
Abstract
The overall purpose of the present study is to explore the romantic relationships of adolescents with ADHD. Romantic relationships are a hallmark of adolescence (Collins, Welsh, & Furman, 2009). By late adolescence, more than 70% of teens have been involved in at least one romantic relationship (Carver, Joyner, & Udry, 2003; Furman, Low, & Ho, 2009) and rely primarily on their romantic partner, rather than their peer group, for support (Kuttler & La Greca, 2004). Romance is also at the forefront of adolescents’ minds; they spend between 5 and 8 hr each week thinking about actual or potential romantic partners (Richards, Crowe, Larson, & Swarr, 1998). These proportions are considerably larger than those attributed to school, peers, and family (Brown, 1999). Until recently, however, adolescent romance had not garnered much interest from the scientific community.
Currently, empirical studies of romantic relationships in adolescence are burgeoning. No longer are these relationships erroneously viewed as trivial and ephemeral. Instead, they are increasingly regarded as a significant factor in adolescent development and subsequent adult functioning (Giordano, Manning, & Longmore, 2006). Healthy romantic relationships may buffer negative outcomes and are associated with several positive aspects of development, including forming a personal identity, promoting harmonious relationships with peers, adjusting to changes in family relationships, shaping positive romantic relationships in adulthood, and lowered levels of adult psychopathology (e.g., Furman & Collins, 2008; Wolfe, Jaffe, & Crooks, 2006). Poor-quality romantic relationships, however, have been linked with alcohol and drug use, exposure to violence in relationships, increases in externalizing and internalizing symptomatology, academic underachievement, and an inadequate rubric for adult relationships (e.g., Woodward, Fergusson, & Horwood, 2002; Zimmer-Gembeck, Siebenbruner, & Collins, 2004). While the last decade has seen a marked increase in the number of studies examining the romantic relationships of typically developing (TD) adolescents, less is known about the nature of romantic relationships in adolescents with various psychopathologies such as ADHD.
When compared with other youth, the presence of ADHD in childhood and adolescence is associated with disturbances in family functioning, peer rejection, and lower quality friendships (e.g., Bagwell, Molina, Pelham, & Hoza, 2001; Johnston & Mash, 2001; Wehmeier, Schacht, & Barkley, 2010). Moreover, adolescent experiences with parents and peers are important precursors of romantic relationship quality in young adulthood (Connolly, Furman, & Konarski, 2000; Seiffge-Krenke, 2003). Individuals with ADHD tend be forgetful, disorganized, distracted, and fail to meet their responsibilities. In addition, they may be more impulsive, explosive, and more likely to have verbal and physical outbursts than their TD peers (Barkley, 2006). It is therefore not unreasonable to expect that such characteristics and behaviors may detrimentally affect their romantic relationships. Nevertheless, the link between romantic relationships and individuals with ADHD has received little empirical attention to date and even less is known about the romantic relationships of adolescents with ADHD.
The study of romantic relationships in adolescence has been hindered by a number of methodological challenges, including operational definitions, obtaining representative samples, and identifying the relevant dimensions of variation in romantic relationships (Collins et al., 2009). To facilitate assessments of romantic relationships, Collins (2003) identified several features that characterize romantic relationships in adolescence: romantic involvement, partner identity, relationship content, relationship quality, and cognitive and emotional processes in the relationship. The present study entails a comparison of adolescents with and without ADHD on three of these features: romantic involvement, relationship content, and relationship quality.
Romantic Involvement
Romantic involvement refers to whether or not a person dates, the frequency and regularity of their dating, and the duration of their relationships (Collins, 2003; Collins et al., 2009). The timing of the initiation of dating is important because early dating is closely associated with early sexual initiation (Cooksey, Mott, & Neubauer, 2002), which in turn is correlated with risky sexual behavior (RSB), depression, violence, academic underachievement, and substance use (Crockett, Bingham, Chopak, & Vicar, 1996).
There is some evidence that the romantic involvement of young adults with ADHD differs from typically functioning adults. Canu and Carlson (2003) found that college students with the inattentive subtype (ADHD-I) achieved dating milestones later and had a lower number of steady dating relationships, than both college students with the combined subtype (ADHD-C) and healthy college students. Similarly, Babinski et al. (2011) reported that when compared with typically functioning peers, girls diagnosed with ADHD in childhood experienced fewer romantic relationships in late adolescence and young adulthood.
