
Abstract
Introduction
Because of its empirical nature, its excellent psychometric properties and its ease of use as a self-report instrument, the Child Behavior Checklist (CBCL; Achenbach, 1991) has been examined as a potential tool to aid in identifying children at high risk of deficits in emotional regulation (Althoff, Rettew, Faraone, Boomsma, & Hudziak, 2006; Faraone, Althoff, Hudziak, Monuteaux, & Biederman, 2005; Hudziak, Althoff, Rettew, Derks, & Faraone, 2005; Mick, Biederman, Pandina, & Faraone, 2003). Several groups have shown that a unique CBCL profile consisting of high scores (2 SDs; aggregate score > 210) on the Attention Problems (AP), Aggressive Behavior (AGG), and Anxious-Depressed (AD) subscales (henceforth referred to as Severe Emotional Dysregulation [CBCL-SED]) has been associated with a wide range of adverse outcomes including a clinical diagnosis of bipolar I (BP-I) disorder in both epidemiological and clinical samples (Achenbach, 1991; Carlson & Kelly, 1998; Geller, Warner, Williams, & Zimerman, 1998; Hazell, Lewin, & Carr, 1999; Mick et al., 2003; Wals et al., 2001). Recent work has also begun to document that even a subsyndromal form of this profile characterized by an intermediate (≥180 but <210) form of the same profile (henceforth referred to as Emotional Dysregulation [CBCL-ED]) was also associated with morbidity and dysfunction (Biederman et al., 2012).
We previously found a linear increase in the prevalence of the CBCL-ED profile in siblings of ADHD probands from lowest in siblings of controls to highest in ADHD probands with the severe profile (CBCL-SED; Biederman et al., 2012). However, because these findings were reported in ADHD families, whether similar patterns can be observed in families of BP-I probands remains unknown.
The main aim of the present work was to further investigate the familiality of emotional dysregulation in a sample of probands with pediatric BP-I disorder. Based on findings in an ADHD sample, we hypothesized that siblings of probands with pediatric BP-I disorder would be at greater risk of emotional dysregulation than controls.
Method
Participants
Detailed study methods have been previously described (Wozniak, Faraone, Martelon, McKillop, & Biederman, 2012). Briefly, children with BP-I disorder 6 to 17 years of age of both sexes were recruited and assessed at the Clinical and Research Program in Pediatric Psychopharmacology at the Massachusetts General Hospital based on the presence of a diagnosis of BP-I disorder in the proband youth by structured diagnostic interview and clinical assessment (Wozniak et al., 2005; Wozniak et al., 2010). Comparators were youth with and without ADHD without BP-I disorder of similar age and sex (Biederman et al., 1992; Biederman et al., 1999; Biederman, Monuteaux, Mick, Spencer, Wilens, Klein, et al., 2006; Biederman, Monuteaux, Mick, Spencer, Wilens, Silva, et al., 2006). We recruited 239 BP-I probands. From families participating in our case-control ADHD studies, we randomly selected 136 non-ADHD control probands without mood disorders (BP-I or major depressive disorder [MDD] full or subthreshold) so that the age and gender distribution was similar to that of the BP-I probands. All studies used the same assessment methodology regardless of the disorder used to classify probands as cases with the exception that children with structured interview diagnosis of BP-I disorder were also assessed buy an expert clinician to confirm the diagnosis (Wozniak et al., 2003). All study procedures were reviewed and approved by the subcommittee for human participants of our institution. All participants’ parents or guardians signed written informed consent forms and children older than 7 years of age signed age-appropriate written assent forms.
