
Abstract
Introduction
ADHD is one of the most common childhood disorders (Pennington, 2008). It is estimated to affect 7% to 10% of children and involves difficulty with inattention, hyperactivity, or impulsivity (American Psychiatric Association [APA], 2013). While there are three subtypes of ADHD currently identified (combined, predominately inattentive, and hyperactive-impulsive), most studies have concentrated on the ADHD:Combined type (ADHD:C).
There are few studies exploring the neuropsychology or neurodevelopment of children with ADHD:Inattentive type (ADHD:I). In Barkley’s model (Barkley, 2006), children with ADHD:I show inattention difficulties that arise from difficulty with selective attention as well as speed of information processing. In contrast, children with ADHD:C are characterized by difficulties with sustained attention and distractibility. Frequent learning difficulties as well as a sluggish cognitive tempo have been identified as major neuropsychological difficulties for children with ADHD:I (McBurnett, Pfiffner, & Frick, 2001). Sluggish cognitive tempo has been found in approximately half of the children with ADHD and has been hypothesized to co-exist with ADHD but also possibly be a separate disorder (Barkley, 2013, 2014). There have been several suggestions that ADHD:I is a different type of attentional disorder, possibly arising from different substrates than ADHD:C (Milich, Ballentine, & Lynam, 2001). Up to this point, there have not been structural studies demonstrating this difference.
The caudate has been implicated as part of a “complex loop” for modulating activity level and impulsivity. It receives information from the association cortices and indirectly sends it via the thalamus to the prefrontal cortex. There have been several structural magnetic resonance imaging (MRI) studies that have evaluated specific brain regions that generally include the caudate and anterior cingulate cortex (ACC) in children with ADHD:C. Two meta-analyses of the structural findings in ADHD indicate that the right globus pallidus, right putamen, and bilateral caudate are compromised in children with ADHD:C (Frodl & Skokasukas, 2011; Nakao, Radua, Rubia, & Mataix-Cols, 2011). A reduction in caudate volumes for neurotypical children with age has been found, while caudate volumes for non-medicated ADHD children remained stable over time (Nakao et al., 2011).
The ACC is another area that is intimately connected to the frontal lobes and has been linked to problems with attention (Castellanos et al., 2008). The ACC has been found to be linked to performance monitoring/evaluation and to error processing (Goto, Ando, Huang, Yee, & Lewis, 2010) as well as inhibitory control, a cardinal difficulty in children with ADHD (Garavan, Ross, Murphy, Roche, & Stein, 2002). A structural MRI study found the ACC to be smaller in adults with a mixed sample of participants with ADHD compared with controls (Seidman et al., 2006). Other studies have demonstrated that thinning of the right ACC is associated with higher levels of parent-reported symptom severity in children with ADHD:C (Bledsoe, Semrud-Clikeman, & Pliszka, 2013). Less is known, however, if the same brain–behavior relationship is implicated in those with ADHD:Predominately inattentive type (ADHD:PI). Given the very different symptom profiles of the ADHD subtypes, studies seeking to explore differences in neuroanatomical and neuropsychological etiological pathways are warranted. Such work could provide helpful information regarding casual differences between the subtypes and may in turn inform subtype-specific treatment interventions.
Studies utilizing functional neuroimaging found that when adults with ADHD completed the Counting Stroop, the frontal–striatal–insular regions were activated, but the ACC cognitive division region (anterior part of the ACC) was not. In contrast to the ADHD group, the ACC cognitive region was activated by the control group (Bush et al., 1999). It was concluded that, for adults, this hypoactivity in the ACC was not related to a poor neuronal responsiveness of the total frontal region. Increased activation of the ACC in response to failed inhibition has been found in neurotypical children but not in children with ADHD (Pliszka et al., 2006). Thus, functional neuroimaging implicates the ACC, in particular, as playing a role in ADHD particularly for error processing.
A review of the extant literature did not find any structural neuroimaging studies that utilized children with ADHD:PI. If Barkley’s model holds true that ADHD:I is due to problems with attention and not impulse control, then it would be expected that children with ADHD:I will not show volumetric differences in the caudate; a structure generally implicated in problems with motor control and impulsivity. It is also plausible that these children may well show differences in the anterior cingulate, which has been found to play a role in monitoring of behavior and attention (Bush, 2011).
Supporting this conclusion is a recent study that evaluated children with ADHD:C and those with ADHD:I using resting-state MRI (Fair et al., 2013). Atypical connectivity in the midline default networks was found for children with ADHD:C. These networks include the ventral striatum and ventromedial cortex and have been linked to the ability to adapt and change behaviors based on the present situation and the effect of future consequences (Musser et al., 2011). In contrast, the ADHD:I group showed differences in the bilateral dorsolateral prefrontal cortex and cerebellum. Atypical activity in these regions is related to task-level control, which is linked to problems with attention (Dossenbach, Fair, Cohen, Schlaggar, & Petersen, 2008).
