
Abstract
Introduction
ADHD is a disorder primarily characterized by inattention, impulsivity, and hyperactivity. Genetic heritability is reported to account for approximately 75% of ADHD cases (Faraone et al., 2005), whereas environmental factors, such as early traumatic experiences, are estimated to account for 25% of cases (Ben Amor et al., 2005).
Although the etiology of ADHD is not fully understood, current evidence indicates that dysregulation of the central dopaminergic and noradrenergic systems may be involved in the pathophysiology of ADHD (Del Campo, Chamberlain, Sahakian, & Robbins, 2011). Catechol-O-methyltransferase (COMT) degrades synaptic dopamine and noradrenaline and plays a specific role in the catabolism of prefrontal cortical dopamine in the context of the relative lack of dopamine transporters in the prefrontal cortex (Napolitano, Cesura, & Da Prada, 1995). The COMT gene has a functional polymorphism at codon 158 that results in a single amino acid change (methionine [Met] for valine [Val]). Due to its important role in prefrontal cortex dopamine neurotransmission, COMT is considered an essential candidate gene in the etiology of ADHD, despite the results of a recent pooled analysis that do not support an association between the Val/Met single nucleotide polymorphism (SNP) and ADHD (pooled odds ratios [OR] = 1.02, 95% confidence interval [CI] = [0.92, 1.13], p = .7267; Sun, Yuan, Shen, Xiong, & Wu, 2014).
The dopamine receptor D4 (DRD4) gene is one of the most frequently studied candidate genes associated with ADHD (Barr et al., 2000). The 7-repeat allele of the exon III variable number of tandem repeats (VNTR) polymorphism of the DRD4 gene resulted in a blunted response toward dopamine (Asghari et al., 1995). In a study of the correlation between ADHD and the DRD4 gene, the meta-analysis of case-control studies and family-based studies demonstrated significant pooled ORs of 1.9 (95% CI = [1.4, 2.2]) and 1.4 (95% CI = [1.1, 1.6]), respectively (Faraone, Doyle, Mick, & Biederman, 2001). Unlike European or Caucasian participants, Asian participants, including Koreans, rarely exhibit the 7-repeat allele of DRD4 exon III 48-bp VNTR polymorphism (Cheon, Kim, & Cho, 2007; B. Kim et al., 2009). In Korean children with ADHD, the homozygosity of the 4-repeat allele at DRD4 was reported to be associated with methylphenidate response (Cheon, Jun, & Cho, 2008) or neuropsychological phenotypes (B. Kim et al., 2009).
Childhood exposure to potentially traumatic events (PTEs) such as maltreatment strongly predicts the development of ADHD and influences biological processes in offspring, a key consideration in selecting viable environmental risk factors in gene–environmental interaction research (Moffitt, 2005). Maltreated children (e.g., victims of physical abuse, sexual abuse, and neglect) exhibit higher levels of ADHD than children who were not maltreated (Ouyang, Fang, Mercy, Perou, & Grosse, 2008). Early chronic stress disrupts hypothalamic–pituitary–thalamic axis (HPA) functioning, which regulates stress reactivity, mental health, and DA neurotransmission (Strathearn, 2011; Twardosz & Lutzker, 2010). Prolonged maternal neglect and separation was inversely associated with DA transporter binding in rat pups (Hall et al., 1998), and poor maternal care during childhood significantly increased the release of DA in the ventral striatum of young adult humans (Pruessner, Champagne, Meaney, & Dagher, 2004).
Neuropsychological deficits are frequently described in ADHD participants in domains such as attention and executive functions (EFs). Sustained attention assessment tools such as the Continuous Performance Test (CPT; Greenberg & Waldman, 1993) have frequently been used for both research and clinical issues concerning ADHD despite controversial results regarding their discriminant validity. The CPT involves the rapid presentation of stimuli on a computer screen for an extended period of time. Children with ADHD are typically measured on the number of omission errors (failing to acknowledge a target stimuli), commission errors (acknowledging a non-target), and response time variability. Attentional and EF deficits were also reported in individuals with children exposed to PTEs (Beers & De Bellis, 2002; DePrince, Weinzierl, & Combs, 2009; Mueller et al., 2010). This common neuropsychological deficit among children with ADHD and traumatized children suggests that early trauma might contribute to the development of ADHD by leading to attentional and EF deficits.
