
Abstract
College presents unique challenges to students with ADHD. These students have been referred to as having a “double-deficit” (Fleming & McMahon, 2012) due to ADHD, emerging adulthood, and the college environment. First, individuals with ADHD struggle with attention, impulse control, and activity-level modulation (American Psychiatric Association [APA], 2013). Second, the developmental stage of emerging adulthood (ages 18-25; Arnett, 2000) is characterized by greater independence than adolescence but cognitive development that is not yet complete. Finally, the college environment is one in which students are experiencing an abrupt decrease in parental support as well as an increase in temptations and distractions.
Likely for these reasons, emerging adults with ADHD who seek postsecondary education are at higher risk for poor academic achievement and are less likely to graduate from college than their typically developing peers (Barkley, Murphy, & Fischer, 2008; Frazier, Youngstrom, Glutting, & Watkins, 2007; Heiligenstein, Guenther, Levy, Savino, & Fulwiler, 1999; Kuriyan et al., 2013). DuPaul, Weyandt, O’Dell, and Varejao (2009) estimated that 2% to 8% of college students met diagnostic criteria for ADHD and that 25% of students receiving disability services were diagnosed with ADHD.
As with other age groups, the treatments available to college students with ADHD include medication and psychosocial treatments. Stimulant medications (e.g., methylphenidate) are frequently prescribed for college students with ADHD (Baverstock & Finlay, 2003) although there is significantly less research on their effectiveness with this age group than with children, adolescents, and adults who are beyond the emerging adulthood stage. The studies that have been conducted with college students are equivocal. Although college students with ADHD report that stimulant medication helps them academically (Advokat, Lane, & Lou, 2011), studies have found that the grade point averages (GPAs) and the overall adjustment to college of students receiving medication treatment for ADHD did not significantly differ from nonmedicated students (Advokat et al., 2011; Rabiner, Anastopoulos, Costello, Hoyle, & Swartzwelder, 2008).
These medications are moderately effective in improving concentration in those with ADHD; yet, they have a number of limitations (Hartung, Canu, Cleveland, et al., 2013; Wilens, Biederman, & Spencer, 1998). For example, psychostimulants have main effects that are limited to the hours in which they are pharmacologically active, are ineffective or intolerable in up to half of adults, and residual symptoms are common (G. Weiss & Hechtman, 1993; Wilens, Biederman, & Spencer, 2002). In our clinical experiences, stimulants tend to improve core symptoms of ADHD (e.g., concentration and distractibility) but not skills associated with academic success (e.g., organization and time management). Finally, there is concern about stimulant misuse and diversion among college students (e.g., Hartung, Canu, Cleveland, et al., 2013; Rabiner et al., 2009; Weyandt & DuPaul, 2008). More specifically, Hartung, Canue, Cleveland, and colleagues (2013) found that college students who have prescriptions for stimulants often do not take the medication regularly and, as a result, may have extra available to share with, or sell to, others. Given the concerns regarding the overall costs and benefits of stimulants, adjunctive psychosocial interventions are often recommended (Dulcan & Benson, 1997; Prince, 2006; Wilens et al., 1998). Unfortunately, few empirical reports testing the efficacy of psychosocial interventions for ADHD among college students have been published (for an exception, see LaCount, Hartung, Shelton, Clapp, & Clapp, 2015).
Although significant work remains to be carried out, cognitive-behavioral therapy (CBT) has been recommended for treating college students with ADHD, as it appears to be the most effective psychosocial treatment for ADHD among nonemerging adults (Ramsay & Rostain, 2006). Several psychosocial interventions for adults with ADHD have been shown to be efficacious in randomized control trials (Knouse, Cooper-Vince, Sprich, & Safren, 2008). Preliminary efficacy studies have yielded promising results for individual CBT (Rostain & Ramsay, 2006; Safren et al., 2010; Virta et al., 2010), group CBT (Salakari et al., 2010; Solanto et al., 2010; Stevenson, Whitmont, Bornholt, Livesey, & Stevenson, 2002; Virta et al., 2008, Wiggins, Singh, Getz, & Hutchins, 1999), coaching (Allsopp, Minskoff, & Bolt, 2005; Kubik, 2010; Swartz, Prevatt, & Proctor, 2005; Zwart & Kallemeyn, 2001), and group mindfulness training (Hesslinger et al., 2002; Mitchell, Zylowska, & Kollins, 2015; Philipsen et al., 2007; Zylowska et al., 2008). Unlike medication, psychosocial interventions provide adults with skills to ameliorate some of the primary functional impairments of ADHD. Overall, results have suggested that psychosocial interventions for adults with ADHD are effective in ameliorating core symptoms and functional impairment; however, no component studies evaluating how useful or efficacious treatment elements appear to be have been performed. Focused investigations on the efficacy of intervention components are necessary to determine the most efficient, effective, and cost-effective combination of intervention components.