Current Study
Based on the above previous findings, we hypothesized that children with ADHD:C would have smaller volumetric measures for the caudate bilaterally, while these findings would not be present in children with ADHD:I or controls. We further hypothesized that children in both ADHD groups would show smaller volumes of the ACC. Parent measures of hyperactivity were expected to be significantly related to the volumes of the caudate, whereas measures of attention and hyperactivity were expected to be related to the volumes of the ACC. This is the first study, to our knowledge, that has analyzed MRI scans of children with ADHD:I.
Method
Participants
This study is part of a larger study that included a comprehensive neuropsychological battery. Participants were right-handed children and adolescents aged 9 to 16 of both genders. There were a total of 74 children in the final sample (27 controls, 25 ADHD:C, 22 ADHD:I). There were 17 males in the control group, 22 in the ADHD:C group, and 19 in the ADHD:I group. MRI data from 3 controls (2 males, 1 female), 5 ADHD:C (5 males), and 4 ADHD:I (3 males, 1 female) were not used for analysis due to excessive movement. Excessive movement was defined as scans that were not possible to be corrected to accurately evaluate the structures. Twenty percent were self-declared minorities. In all, 17 children with ADHD:C and 9 children with ADHD:I were on stimulant medication. Written informed consent was obtained from each parent and assent from the child. Participants were recruited through a university website and through advertisements and posters in the community. Participants were drawn from the United States and were all native English speakers. Each child completed a comprehensive neuropsychological evaluation as part of a related study. From these findings, children with a history of a seizure disorder, traumatic brain injury, serious psychopathology, learning disability, or mental illness were excluded.
Diagnostic Procedure
Each participant completed a brief screening to determine eligibility for the study. Doctoral-level graduate students trained in administering a comprehensive neuropsychological battery individually assessed the participants. These graduate students were blind to the diagnosis of the child. Diagnoses were determined through consensus between two practicing licensed clinical psychologists (M.S.C. and J.G.F.). Parents completed a semi-structured interview with Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000) criteria and consistent with DSM-5 (5th ed.; APA, 2013). The interview was adapted from the Kiddie-SADS (Schedule for Affective Disorders and Schizophrenia) and used in several previous articles (Hynd et al., 1993; Semrud-Clikeman, Pliszka, Lancaster, & Liotti, 2006). For a diagnosis of ADHD:C, seven symptoms of inattention and seven symptoms of hyperactivity/impulsivity were required to be endorsed. Difficulty was reported in two settings and onset of symptoms began prior to age 7. A diagnosis of ADHD:I required seven symptoms of inattention and less than four symptoms of hyperactivity and impulsivity. Difficulty was reported in two settings and onset of symptoms began prior to age 7. These criteria are a bit more stringent than DSM-5 to make sure that subclinical children were not included in the study. Only children with a full-scale IQ (FSIQ) above 80 were included in the sample. All children completed the Wechsler Abbreviated Scale of Intelligence (WASI; Psychological Corporation, 1999). The WASI is a well-standardized and reliable measure that provides an estimated FSIQ. All parents completed the Behavior Assessment System for Children–2 (BASC-2; Reynolds & Kamphaus, 2004) for a standardized measure of hyperactivity and attention. The BASC-2 is a well-standardized omnibus measure of behavioral and emotional functioning. For this study, we utilized the hyperactivity and attention scales.
MRI Procedure
No child had had undergone a previous MRI. Following the diagnostic interview adapted from DSM-5 criteria, each child completed a MRI scan and each scan was read by a clinical technologist for abnormalities, and reviewed by a radiologist if necessary. The MRI was obtained on a 3T Signa® HDx MR scanner (GE Healthcare, Waukesha, WI) with an eight-channel head coil. High-resolution volumetric T1-weighted 3D inversion recovery prepared fast spoiled gradient recalled sagittal images with cerebrospinal fluid (CSF) suppressed were obtained to cover the whole brain with the following parameters: time of echo = 5 ms, time of repetition = 11.4 ms, time of inversion = 500 ms, flip angle = 8°, receiver bandwidth = ±15.6 kilo Hertz, field of view = 24 cm, slice thickness = 1.5 mm, matrix size = 256 × 192, number of slices = 124 (4 discarded), number of excitation = 1, and scan time = 7 min 47 s.
Preprocessing with Analysis of Functional NeuroImages (AFNIs)
The current study used the AFNIs software program, version 2.56b (Cox, 1996) to complete the volumetric analysis for the caudate and ACC of the MRI images. Upon importing the MRI image into the AFNI program, the image voxels, or the cubic units used to identify volumetric units of the brain, were resampled to 1 × 1 × 1 mm and completed on the original domain. The AFNI plug-in module “3DUniformize” was used to correct for T1 image intensity non-uniformity. All brains were aligned using the anterior commissure (AC) and posterior commissure (PC) axis assuring a uniform orientation across participants. The caudate and ACC were hand drawn using the boundaries explained below.