Given the negative neurobiological sequelae of trauma in humans and non-human animals, an interaction between early trauma and genetic variations for the neuropsychological deficits of ADHD is biologically plausible. Therefore, in this study, we investigated the interaction between childhood exposure to PTEs with the DRD4 exon III VNTR polymorphism and the COMT Val158-Met (rs4680) polymorphisms in relation to neuropsychological measures in children with ADHD.
Method and Materials
Participants
Participants were drug-naive children aged 6 to 15 years who were diagnosed with ADHD according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria. Between May 2012 and January 2013, a total of 55 participants were recruited from the Department of Psychiatry at Seoul National University Hospital in Korea, advertising a free assessment for ADHD including the neuropsychological test. Children meeting any of the following criteria were excluded: (a) intelligence quotient (IQ) score below 70; (b) past or current neurological disease; (c) a past or ongoing history of tic disorder, obsessive compulsive disorder, language disorder, learning disorder, convulsive disorder, pervasive developmental disorder, schizophrenia, bipolar disorder, or brain damage; or (d) a recent history, over the last 4 weeks, of taking stimulants or atomoxetine.
The study protocol was approved by the Institutional Review Board for human participants at the Seoul National University Hospital. Detailed information about the study was given to the parents and children, and written informed consent was obtained prior to study entry.
Diagnostic and Clinical Evaluations
We evaluated the presence of ADHD and other psychiatric diagnoses using a semi-structured diagnostic interview, the Kiddie–Schedule for Affective Disorders and Schizophrenia–Present and Lifetime Version (K-SADS-PL). The validity and reliability of the original and the Korean versions of the K-SADS-PL have been established (Y. S. Kim et al., 2004). The parents completed the Korean version of the ADHD Rating Scale–IV (ADHD-RS; So, Noh, Kim, Ko, & Koh, 2002) to assess the severity of ADHD symptoms.
Neuropsychological Assessments
Level of attention and response inhibition was assessed using a standardized auditory version of the computerized CPT (Greenberg & Waldman, 1993; Shin, Cho, Chun, & Hong, 2000). The test involves three easily recognizable auditory stimuli (two non-target stimuli and one target stimuli) for an extended period of time. In this study, we used three major variables: omission errors (failing to press for a target, a measure of inattention), commission errors (pressing for a non-target, measure of impulsivity), and response time variability (the standard deviation of the response times for correct responses to the target, a measure of consistency of attention). All data are presented as T-scores adjusted for age, and lower T-scores indicate better test performance.
Childhood Trauma
The Early Trauma Inventory Self-Report–Short Form (ETISR-SF) is a 27-item questionnaire used for the assessment of physical, emotional, and sexual abuse and general traumatic experiences that may have occurred before age 18. The measure has been shown to have excellent validity and internal consistency (Bremner, Bolus, & Mayer, 2007). Physical abuse was described as physical contact, constraint, or confinement with the intent to hurt or injure. Emotional abuse was described as verbal communication with the intent to humiliate or degrade the victim. Sexual abuse was described as unwanted sexual comments or contact performed solely for the gratification of the perpetrator or for the purposes of dominating or degrading the victim. General traumatic events included a range of stressful and traumatic events that are mostly secondary to chance events, as opposed to events in the abuse domains that typically involve perpetration by an individual known to the victim with the specific intent to harm the victim. Each traumatic experience was scored dichotomously (yes/no). Participants who experienced any traumatic events were placed in the PTE group, and participants who did not experience any traumatic events were placed in the non-PTE group.
Genotyping
Genomic DNA was extracted from blood (stored frozen) using a G-DEXTM II Genomic DNA Extraction Kit (Intron, Korea) according to the manufacturer’s protocol. SNP detection was based on an analysis of primer extension products generated from previously amplified genomic DNA using a chip-based MALDI-TOF mass spectrometry platform (Sequenom, Inc., California). The general procedures were performed according to the manufacturer’s standard protocol. For the COMT polymorphism, the oligonucleotide primers (5’-ACG TTG GAT GTT TTC CAG GTC TGA CAA CGG and 5’- ACG TTG GAT GAC CCA GCG GAT GGT GGA TTT) were used to generate polymerase chain reaction (PCR) products. For the DRD4 exon III VNTR polymorphism, the oligonucleotide primers (5’-ACC ACC ACC GGC AGG ACC CTC ATG GCC TTG CGC TC-3’ and 5’-CTT CCT ACC CTG CCC GCT CAT GCT GCTGCT CTA CTG G-3’) were used to generate the DRD4 exon III polymorphic region (2-10 variable repeat units, 1 unit = 48 base pairs).
