
Abstract
Introduction
ADHD and autism spectrum disorder (ASD) are both a collection of childhood-onset neurodevelopmental disorders. They are classified as distinct disorders within The ICD-10 International Classification of Mental and Behavioural Disorders (ICD-10; World Health Organization, 1992) and Diagnostic and Statistical Manual of Mental Disorders (5th ed., DSM-5; American Psychiatric Association, 2013) diagnostic classification systems. ADHD is characterized by severe inattention, hyperactivity, and impulsivity, whereas ASD is characterized by impaired communication and social interaction skills, as well as repetitive and restricted behavior and interests. Both disorders are substantially more common in boys than in girls, with a male:female ratio of around 4:1 on average (Rutter, Caspi, & Moffitt, 2003). The consistency of this observation across time and study populations suggests the involvement of sex-specific biological risk factors in the etiology of both disorders. Importantly, ADHD and ASD also show remarkably high co-occurrence with each other, at trait and full disorder level. Accumulating evidence indicates that 20% to 50% of children with ADHD are meeting criteria for ASD and 30% to 80% of children with ASD are meeting criteria for ADHD (Rommelse, Franke, Geurts, Hartman, & Buitelaar, 2010). In addition, ADHD and ASD have yielded some overlapping findings with respect to brain magnetic resonance imaging (MRI; Brieber et al., 2007) and cognitive correlates (Rommelse, Geurts, Franke, Buitelaar, & Hartman, 2011). These findings support the idea that there are some common genetic influences operating across autistic traits and ADHD behaviors throughout normal variation as well as at the extreme (Carlsson et al., 2013). Indeed, James (2008b) argued that elevated intrauterine testosterone levels may be partially involved in the development of both disorders.
The existence of sex biases points to certain causal factors, such as genes and hormones (Baron-Cohen et al., 2011). Understanding the basis for the male:female ratio may be an important step toward understanding the etiology of the disorder (Rutter et al., 2003) and has the potential to advance theories of child psychopathology (Zahn-Waxler, Shirtcliff, & Marceau, 2008).
One major theory that invokes a role for testosterone in ASD etiology in particular is the Extreme Male Brain (EMB) theory of autism. Prenatal testosterone has an effect on cerebral organization and lateralization in the developing brain and is often implicated in the etiology of behaviors and diseases. The EMB theory proposes that ASD arises from hypermasculinization of the brain (Baron-Cohen, 2002; Baron-Cohen & Hammer, 1997; Baron-Cohen, Knickmeyer, & Belmonde, 2005). The theory has been proposed as a possible explanation for the predominance of males to females in ASD. It suggests that people with an ASD display an extreme of the typical male pattern of systemizing skills (females tending to have stronger empathic ability), and that exposure to high levels of prenatal testosterone may be one risk factor among other contributing factors. Results from the ongoing longitudinal Cambridge Fetal Testosterone project have demonstrated that fetal testosterone levels measured in women who had amniocentesis for other reasons were associated with a number of autistic traits in their offspring (Auyeung et al., 2009).
Direct measures of prenatal testosterone are not normally available and a number of indirect biomarkers for prenatal testosterone exposure and sensitivity have been employed in all but The Cambridge Fetal Testosterone project.
One often used potential indirect or proxy measure of steroid hormone exposure is the relative length of the phalangeal digits. The ratio of the second to fourth finger length (i.e., 2D:4D ratio) is significantly lower (more masculine) in males than in females from infancy onward, and the ratio 2D:4D is, therefore, considered a useful indirect marker of prenatal testosterone exposure during critical neurodevelopmental phases of fetal life (Manning, Scutt, Wilson, & Lewis-Jones, 1998). A low 2D:4D ratio may indicate the fetus was exposed to a high level of prenatal testosterone. Equally, a high 2D:4D ratio may indicate low prenatal level of testosterone. A meta-analysis of seven studies comparing the 2D:4D digit ratio showed that 2D:4D ratio was substantially lower in people diagnosed with ASD than in normal controls (Hønekopp, 2012).