Relationship Content
Relationship content refers to the shared activities of relationship partners (Collins, 2003; Collins et al., 2009). Adolescents in romantic relationships engage in patterns of interaction that differ from interactions with parents or peers. Two aspects of relationship content that have garnered considerable attention are sexual behavior and aggression between partners. Although many adolescent couples are in healthy and supportive relationships, physical aggression occurs in a sizeable proportion of adolescent romantic relationships. Estimates vary widely across samples (e.g., national vs. regional surveys) and assessment methods (one-time retrospective vs. cumulative), but roughly 10% to 48% of adolescents experience physical aggression and 25% to 50% endure psychological aggression in their dating relationships (Halpern, Oslak, Young, Martin, & Kupper, 2001; Jouriles, McDonald, Garrido, Rosenfield, & Brown, 2005). Young adults with ADHD have been found to resort to more frequent negative conflict resolution patterns (Canu & Carlson, 2007; Overbey, Snell, & Callis, 2011) and to be more verbally aggressive and violent in their romantic relationships (Wymbs et al., 2012) than young adults without ADHD.
Existing research on the sexual behavior of individuals with ADHD focuses on young adults and exposes some alarming tendencies. When compared with age-matched peers, young adults with ADHD are at an increased risk for unwanted pregnancies, sexually transmitted infections (STIs), earlier initiation of sexual activity, and a greater frequency of casual sex and sexual partners (Barkley, Murphy, & Fischer, 2010; Flory, Molina, Pelham, Gnagy, & Smith, 2006; Huggins, Rooney, & Chronis-Tuscano, 2012; White & Buehler, 2012; Winters, Botzet, Fahnhorst, Baumel, & Lee, 2008). Such RSB has been linked to sexual victimization in both the general population (Fargo, 2009) and in adolescents with ADHD (White & Buehler, 2012). Other studies, however, have found no significant associations between ADHD symptomatology and RSB when co-occurring conduct disorder (CD) is taken into account (Monuteaux, Faraone, Gross, & Biederman, 2007; Ramrakha et al., 2007). Mixed results also exist with respect to antisocial sexual activities (e.g., forced sex) among adults diagnosed with ADHD in childhood. Mandell (1999) and Theriault and Holmberg (2001) found ADHD symptomatology and CD to be small but significant predictors of both physical and sexual aggression; however, Barkley, Fischer, Smallish, and Fletcher (2004) did not find any such association. Although these inconsistent findings appear puzzling, they most likely reflect methodological variability across studies, such as differing sample characteristics (e.g., gender, population-based vs. clinic-referred) and assessment methods (e.g., structured interviews, self-report).
Relationship Quality
Relationship quality refers to the manifestation of affection and nurturance to create generally beneficial experiences (Collins, 2003; Collins et al., 2009). Evidence suggests that the skills necessary for establishing and maintaining friendships in childhood serve as the building blocks for establishing high-quality romantic relationships later in life (Collins, Hennighausen, Schmit, & Sroufe, 1997). Furthermore, the quality of peer and family relationships early in life significantly predicts the quality of ensuing romantic relationships (Collins & Van Dulmen, 2006; Roisman, Booth-LaForce, Cauffman, & Spieker, 2009). Low-quality relationships are marked by irritation, controlling behavior, antagonism, high levels of discord, and an imbalance between conflict and support (Galliher, Welsh, Rostosky, & Kawaguchi, 2004). High-quality relationships, however, are associated with a high level of commitment, feeling appreciated, good communication, and being attracted to the partner (Levesque, 1993). Although interactions with romantic partners involve more conflict than with friends and less responsiveness and communication than with mothers, adolescents perceive themselves as receiving more support from their partners (Furman & Shomaker, 2008).
To date, the quality of romantic relationships of individuals with ADHD has only been studied in adults. Spouses of adults with ADHD, who themselves are not diagnosed with ADHD, report feeling resentful and overwhelmed due to inadequate emotional support and an unequal distribution of household tasks pertaining to planning, organizing, financial decisions, and maintaining family harmony (Robin & Payson, 2002; Weiss, Weiss, & Trokenberg-Hechtman, 1999). Thus, it not surprising that, when compared with controls, ADHD status is associated with lower relationship satisfaction and a higher incidence of divorce (Biederman et al., 1993; Murphy & Barkley, 1996).
Rationale and Purpose of the Current Study
Collectively, the findings described above paint a bleak picture of romantic relationships in individuals with ADHD, with most of the existing research involving adult current or retrospective report. Adolescence, however, represents a period of flexible change and somewhat of a blank slate for individuals who have yet to experience a romantic relationship. Hence, it is evident that an additional emphasis should be placed on the exploration of adolescent relationships, as they represent the foundation for romantic relationships throughout the life span (Collins & Sroufe, 1999).