In a review of treatments used to address the challenges of adults with ADHD, we divided the multicomponent approaches as a first step toward identifying the “active ingredients” of the psychosocial interventions (Hartung, Lefler, LaCount, Mancil, & Canu, 2012). Common elements of existing programs included psychoeducation; organization, time management, and planning skills (OTMP); memory management; study skills and accommodations; increasing attention span; adaptive thinking; and mindfulness. Among the components of existing psychosocial treatments for adults, the targeting of deficits in OTMP seems to be particularly relevant to college students with ADHD.
Disorganization and inattention appear to be the primary factors of impaired functioning among college students, especially in the area of academics. These symptoms have been associated with poorer time management, and being absent from or tardy to classes, meetings, and work (Kern, Rasmussen, Byrd, & Wittschen, 1999; Meaux, Green, & Broussard, 2009; Schwanz, Palm, & Brallier, 2007). Therefore, OTMP skills training interventions seem appropriate for college students with ADHD because they have significant impairments in organization that may contribute to the observed difficulties in academic achievement.
For many emerging adults with ADHD, impairment in three domains of functioning specific to the college environment—OTMP—often persist into adulthood, when ADHD is associated with greater risk of unemployment, financial difficulties, depression, anxiety, relationship difficulties, and poor life satisfaction (Biederman et al., 2006). From this, it has been hypothesized that treatment approaches targeting the skills that seem relevant to academic functioning (e.g., OTMP) could be crucial in improving short- and long-term functioning in college students with ADHD (Fleming & McMahon, 2012; Green & Rabiner, 2012). Thus, there is a need for trials targeting OTMP skills with college students to evaluate the efficacy of such targeted interventions.
The aim of the current study was to provide a preliminary evaluation of an OTMP skills training intervention with a sample of college students reporting elevated levels of inattention or hyperactivity/impulsivity ADHD symptom severity (hereafter referred to as ADHD-I and ADHD-H/I, respectively) and elevated levels of academic impairment. The primary dependent measures were ratings of academic impairment, use of OTMP skills (e.g., calendar, task lists), and ADHD-I and ADHD-H/I. In testing the feasibility of an OTMP skills training intervention for college students with ADHD and academic impairment, it was hypothesized that participants who received the intervention would improve more significantly from pre- to postmeasurement of ADHD-I, ADHD-H/I, use of OTMP skills, and academic impairment relative to a comparison group. In addition, it is critical that treatment development researchers examine change on more distal outcomes to evaluate the impact of an OTMP intervention on academic performance (for a more in-depth discussion, see Chronis-Tuscano, Chacko, & Barkley, 2013; Sonuga-Barke et al., 2013). Therefore, we sought to evaluate the extent to which change in OTMP skills affect more distal outcomes, such as academic performance (i.e., GPA). Last, treatment feasibility and acceptability were assessed to supplement the primary analyses and guide future treatment development.
Method
Participants
Participants in this study included undergraduate students enrolled in psychology courses at the University of Wyoming who completed research as a course requirement or for extra credit. Participants were eligible for the study if they completed the psychology department prescreener and scored 1 SD above the sample mean on a measure of self-reported ADHD-I or ADHD-H/I (APA, 2013) and 1 SD above the mean on a measure of academic impairment. Students indicating that they are currently receiving psychosocial treatment for ADHD were excluded from participating in the study because the treatment might overlap with the OTMP skills training intervention.
Differences in students’ schedules and the policies for assigning research credit precluded us from using random assignment. Participants meeting the inclusion criteria were first emailed an invitation to participate in a 3-week-long academic skills study in exchange for course credit (i.e., intervention group). Those who declined to participate in the intervention group or had a scheduling conflict with the group meeting times were invited to participate in an online study in which they completed a set of online questionnaires on two occasions during the school semester in exchange for course credit (i.e., comparison group).