Relatedly, a number of articles have reported associations of low 2D:4D with various ADHD subtypes in children (De Bruin, Verheij, Wiegman, & Ferdinand, 2006; Martel, Gobrogge, Breedlove, & Nigg, 2008; McFadden, Westhafer, Pasanen, Carlson, & Tucker, 2005; Stevenson et al., 2007). In a review dealing with potential hormonal mechanisms of ADHD, Martel, Klump, Nigg, Breedlove, and Sisk (2009) concluded,
Taken together, research on finger-length ratios may suggest that prenatal testosterone exposure is positively related to ADHD symptoms, at least in boys, and possibly to correlated traits such as externalizing problems and sensation seeking. Thus, there is some support for the hypothesis that prenatal levels of testosterone are positively correlated with ADHD symptoms. (p. 471)
In keeping with the EMB theory of autism, James (2008a) has hypothesized that mammalian (including human) sex ratios (the proportion of males) at birth are partially controlled by parental hormone levels around the time of conception; higher parental levels of testosterone (and concomitant lower levels of estrogen) being associated with a higher proportion of male offspring. Hence, it might follow that, if a neurodevelopmental disorder (e.g., ADHD or ASD) were at least partially caused by high intrauterine testosterone level, then that disorder would be expected to occur more frequently in males.
Testosterone levels in women tend to persist across time (Apter & Vihko, 1990), and sex ratios may be potential consequences of hormone profiles that existed when the children were conceived. If the sibling sex ratio was significantly raised, too, this would constitute indirect evidence for the hypothesis that mothers of people with early onset neurodevelopmental disorders are predisposed to produce both the disorder and children of the male sex (James, 2008a).
The suggestion that mothers of children with ASD might be higher in testosterone is supported by the study of Ingudomnukul, Baron-Cohen, Wheelwright, and Knickmeyer (2007). The authors found that both females with ASD and their mothers reported increased incidence of testosterone-related diseases.
James (2008b) has called attention to the relevance of studying the sex ratio of the sibs of individuals with neurodevelopmental disorders, arguing that sibling sex ratio is a proxy variable for parental testosterone at the time of conception. In addition, he collected data about sibling sex ratios from a number of earlier published studies dealing with different neurodevelopmental disorders, including ASD and ADHD. In both disorders, James found a higher (but non-significant) sex ratio in siblings: 0.525 (p = .24) and 0.539 (p = .12), respectively, compared with a U.S. live birth sex ratio of 0.512 over the same period, suggesting that intrauterine testosterone may be involved in the etiology of both disorders.
In the present study, we want to expand on that earlier study by studying a larger and population-based cohort. Based on the outlined literature, we hypothesized that a diagnosis of ADHD is associated with an elevated sibling sex ratio compared with the live sex birth ratio in the Danish population over the relevant years. In addition, we predicted that this male preponderance is particularly pronounced in full siblings of people with a diagnosis of ADHD.
Participants and Method
Study Population and Procedures
The study was based on data from two nationwide registers: The Danish Psychiatric Central Register (DPCR; Mors, Perto, & Mortensen, 2011) and The Danish Civil Registration System (DCRS; Pedersen, Gøtzsche, Møller, & Mortensen, 2006).
The DPCR contains computerized cumulative data on all admissions to Danish psychiatric, including child and adolescent, inpatient facilities from 1969. From January 1, 1995, information on outpatient visits to psychiatric departments and emergency rooms were included in the register. There are no private psychiatric inpatient facilities in Denmark, ensuring that all psychiatric admissions are represented in the register. The diagnostic classification used until December 31, 1993, was ICD-8. Beginning January 1, 1994, the ICD-10 classification was used. The clinical diagnosis of ADHD reported to the DPCR is usually applied by teams consisting of specialists in child and adolescent psychiatry, psychologists, psychiatric nurses, and educators using clinical assessments in accordance with internationally standardized procedures.
First, we retrieved all people registered in the DPCR until May 28, 2013, with a main or subsidiary ICD-10 diagnosis of ADHD (i.e., ICD-10 code F90.0), and who were less than 18 years old at diagnosis. The individuals’ personal identification number identified each person. The personal identification number enables accurate linkage of information between registers at the individual level. We found 16,381 individuals with ADHD (12,669 males and 3,712 females) who had a valid personal identification number, and these 16,381 people make up the patients in our study population. The patients were born between 1977 and 2011.
