
Abstract
Epidemiology of MPH Prescriptions in Israel
ADHD is a major health problem affecting between 8% and 12% of children, and 4% of adults worldwide (Biederman & Faraone, 2005; Faraone, Sergeant, Gillberg, & Biederman, 2003; Kessler et al., 2005) and is the most common neurodevelopmental disorder of childhood. (Robison, Sclar, Skaer, & Galin, 1999; Rowland, Lesesne, & Abramowitz, 2002). A wide range of medications are used in the treatment of ADHD, among which the psychostimulant methylphenidate (MPH) is the most frequently prescribed in many locales, and is considered to be the first-line therapy by many clinicians (Robison et al., 1999; Schachter, Pham, King, Langford, & Moher, 2001).
Numerous studies have examined the efficacy of stimulants in ADHD and most have shown a response rate of 70%. Improvements have been observed in many areas of functioning, including inattentiveness, impulsiveness, and secondary low self-esteem. In recent years, there has been a significant increase in the diagnosis of ADHD, and in the use of prescription medications in the treatment of this disorder (Cox, Motheral, Henderson, & Mager, 2003; Greenhill, Pliszka, Dulcan, &American Academy of Child and Adolescent Psychiatry, 2002; Olfson, Gameroff, Marcus, & Jensen, 2003; Robison, Skaer, Sclar, & Galin, 2002; Safer, Zito, & Fine, 1996).
One regional survey performed in Germany in 2007 determined the overall prevalence of ADHD in all age groups (0-18 years) at 2.21%, 45% greater than the corresponding assessment for the year 2000. Figures increased by a larger degree among girls 6 to 18 years of age, than among boys in the same age group (Schubert, Köster, & Lehmkuhl, 2010). However, the overall prevalence of MPH use among children and adolescents in Germany was 1%, comparable to figures reported in other European countries including Switzerland (Huissoud, Jeannin, & Dubois-Arber, 2007), the Netherlands (Hugtenburg, Heerding, & Egberts, 2004), and Norway (Asheim, Nilsen, Johansen, & Furu, 2007). National prevalence rates tended to be higher for the United States (Habel, Schaefer, Levine, Bhat, & Elliot, 2005; Zuvekas, Vitiello, & Norquist, 2006) and Iceland (Zoëga, Baldursson, & Halldorsson, 2007).
Previous epidemiological surveys indicated that the willingness of primary care physicians, or consulting medical specialists, to prescribe psychostimulants in general, and MPH specifically, in the treatment of ADHD, depends to a significant extent on the community wherein the child resides (King et al., 2006). In the United States there exist striking differences in prescribing and dispensing practices between states as well as between counties (Singh, 2005). Factors such as socioeconomic status (SES), geographic location, and racial background have been shown to independently influence the likelihood of treatment with MPH (Brownell & Yogendran, 2001; King et al., 2006; Rowland et al., 2002).
The interest in prescribing patterns for MPH is multifold: MPH prescription patterns are an indirect barometer of diagnostic patterns of ADHD. Furthermore, prescription trends according to age, gender, and community status not only indicate social trends, but also target areas of concern for potential abuse of prescriptions, especially where dispensing trends exceed, or fall short of epidemiologically based expectations (Cohen, Jhung, & Budnitz, 2006; Dafny & Yang, 2006; Fone & Nutt, 2005).
Epidemiological data of ADHD and MPH prescribing in Israel is scarce. However, monitoring the prescription trends is an important step in delineating both patterns of access to medication, where the clinical need has been proven, as well as identifying potential overprescribing due to expediency, or possible abuse in different age groups, especially among adolescents.
The aims of the present study were to investigate the use of MPH among children in the central region of Israel, the pattern of prescribing the medication, and the demographic features of the users, as an indication of epidemiological trends in diagnosing ADHD, as well as a reflection of attitudes and practices among prescribing professionals vis-à-vis the use of MPH as a therapeutic avenue among different population groups.