The major purpose of present study was to compare the romantic relationships of adolescents with and without ADHD on the following three relationship features: (a) romantic involvement, (b) relationship content, and (c) relationship quality. With regard to romantic involvement, based on previous studies (Babinski et al., 2011; Canu & Carlson, 2003), it was expected that adolescents with ADHD would commence dating later and have fewer and shorter-lasting relationships than their TD peers. In spite of commencing dating later in life, it was anticipated that the increased impulsivity of adolescents with ADHD may lead them to engage in sexual activity at a younger age and with more partners outside the context of an ongoing romantic relationship, than teens without ADHD. Based on previous research on adults with ADHD (e.g., Barkley et al., 2010; Canu et al., 2007; Flory et al., 2006; Overbey et al., 2011; Wymbs et al., 2012), differences between adolescents with and without ADHD were anticipated on measures of relationship content and quality. When in relationships, it was predicted that adolescents with ADHD would report higher levels of dissatisfaction, conflict, and aggressive behaviors (verbal, relational, sexual, physical), and lower levels of affection and nurturance than TD adolescents. Finally, it was also expected that adolescents with ADHD would report higher levels of RSB (e.g., unprotected sex, unwanted pregnancies, promiscuity, intercourse while using drugs or alcohol, and STIs) than TD adolescents.
Method
Participants
A community sample of 30, 13- to 18-year-old adolescents with ADHD (40% female [n = 12]; Mage = 15.71, SD = 1.49) and 28 TD peers (57% female [n = 16]; Mage = 16.0, SD = 1.68) were recruited by distributing flyers to a select number of schools in the Greater Toronto Area (n = 2), children’s mental health centers (n = 9), family doctors and psychologists (n = 3), advertisements in newspapers (n = 2), and phoning research participants from previous studies who had consented to be contacted regarding future studies (n = 42). Flyers informed participants that they would be filling out questionnaires about their peer, family, and romantic relationships. All participants were in Grades 7 through 12 with average intellectual ability (IQ ≥ 85) as assessed by the Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler, 1999). Eligibility criteria for the ADHD sample included (a) a parent-report of a previous diagnosis of ADHD from a physician or psychologist, based on Diagnostic and Statistical Manual of Mental Disorders (4th ed.; text rev.; DSM-IV-TR; American Psychiatric Association, 2000) criteria; and (b) at least one clinically significant score (T ≥ 70) on the DSM-IV-TR ADHD scales of the parent form of the Conners–3rd Edition (Conners, 2008); or (c) at least one borderline range score (T = 65-69) on the DSM-IV-TR ADHD scales of the parent form of the Conners, and at least one score on the same scales by another informant (self-report or teacher) in the borderline or clinical range (T ≥ 65). TD adolescents required scores on the Conners’ parent scales within the average range (T ≤ 60). While adolescents with co-occurring learning disabilities (LDs), CD, oppositional defiant disorder (ODD), anxiety, or depression were included in the sample, participants with Pervasive Developmental Disorders, Psychotic Disorders, Bipolar Disorder, Obsessive-Compulsive Disorder, and Tourette’s Syndrome were excluded.
Among the ADHD sample, 17 (57%) adolescents regularly took stimulant medication. Significantly more adolescents with ADHD (81%) had one or more parent-reported comorbid diagnoses compared with their TD (10%) peers, χ2(1, N = 58) = 23.59, p < .001. Within the ADHD group, 19 adolescents were diagnosed with a comorbid LD, 3 with Anxiety, 2 with Depression, 1 with Oppositional Defiant Disorder, and none with CD. Within the comparison group, three participants were diagnosed with an LD.
As shown in Table 1, t tests revealed no significant group differences on age, IQ, or years of parental education. Furthermore, chi-square tests revealed no significant groups differences on gender, χ2(1, N = 58) = 2.00, p = .16; parental marital status, χ2(1, N = 58) = .01, p = .94; or proportion of families where a language other than English was spoken at home, χ2(1, N = 58) = 1.22, p = .27. As expected, participants with ADHD had significantly higher scores on variables measuring current manifestation of inattentive and hyperactive/impulsive symptoms (parent, teacher, and self-reports). However, ratings of conduct problems were mixed. Whereas parents of adolescents with ADHD rated their children as having significantly more conduct problems than did parents of TD adolescents, teacher and self-reports indicated no differences in conduct problems for the subsample of participants with romantic experience (see DSM CD, Table 1).
Sample Characteristics and Demographics.