Table 1 presents the characteristics of the 16,381 individuals with ADHD with respect to age at time of diagnosis and by end point of the study (i.e., May 28, 2013), gender, and male:female ratio.
Characteristics of 16,381 Individuals Known With an ICD-10 Diagnosis of ADHD (F90.0) in the Nationwide Danish Psychiatric Central Register by May 28, 2013.
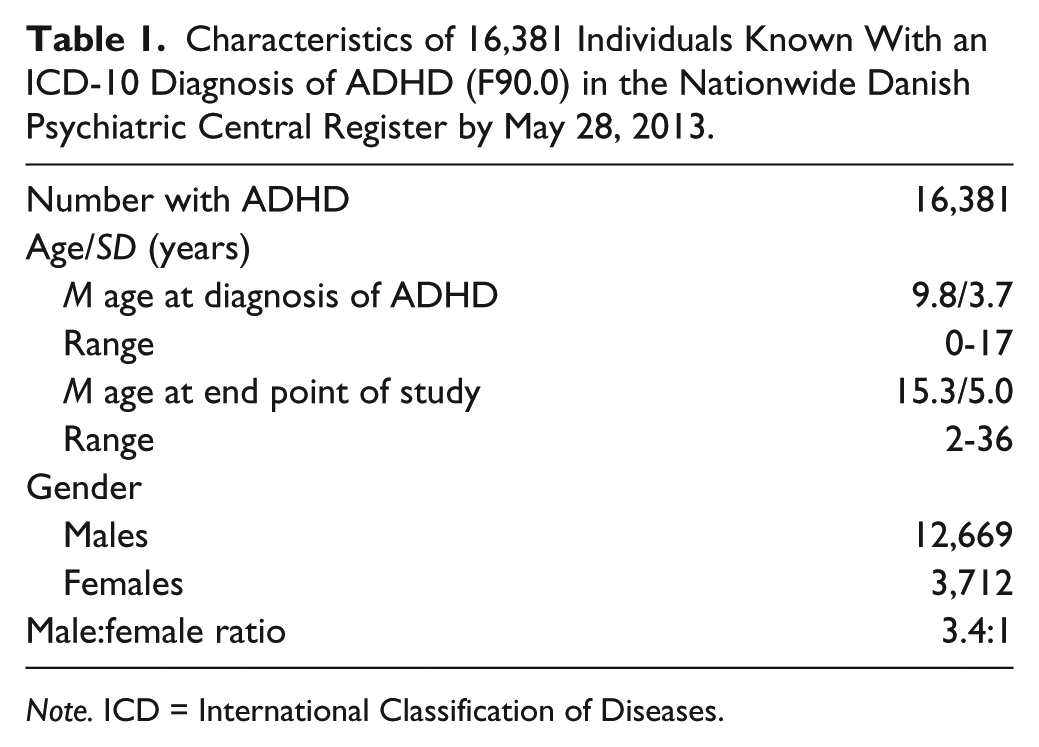
Note. ICD = International Classification of Diseases.
Second, information on the number of full and half siblings were retrieved from the DCRS by linking the 16,381 patients’ personal identification number. The DCRS was established in 1968 where all persons alive and living in Denmark were registered in the DCRS. From that time, all live-born children and new residents in Denmark have been assigned a unique personal identification number, which is stored in the DCRS along with information about place and time of birth, gender, vital status, address, and personal identification number of family members (i.e., parents, children, and siblings). We found 33,151 siblings (17,041 males and 16,110 females), and these siblings make up our study population. Details about the 33,151 retrieved siblings with respect to the number and gender of full and half siblings and sex ratio (proportions of males) are presented in Table 2.
Gender and Sex Ratio of 33,151 Full and Half Siblings of 16,381 Patients Registered With an ICD-10 Diagnosis of ADHD (F90.0) in the Nationwide Danish Psychiatric Central Register Between January 1, 1994 and May 28, 2013.