Figure 1 outlines the participant recruitment process. Of the 41 students who participated in the study, 25 enrolled in the intervention group and 16 enrolled in the comparison group. A total of 4 participants were excluded from analyses. Specifically, one comparison group participant did not complete any of the postmeasures and two intervention group participants were research assistants in our lab. One intervention group participant was omitted because he or she was undergoing an ADHD assessment, and eventually received therapeutic services, from the intervention group leader. Characteristics of the final sample (N = 37) are provided in Table 1. This study was reviewed and approved by the local institutional review board (IRB).
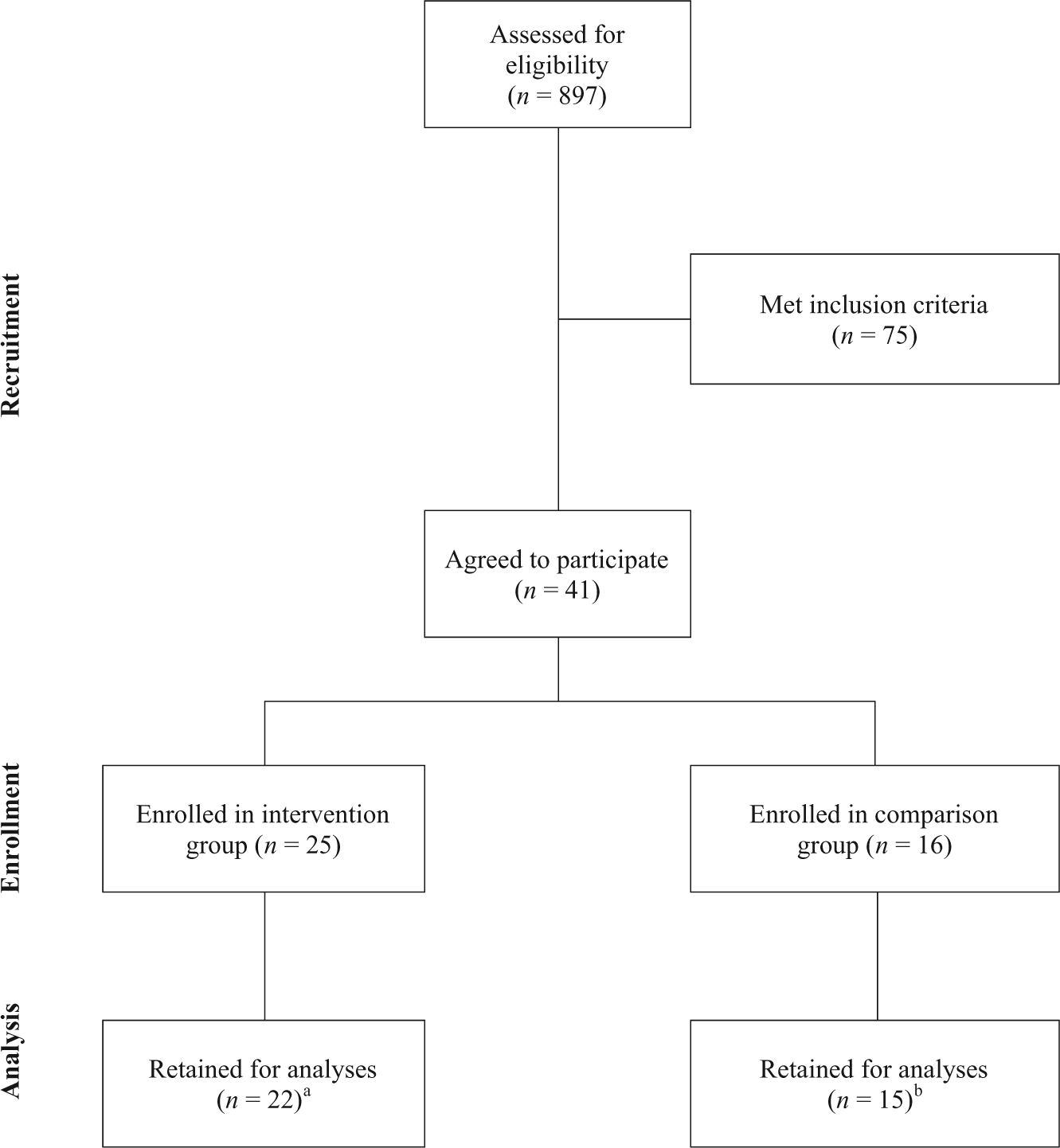
Sample recruitment and participation flowchart.