Ascertainment Method
Potential BP-I probands were ascertained from our clinical service, referrals from local clinicians, or self-referral in response to advertisements. Participants were administered a phone screen reviewing symptoms of Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) BP-I disorder and, if criteria were met, were scheduled for a face-to-face structured diagnostic interview. In addition to the structured diagnostic interview, an expert clinician (J.W.) met with each BP-I proband and his or her parents for a clinical interview to confirm the diagnosis of BP-I disorder using the Schedule for Affective Disorders and Schizophrenia for School-Age Children–Epidemiological version (KSADS-E) mania module. We have published data on the convergence of these clinical interviews with our structured interview diagnosis on the first 69 cases. We reported 97% agreement between the structured interview and clinical diagnosis in this analysis of 69 children (Wozniak et al., 2003). As previously reported (Biederman et al., 1992; Biederman et al., 1999; Wozniak et al., 2010), controls were ascertained from out-patients referred for routine physical examinations to pediatric medical clinics and from computerized records as not having ADHD and screening for not having ADHD.
Diagnostic Procedures
Psychiatric assessments of participants <18 years of age relied on the KSADS-E (Orvaschel, 1994) and for participants ≥18 years on the Structured Clinical Interview for the DSM (SCID) supplemented with modules from the KSADS-E to capture childhood disorders. Diagnoses of youth were based on independent interviews with mothers and direct interviews with children older than 12 years of age. Data were combined such that endorsement of a diagnosis by either report resulted in a positive diagnosis.
All interviews were conducted by extensively trained and supervised psychometricians with undergraduate degrees in psychology. This training involved several weeks of classroom instruction of interview mechanics, diagnostic criteria, and coding algorithms. They also observed interviews by experienced raters and clinicians and were observed while conducting interviews during the final training period. In addition, all diagnoses were reviewed by a sign-off committee of experienced board-certified child and adolescent psychiatrists or clinical psychologists. The committee members were blind to the participants’ ascertainment status, ascertainment site, and data collected from other family members. We computed kappa coefficients of agreement by having experienced clinicians diagnose participants from audio-taped interviews made by the assessment staff. Based on 500 interviews, the median kappa coefficient between raters and clinicians was 0.99. For individual diagnoses, the kappas were as follows: ADHD (0.88), conduct disorder (1.0), major depression (1.0), mania (0.95), separation anxiety (1.0), agoraphobia (1.0), panic (0.95), substance use disorder (1.0), and tics/Tourette’s (0.89). The median agreement between individual clinicians and the clinical review committee was 0.87 and for individual diagnoses was as follows: ADHD (1.0), CD (1.0), major depression (1.0), bipolar (0.78), separation anxiety (0.89), agoraphobia (0.80), panic (0.77), substance use disorder (1.0), and tics/Tourette’s (0.68).
Children and adolescents were diagnosed with BP-I disorder according to DSM-IV criteria. The DSM-IV requires participants to meet Criterion A for a distinct period of extreme and persistently elevated, expansive or irritable mood lasting at least 1 week, plus Criterion B, manifested by three (four if the mood is irritable only) of seven symptoms during the period of mood disturbance. To ensure that the Criterion B symptoms were concurrent with Criterion A mood disturbance, participants were directed to focus on the worst or most impairing episode of mood disturbance while being assessed for the presence of the confirmatory Criterion B symptoms, that is, the participant was asked to consider the time during which the screen was at its worst for the purpose of determining whether the remaining symptoms were also evident at the same time as the screening item. Also recorded was the onset of first episode, the number of episodes, offset of last episode, and total duration of illness. Any participant meeting criteria for bipolar II (BP-II) or bipolar disorder not otherwise specified (BP-NOS) was not included in this study. To gauge a distinct episode, our interviewers asked for “a distinct period (of at least 1 week) of extreme and persistently elevated, expansive or irritable mood” and further required that the irritability endorsed in this module is “super” and “extreme.”
Child Behavior Checklist
The parent (usually the mother) of each participant completed the 1991 version of the Child Behavior Checklist for ages 4 to 18 years (CBCL/4-18). The CBCL is an affordable pencil and paper test completed by the child’s caregiver, requiring no administration by a physician or rater. The CBCL queries the parent about the child’s behavior in the past 6 months and aggregates these data into behavioral problem T scores (Achenbach, 1991). A computer program calculates the T scores for each scale. Raw scores are converted to gender- and age-standardized scores (T scores having M = 50 and SD = 10). A minimum T score of 50 is assigned to scores that fall at midpoint percentiles of ≤50 on the syndrome scales to permit comparison of standardized scores across scales. As described previously, the CBCL–Severe Dysregulation profile (Biederman et al., 2009) was defined as positive by a score of ≥210 (2 SDs) on the sum of the Attention, Aggression, and Anxious/Depressed CBCL scales. An intermediate or subsyndromal emotional dysregulation profile was defined as positive by a score of ≥180 (≥ 60 on average on each scale) but <210 (average T score of ≥60 and <70; Spencer et al., 2011).