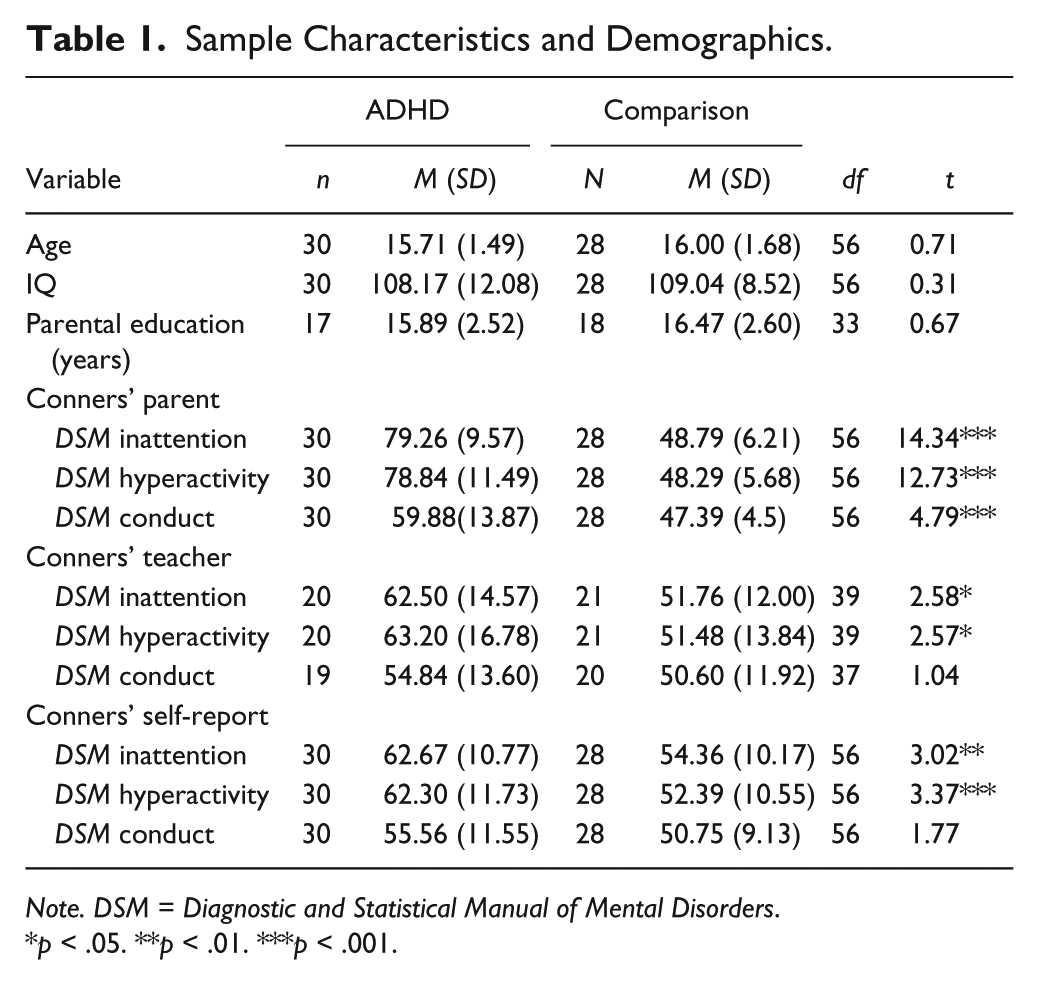
Note. DSM = Diagnostic and Statistical Manual of Mental Disorders.
p < .05. **p < .01. ***p < .001.
Measures
Sample definition and description
The Conners’ Rating Scale–3rd Edition (Conners, 2008) Parent, Teacher, and youth Self-Report long-forms were used to confirm current manifestation of ADHD symptoms. The Conners is a well-validated standardized measure consisting of 99 to 115 items on a 4-point Likert scale from 0 (not at all/seldom, never) to 3 (very much true/very often, very frequent). Internal consistency coefficients are high, .90 or above for Parent and Teacher scales, and .85 or above for self-report scales (Conners, 2008). Test–retest reliability ranges from .82 to .98 (Parents), .83 to .90 (Teacher), and .71 to .83 (Self-Report; Conners, 2008).
Cognitive ability was assessed using the WASI (Wechsler, 1999), an individually administered, brief test of intelligence. This abbreviated IQ scale demonstrates solid psychometric properties with high internal consistency (.93), test–retest reliability (ranging from .88 to .93), and concurrent and construct validity (Wechsler, 1999).
Romantic relationships
The Health and Sexual Behaviors Questionnaire (HSBQ; Flory et al., 2006) was used to obtain a history of participants’ romantic involvement and assess their engagement in potentially RSB. Items included questions pertaining to age of first sexual experience and intercourse, promiscuity, frequency of casual sex, use of reliable contraception and STIs prevention methods, and unwanted pregnancies. To minimize discomfort, the romantic relationships measures were branched such that answering “no” to questions pertaining to previous involvement in romantic relationships and intercourse precluded participants from answering more in-depth questions. Thus, participants were first asked if they had ever kissed someone. Next they were asked if they had ever had sexual relations (more than kissing, but not intercourse). Finally, participants were asked if they had ever had sexual intercourse. Participants’ responses to this last question formed the basis for the variable “sexual partners.” Most items were dichotomized to be consistent with cut-offs for RSB used in other studies (Flory et al., 2006; Grunbaum et al., 2004).