Baseline Demographics and Clinical Characteristics by Condition.

Note. The table does not include the data of the participants who were omitted from outcome analyses (n = 4). GPA = grade point average; ACT = American College Test; ADHD diagnosis = reported to have received a diagnosis of ADHD; ADHD medication = reported to be taking ADHD medication during the study.
p values are two-tailed.
Eleven students were completing their first semester of college and therefore had no college GPA to report.
Nine students did not indicate their ACT composite score.
Courses from which the student withdrew were not included in calculating the number of credits they were enrolled in during the semester of the study.
Fisher’s (1992) exact test was employed given the low frequency count within cells.
Measures
Barkley Adult ADHD Rating Scale–IV (BAARS-IV)
This form (Barkley & Murphy, 2006) includes 18 items that closely follow the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-V; APA, 2013) criteria for ADHD. Participants were asked to rate their current behavior from 0 (never/rarely) to 3 (very often). The scale has demonstrated good internal consistency for college students for Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) hyperactivity/impulsivity (α = .86) and DSM-IV inattention (α = .84; Fedele, Lefler, Hartung, & Canu, 2012). The present study used the total scores for the nine inattention symptom items and nine hyperactivity/impulsivity symptom items as measures of symptom severity.
Weiss Functional Impairment Rating Scale (WFIRS)
The WFIRS (M. D. Weiss, 2000) is a 70-item measure designed to measure current ADHD-related impairment across seven domains of functioning (i.e., Family, Work, School, Life Skills, Self-Concept, Social, and Risk). Hartung, Canu, Lefler, and colleagues (2013) reported good internal consistency for Family, Life Skills, Social, and Risk subscales (α = .86, α = .89, α = .88, and α = .88, respectively) and excellent internal consistency for Work, School, Self-concept, and Total Impairment subscales (α = .91, α = .90, α = .94, and α = .96, respectively). Hartung, Canu, Lefler, and colleagues also reported a strong correlation (p < .001) between the impairment subscales and ratings of current inattention (r = .45 to r = .68) and hyperactivity/impulsivity (r = .38 to r = .60). In the current study, the School subscale was used as a measure of academic impairment and contains items asking participants to rate how often they have problems in various domains of academic functioning (e.g., completing assignments, getting work done efficiently, attending class, being late). Only the School subscale of the WFIRS was included in outcome analyses.
Course grades
At the end of the semester in which students participated in the study, course grades were collected for all study participants. The colleges at the university used the same scale for grades where A = 4.0, B = 3.0, C = 2.0, D = 1.0, and F = 0.0. GPA for the semester was calculated as the average of participants’ class grades. Courses with dichotomous grading scales (i.e., satisfactory or unsatisfactory) were not included in the computation of the semester GPA.
OTMP Skills Utilization Scale
This form contains 12 items asking participants to indicate how many days in the past week they used specific OTMP skills and strategies (e.g., put appointment into calendar, rating importance of task on to-do list). This measure was created for the current study and the items correspond to the use of the skills taught in the OTMP intervention. The OTMP total score demonstrated good internal consistency in the current sample (α = .89).
Treatment Acceptability Questionnaire
In addition to outcome measures, the acceptability of the OTMP group intervention was assessed with a nine-item questionnaire. The majority of items assessed the usefulness of specific treatment components in improving their OTMP abilities. For example, participants in the OTMP group were asked to rate the usefulness of a daily planner to manage their schedules in improving their OTMP. Participants indicated the usefulness with each statement on a 5-point Likert-type scale from 0 (not at all useful) to 4 (very useful). In addition, participants were asked to provide qualitative feedback on the intervention.
