there are methodological limitations of these studies, their findings suggest that the integration of elements of mindfulness meditation and DBT, with treatments for social impairment, may enhance the impact of those treatments.
Limitations
The main limitations to this study pertain to those inherent in self-report. Adolescents with ADHD tend to over- and under-report the deficits they experience in diverse areas of performance (Owens et al., 2011). However, it has been argued that, given increased cognitive maturity and the largely internal and subjective nature of emotion regulation, self-report may be an appropriate measurement method with adolescents (Rohrbeck, Azar, & Wagner, 1991; Soto, John, Gosling, & Potter, 2008; Walden, Harris, & Catron, 2003). Nevertheless, youth may have limited awareness of some aspects of ED that may be critical to understanding its role in social functioning. Similarly, there are problems with the assessment of social functioning with adolescents as parents and teachers are less aware of adolescents’ social behavior than they are of children’s social behavior. These limitations emphasize the need for a multi-informant approach to assessment and call for future research to include sources of information beyond self-report to measure ED. Finally, the present data were obtained with a primarily Caucasian sample; therefore, replication of our findings with samples of varying ethnicity is important with respect to the generalizability of the reported effects.
Summary
In summary, our findings add to the literature and expand on previous findings by providing data on the role of ED in the social impairment of young adolescents with ADHD. Barkley (1997, 2010) argued that ED is a core deficit in ADHD. Our findings indicate that emotional inflexibility and a slow return to emotional baseline, a low threshold for emotional excitability, impatience, and socially inappropriate behaviors, and difficulty in behavioral control when experiencing negative emotions are exhibited by young adolescents with ADHD and these elements of ED are associated with social impairment. Regardless of whether ED is considered central to the disorder or not, our findings add to the evidence that ED is impaired in many youth with the disorder and associated with social impairment above and beyond the contributions of comorbid ODD. As a result, ED should be considered in intervention development for the social impairment of youth with ADHD to enhance their self-regulation of emotions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: During the preparation of this article, Nora Bunford was supported in part by a fellowship from the American Psychological Foundation (Elizabeth Munsterberg Koppitz Dissertation Fellowship). Steven W. Evans and Joshua M. Langberg were supported in parts by grants from the National Institute of Mental Health (5ROIMH082864) and Steven W. Evans by a grant from the Department of Education, Institute of Educational Sciences (R324C08006).