Method
Details of all prescriptions for MPH filled from January 1, 2011, to December 31, 2011, in the Sharon-Shomron (S-S) and Dan-Petah Tikva (DPT) districts in the central region were drawn from the database of the Clalit Health Services, the largest health maintenance organization (HMO) in Israel, that insures approximately 70% of the population. The study included children aged 6 to 18 years of age, who were residents of those areas, and had received at least one prescription/year for MPH. Data for the years 2005 and 2007 of the S-S district were also obtained from the same database.
The geographical area of the study does, in fact, represent the general population of the country by virtue of the sheer numbers of insurees reviewed (the Clalit HMO encompasses 875,000 members of all ages in the two districts, representing 13% of the total population of Israel), as well as by dint of the variety of communities represented in the sample. Included in the area are five municipalities of over 200,000 inhabitants each (Ramat Gan, Bene Beraq, Petah Tiqva, Givatayim, Netanya), plus a myriad of smaller cities over 120,000 each (Ramatayim, Kefar Sava, Raanana, Herzliya, Taibe), along with a plethora of small suburban towns (Tira, Elad) and rural communities, including several kibbutzim, and the more numerous moshavim (comparable to rural villages and towns in the American South and Midwest, as well as in southern and central Europe). As such, the area is a microcosm of the country in general and reflective of outlying areas as well, where urban centers and upwardly mobile suburban areas with their local kibbutzim, few in number though relatively socially influential, set the tone in terms of social trends in preferential use of certain medications.
Prescriptions for MPH were chosen as a marker for the prevalence of ADHD/HD that is severe enough to warrant medication treatment. MPH remains the medication of choice by most prescribing professionals in the country and is the most readily available, at reasonable and contained cost, within the public health care system. The initiative to treat ADHD/HD during the course of the study remained the exclusive prerogative of pediatric neurologists, psychiatrists, and developmental specialists, whereas ensuing prescriptions were the responsibility of the primary care physician.
A prescription was defined as one package of 30 tablets. Each patient was included in the analysis only once, regardless of the total number of monthly prescriptions each had received. Other data extracted from the prescriptions were patient’s residential address, gender, and date of issue. Thirty-four percent were first time-prescriptions.
Data on the type of community (urban, suburban, and rural) in which the children resided were also obtained from the same database. SES of the population served by the community clinic was determined by the percentage of insured health service members receiving supplemental income remittances from the Social Security Administration. As many municipalities and neighborhoods in Israel tend to be homogeneous in composition along SES and ethnocultural lines, eight community clinics and their pharmacies were selectively studied in the DPT district as being representative of the different ethnic, SES, and religious communities.
Results
Of the 601,862 residents of the S-S district, insured by Clalit Health Services in 2011, 122,660 (20%) were between the ages of 6 and 18. Of these, 9,157 received prescriptions for MPH at an overall 1-year prevalence rate of 7.5% (Table 1). Calculations according to sector revealed that the rate was 7,630/67,587 (11%) in Jewish children and 1,413/55,917 (2.5%) in Arab children, a more than 4fold difference along ethnoreligious lines (Figure 1; p < .001; 114 medicated children were excluded).
The Percentage of Children and Adolescents (6-18 Years Old) Grouped by Sex and Age for Whom Methylphenidate Was Prescribed in the Years 2005, 2007, and 2011.