Anatomical guidelines
Guidelines for anatomical boundaries for the caudate and ACC were adapted from previously published work for the caudate, superior frontal, and prefrontal regions (Filipek et al., 1997) and adapted from Riffkin et al. (2005) for the ACC. The ACC cortex is found bilaterally in the medial wall of the frontal lobes. It surrounds the rostrum of the corpus callosum. The superior border was the cingulate sulcus and the inferior border was the callosal sulcus. A vertical line perpendicular to the AC–PC line and passing through the AC was used as the posterior boundary. Figure 1 illustrates a slice showing the ACC.

Outline of anterior cingulate cortex.
The caudate was measured using the lateral border of the lateral ventricle as the medial border. The lateral boundary was the medial aspect of the internal capsule. The posterior boundary was found 20 mm posterior to the AC. The superior frontal lobes were defined laterally by the central sulcus, posteriorly by the lateral sulcus, and anteriorly by the presence of the corpus callosum. The prefrontal region was defined as the first slice anterior to the corpus callosum to the most anterior point of the cerebrum. Figure 2 illustrates the caudate.

Outline of bilateral caudate.
Tissue and ROI segmentation with Free Surfer (FSL)
The semi-automated FSL program was used to obtain gray (GM) and white matter (WM) volumes that cannot be obtained using the AFNI program. Analyses of these volumes for the structures were conducted with the Brain Extraction Tool (BET) and the Automated Segmentation Tool (FAST) developed at the Oxford Centre for Functional MRI of the Brain (FMRIB; Smith et al., 2004). The BET tool was used to segment brain–non-brain tissue (fat, eyes, and muscle) and remove non-brain tissue before carrying out brain tissue segmentation. The BET provided a spherical smoothed surface based on the local intensity structure of each tissue type that reduced image bias field errors. After BET was complete, command line FAST was used to classify voxels into GM, WM, and CSF and to output the volumes of these three tissue types. The fslroi tools were used to separate the right and left hemispheres (based on the mid-sagittal slice in the x-axis). With the separation, a new file with only the right/left hemisphere was created and analyzed with FAST and fslstats.
Measurement Reliability
Blind to the identity of previous image analyses, approximately one fourth of participants’ images were re-measured and compared with the initial measurement to establish test–retest reliability. A reliability analysis, interclass coefficient, was calculated in SPSS to provide an estimate of rater reliability. The interclass coefficient for the ACC was 0.89 and 0.93 for the caudate, which is within the acceptable limits based on previous studies (Wellington, Semrud-Clikeman, Murphy, Gregory, & Lancaster, 2006).
Results
There was no significant difference in overall IQ among the groups, F(2, 71) = 2.34, p = .1, partial η2 = .06, or in age, F(2, 71) = 2.53, p = .13, partial η2 = .07. While there was not a significant age difference among the groups, it was decided to use total brain volume as a covariate due to the large standard deviations in all groups for age. As expected, there were significant group differences in the behavioral measures. On measures of hyperactivity and total symptoms, the ADHD:C group was rated the most poorly compared with the other two groups. As expected, both ADHD groups were rated significantly different than the control group on attention but did not differ from each other. Table 1 provides the demographic data for these children.
Demographics and Selection Test Scores.
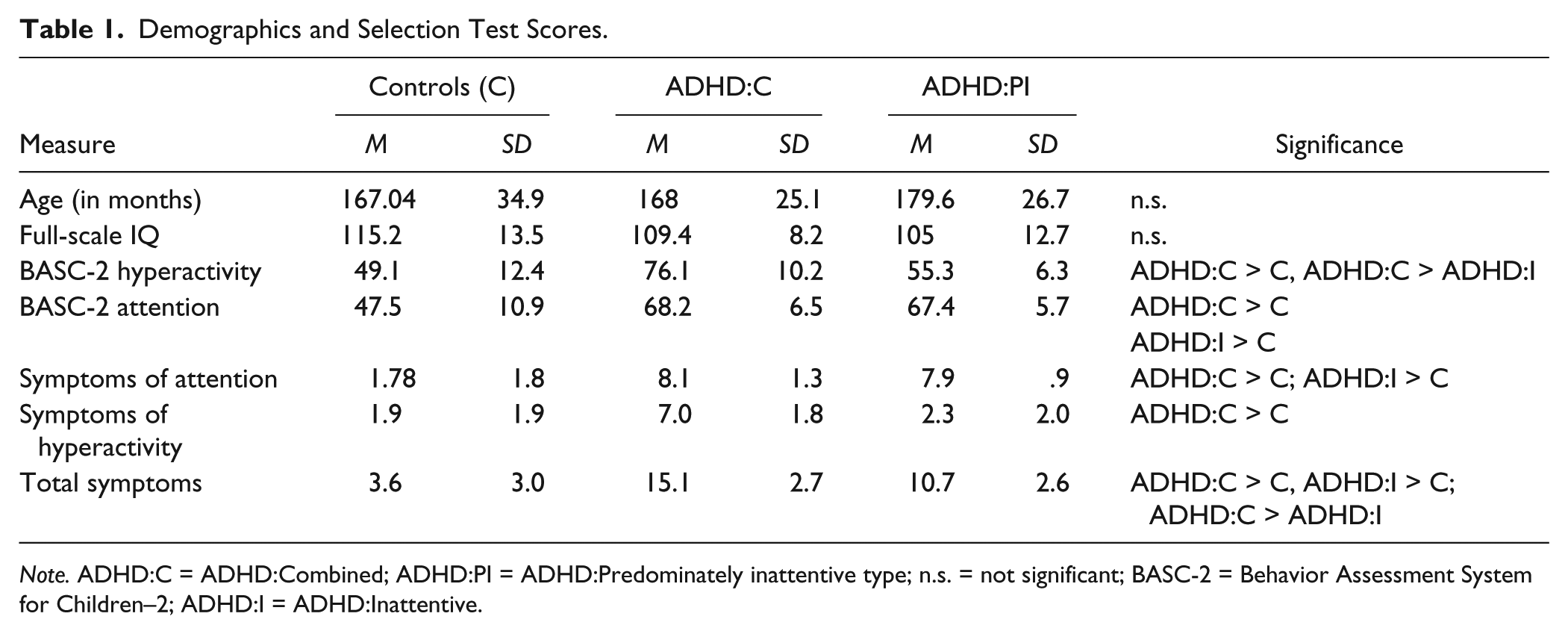
Note. ADHD:C = ADHD:Combined; ADHD:PI = ADHD:Predominately inattentive type; n.s. = not significant; BASC-2 = Behavior Assessment System for Children–2; ADHD:I = ADHD:Inattentive.