Procedure
Over the course of 7 weeks, intervention and comparison group participants were scheduled to complete pre- and postratings. All participants completed the aforementioned questionnaires through Survey Monkey, an online survey software. It was estimated that the set of questionnaires would take an hour to complete and allowed participants to take breaks as long as they did not close out of their web browser and exit the survey. Intervention group participants were also required to attend three OTMP intervention sessions. In addition to earning research credit for their participation, participants in the intervention group earned raffle tickets for each scheduled meeting they attended and five additional tickets for attending all planned meetings (i.e., “perfect attendance”). At the end of the study, one participant won an iPad Mini. Throughout the study, researchers sent electronic reminders to participants (i.e., text messages, emails) the day prior and the day of scheduled group meetings.
OTMP intervention
The OTMP intervention delivered in this study was a condensed adaptation of the treatment protocol developed by Solanto, Marks, Mitchell, and Wasserstein (2011) to help adults cope with ADHD. The treatment developed by Solanto and colleagues (2011) included 12 sessions that covered several topics, such as psychoeducation about ADHD, but largely focused on developing, implementing, and maintaining OTMP skills. The intervention in the current study was delivered in three weekly, 1-hr group sessions in the evening, with each session targeting specific OTMP skills. Although not mandatory, take-home exercises were dispersed to participants at the end of the first two sessions and collected at the beginning of the meeting following the one in which they were originally handed out.
Session 1: Time awareness and scheduling
This session consisted primarily of the introduction of task list and calendar systems and the use of timepieces (e.g., watches, clocks) to improve time management. The group leader also helped each participant decide on an organizational system to start using (e.g., paper-and-pencil planner, Wunderlist, Google calendar). The participants were instructed to write all appointments in their calendars and to begin constructing “to-do” lists. As part of their take-home exercises, they were instructed to keep a log of everything they did on a weekday of their choice during the next week to help determine how they used their time. They were also tasked with estimating how long specific tasks took for them to complete (e.g., getting ready in the morning, completing a school assignment) and then record how long the tasks actually took during the next week.
Session 2: Task and motivation management
During this session, participants were presented with the strategies for making tasks more manageable and how to increase motivation through strategies, such as contingent self-reinforcement. During the session, the group leaders facilitated in-session exercises that included breaking down a large task into more manageable “chunks” and generating personal reward lists. Students were instructed to schedule and complete one or more small tasks and continue time-logging and time-estimation exercises as needed during the next week.
Session 3: Implementing an organizational system
In this final session, participants were presented with strategies for identifying priorities, using planners for prioritizing tasks, transferring items from to-do lists to schedules. Students were instructed to schedule to-do list items and assign priority to tasks for a week. To facilitate the latter, participants classified tasks within one of four quadrants in an importance grid (urgent and important, not urgent and important, urgent and not important, and not urgent and not important; Covey, 1991).
Analytic Approach
Independent-samples t tests and chi-square models for continuous and categorical variables, respectively, were performed to examine the differences in the demographic and baseline clinical characteristics of the two groups and baseline differences between groups across primary outcome variables (i.e., academic impairment, ADHD symptom severity, and OTMP utilization). Fisher’s (1922) exact test was used in place of chi-square when the frequency count within cells was low (n < 5). Next, differences in academic impairment, OTMP utilization, and ADHD-I and ADHD-H/I severity across conditions were examined through multiple 2 (Group: OTMP and comparison) × 2 (Time: pre- and postintervention) repeated-measures ANOVAs. When Group × Time interactions were significant, paired-samples t tests were used to evaluate differences within groups. When Group × Time interaction effects did not reach significance, independent-samples t tests were used to evaluate differences between groups on postintervention measures. Assuming there are minimal differences between groups on their baseline ratings, these analyses provide a parsimonious model for exploring group differences across the primary outcome variables that preclude violations of sphericity in designs with three or more repeated measures (Vasey & Thayer, 1987). Last, we wanted to explore the possible impact of the intervention on more distal measures of functioning. Therefore, independent-samples t tests were used to compare the end-of-semester GPAs between the two groups.
The magnitude of omnibus effects for repeated-measures ANOVAs was calculated using partial eta squared (
Results
Baseline Equivalence
Chi-square models and independent-samples t tests demonstrated equivalency between the intervention (n = 22) and comparison groups (n = 15) on all but one demographic variable (see Table 1). Specifically, there was a larger proportion of women in the comparison group (80%) than the intervention group (55%; p = .04). Independent-samples t tests demonstrated pretreatment equivalence between the intervention and comparison groups on academic impairment (p = .25), OTMP skills utilization (p = .48), ADHD-I (p = .50), and ADHD-H/I (p = .08).