Statistical Analysis
We determined the allele frequency and then calculated the Hardy–Weinberg equilibrium using a goodness-of-fit chi-square test. Due to the small number of participants with the COMT Met/Met genotype, the sample was divided according to the presence or absence of the rare Met allele. The genotype variable dichotomized participants into two groups: those with the COMT Val/Val genotype and those with the Val/Met or Met/Met genotype or those with the DRD4 4/4 genotype and those with another genotype. This differentiation was selected because previous studies have reported an association between the Val/Val homozygote of COMT or the 4-repeat allele homozygote of DRD4 (Cheon et al., 2007; B. Kim et al., 2009) with clinical and neuropsychological phenotypes of ADHD.
We compared the clinical and neuropsychological characteristics of the PTE(+)-group and the PTE(−)-group using an independent t-test for continuous variables and a chi-square or Fisher’s exact test for categorical variables. A two-way analysis of variance (ANOVA) was conducted to examine the effect of the DRD4 or COMT genotype and the PTE on each CPT variable scores; the presence of PTE, the DRD4 or COMT genotype, and a genotype-by-PTE interaction term were included in the model. All statistical analyses were performed using SPSS (version 21.0; SPSS Inc., Chicago, Illinois), with statistical significance defined as an alpha level <.05.
Results
A total of 55 children participated in this study. Table 1 shows the group-specific demographic and clinical characteristics. The age and gender distributions were not significantly different between the PTE(+)- and PTE(−)-ADHD groups. The PTE(+)-group showed significantly higher commission errors (t = −2.62, p = .011) than the PTE(−)-group.
Characteristics of Children With ADHD by the Presence of Childhood PTE.