Total, GM, and WM volumes were obtained through FSL analysis. A 3 (group) × 1 (total volume) ANOVA found no significant group effects, F(2, 71) = 0.23, p = .79, partial η2 = .007. A 2 (white, gray) × 3 (group) MANOVA found no significant group effect for total GM. An ANOVA resulted in no significant group differences in total volume, F(2, 88) = 0.38, p = .68. A 3 (group) × 2 (WM, GM) MANCOVA with total volume as a covariate approached significance, F(1, 68) = 2.39, p = .09, partial η2 = .07. Further evaluation of right and left group differences in GM and WM volumes revealed no significant group differences, F(8, 130) = 1.53, p = .15, partial η2 = .09. Table 2 provides these measurements.
Volumetric Measures (mm3) for Three Groups.
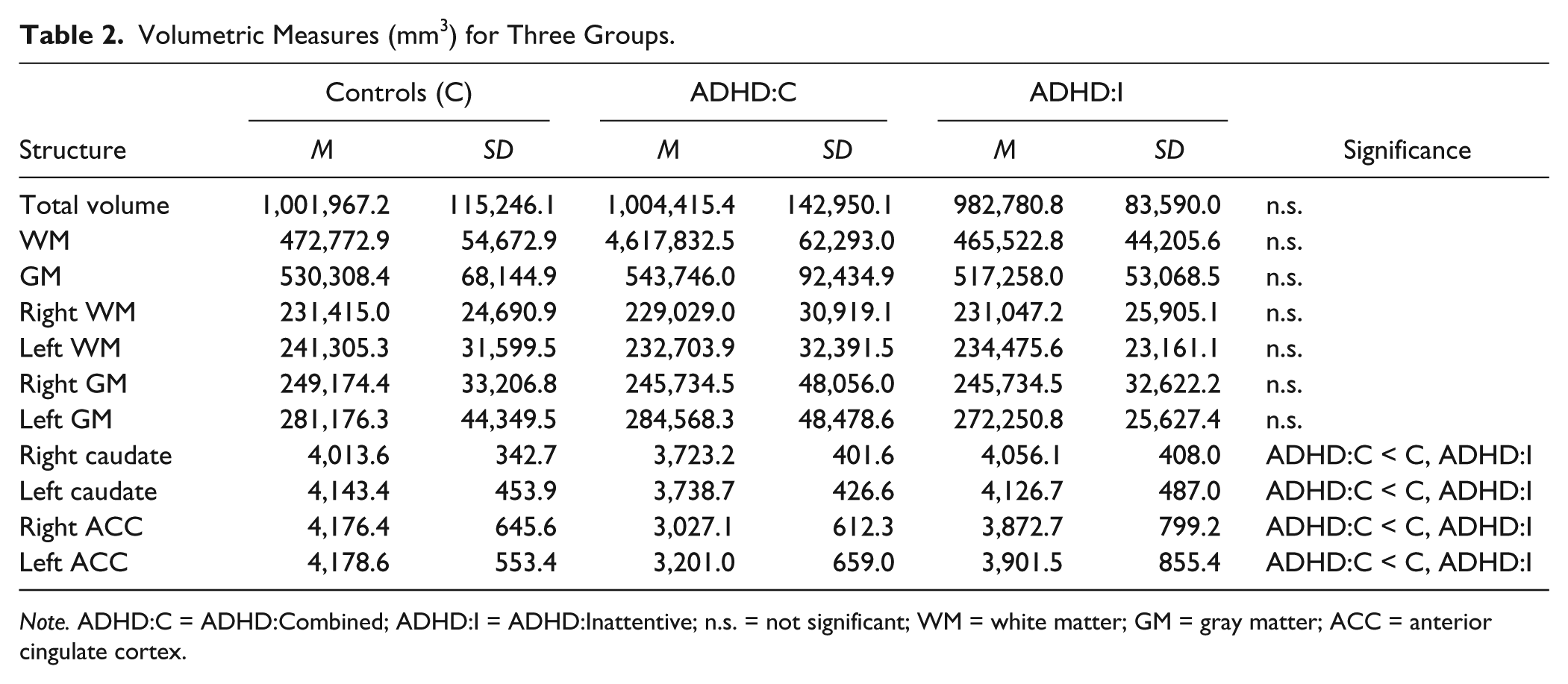
Note. ADHD:C = ADHD:Combined; ADHD:I = ADHD:Inattentive; n.s. = not significant; WM = white matter; GM = gray matter; ACC = anterior cingulate cortex.