The Networks of Relationships Inventory–Behavioral Systems Version (NRI-BSV; Furman & Buhrmester, 2009) is based on an integration of attachment theory and Sullivanian theory. It assesses how frequently different relationships (e.g., mother, father, romantic partner, same-sex friend) are used to “fulfill the functions of three behavioral systems: attachment, caregiving, and affiliation” (Furman & Buhrmester, 2009). It is a 24-item survey, with 3 items per scale, rated on a 5-point scale from 1 (little or none) to 5 (the most). It assesses five support features (Provides Secure Base, Seeks Secure Base, Provides Safe Haven, Seeks Safe Haven, Companionship) and three negative interactions (Conflict, Antagonism, Criticism). Two second-order factors are computed by averaging the five support and three negative interactions scales. For the purposes of this study, only responses pertaining to the participants’ romantic partner were explored. The NRI-BSV has strong internal consistency relating to romantic partners with alphas ranging from .75 to .92. For this particular sample, internal consistency was also strong, with alphas ranging from .82 to .95.
The Conflict in Adolescent Dating Relationships Inventory (CADRI; Wolfe et al., 2001) is a 35-item self-report scale assessing abusive behavior among adolescent dating partners on five primary factors (Sexual Abuse, Threatening Behavior, Verbal or Emotional Abuse, Relational Abuse, and Physical Abuse). An Overall Abuse factor is generated by summing all 25 items pertaining to abuse (range = 25-100), whereas a Restricted Abuse factor is derived by summing all items from the Threatening Behavior, Verbal or Emotional Abuse, and Physical Abuse factors (range = 18-72). The remaining 10 items on the CADRI assess conflict resolution within the couple. Participants with and without ADHD were compared on the Overall Abuse Factor (perpetrated and incurred), the five primary factors, and the Conflict Resolution scale within the couple.
The CADRI is scored on a scale of 1 to 4 (from never to often) with higher scores indicating greater levels of abuse. The CADRI has fair internal consistency with alphas in the mid ’80s for Verbal, Physical, and Overall abuse, and .51 to .66 for the remaining scales. With the exception of Sexual Abuse (.28), the remaining scales of the CADRI have acceptable test–retest reliability ranging from .58 to .72. For this particular sample, internal consistency was also fair, with alphas ranging from .83 to .89 for Conflict Resolution and Verbal and Emotional, and Overall abuse, and.47 to .63 for the remaining scales.
Procedures
Institutional ethic’s board approval was obtained from the University of Toronto (protocol reference #25468) and all participants and their parents provided informed written consent prior to the start of the study. During an initial phone screening, parents of participants provided demographic information about their child and family, completed the Conners–Parent long form, and consented to having their child’s teacher fill out the Conners–Teacher long form. On the day of testing, researchers assisted participants in completing an individually administered battery of standardized tests and self-report measures that were part of a large-scale study assessing the peer and family relationships of adolescents with ADHD. Researchers were graduate students in school and clinical child psychology with considerable training in psychological testing. Participants were given the choice of receiving $30 as compensation for their time (approximately 4 hr) and travel expenses incurred, or receiving a volunteer community service certificate documenting time spent participating in the study. In addition, participants were provided with an educational report detailing their cognitive, academic, and socio-emotional functioning.
Data Analyses
Statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS) version 20. Descriptive statistics were calculated for the demographic characteristics (e.g., age, gender, IQ, parental marital status, parental education, language spoken at home) of the ADHD and comparison groups separately. Data points of variables with SDs larger than 3 were adjusted using the winsorizing method. Statistical assumptions checking for homogeneity of variance and normality of the outcome variables were met. If t tests revealed gender differences on outcome variables, gender and group status were included as fixed factors in subsequent 2 × 2 ANOVAs. Partial η2 values were computed to ascertain effect size and determine clinically meaningful differences. According to Vacha-Haase and Thompson (2004), η2 ≥ .01 constitutes a small effect, η2 > .09 corresponds to a medium effect, and η2 > .25 represents a large effect. To minimize the possibility of type I error, overarching scales were first examined, and only when significant differences existed were the results of item-level differences reported.
Results
History of Romantic Involvement
As shown in Table 2, adolescents with ADHD reported having more romantic partners than their TD counterparts, F(1, 53) = 5.18, p = .03, η2 = .09. Males reported beginning dating at a younger age than females, F(1, 53) = 3.79, p = .05, η2 = .07; there was no group main effect nor Group × Gender interaction effect on age of onset of dating. Females with ADHD had shorter romantic relationships than their TD counterparts, whereas males with and without ADHD reported equally short relationships across groups, F(1, 53) = 5.53, p = .02, η2 = .10. A significant interaction effect also indicated that males with ADHD reported a younger age of first intercourse than their TD male counterparts, while females with and without ADHD reported their first intercourse to occur at approximately the same age, F(1, 17) = 4.41, p = .05, η2 = .21.
Romantic Involvement of Adolescents With and Without ADHD by Gender.