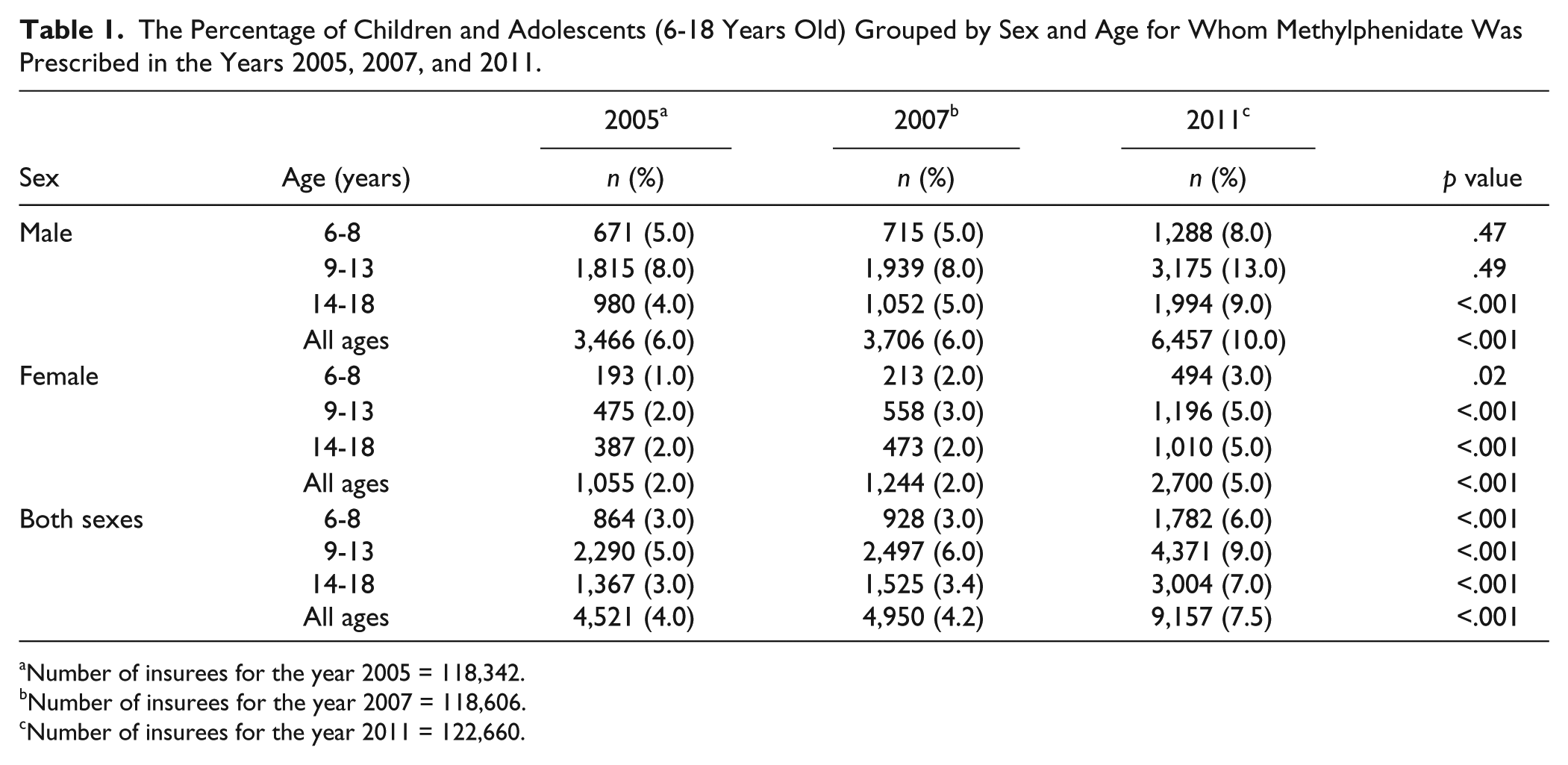
Number of insurees for the year 2005 = 118,342.
Number of insurees for the year 2007 = 118,606.
Number of insurees for the year 2011 = 122,660.

The percentage of insurees receiving methylphenidate prescriptions, according to age, gender, and ethnic group (2007 and 2011).