Primary Outcome Analyses
Academic impairment
Academic impairment evidenced a large Group × Time interaction effect (p = .02,
Comparison of Outcomes at Posttreatment.

Note. School = academic impairment; OTMP = organization, time management, and planning skills utilization; ADHD-I = ADHD–inattention symptom severity; ADHD-H/I = ADHD–hyperactivity/impulsivity symptom severity.
Effect size for within-group pairwise comparisons of intervention group participants, standardized using variability of scores at baseline.
OTMP skills utilization
Although postmeasures of OTMP skills utilization was higher among participants in the OTMP intervention group (M = 42.27, SD = 25.94) than in the comparison group (M = 28.67, SD = 17.56), there was not a significant Group × Time interaction effect for OTMP skills utilization (p = .20,
ADHD-I symptom severity
A medium-sized Group × Time interaction was observed for ADHD-I (p = .04,
ADHD-H/I symptom severity
ADHD-H/I evidenced a large Group × Time interaction effect (p < .001,
Semester grades
Independent-samples t tests were used to compare semester GPAs between groups. There were no statistically significant differences between participation semester GPAs for students in the comparison group (M = 2.74, SD = 0.85) and the intervention group (M = 2.40, SD = 1.09; p = .32 g = .33).
OTMP Feasibility and Acceptability
Regarding treatment feasibility, all 25 of the participants in the intervention group completed the study, whereas 1 of the 16 in the comparison group participants did not complete the study (see Figure 1). On average, intervention group participants attended 2.78 (SD = 0.44) out of three sessions, which is an attendance rate of 92%. No intervention group participant missed more than one session and only 6 participants missed one session. Although completing the two take-home exercises was not compulsory for participants to earn research credits or raffle tickets, the completion rate of the two take-home exercises for participants who attended the group meeting in which the exercises were assigned was 82%.
Treatment acceptability was evaluated through intervention group participants’ open-ended responses on a poststudy questionnaire. Examination of item mean scores revealed that participants felt that using a calendar to manage their schedule (M = 3.3, SD = 0.9) and breaking down large tasks into more manageable tasks (M = 3.2, SD = 0.7) were the most useful skills for improving their OTMP abilities. Students also reported that they would feel comfortable recommending this intervention to a friend (M = 2.9, SD = 0.9) and felt confident in their ability to continue to use the strategies learned in the intervention in the future (M = 2.7, SD = 1.1).
Participants’ responses also indicated that the two least helpful OTMP skills were wearing a watch (M = 1.9, SD = 1.8) and using time awareness exercises (M = 2.3, SD = 1.4), such as completing an hourly activity log or estimating how long a task will take to complete, completing the task, and comparing the predicted time with the actual time. Indeed, when students were asked to provide feedback on the intervention, many commented that less emphasis should be placed on wearing a watch. For example, many noted they typically have access to various sources of time (e.g., phones, computers, wall clocks).
Discussion
The present investigation evaluated the acceptability, feasibility, and preliminary efficacy of an OTMP group intervention for college students who self-reported elevated levels of inattention or hyperactivity/impulsivity and academic impairment. The hypotheses that academic impairment, ADHD-I, and ADHD-H/I would improve for participants in the intervention group relative to a comparison group were supported with medium to large effect sizes. These results are consistent with previous research published on OTMP skills interventions for ADHD among children and adolescents (e.g., Abikoff et al., 2013; Langberg, Epstein, Becker, Girio-Herrera, & Vaughn, 2012), as well as the results of more time-consuming, multicomponent treatments for adults with ADHD (e.g., Safren et al., 2010; Solanto et al., 2010). The hypothesis that OTMP skills utilization would improve over time for participants in the intervention group relative to the comparison group was partially supported. Although results indicated that participants in the intervention group improved in their use of OTMP skills and participants in the comparison group exhibited no reliable change in their use of OTMP skills, the improvements among participants in the intervention group were not reliably greater than those in the comparison group. Last, the exploratory analyses did not yield results supporting that a brief OTMP intervention can have significant effects on participation semester grades.