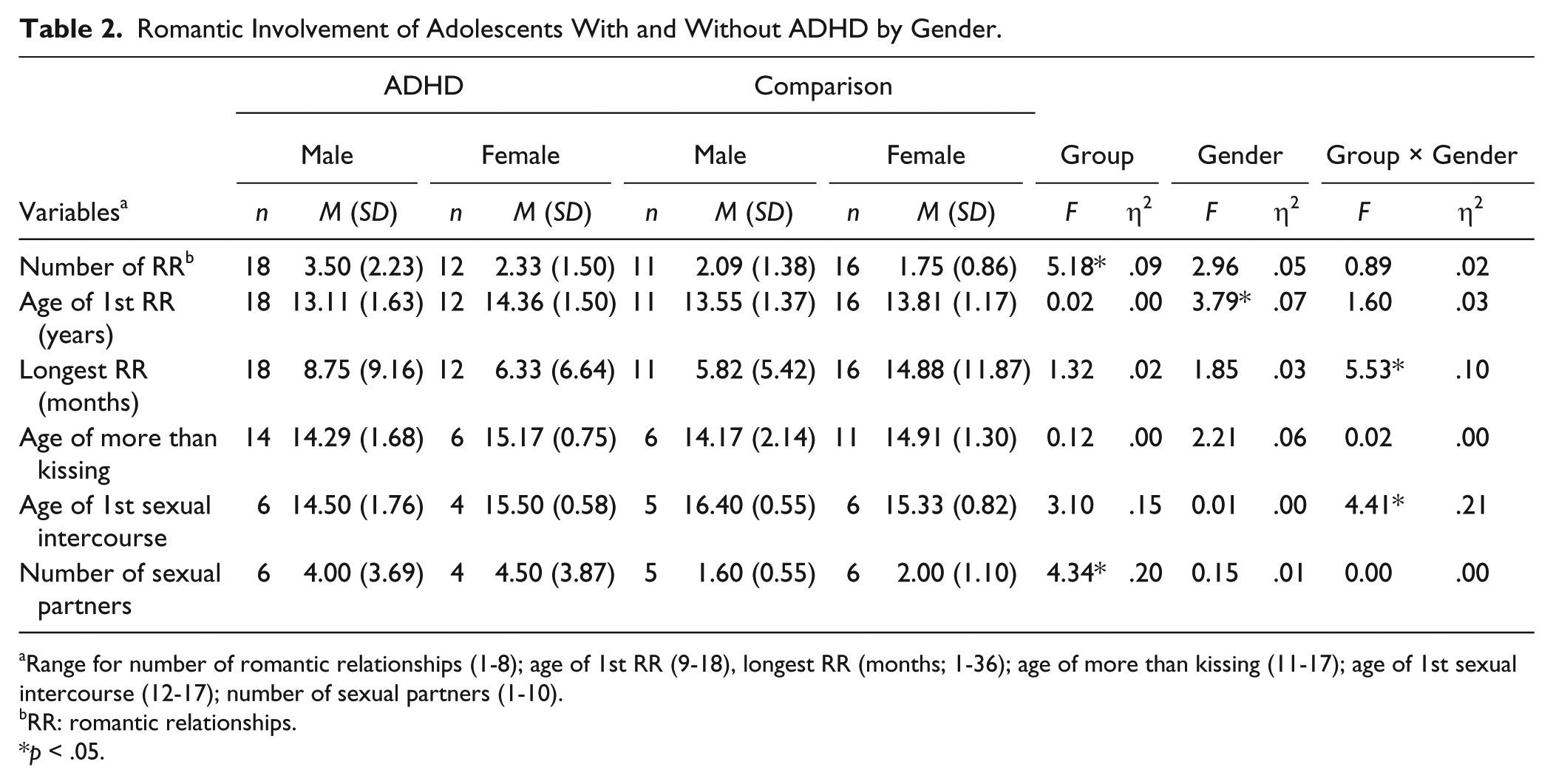
Range for number of romantic relationships (1-8); age of 1st RR (9-18), longest RR (months; 1-36); age of more than kissing (11-17); age of 1st sexual intercourse (12-17); number of sexual partners (1-10).
RR: romantic relationships.
p < .05.
Relationship Content and Quality
As reported on the HSBQ, when compared with their TD peers, adolescents with ADHD were significantly more likely to have had multiple sex partners in their lifetime (defined as four or more), and to have had casual sex within the past year (Table 3). While adolescents with and without ADHD did not differ in terms of other high-risk sexual behavior, both adolescent groups showed alarming rates for the frequency of intercourse while under the influence of drugs/alcohol, and irregular use of a combination of reliable contraception and STI prevention methods.
Risky Sexual Behavior Among Adolescents With and Without ADHD.

Note. STI = sexually transmitted infection.
Multiple is defined as 4 or more partners.
Defined as some of the time, half of the time, most of the time.
Infrequent is defined as less than almost always.
Reliable methods of birth control plus STI prevention defined as use of condom + birth control.
p < .05.