Calculation of prevalence according to gender showed that 10% of recipients of MPH prescriptions were males and 5% females, a 2-fold difference (Table 1). By comparison, the overall prevalence for the year 2007 was 4.2%. Among Jewish and Arab children, the prevalence was 6.9% and 0.9%, respectively, a 7.7-fold difference. Conversely, the overall prevalence for MPH prescriptions in the year 2005 had been 4% (among Jews: 6.3% and among Arabs: 0.7%, a 9-fold difference). Between the years 2007 and 2011, the overall prevalence rate of MPH prescriptions increased by 1.6-fold in males and 2.5-fold in females. From 2007 to 2011, the prevalence of MPH prescriptions among Arab females and males increased by 4-fold and 3-fold, respectively (Figure 1).
A comparison of the total percentage of 6- to 18-year-olds who were prescribed MPH in the years 2005, 2007, and 2011 showing the differential contribution according to age and gender is depicted in Figure 2.

The percentage of children and adolescents 6- to 18-years old who were prescribed methylphenidate according to age and gender in the years 2005, 2007, and 2011.
There was a significant increase from 5% to 9% (p < .001) in prevalence among males aged 14 to 18 years. The increase among females, 9 to 13 years of age, rose from 3% to 5% and at 14 to 18 years of age from 2% to 5% (p < .001). Across all ages and both genders, there was an overall increase in prevalence from 6% to 10% for males, and from 2% to 5% for females.
Prevalence for all age groups combined increased from 4.2% to 7.5%, an upsurge of 85%. The contribution to the increase was greatest in the 14- to 18-year-old age group, from 3.4% to 7%, representing a rise of 97% (Table 1).
The prevalence was also calculated separately according to the community of residence. In the S-S district, there are 24 kibbutzim and 63 moshavim (rural and communal-type settlements) where SES tended to be higher than that in most urban settings and social pressures more acutely felt, given the small community-type of social fabric. The S-S district also includes 7 predominantly Jewish cities, 14 predominantly Jewish towns, 14 predominantly Arab cities and towns, and 4 new rural Jewish locations, without official designation of their municipal status at the time the study was conducted. The rate of MPH prescriptions ranged from 18.9% for the kibbutzim compared with 2.5% in urban Arab settings, a 7.6-fold difference (Table 2).
Prevalence of Methylphenidate Use (During 2011) in 8,487 Children, Aged 6 to 18 Years, Residing in 126 Locations in the Central Region (Sharon-Shomron District) of Israel.

Primary care physicians issued most of the prescriptions, although many of the original recommendations for use of the medication were made by developmental pediatricians, psychiatrists, or neurologists.
Data from the DPT, a primarily urban area, was analyzed for 21,811 members between the ages of 6 and 18 years, out of a total of 55,434 insurees of all ages. These represented 15% of the total population of HMO insurees for the entire district, and had been arbitrarily selected for comparison purposes, due to the homogeneity of the SES and ethnoreligious characteristics of their respective neighborhoods (thus representing a potential bias factor in later epidemiological analyses). Of these, 1,117 received prescriptions for MPH, at an overall prevalence rate of 6% (6.8% and 2% among Jewish and Arab children, respectively, a 3.5-fold difference; Table 3).
Prevalence of Methylphenidate Use in Children Aged 6 to 18 Years in Selected Locations of the Dan-Petah Tikva District in Israel during 2011.