A 3 (group) × 2 (right caudate, left caudate) MANCOVA with total brain volume as the covariate resulted in a significant group effect, F(4, 134) = 2.65, p = .03, partial η2 = .07. Follow-up ANCOVAs found a significant group effect for the right caudate (p = .01) and left caudate (p = .009). Post hoc analyses found that the children with ADHD:C had a smaller right caudate compared with the control (p = .016) and ADHD:I (p = .007) groups. The left caudate was significantly smaller in the ADHD:C group compared with the control (p = .006) and ADHD:I (p = .008) groups. There were no significant group differences between the ADHD:I and control groups (see Table 2 and Figure 3). This finding confirms our first hypothesis that the ADHD:C group would show smaller caudate volumes compared with controls.
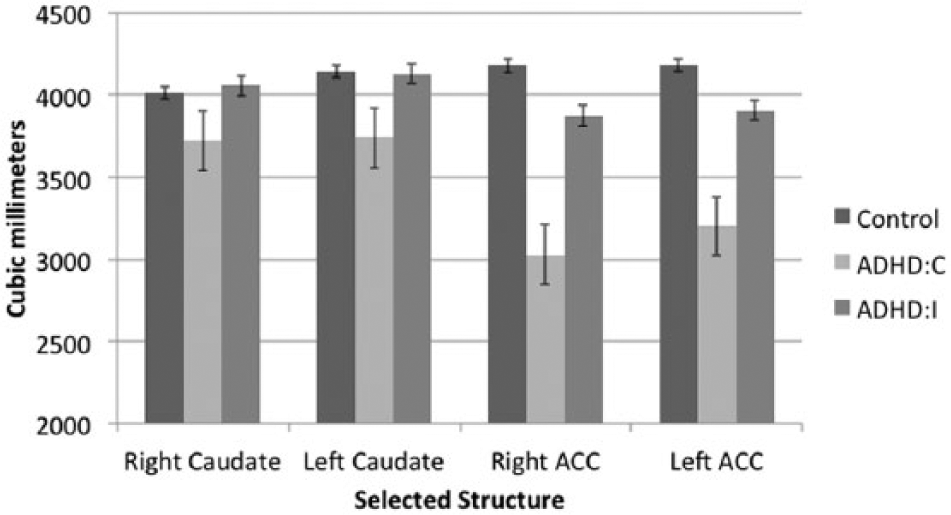
Volumes of selected ROIs.
Based on previous research it was hypothesized that the ACC cortex (ACC) would differ in the ADHD groups compared with controls. This hypothesis was confirmed only for the ADHD:C group. A 2 (right ACC, left ACC) × 3 (group) MANCOVA with total volume as a covariate was found to be significant, F(4, 136) = 8.3, p < .0001, partial η2 = .2, with a moderate effect found. Follow-up ANCOVAs found a significant group effect for the right ACC (p < .0001) and left ACC (p < .0001). Post hoc analysis found that ADHD:C group had the smallest ACC volumetric measures bilaterally compared with the control and ADHD:I groups (p < .0001). The ADHD:I group did not differ from the control group on the right ACC (p = .13) or left ACC (p = .18). This finding partially confirmed our second hypothesis, namely, that both ADHD groups would show significantly smaller ACC volumes compared with the control group. See Figure 3.
Relation of the Caudate and ACC Volume to Behavioral Measures
The correlation between the right and left caudate was high (r = .877, p < .001), thus separate regressions were conducted for the right and left caudate on parent ratings of attention and hyperactivity with total volume controlled. The models for both the right and left caudate were significant, suggesting that children with smaller caudate volumes are rated as having higher levels of hyperactivity. The right caudate and whole brain volume together explained 9.2% of the variance in hyperactivity scores (R2 = .092), F(2, 68) = 3.39 (p = .040), but only the right caudate was a significant predictor (β = −.306, p = .011, R2 change = .092), while total volume was not (β = .029, p = .807, R2 change = .000). Similarly, the left caudate was the only significant predictor of hyperactivity with whole brain volume in the model (caudate: β = −.338, p = .006, R2 change = .106; whole brain: β = .074, p = .539, R2 change = .000). The left caudate and whole brain volume together accounted for 10.6% of the variance in hyperactivity scores, R2 = .106, F(2, 68) = 3.99, p = .023. See Table 3.