Statistical Analysis
Differences in demographics and clinical characteristics were assessed using an analysis of variance (ANOVA) for continuous outcomes, Pearson’s chi-square for binary outcomes, and the Poisson regression likelihood ratio test for socioeconomic status (SES). A Pearson correlation coefficient tested the association between proband and sibling CBCL-ED scores. Pairwise comparisons of emotional dysregulation scores were made between the five proband groups defined above using linear regression and Tukey’s correction for multiple comparisons; estimates and 95% confidence intervals (CIs) were reported. All tests were two-tailed, and our alpha level was 0.05 for all analyses.
Results
Out of the original samples of BP-I, ADHD, and control probands used in our family study analysis (Wozniak et al., 2012), CBCL data were available on 140 BP-I probands, 83 ADHD probands, and 117 controls. These probands had 106, 68, and 98 siblings, respectively. BP-I probands were further stratified based on the severity of their CBCL-ED scores. Thus, comparisons were made between five proband groups: (a) control participants without ADHD or mood disorders (CONTROLS), (b) ADHD participants without mood disorders (ADHD), (c) BP-I disorder participants without emotional dysregulation (CBCL scores < 180; BP-I), (d) BP-I participants with a positive intermediate CBCL-ED score (≥180 and <210; BP-I + ED), and (e) BP-I participants with severe CBCL-ED scores (≥210; BP-I + SED).
As shown in Table 1, there were no meaningful differences in sociodemographic characteristics between the proband and sibling groups.
Socio-Demographic Characteristics of Probands and Siblings.
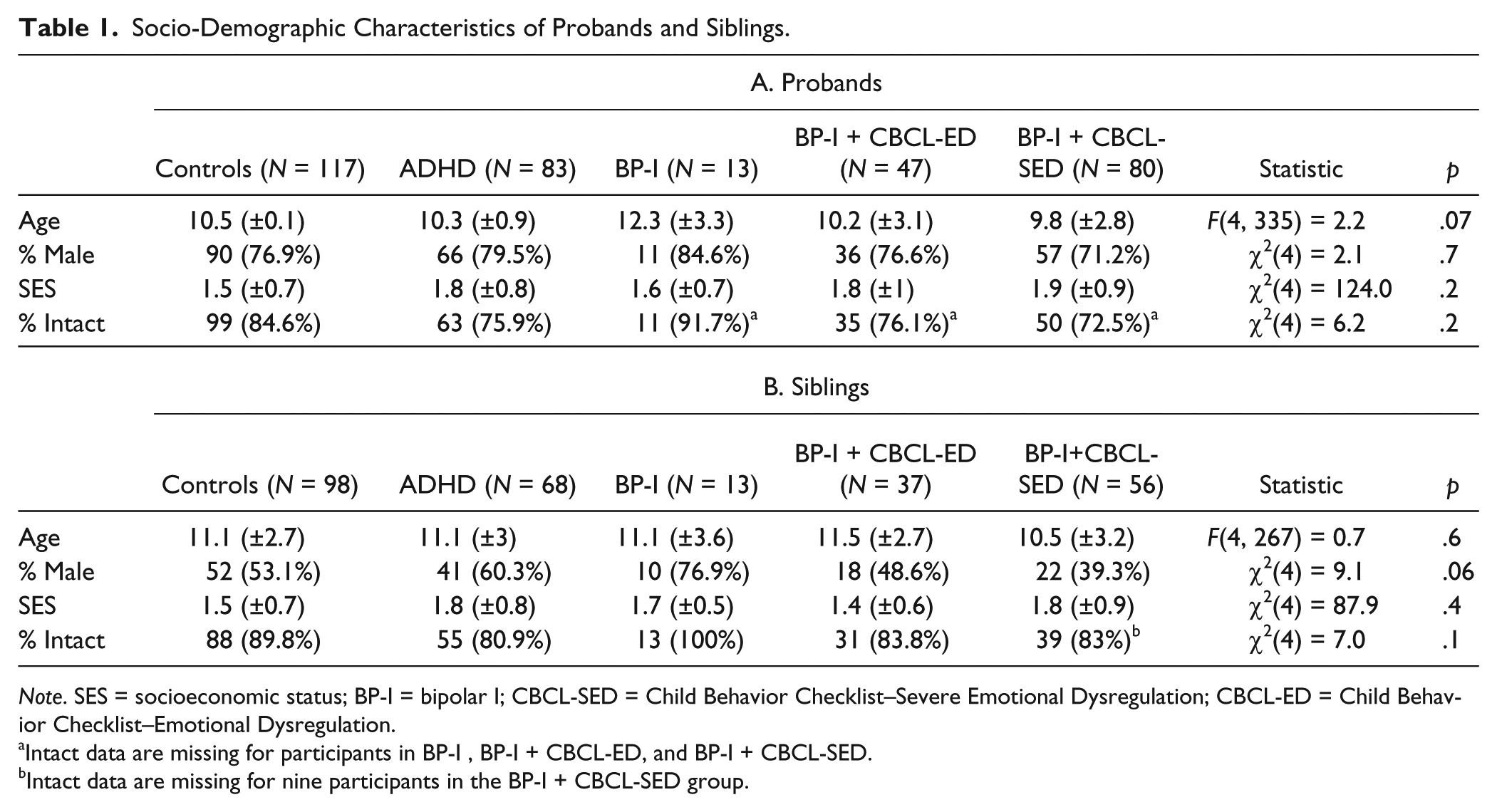
Note. SES = socioeconomic status; BP-I = bipolar I; CBCL-SED = Child Behavior Checklist–Severe Emotional Dysregulation; CBCL-ED = Child Behavior Checklist–Emotional Dysregulation.
Intact data are missing for participants in BP-I, BP-I + CBCL-ED, and BP-I + CBCL-SED.
Intact data are missing for nine participants in the BP-I + CBCL-SED group.
As shown in Figure 1, CBCL-ED scores were significantly correlated between probands and siblings (r = .40, p < .001). Further examination of the distribution of CBCL-ED scores showed an overall significant difference across the groups, χ2 = 44, p < .001, accounted for by the significantly elevated CBCL-ED scores in the siblings of BP-I + CBCL-SED probands (vs. controls, p < .001, vs. ADHD, p < .001, and vs. BP-I + CBCL-ED, p = .005; see Figure 2).