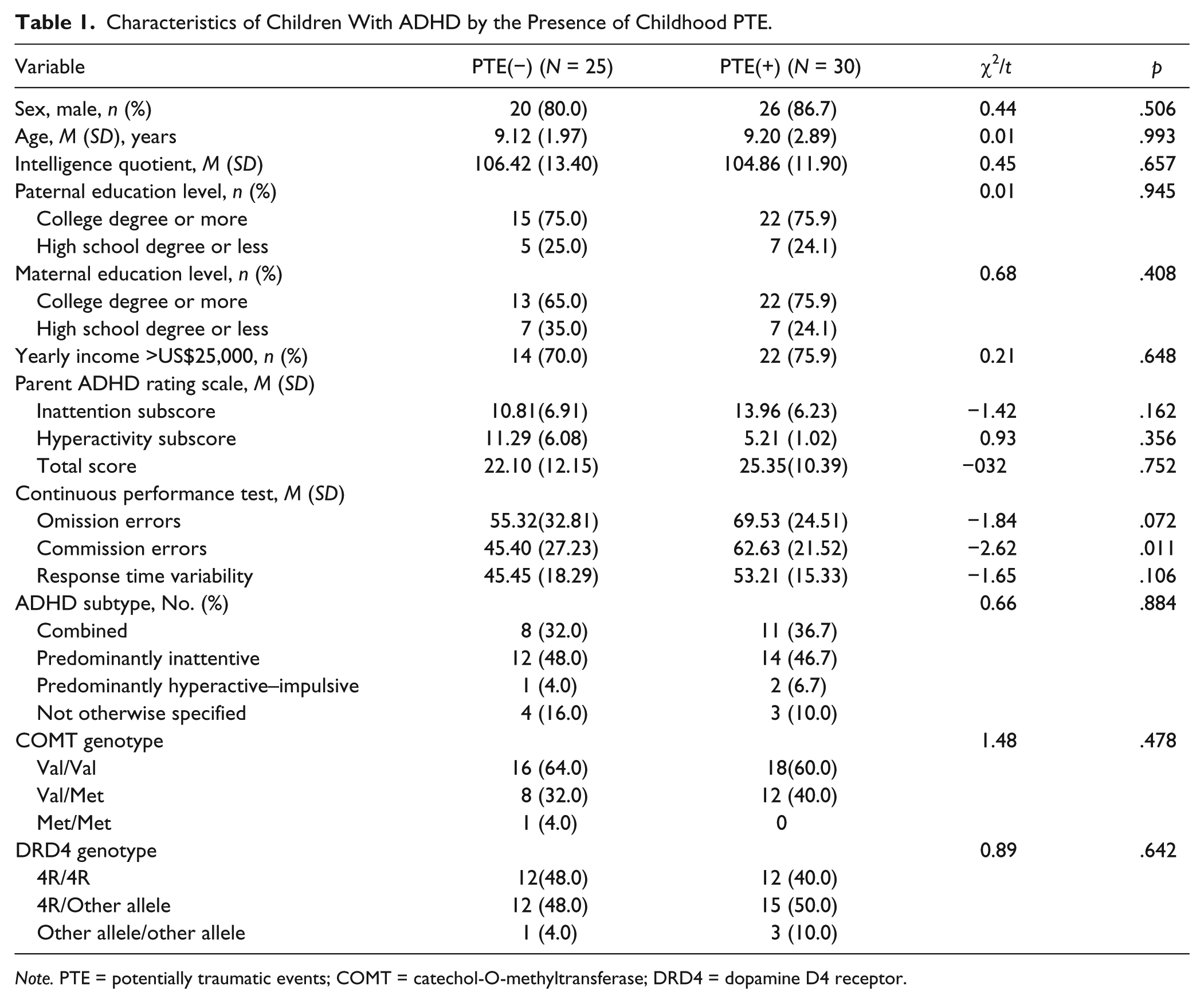
Note. PTE = potentially traumatic events; COMT = catechol-O-methyltransferase; DRD4 = dopamine D4 receptor.
Genetic distributions of the exon III VNTR polymorphism of DRD4 and Met/Val polymorphism of COMT coincided with the expected values of the Hardy–Weinberg Equilibrium (p > .05). Among DRD4 genotypes, the 4/4 genotype was observed in 25 (45.5%) out of 55 participants in our sample, the 4/4 genotype in 24 participants (43.6%), and the 2/5 genotype in 2 participants (3.6%). The 2/2, 3/4, 4/6, and 5/5 genotypes were observed in 1 participant (1.8%) each. Among COMT genotypes, the G/G genotype was observed in 34 (61.8%) out of 55 participants in our sample, the G/A genotype in 20 participants (36.4%), and the A/A genotype in 1 participant (1.8%).
Presence of the PTE significantly affected commission error scores in both the COMT model, F(1, 51) = 4.40, p = .041, and DRD4 model, F(1, 51) = 6.59, p = .013. There was a statistically significant interaction between the effects of the COMT genotype and PTE in commission errors, F(1, 51) = 4.19, p = .046 (Table 2). Simple main effects analysis showed that the PTE(+)-group showed significantly higher commission errors than the PTE(−)-group in participants with the COMT Val/Val genotype (p = .004), but there were no differences between PTE(+)- and PTE(−)-groups in participants with the Met/Val or Met/Met genotype (p = .822; Figure 1). Interactions between the effects of the DRD4 genotype and PTE were not statistically significant (Table 2).
Two-Way ANOVA Models Examining the Main and Interaction Effects of the COMT/DRD4 Genotypes and PTE on the Continuous Performance Test Scores.

Note. PTE = potentially traumatic events; COMT = catechol-O-methyltransferase; DRD4 = dopamine D4 receptor.