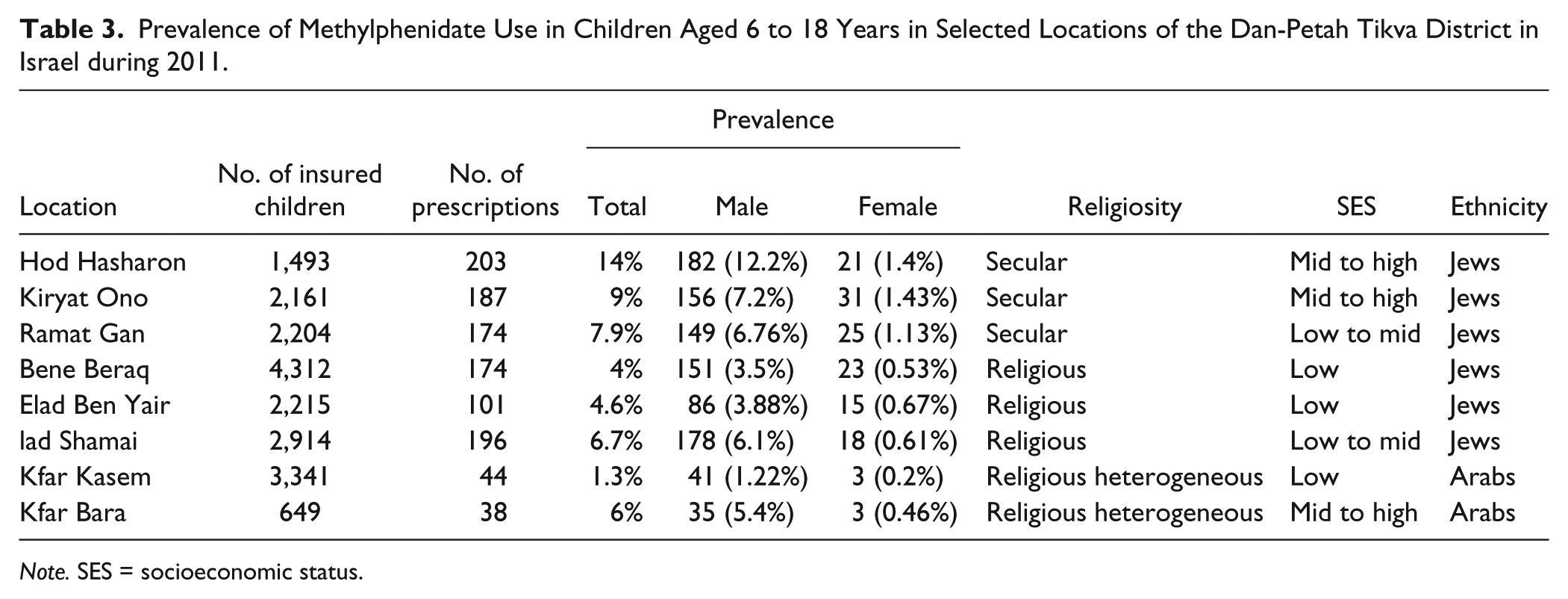
Note. SES = socioeconomic status.
Within each community of the DPT, possible correlation with SES background, degree of religiosity, and ethnicity was examined. The highest prevalence of MPH use was 14% for Hod Hasharon, a mid-high SES and secular locale. Within the Orthodox community, Elad Shamai, a low to mid SES area, the prevalence was 6.7% compared with Elad Ben Yair and Bene Beraq, both low SES neighborhoods, with 4.6% and 4%, respectively (p < .001). Within the Arab community, Kfar Bara, a mid to high SES locale, showed a prevalence of 6% compared with 1.3% for Kfar Kasem, a low SES rating (p < .001; Table 3).
Across the diverse ethnocultural divide, females were consistently undertreated, representing only 7% of the MPH-treated children in Kfar Kasem, the low SES Arab locale, compared with 10% of the total number of MPH-treated children in Hod Hasharon, the mid-high SES secular Jewish locale (p < .001). Female treatment prevalence figures have begun to catch-up in general, comprising 17% of all treated children in Kiryat Ono, another mid to high SES secular Jewish locale, and 15% for Elad Ben Yair, a low SES religious (Orthodox) neighborhood.
Discussion
The aims of the present study were to investigate the use of MPH among children diagnosed with ADHD, the trends over time regarding its use, and the demographic features of the users. There has been an enormous increase in the rates of diagnosis of ADHD, along with disparities in the use of medication in the treatment of this disorder. We hope that this study will contribute to a more equitable approach to the treatment of ADHD and its associated behavioral and learning disabilities among children in all communities, based on universally accepted clinical criteria. The issue constitutes an integral part of public policy discussion over the use of stimulants among the pediatric age group, both from a safety, as well as an educational and social point of view, especially with regard to the impact of overcrowded classrooms and availability of nonmedical educational and mental health services for children in the public school system (DeFelice, 2005).