Results of Simultaneous Regressions of BASC-2 Ratings on Regions Interest With Total Volume Controlled.
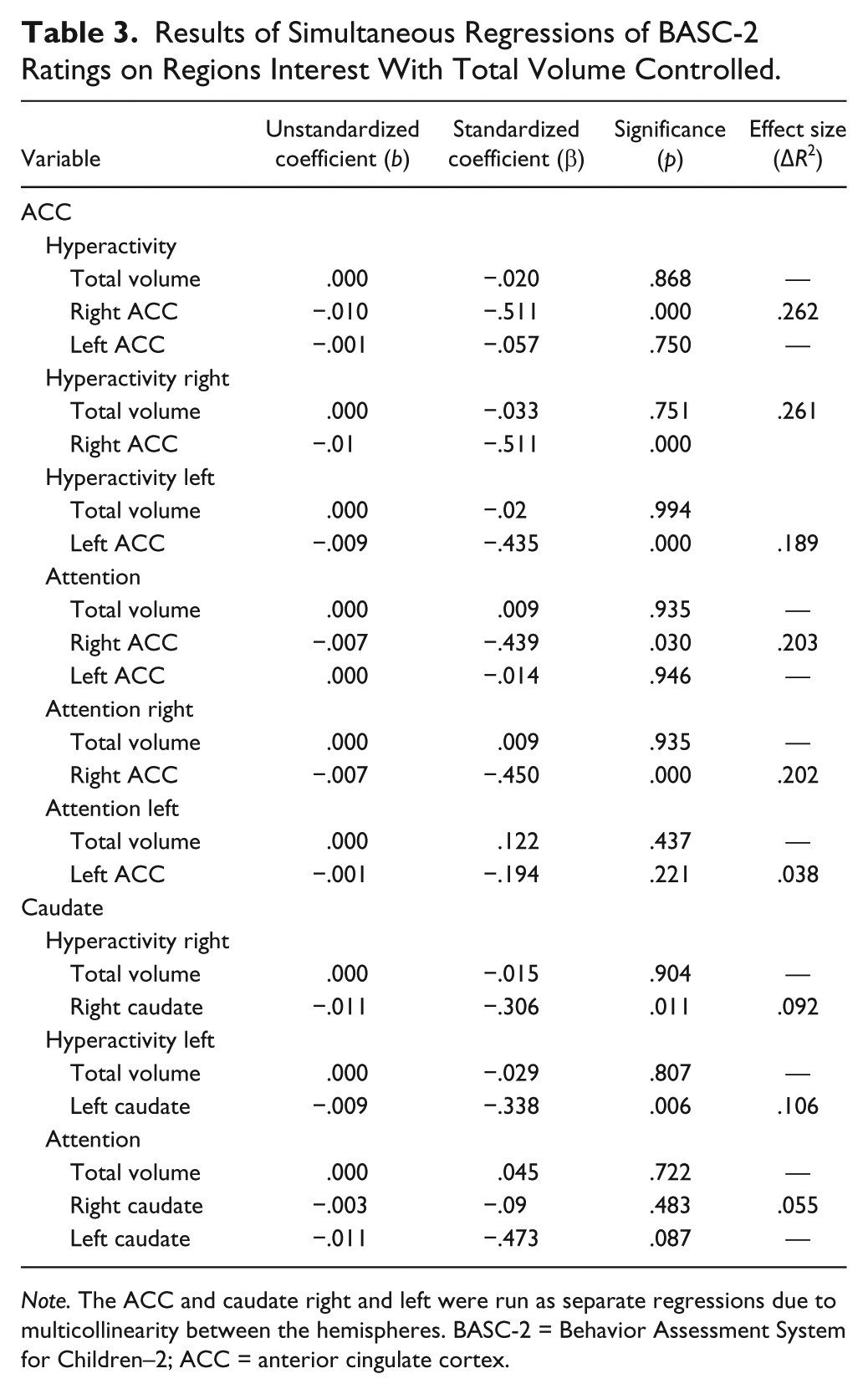
Note. The ACC and caudate right and left were run as separate regressions due to multicollinearity between the hemispheres. BASC-2 = Behavior Assessment System for Children–2; ACC = anterior cingulate cortex.
To test whether there was a relation between the caudate and the hyperactivity scale solely using the ADHD groups, a regression was performed. The model was significant for the caudate, R2 = .172, F(1, 40) = 2.78, p = .046, indicating that the 17% of the variance on the caudate measure can be accounted for by total brain volume and parent ratings of hyperactivity on the BASC-2. Along with total brain volume, the hyperactivity ratings had a small yet significant effect size on volume of the right caudate, ΔR2 = .17, F(1, 41) = 4.14, p = .023, and left caudate, ΔR2 = .16, F(1, 41) = 3.92, p = .028.