In addition, the results indicated that a group-based OTMP intervention is feasible and acceptable. All of the OTMP group participants completed the intervention, the vast majority of the participants attended all three group sessions, and a large portion of the participants completed all the take-home exercises—the last being particularly compelling because the earning of raffle tickets and research credits was not linked to completing the take-home exercises. Participants’ evaluations of the intervention were strong as well, which indicated they felt the content was relevant to improving their academic functioning, felt confident about continuing to use the strategies in the future, and would recommend the intervention to a peer. Overall, the results suggest that a brief group intervention targeting OTMP skills for college students with elevated academic impairment and ADHD symptomatology is promising for improving academic functioning (e.g., completing assignments, working efficiently, attending class, arriving to appointments on time) and ameliorating inattention and hyperactivity/impulsivity.
Participants’ reported use of OTMP skills, regardless of whether they were in the intervention or comparison condition, increased from pre- to postassessment. However, the differences between groups in the degree to which they improved in this area was not significant. This surprising finding may have important implications for investigating and developing treatments for college students with ADHD.
One possible explanation for these findings is that completing the pretest measures may have made participants more aware of the importance of OTMP skills, leading to both groups being more focused on these skills over the course of the study. That is, the completion of the baseline measures, in and of themselves, may have served as a mild intervention for improving time management and OTMP skills utilization. Yet, it may be that the resulted improvements in these areas are not enough to improve inattention, hyperactivity/impulsivity, and academic impairment. Another possibility is that college students’ reporting on these measures may have been subject to demand characteristics and social desirability. That is, being asked to report on their organization and time management at the beginning and end of the studies may have inadvertently cued the college students to report behaviors that they know they should be doing (e.g., chunking out large assignments rather than procrastinating) rather than what they were actually doing. Last, the questionnaire used to assess OTMP skills utilization was constructed for this study and its psychometric properties have not been formally evaluated beyond internal consistency among this sample. For example, giving equal weight to an item asking students to report how many times in the last week they wore a watch with an item asking them to report how many times they reviewed their calendar may have negatively impacted the validity of the questionnaire—especially when considering that participants’ responses indicated that wearing a watch was the least helpful component of treatment.
Limitations
Although the results from this investigation are encouraging, there are limitations to this preliminary study. First, treatment outcomes were examined by primarily using subjective self-report measures with the exception of semester grades. Although the primary outcome variables, with the exception of the OTMP Skills Utilization Scale, have evidenced valid and reliable properties in psychometric investigations, the data obtained through self-report are less detailed, and more subjective, than what would be obtained through observational methods. That is, participants may not be able to provide the level of detail that the researcher is interested in obtaining. For example, it would have been valuable to explore how participants used their calendar (e.g., smartphone, paper calendar) to evaluate the relative efficacy of different schedule management approaches. Furthermore, the gains observed in students in the intervention condition through self-report measures may have been confounded by various biases, such as social desirability bias (Demaio, 1984). Reported behaviors may have deviated from actual behavior in fear of being perceived as uncooperative. Therefore, future investigations should include more objective (e.g., collateral reports of ADHD symptoms) and more distal outcome measures (e.g., homework completion, exam performance). However, these outcome measures that have been used with children and adolescents are difficult to use for college students. For example, the course work, class grade distributions, and credit loads can vary considerably between college students and results in a lot of “nuisance” variance. This makes detecting reliable differences between groups on semester grades, for example, difficult unless the sample is very large. Even when an intervention emphasizes OTMP skills, is more time intensive (i.e., eight group CBT session and one-on-one peer mentoring), and results in similar improvements in ADHD symptomatology and academic functioning with a sample approximately twice the size of the current study, semester GPA remains constant (Anastopoulos & King, 2015).
Second, participants were not randomly assigned to conditions and this increases the likelihood of spurious therapeutic effects (Lilienfeld, Ritschel, Lynn, Cautin, & Latzman, 2014). Although baseline measures, demographic measures, and clinical characteristics were approximately similar, with the exception of sex, we cannot be certain that the treatment effects were not due to other possible group differences that were not measured. There were likely preexisting differences between students who enrolled in a study requiring attendance at three weekly group meetings (i.e., intervention group) and those who elected to instead participate in a two-part online survey study (i.e., comparison group). For example, those who elected to participate in the relatively time-intensive OTMP intervention may have been more motivated to adopt skills to improve their performance in their classes. Given this limitation, the results of this study should be considered preliminary, and replication is warranted.