Adolescents with and without ADHD did not differ on the Overall Abuse factor of the CADRI (Sexual Abuse, Threatening Behavior, Verbal or Emotional Abuse, Relational Abuse, and Physical Abuse), assessing abuse perpetrated by the participant, F(1, 41) = 1.59, p = .22, η2 = .04, or incurred by the participant, F(1, 41) = .03, p = .86, η2 = .00. Nor did they differ on the frequency of more adaptive, conflict resolution, patterns of behavior, F(1, 41) = .05, p = .82, η2 = .00. Similarly, adolescents with and without ADHD did not differ on the Social Support, F(1, 40) = .16, p = .69, η2 = .00, or Negative Interactions (Conflict, Antagonism, Criticism), F(1, 40) = 1.14, p = .29, η2 = .03, factors of the NRI-BSV.
Discussion
The current study set out to compare the romantic relationships of adolescents with and without ADHD on three features of romantic relationships: romantic involvement, relationship content, and relationship quality. Adolescents with ADHD were found to have significantly more romantic partners than their TD peers, and in particular, female adolescents with ADHD were found to have shorter romantic relationships than their TD counterparts. In addition, males with ADHD reported their age of first intercourse to be nearly 2 years prior to males without ADHD, and adolescents with ADHD, irrespective of gender, had nearly double the number of lifetime sexual partners than TD adolescents. However, in the current study, adolescents with and without ADHD did not differ on measures assessing the quality of their romantic relationships or the levels of aggression perpetrated or incurred.
Romantic Involvement
Nearly identical proportions of males and females with and without ADHD reported experiencing a romantic relationship in their lifetime. Adolescents with ADHD had more romantic partners than their TD peers, but, similar to the findings of Canu and Carlson (2003) regarding college students with ADHD−Combined Type, adolescents with and without ADHD did not differ on their age of entry into romantic relationships. Although Babinski et al. (2011) found that college students with ADHD have a lower number of romantic partners than TD students, only female students were included in their sample whereas in the present study the majority of students with ADHD were male. As predicted, differences also emerged in terms of duration of romantic relationships; females with ADHD reported shorter romantic relationships than their TD counterparts, whereas males with and without ADHD reported relationships of similar lengths. These results suggest that the deficits in social skills, excessive negative behavior, and poor social information processing present in girls with ADHD (Crick & Dodge, 1994; Hoza, Waschbusch, Pelham, Molina, & Milich, 2000), may not only affect the stability of the friendships they form (Bagwell et al., 2001; Blachman & Hinshaw, 2002), but also their romantic relationships.
Boys with ADHD reported their first intercourse to be nearly 2 years sooner than their TD counterparts and a year earlier than girls with ADHD, who did not differ from TD girls. Furthermore, when compared with TD adolescents, adolescents with ADHD had nearly double the number of lifetime sexual partners. These findings have important implications because sexual precociousness and exposure to multiple sex partners early in adolescence are associated with HIV infections (Overby & Kegeles, 1994) and a host of other negative outcomes including depression, academic underachievement, substance use, and further RSB (Crockett et al., 1996).
Relationship Content
Like other studies examining the sexual behavior of young adults with ADHD (Barkley et al., 2010; Flory et al., 2006; Huggins et al., 2012; White & Buehler, 2012; Winters et al., 2008), when compared with their TD peers, adolescents with ADHD were significantly more likely to have had multiple sex partners in their lifetime (defined as four or more) and to have had casual sex within the past 12 months. Despite the sample’s young age, these high proportions of promiscuity are disconcerting, and a risk factor for subsequent internalizing and externalizing psychopathology.
Unlike findings from previous research (Barkley et al., 2010; Flory et al., 2006), in the current study, participants with ADHD were not more likely than their TD peers to have contracted an STI or become unintentionally pregnant. Discrepant results may be partially explained by the small sample size and younger age of the current sample relative to other studies. More specifically, adolescents may have thus far been fortunate enough to escape further ramifications of their RSB, in spite of their irregular use of a combination of reliable contraception and STI prevention methods. Alternatively, participants may have been concerned about the confidentiality of their responses, or reluctant to divulge potentially embarrassing information, thereby decreasing their endorsement of socially undesirable items.
Adolescents with and without ADHD did not differ on other items assessing RSB. Both groups showed startlingly high rates for the frequency of intercourse while under the influence of drugs/alcohol, and infrequent use of a combination of reliable contraception and STI prevention methods. In addition to the numerous risk factors of unprotected sex mentioned above, alcohol and drug use prior to sex is associated with further lapses in judgment, disinhibition of sexual behaviors, and an increased likelihood of additional RSB (Cooper, 2002; Staton et al., 1999).