Epidemiological studies from the United States using standardized diagnostic criteria suggest that approximately 3% of the school-age population is medically treated for ADHD (Greenhill et al., 2002). Our present study found an overall prevalence of 7% in the central, and most densely populated, urbanized area of the country.
The overall prevalence for MPH prescriptions was 4.0% and 4.2% for the years 2005 and 2007, respectively. Between the years 2007 and 2011, the overall prevalence rate of MPH prescriptions increased by 1.6-fold in males and 2.5-fold in females. A 4-fold increase in the prevalence of MPH prescriptions for Arab females and a 3-fold increase for Arab males was also observed between the years 2007 and 2011.
This rate is high compared with European figures, and high even for comprehensive data from previous studies in the United States (Habel et al., 2005; Zuvekas et al. 2006). Pharmacological treatment of ADHD in the United States and the United Kingdom has increased dramatically in recent years (approximately 2.5-fold; Rappley, Gardiner, Jetton, & Houang, 1995; Safer et al., 1996). Comparison of these statistics with the current rate in central Israel, together with figures published in 2007 for the same population (3.75%; Fogelman, 1999), yielded an increase of nearly 90%, making local rates comparable with the highest figures attained in select communities throughout the United Kingdom (McCarthy et al., 2012) and United States (Chai et al., 2012; Emanuel et al., 2013).
We found a significant difference in the proportion of medicated children among the different types of communities, as was the case between high SES Jewish males versus low SES Arab females. A similar study in Michigan (United States) reported a 10-fold disparity that the authors attributed to the wide range of prescription practices among physicians. This was supported by a U.S. national survey of the knowledge and attitudes of pediatricians regarding the diagnosis and treatment of ADHD (Kwasman, Tinsley, & Lepper, 1995) and by other studies as well (Wolrich, Lindgern, & Stromquist, 1990).
Moreover, differences in access to medical and mental health services may be an important factor. Cowart (1988) suggested that children with limited access to preventive health care services and to centers that assess behavioral and developmental problems may be underdiagnosed and undertreated. Accordingly, Zito and colleagues (Zito, Safer, dosReis, Magder, & Riddle, 1997) found that Afro-American youths were 2.5 times less likely to receive MPH than Caucasian youth. Safer and Krager (1988) reported that the higher the SES status, the greater the probability of stimulants being prescribed. In Zito, Safer, dosReis, and Riddle’s (1998) landmark pharmaco-epidemiological study of ADHD, Afro-American youths were also found to have relatively less access to psychotropic medications, thought to be due in part to similar religious and cultural attitudes, as among Israel’s Arab minority.
In our study, differences among diverse ethnocultural communities did not explain the enormous variation in MPH use. Data from the DPT region indicated an SES divide within each of the different communities (secular Jewish, ultra-orthodox Jewish, and Arab), where the more affluent child health care centers registered more dispensing of MPH. Rather, there appears to be an additive/cumulative effect resulting from other factors as well. The SES factor interacts with culturally based attitudes, and factors shaping the pediatricians’ willingness to issue prescriptions in response to both consumer demands and public expectations. These appear to affect primarily the criteria judged as sufficient to induce initiation of treatment with medication (approximately 34% of the prescriptions listed were for first-time use). Of special interest in our study were the implicit attitudes toward the most underprescribed pediatric groups, namely, females, in all the communities under study, where the presenting symptoms were less disruptive behavior, and more dysfunctional learning. The greater tendency to treat males within the same cultural and socioeconomic group reflects similar findings in a previous study by Angold and Costello (2000).