Third, generalization of the current findings is limited to college students reporting elevated inattention or hyperactivity/impulsivity and academic impairment, and not necessarily those diagnosed with ADHD. The participants were also not seeking help to ameliorate their ADHD symptoms and ADHD-related impairment so they likely were less motivated to adopt the skills than individuals who are seeking treatment would be. Thus, the sample is probably best defined as college students self-reporting elevated levels of ADHD-related behaviors and academic difficulties and agreeing to participate in a study in exchange for course credit. So although the sample may be compromised by the lack of similarities shared with those who seek treatment for their ADHD symptoms and impairment, the external validity of the sample is rather suitable for such an intervention.
Last, the limited sample size underscores the need for replication of the findings. In addition, the small sample likely attenuated the probability of detecting statistically significant effects on some of the primary outcome measures with small effect sizes. This may explain the lack of significant findings on the change in use of OTMP skills, because intervention effects were smaller than the other outcome measures. The small sample also hindered our ability to run adequately powered analyses to evaluate theoretical mechanisms of change (e.g., change in OTMP skills utilization as mediator for improvements in other primary outcome variables) or assess possible moderators of treatment effects (e.g., ADHD medication status, sex). Although a small sample size was a hindrance to some conclusions that could be formed from this study, it is encouraging that we found medium- to large-sized improvements across most outcome measures despite being limited by sample size.
Future Directions
Although a brief OTMP intervention appears to have promise for improving academic functioning and decreasing inattention and hyperactivity/impulsivity symptom severity, there is considerable work to be done in developing and disseminating effective interventions for this population. First, more work is needed to develop reliable and valid OTMP skills utilization measures and outcome measures that are uniquely tailored to the college population. Research on the psychometric properties of distal outcome measures for this population is particularly scarce. Future investigations should evaluate factors that contribute to the large variability in distal measures of academic performance (e.g., GPA). Given that both groups in the present study evidenced improvements in OTMP skills utilization, researchers should evaluate the efficacy of modifying the present OTMP-focused treatment design to better foster improvements in these domains—such as increasing the length of the intervention to increase “dosage” and allow for further practice of the OTMP skills. Moreover, researchers should use designs that allow investigators to assess the positive effects of a shorter OTMP intervention relative to a multicomponent intervention to better understand whether the individual OTMP component is equally effective to a more comprehensive intervention. Studies including an active comparison group, where students receive therapist attention, will allow for the potential impact of nonspecific therapeutic effects to be measured. In addition, we only examined treatment outcomes in terms of pre- and posttreatment differences. Future studies should investigate the maintenance of gains by including a follow-up period and possible mechanisms of change (e.g., calendar usage). It may also be that this intervention will work well for some college students, but less well for others. For instance, this treatment may not work well for college students experiencing co-occurring depression and anxiety. Thus, future studies are necessary to answer questions about moderators of treatment response.
Conclusion
Consistent with previous studies on interventions for children and adolescents with ADHD (e.g., Abikoff et al., 2013; Langberg et al., 2012), the present investigation demonstrated that interventions focusing on OTMP skills have potential for meaningful improvement in ADHD symptomatology and academic impairment in college students. This intervention may be an appropriate first-line approach for treating college students with ADHD symptomatology because it yields similar effects as stimulant medications (Wilens et al., 1998) with relatively lower risk of deleterious effects (Hartung, Canu, Cleveland et al., 2013; Rabiner et al., 2009; Weyandt & DuPaul, 2008) and is more efficient, feasible, and cost-effective than multidimensional treatment programs (e.g., Safren et al., 2010; Solanto et al., 2010). Further investigations of interventions focusing on organizational skills are needed to substantiate the efficacy of this treatment approach. However, these data suggest a low-intensity (3-week) group intervention for college students with ADHD-related academic impairment can produce robust changes in inattention, hyperactivity/impulsivity, and academic functioning. In turn, these improvements may enhance students’ test performance, assignment quality, rates of homework completion, and likelihood of graduating from college.
Footnotes
Acknowledgements
We thank the college students who participated and our colleague Joshua D. Clapp for assisting in preparing the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article is based on the first author’s master’s thesis and was supported in part by a research grant from the University of Wyoming, Lillian Portenier Trust Fund.