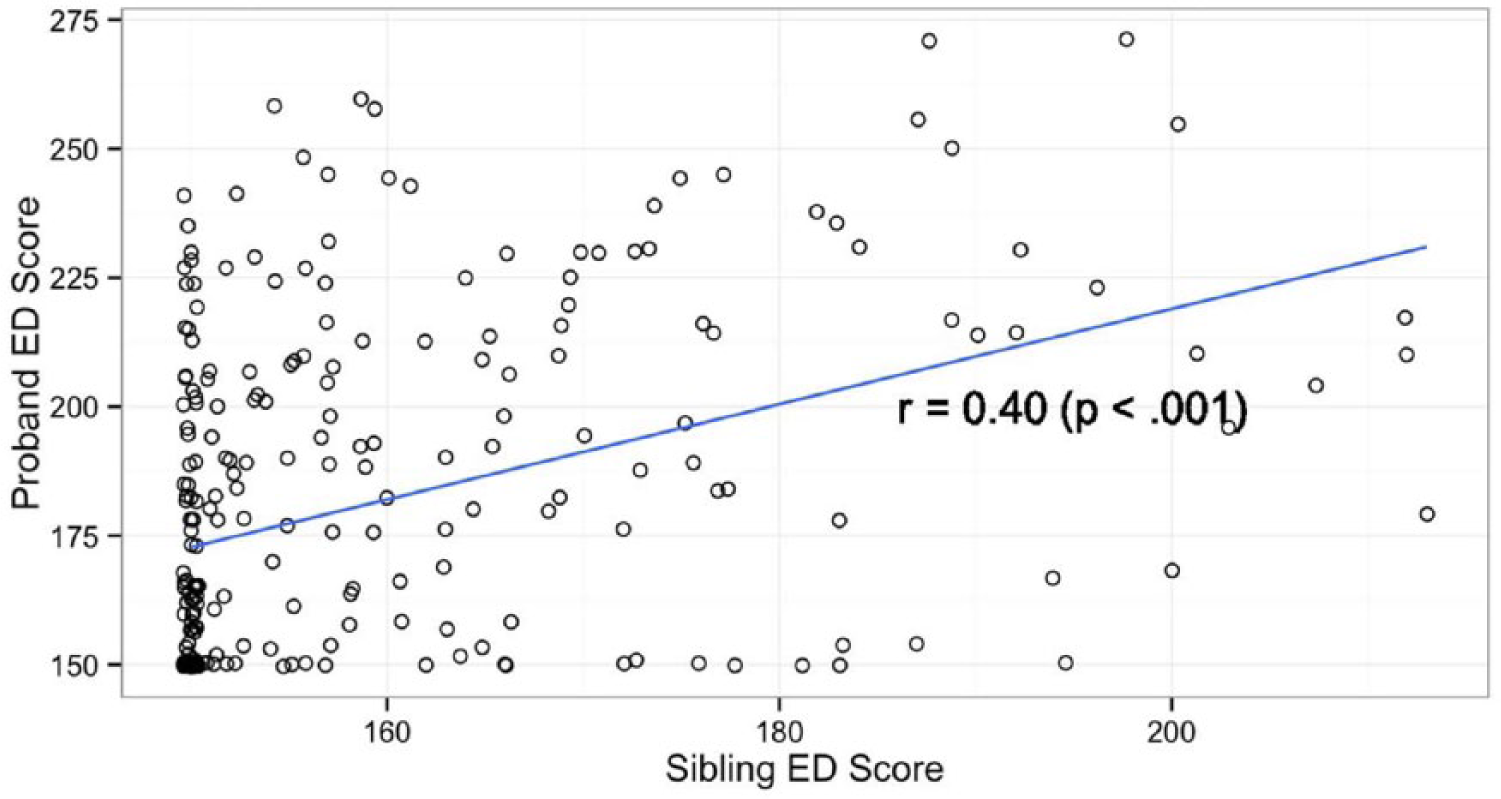
Association between proband and sibling ED scores.
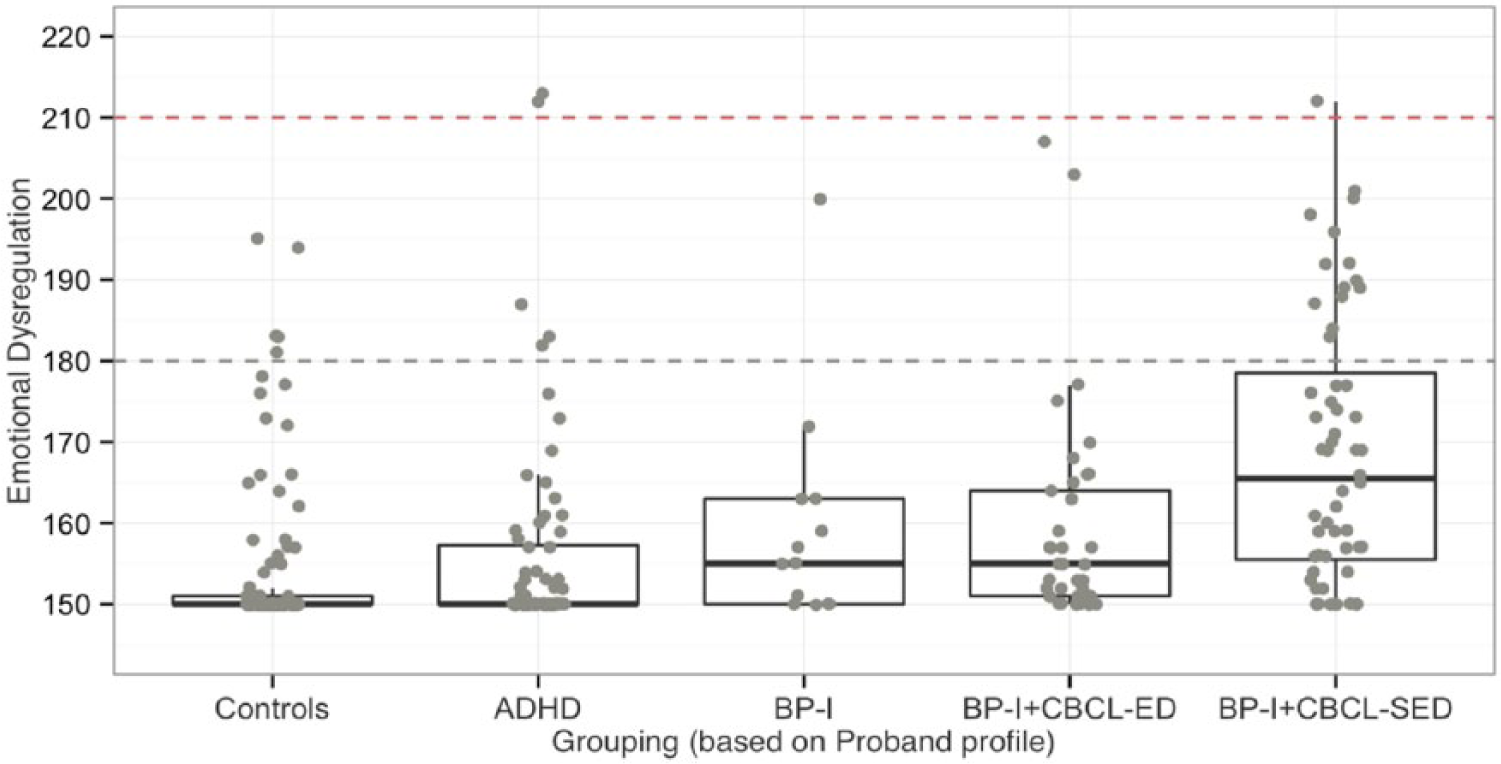
Emotional dysregulation distribution across proband profile groups.
Discussion
Emotional dysregulation as assessed through the CBCL was significantly correlated between probands and siblings such that the higher the CBCL-ED score in the proband, the higher the score in the sibling. Our results also showed that BP-I probands with severe emotional dysregulation had the highest representation of siblings with emotional dysregulation. These results extend previously reported findings suggesting that emotional dysregulation has familial underpinnings in families of ADHD youth to pediatric BP-I families.
Our finding showing linear increases in the prevalence of the CBCL-ED profile in siblings by severity of the CBCL profile in probands is consistent with findings previously reported in our ADHD study that also found a significantly higher rate of a positive CBCL-SED profile in the siblings of ADHD probands with the same profile (Biederman et al., 2012).
Our findings are also consistent with previous results showing that a positive CBCL-ED profile consistently identifies children with more severe correlates. For example, children with BP-I disorder with a positive CBCL-ED profile had an earlier age of onset of BP-I disorder, higher rates of psychiatric hospitalization, and higher rates of major depression, oppositional defiant disorder, social anxiety, panic disorder, and generalized anxiety disorder when compared with those without it (Biederman et al., 2013). Taken together, these results indicate that the CBCL-ED profile identifies children with severe and dysfunctional correlates and outcomes.