The enormous increase in diagnosed ADHD, and the inclination to medically treat over the past 4 years, since the last epidemiological survey was conducted in Israel, appears to be at variance with the conclusions drawn regarding the meta-analysis of worldwide prevalence trends for ADHD/HD as outlined in the study by Polanczyk et al. (Polanczyk, Silva de lima, Lessa Horta, Biederman, & Rohde, 2007), where variability was primarily attributed to methodological differences in the studies assessed. Here, there appears to be at work a combination of local factors, namely, increasing class size and decreasing investment in the public school system with attendant reduction in pupil-based services, as well as more worldwide trends related to globalization: The shift to greater emphasis on competition to succeed within an information-based economy, higher consumer awareness of medical treatment options, and a greater acceptance of pharmacotherapy for children (Fogelman & Kahan, 2001; Organisation for Economic Co-Operation and Development, 2011; Levi, 2010).
With regard to the impact of SES and its influence on the public’s ability to afford the variety of medications available, it should be noted that within the public health care system in which the survey was conducted, the cost of generic MPH (as opposed to the variety of long-acting varieties available on the market) is nominal and did not constitute a barrier to medication use or availability. Rather, SES appeared to play a role in enabling access to a greater variety of stimulant medications, with their increased efficacy and potential attractiveness for the consumer. Therefore, SES did not constitute an absolute barrier to medication use, but rather a relative one, which interacted effectively with cultural and physician dispensing pattern factors.
Limitations and Benefits
One limitation of this study is that it is based on data from a single HMO, albeit the largest in the country. In addition, the public health system is home to three other health service delivery organizations, governed by medication dispensing policies of their own, in accordance with government regulations. Conversely, one of the benefits of this study is that the nonrestrictive nature of the database enabled the study to be performed without a priori limitation, including recall or refusal bias.
It should be noted that the study was based on dispensing patterns, including cases of even one prescription per subject, at best, and not on the actual diagnosis of ADHD, or even on clinicians’ recommendations for treatment. Whereas cases of single prescriptions were inevitably part of the total dispensing data, in the overall prevalence data they were expected to be balanced out by unaccounted for prescriptions at private pharmacies and considered to carry negligible weight at best. Similar studies indicated that the diagnosis of ADHD, as well as the actual use of MPH, significantly exceed the official dispensing figures from public, as opposed to private pharmacies, suggesting loopholes in the actual access to strictly regulated medications, such as psychostimulants (Schubert et al., 2010).
Conclusion
The use of medication in the treatment of ADHD in the pediatric age group is a function not only of medical judgment and diagnosis, but of community cultural attitudes and practices, with a clear SES and gender divide within each community, in favor of higher SES and male gender. The reasons for these differences vary and still need to be more fully investigated. Where costs are contained, and there is easy access to uniformly good primary medical care, the decision to medically treat appears to be the additive result of a combination of the factors. It appears the worldwide trend favors increased reliance on medication, with variations in prevalence according to the peculiarities of the different locales.
This study highlights two important questions: (1) Are these increasing general trends a sign of a basic flaw in the social fabric, or in the educational system, or rather an indication of improved overall awareness of ADHD? (2) Are the children at the extreme ends of the accessibility spectrum a cause for concern, namely, undertreatment due to social and cultural attitudes, especially for low SES and female gender, and is overtreatment or possible abuse, especially by high SES adolescents in cases where upwardly mobile pressures exist for achievement in school, requiring optimal attention and stamina levels over extended periods of time?
Footnotes
Acknowledgements
The authors thank Miss Keren Edri Maman for providing vital resources, Miss Haneen Jbali for her secretarial assistance, and Miss Pearl Lilos for statistical analysis.
Authors’ Note
This article was accepted as a Poster Presentation at the Third Global Congress for Consensus in Pediatrics & Child Health (CIP), Bangkok, Thailand, February 13-16, 2014, and the abstract was awarded First Prize at the Fourth European Confederation of Primary Care Paediatricians (ECPCP) Conference, Tel Aviv, Israel, 3-5 July, 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.