The correlation between the right and left caudate was high (r = .811, p < .0001), thus separate regressions were conducted for the right and left ACC on parent ratings of attention and hyperactivity with total volume controlled. To test whether the ACC volume was related to scores on the hyperactivity scale from the BASC-2, a regression of hyperactivity ratings on ACC volume measures with total brain volume controlled was performed. The model was significant for the ACC, R2 = .262, F(2, 68) = 12.075, p < .0001, indicating that 26% of the variance on the ACC measure can be accounted for by total brain volume and parent ratings of hyperactivity. Along with total brain volume, the hyperactivity ratings had a significant and moderate effect size on volume of the right ACC, ΔR2 = .261, F(1, 69) = 24.37, p < .0001, but not left ACC, ΔR2 = .001, F(1, 68) = 0.103, p = .75. Table 3 provides these data.
To test whether there was a relation between the ACC and the hyperactivity scale solely utilizing the ADHD groups without the control group, a regression was performed. The model was significant for the ACC, R2 = .25, F(1, 44) = 6.898, p = .003, indicating that 25% of the variance on the ACC measure can be accounted for by total brain volume and parent ratings of hyperactivity in the two ADHD groups. Along with total brain volume, the hyperactivity ratings had a significant and moderate effect size on volume of the right ACC, ΔR2 = .258, F(1, 42) = 7.28, p = .002, and the left ACC, ΔR2 = .189, F(1, 42) = 16.09, p = .001.
There was no significant relation between either the left or right caudate and BASC-2 inattention scores,
Discussion
We hypothesized that the ADHD:C group would show smaller caudate and ACC volumes compared with the control and ADHD:I groups. There is little empirical evidence as to what would be found for the ADHD:I group but we suggested that this group would show differences in the ACC but possibly not in the caudate. It was found that the bilateral caudate volumes were smaller for the ADHD:C group as hypothesized with no difference from the control group found for the ADHD:I group. Contrary to our hypothesis, the ADHD:I group did not show ACC volumes different from the control group.
We were also interested in the relation of the measures of attention and hyperactivity to both structures. We had anticipated that there would be a relation of the bilateral ACC to the BASC-2 parent ratings of attentional difficulties. This hypothesis was partially confirmed for the right ACC and the left ACC for the total group. In addition to testing this hypothesis for the total group, we conducted significance tests comparing the two ADHD groups. The regression for the right ACC on the BASC-2 attention scale with total brain volume controlled approached significance. It is likely that the test was underpowered to detect a small effect size.
Similarly, we had anticipated that there would be a relation between the caudate and attention and hyperactivity measures. This hypothesis was confirmed only for the right caudate and only for hyperactivity. When solely the ADHD groups were compared, there was a significant relation between bilateral caudate volume and the parent report of hyperactivity. The relation, although significant, was less robust then the relation found with the right caudate when the full group was utilized for analysis probably due to change in the variance. A relation between the caudate and the attention scale of the BASC-2 was not found to be significant when three groups were compared or when the ADHD groups were compared.
Differences in the caudate volume have been well documented by several researchers (Castellanos et al., 1994; Hynd et al., 1993; Semrud-Clikeman et al., 2006). A review of the literature on neuroimaging in ADHD:C found that the caudate nucleus is generally 10% smaller in these children compared with controls (Swanson, Castellanos, Murias, LaHoste, & Kennedy, 1998). Our finding of smaller caudate volume solely in the ADHD:C group is consistent with previous research and again was in the range of 10% smaller compared with neurotypical children.
Our finding of no statistically significant difference between the ADHD:I and control group strongly suggests a neural network difference for this group compared with the ADHD:C group. A resting-state functional connectivity MRI study comparing children with ADHD:C and ADHD:I also suggests that different neural networks are involved in these two disorders (Fair et al., 2013). Atypical connectivity in the midline network, which includes the caudate for the ADHD:C group, while the ADHD:I group showed differences in the dorsolateral prefrontal cortex and cerebellum was found in the Fair et al. (2013) study. While the Fair et al. (2013) study did not utilize structural analysis, the findings of differences in connectivity are consistent with our findings of caudate volumetric differences between the two subtypes.
It has been suggested that the network which includes the caudate and thalamus as well as the dorsolateral prefrontal cortex is related to the ability to stop activity or to use a “braking mechanism” (Castellanos, 1997). The reduced volume in the caudate likely correlates with the difficulty that children with ADHD:C experience in inhibiting their responses and in controlling their impulses. The finding of normal caudate volume for children with ADHD:I may be related to better control of impulsive responding seen in these children compared with those with ADHD:C.
The ACC orchestrates behavioral adjustments in behavior based on feedback as to performance (Bush et al., 2002). These skills are particularly compromised in children with ADHD:C. Children with ADHD:C have significant problems managing their own behavior, changing their behavior to fit the situation, and in reward-cost benefit analysis.