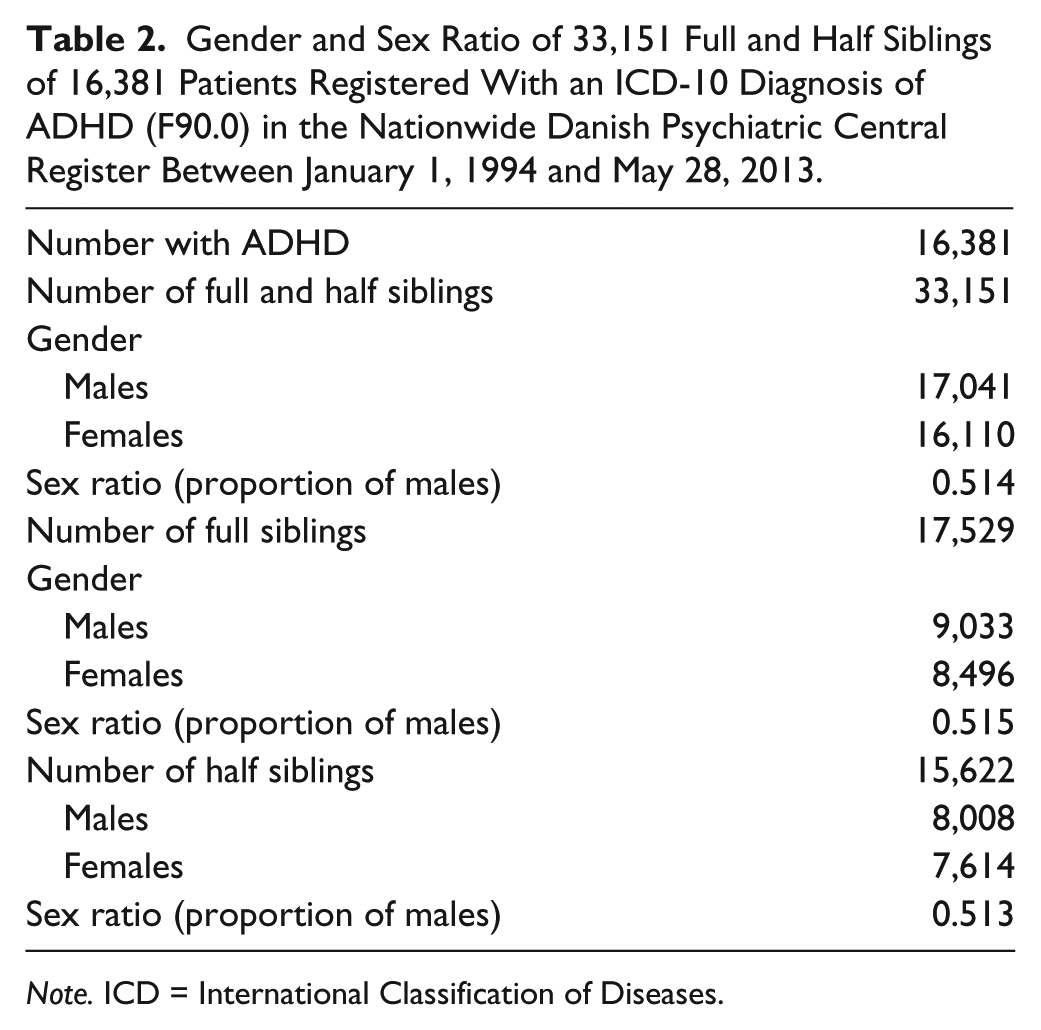
Note. ICD = International Classification of Diseases.
Statistical Analysis
The statistical analysis program STATISTIX (Analytical Software, 2006) was used for data handling and analysis. The sex ratio of siblings of patients with ASD was compared with the Danish live birth sex ratio of 0.513 during the relevant years (i.e., 1977-2011) by performing chi-square goodness of fit tests. A probability level of .05 was used to indicate significant differences.
Ethics
The Danish Data Inspectorate approved the study protocol.