Contrary to expectations and studies assessing relationship aggression and conflict resolution in adults with ADHD (Canu & Carlson, 2007; Overbey et al., 2011; White & Buehler, 2012; Wymbs et al., 2012), adolescents with and without ADHD did not differ on any variables assessing abuse perpetrated or incurred. Nor they did differ on the frequency of more adaptive, reconciliatory, patterns of behavior. These results may be partially explained by the relatively low ratings of conduct problems in the sample of adolescents with ADHD. Although there were significant group differences in parental appraisal of conduct problems, the mean score of the ADHD sample still fell within the average range. Furthermore, no group difference emerged according to teacher and self-reports of conduct problems. CD and its successor antisocial personality disorder (ASP) are linked with intimate partner violence (Schumacher, Feldbau-Kohn, Smith Slep, & Heyman, 2001). The moderately low scores of adolescents in this sample may therefore be mitigating the levels of relationship aggression found in other studies. Alternatively, it is also possible that participants with ADHD were reluctant to disclose abusive and potentially self-incriminating behavior.
Relationship Quality
Finally, adolescents with and without ADHD did not differ on measures of relationship quality, as assessed by levels of social support and negative interactions. While ADHD status in adulthood is associated with lower relationship satisfaction and a higher incidence of divorce (Biederman et al., 1993; Murphy & Barkley, 1996), and non-ADHD spouses report feelings of resentment and dissatisfaction due to inadequate emotional support and an unequal distribution of household responsibilities (Weiss et al., 1999), it is possible that the expectations and level of support implied in adolescent relationships are not as demanding as in adulthood. Furthermore, several studies and comprehensive reviews (e.g., Hoza et al., 2004; Owens, Goldfine, Evangelista, Hoza, & Kaiser, 2007) describe how individuals with ADHD tend to underreport the presence of problems and overestimate their own competence in social domains.
Limitations and Future Directions
These preliminary results, while interesting, should be considered in light of several important caveats. As in all studies, the generalizability of the findings is constrained by sample characteristics. The small sample size decreased the power of this study to detect small effects. Furthermore, the small sample prevented further exploration of factors potentially moderating the relationship between ADHD status and various outcome variables. Future studies should examine the role of the distal context (e.g., culture, ethnicity, socioeconomic status), the immediate context (e.g., family structure, family relations, parental monitoring, peer groups) and child characteristics (comorbidity, self-esteem, attachment, achievement) in explaining the association between ADHD and the features of romantic relationships. For example, comorbid externalizing behaviors have been found to exacerbate the social skills problems and peer functioning difficulties associated with ADHD (for reviews, see Becker, Luebbe, & Langberg, 2012; Villodas, Pfiffner, & McBurnett, 2012). Thus, while it is likely that comorbid ODD/CD would also affect romantic functioning similarly, the absence of comorbid ODD/CD diagnoses in the present sample did not allow for further exploration of this predictor.
Conversely, it would also be interesting to examine how romantic relationships can positively or negatively affect other developmental outcomes, including cognitive and emotional processes, educational attainment, family and peer functioning, substance use, and externalizing and internalizing symptomatology. Finally, future studies should also examine other features of romantic relationships defined by Collins (2003) that were not described in the present study. For example, it would be important to investigate the characteristics of the partner with whom the adolescent has had a romantic experience.
Another limitation of this study was its reliance on self-report to assess relationship content and quality. Although the use of self-report is commonplace in the study of adolescent behavior, it is susceptible to response bias (Kazdin, 1998; Wolfe et al., 2001). Eakin et al. (2004) suggests that in ADHD couples, partners often have conflicting views regarding their relationship. In addition, adolescents with ADHD have a propensity to inflate self-appraisals and downplay problematic behavior. Accordingly, obtaining corroboration from romantic partners would lend more credibility to the findings.
Given the unique contributions of this multi-faceted study, it would appear that the strengths of the current investigation outweigh its limitations. This investigation explored several aspects, rather than just one facet, of romantic relationships in individuals with ADHD. Moreover, the sample included both males and females and the age range was 13 to 18. The inclusion of adolescents who are still attending middle school or secondary school is important because romantic relationships of adolescents with ADHD in this age range has been understudied. The young age of the sample also meant that participants did not have to retrospectively recall their relationship history, thus limiting the confounding and biased effects of recall.
Clinical Implications
The findings regarding romantic involvement and sexual behavior in the current study have important implications for the parents, educators, and clinicians who work with adolescents with ADHD. Unfortunately, only a minority of adolescents with ADHD, about one in eight, receive care for their disorder (Jensen et al., 1999). Most are treated with stimulant medication (Smith, Waschbusch, Willoughby, & Evans, 2000) and few receive some form or psychosocial or educational intervention. Given the poor outcomes associated with RSB, relationship instability, and negative partner characteristics, it is imperative that any comprehensive assessment of adolescents with ADHD include queries into the nature of their romantic relationships. In turn, information obtained may help clinicians devise specific and individualized strategies to help adolescents prevent and/or cope with romantic relationship difficulties. At a more universal level, results from this study, although preliminary, may help inform sex education programs seeking to reduce unsafe sexual behavior in this at-risk population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The current study was supported by the Social Sciences and Humanities Research Council of Canada.