Structural imaging has found small volumes in the ACC (Semrud-Clikeman et al., 2006) and cortical thinning in this region as well in children with ADHD:C (Shaw et al., 2006) as well as with adults (Makris et al., 2008). In addition, we previously reported that thinning of the right ACC was related to increased parent-reported behavioral problems in a sample of children with ADHD:C (Bledsoe et al., 2013). Functional neuroimaging has found underactivation in this region in adults with ADHD (Bush et al., 1999) and in adolescent boys with ADHD (Tamm, Menon, Ringel, & Reiss, 2004). A meta-analysis of neuroimaging studies found hypoactivity in the regions of the dorsolateral prefrontal cortex, ventrolateral prefrontal cortex, superior parietal cortex, caudate, and thalamus as well as in the ACC (Dickstein, Bannon, Castellanos, & Milham, 2006; Lancaster, Laird, Fox, Glahn, & Fox, 2005; Seidman et al., 2006). This hypoactivity may be related to smaller ACC volumes in the ADHD:C group of this study.
Our finding of differences in volumes of the ACC and caudate between the ADHD:C and ADHD:I group lends additional support to the hypothesis that ADHD:I arises from a different neural substrate than ADHD:C. Our study was designed to evaluate selected regions of interest, and further study should evaluate additional areas that may be responsible for the inattention difficulties seen in ADHD:I. It may be that ADHD:C is the result of widespread frontal lobe dysfunction, while ADHD:I is related to difficulties based only on one of these systems; namely the dorsolateral system. This hypothesis is consistent with the findings from the Fair et al. (2013) study. It is also possible that ADHD:I is not due to structural differences but due to functional variance. Studies need to be conducted to determine whether there are functional differences between ADHD:C and ADHD:I using functional MRI or whether there are WM tract differences which could be investigated using diffusion tensor imaging.
Link of Volumetric Findings to Behavioral Ratings
We had hypothesized that volumes of the caudate and ACC would predict parent behavioral ratings of attention and hyperactivity. BASC-2 hyperactivity and attention scores were found to be related to the right ACC volumes, in that higher scores on these scales (poorer performance) were related to smaller volumes of the right ACC. This finding supports earlier work that demonstrated a brain–behavior relationship between right ACC cortical thickness and parent ratings of symptom severity in a population of children with ADHD:C (Bledsoe, Semrud-Clikeman, Pliszka, 2011). In contrast, the current study did not find differences in the volume of the ACC in those with ADHD:PI. This suggests that the causal pathway to ADHD:PI is likely different than ADHD:C and may not involve anatomical differences in the ACC. Again, this finding is consistent with previous research that suggests the ACC to be related to difficulty with monitoring, attention, and response inhibition (Bush, 2011). Given the neuroimaging findings of hypoactivation in this region, it is reasonable to speculate that this hypoactivation is related to smaller volumes and possibly less integrity of this structure in ADHD.
When a comparison was made using the ADHD groups without the control group, a small but significant effect was found for hyperactivity and the ACC bilaterally. Similarly, comparison of the caudate and the hyperactivity ratings also produced a significant, though small, effect bilaterally for the ADHD groups. This finding suggests that the relation between hyperactivity and brain volume measures is not due to group differences but rather due to a relation between the symptoms and volume. We did not find a relation between attention and the caudate for either the full group or using the ADHD groups. We did, however, find a significant relation between the ACC and attention, particularly with the right ACC for the total study but not for the ADHD groups analyzed separately.
Some support of these findings is found in neuroimaging studies of the cingulo–frontal–parietal cognitive/attention network. In this network, it is believed that the ACC is responsible for integrating information from inputs from the dorsolateral frontal and parietal attention networks allowing for planning and goal-setting. Disruption of this network results in problems with hyperactivity and impulse control (Bush et al., 2013). Similarly, the ventral network is important for focusing attention and suppressing distractibility working through the ACC (Liston, Matalon, Hare, Davidson, & Casey, 2006). These results are consistent with our findings of a relation of the volume ACC to attention and hyperactivity.
In conclusion, we found structural differences in the ADHD:C group compared with children with ADHD:I and controls in the caudate and ACC. In both cases, the ADHD:C group had smaller volumes on the right. We also found a significant relation between parent behavioral ratings of attention and hyperactivity and the bilateral volumes of the ACC and bilateral caudate. It remains to be seen whether children with ADHD:I have differences in other regions of the brain that can account for the attentional difficulties seen.
Limitations
As with any neuroimaging study, one of the limitations is the number of participants. In this study, we could not achieve a gender-matching population for each group. While gender differences in regional brain volumes were not found in our study, the number of girls in the overall sample was very limited. We also could not control for medication status due to the relatively small size of the population. There is a possibility that medication history may be related to differences. Again, there were not sufficient numbers of children to test the effect of medication on these results, and so, medication history is also a limitation. There is a 10-point difference in IQ among the groups, which while not significant may have affected the results. Most recent studies suggest that brain volume is not strongly associated with IQ in typically developing children aged 4 to 18 years (Brain Development Cooperative Group, 2012). Finally, our children did not have comorbid disorders; something that is frequently seen in children with ADHD. We decided to do so to attempt to limit confounding factors. This exclusion makes our findings less generalizable to the population as a whole.
Footnotes
Acknowledgements
Neuroimaging scans were provided by the Department of Radiology at the Michigan State University for which the authors are very thankful.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for Drs. Semrud-Clikeman, Fine, and Bledsoe was provided by the Departments of Psychiatry and Psychology.