Results
Details of the sex ratios in the siblings of individuals with ADHD are given in Table 2. As can be seen the sex ratio varies between 0.513 (half siblings) and 0.515 (full siblings), against the comparable Danish live birth sex ratio of 0.513 (sex ratio range between 0.509 [2011] and 0.517 [1987]) during the relevant years (Danish Bureau of Statistics, 1977-2011).
Observed and expected number of male and female siblings is summarized in Table 3. In considering all 33,151 full and half siblings, we found a sibling sex ratio of 0.514. This is not statistically significant different (p = .70) from the comparable Danish live birth sex ratio of 0.513 during the relevant years. If the analysis is restricted to the 17,529 full siblings only, the sibling sex ratio is 0.515 (p = .54). If the 15,622 half siblings are analyzed separately, we found an even smaller difference (p = .92). The sibling sex ratio is 0.513, which is similar to the Danish live birth sex ratio during the relevant years. Taken as a whole, our results indicate that a diagnosis of ADHD was not associated with an increased sibling sex ratio.
Observed and Expected Number of Full and Half Siblings of 16,381 Individuals With ADHD.
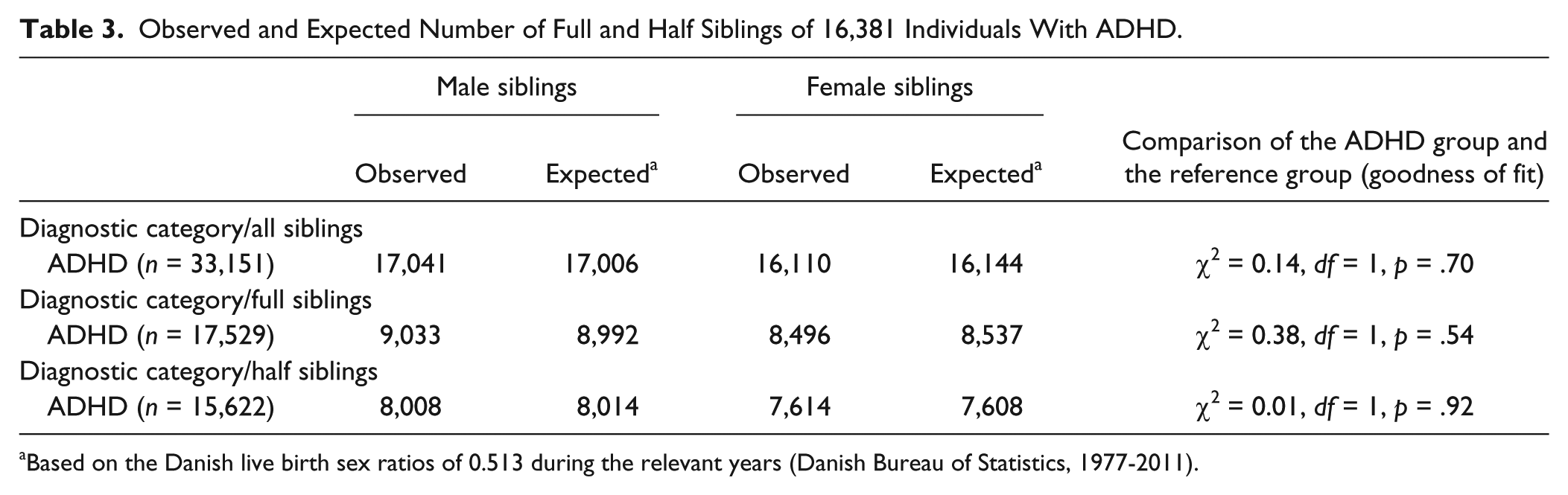
Based on the Danish live birth sex ratios of 0.513 during the relevant years (Danish Bureau of Statistics, 1977-2011).
Discussion
In Western industrialized countries, the human sex ratio at birth is strikingly stable, seldom varying significantly from values that lie roughly between 0.505 and 0.520 (James, 2008a). Thus, in almost all human populations, there is a slight excess of males at birth. The factors behind this male excess have not been fully elucidated.