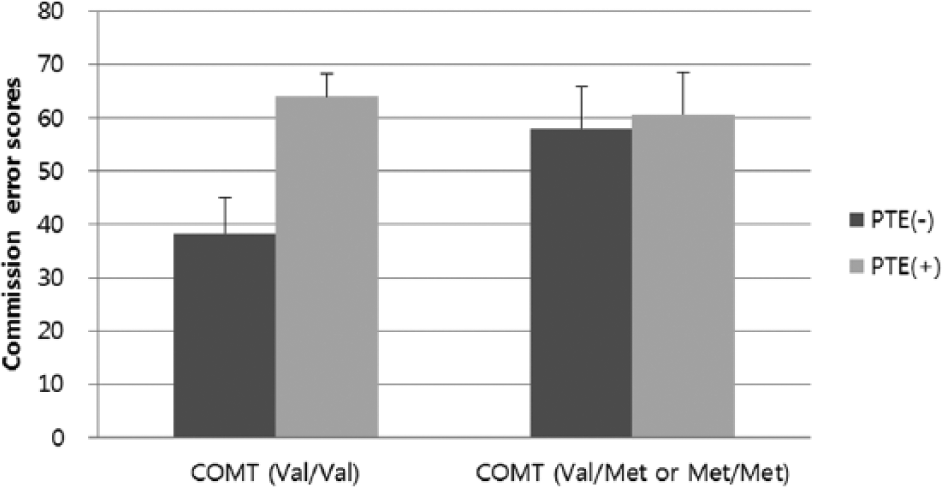
Commission error scores according to the PTE and the COMT genotype.
Discussion
To the best of our knowledge, this is the first study that has identified an association between childhood traumatic experiences and poor attentional performance in ADHD children with evidence of gene–environment interactions for the COMT genes and early traumatic experiences.
The most notable difference between ADHD children with and without PTEs was observed in commission errors. Commission errors are indicators of a deficit in response inhibition, which is frequently reported in ADHD, particularly in combined subtype (Aron & Poldrack, 2005; Barkley, 1997). This result is consistent with that of a previous study that reported that maltreatment or accidental trauma places children and adults at risk of symptomatic problems paralleling those in ADHD (e.g., inhibitory deficits; Beers & De Bellis, 2002; Mueller et al., 2010). Our results suggest that early traumatic experiences may play an important role either in the neurotransmitter system or during the neurodevelopmental process, possibly increasing the risk for a specific phenotype of ADHD.
It is intriguing that the association between early traumatic experiences and the CPT results were observed only in participants with specific genotype, the Val/Val genotype of COMT. We could speculate that for genetically susceptible participants, neural substrates associated with attentional systems may be more susceptible to childhood trauma exposure. The Val/Val genotype of the COMT (Val158-Met) was reported to be associated with a better response to methylphenidate treatment in Korean children with ADHD (Cheon et al., 2008), suggesting that persons with this allele would be more susceptible to external influences. Individuals with the COMT Val allele presumably have relatively fewer synaptic catecholamine neurotransmitters available and concomitantly show worse performance in neuropsy-chological measures of executive functioning than individuals with the Met allele (Joober et al., 2002; Malhotra et al., 2002). Individuals with the Val/Val genotype may have lower cortical dopamine levels (Mattay et al., 2003), resulting in more active striatal dopamine neurotransmission by attenuating prefrontal dopaminergic negative control on the subcortical dopaminergic system. Because deficits in response inhibition are more closely related to striatal function, the COMT interaction effect on the negative influence of early traumatic experiences might be pronounced in the commission error domain.
There were several limitations to this study. First, because our data were cross-sectional and correlational, no inferences about causality are possible at this time. Several possible bidirectional or interactive relationships could link childhood trauma exposure with symptomatic and neuropsychological problems that parallel those in ADHD. One possibility is that children with ADHD, especially those having severe inhibitory deficits, may be at risk of trauma exposure because they have interpersonal and self-regulatory problems that could place them at risk of harm, especially maltreatment. In contrast, childhood PTEs may contribute to or exacerbate inattention and inhibitory deficits. Second, the ETISR-SF used for the assessment of childhood trauma was developed for adults above 18 years and was not yet validated for children. Third, there was no control group. To determine whether the influence of the genotype-PTE interaction on attentional performance is specific to ADHD patients, we should have obtained data from healthy controls. Finally, the sample size of the present study was very small, particularly for the genotypic analysis; thus, the results should be carefully interpreted.
Despite these limitations, the results of this study suggest a genetic influence on the association between childhood trauma exposure and the severity of inhibitory deficits in children with ADHD. Further studies in a larger sample size and in other populations are warranted to further evaluate the association between childhood trauma exposure and ADHD with gene–environment interactions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Basic Science Program through the National Research Foundation of Korea (NRF) funded by the Korean government (2013R1A1A3008158) and a grant of the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (A120013).