Our findings need to be viewed in light of some methodological limitations. Because the sample was referred and largely Caucasian, findings may not generalize to community samples and other ethnic groups. Despite these limitations, our results showing significant correlations between CBCL-ED scores in probands and siblings suggest that emotional dysregulation may have familial underpinnings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Joseph Biederman is currently receiving research support from the following sources: the Department of Defense, American Academy of Child and Adolescent Psychiatry, Alcobra, Forest Research Institute, Ironshore, Lundbeck, Magceutics Inc., Merck, PamLab, Pfizer, Shire, SPRITES, Sunovion, VAYA Pharma/Enzymotec, and National Institutes of Health (NIH). In 2014, he received honoraria from the Massachusetts General Hospital (MGH) Psychiatry Academy for tuition-funded Continuing Medical Education courses. He has a U.S. patent application pending (Provisional Number 61/233,686) through MGH corporate licensing, on a method to prevent stimulant abuse. He received departmental royalties from a copyrighted rating scale used for ADHD diagnoses, paid by Ingenix, Prophase, Shire, Bracket Global, Sunovion, and Theravance; these royalties were paid to the Department of Psychiatry at MGH. In the past year, Dr. Faraone received income, travel expenses, and/or research support from and/or has been on an advisory board for Pfizer, Ironshore, Shire, Akili Interactive Labs, CogCubed, Alcobra, VAYA Pharma, Neurovance, Impax, and NeuroLifeSciences, and received research support from the NIH. His institution is seeking a patent for the use of sodium–hydrogen exchange inhibitors in the treatment of ADHD. In previous years, he received consulting fees or was on advisory boards or participated in continuing medical education programs sponsored by Shire, Alcobra, Otsuka, McNeil, Janssen, Novartis, Pfizer, and Eli Lilly. He receives royalties from books published by Guilford Press (Straight Talk About Your Child’s Mental Health) and Oxford University Press (Schizophrenia: The Facts). Dr. Thomas Spencer has received research support from, has been a speaker for or on a speaker bureau, or has been an advisor of or on an advisory board of the following sources: Alcobra, Cephalon, Eli Lilly, GlaxoSmithKline, Heptares, Impax, Ironshore, Janssen, Lundbeck, McNeil, Novartis, Pfizer, Shire, Sunovion, VAYA Pharma, the Food and Drug Administration, the National Institute of Mental Health, and the Department of Defense. He receives research support from Royalties and Licensing fees on copyrighted ADHD scales through MGH Corporate Sponsored Research and Licensing. He has a U.S. patent application pending (Provisional Number 61/233,686), through MGH corporate licensing, on a method to prevent stimulant abuse. In 2013 to 2015, Janet Wozniak has received research support from Merck/Schering-Plough and income from MGH Psychiatry Academy. In the past, she has received research support, consultation fees, or speaker’s fees from Eli Lilly, Janssen, Johnson and Johnson, McNeil, Pfizer, and Shire. She is the author of the book Is Your Child Bipolar published May 2008 by Bantam Books. In 2013 to 2015, her spouse received income from Associated Professional Sleep Societies, Cambridge University Press, Gerson Lerman Group, MGH Psychiatry Academy, Summer Street Partners, UCB, and Cantor Colburn. In the past, he has received research support, consultation fees, royalties or speaker’s fees from Axon Labs, Boehringer-Ingelheim, Cambridge University Press, Covance, Cephalon, Eli Lilly, GlaxoSmithKline, Impax, Jazz Pharmaceuticals, King, Luitpold, Novartis, Neurogen, Novadel Pharma, Pfizer, Sanofi-Aventis, Sepracor, Takeda, UCB (Schwarz) Pharma, UptoDate, Wyeth, Xenoport, and Zeo. James Chan and K. Yvonne Woodworth report no financial disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from National Institutes of Health to Dr. Wozniak (K08MH001503 and R01MH066237) and to Dr. Biederman (R01MH050657 and R01HD036317). This work was also supported by a grant from the Heinz C. Prechter Bipolar Research Fund, and had the support of members of the Massachusetts General Hospital Pediatric Psychopharmacology Council and the Susan G. Berk Endowed Fund for Juvenile Bipolar Disorder.