Males are more likely to develop ADHD than females (Rutter et al., 2003). Although this male preponderance is not unique to ADHD, it has been taken as an important pointer toward possible biological etiologies of ADHD (Rutter et al., 2003). Early exposure to increased levels of prenatal testosterone has received much attention as a possible biological mechanism contributing to ASD (Auyeung et al., 2009) and ADHD (Martel et al., 2009).
The aim of the current study was to add to our understanding of potential sex differences in siblings of people with ADHD. If the hypothesis of high parental levels of testosterone at the time of conception is correct, then individuals with ADHD could have an excess of brothers among their siblings (James, 2008b). Accordingly, the sibling sex ratio of people with ADHD could then serve as a marker of increased parental testosterone level around conception.
In science, results must be repeated before a finding can be accepted as well established. In the present study, our aim was to replicate and expand on the earlier pioneering study of James (2008b) by including a larger and nationwide cohort. James (2008b) included 998 siblings (430 males and 368 females) of people with ADHD in his study and found an elevated, but non-significant sibling sex ratio of 0.539.
In our cohort of 33,151 full and half siblings (17,041 were males and 16,110 females), we found a sibling sex ratio of 0.514. This is higher but not significantly different (p = .70) from the comparable Danish live birth sex ratio of 0.513 during the relevant years (i.e., 1977-2011). If the analysis is restricted to the 17,529 full siblings, the result remains unchanged. Sibling sex ratio was 0.515 and p = .54. Contrary to our hypothesis, but in congruence with the result in the study of James (2008b), we found that individuals with ADHD do not have a statistically significant excess of brothers among their siblings. In this connection, it is important to emphasize that our results should not be taken as a strong argument against the EMB theory but could be interpreted as a strong disconfirmation of the existence of the studied indirect association (elevated sibling sex ratio).
Methodological Issues
Our study has several strengths in relation to the population studied. First, our results are based on a large nationwide cohort of people diagnosed as children and adolescents with ADHD, which is thought to be representative of the population of people with ADHD in Denmark. Second, the use of registers ensures prospective, uniformly and neutrally collected data, which restrict the methodological problems of loss to follow-up and selection bias. It is a major strength of our study that by using data from the DCRS, we have complete information about all siblings.
A limitation of our study is related the fact that only a small number of variables (full, half, and all siblings) could be included in the analysis. In future studies, it would be of interest not only to include people with an ICD-10 diagnosis of disturbance of activity and attention, corresponding to ICD-10 code F90.0 but also ADHD/hyperactive impulsive type and ADHD/inattentive type, since McFadden et al. (2005) found that the Combined and Inattentive type may be conceptualized as different disorders, not versions of a single disorder. Another potential limitation of our study is that the validity of the data retrieved from the DPCR is unknown. The ADHD diagnosis reported to the DPCR is a clinical diagnosis and is not always based on systematic child and adolescent psychiatric assessment with standardized instruments. Diagnoses result from heterogeneous assessments carried out by specialists in child and adolescent psychiatry throughout Denmark. However, for the diagnoses of schizophrenia (Uggerby, Østergaard, Røge, Correll, & Nielsen, 2013), affective disorder (Kessing, 1998), and childhood autism (Lauritsen et al., 2010) studies have validated the clinical diagnosis in DPCR against research criteria diagnoses. The results showed high agreement between the diagnoses. Although not comprehensive or definitive, these results support the belief that, in general, the validity of the reported diagnoses in the DPCR is good.
To summarize, this study extended a recent pioneering study examining the sex ratio in siblings of people with ADHD. In the current study, we found no evidence to support the hypothesis that the sex ratio is elevated in siblings of people with ADHD, neither with respect to full or half siblings. Accordingly, taking into account the large and nationwide number of siblings analyzed in the present study and the lack of association found, we conclude that our results do not support the hypothesis that the sex ratio is elevated in siblings of people with ADHD. But our study is not able to elucidate whether the explanation for our negative result is that sibling sex ratio is an invalid measure for parental testosterone or can be taken as a (indirect) falsification of the EMB theory.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.