
Abstract
ADHD is a complex and heterogeneous neurobiological and behavioral disorder that is mainly characterized by developmentally inappropriate levels of inattention, hyperactivity, and impulsivity. These two last subdomains are grouped into a single subdomain in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994).
ADHD Diagnosis
The complexity of ADHD is agreed upon by all major researchers in the field. This becomes even more of an issue when diagnostic criteria developed primarily on clinical-referred children are used to diagnose adults. Most adults who suffer from ADHD report some of the following behaviors: difficulties in self-control; frequent mood changes; hypersensitivity; low tolerance to the daily-life stress; low tolerance to frustration; unstable attention; delaying in some tasks but not in others; forgetfulness, impulsivity, anxiety, and depression; difficulty in achieving a suitable level of activation; disorganization; a tendency to have driving accidents; difficulties in social relationships, marriage, and employment; difficulties in achieving long-term goals; and a limited ability to postpone gratification. However, not all of these symptoms are listed as criteria for ADHD in the DSM-IV.
Four aspects are relevant in the DSM-IV criteria of ADHD. First, it is a comparative diagnosis based on the degree to which certain types of behaviors are exhibited and found to be detrimental to normal life. Second, the impairment must be documented in at least two life domains, such as home, work, school, or social settings. Third, the diagnosis of this disorder is dependent on the developmental level of the individual and the contextual situation. Although all children possess some of the behavior characteristics of ADHD, it is the degree to which they are developmentally inappropriate that determines whether or not they are indicative of the disorder. This relates directly to diagnosis in adulthood, where the history of the individual (age of onset and persistency of the disorder) is an important diagnostic marker. The contextual situation of behavioral symptoms is important because most individuals who suffer from ADHD do not display attention or hyperactivity problems all the time. Fourth, ADHD is in some ways a diagnosis of exclusion. The diagnosis is applied when no other condition better explains the individual’s characteristics. As such, there are a number of conditions with similar characteristics that must be ruled out in diagnosis to prevent either over- or underdiagnosis. With regard to this last point, different studies emphasize that in the adult population ADHD coexists with other psychiatric disorders in 50% of the cases (Biederman, Newcorn, & Sprich, 1991). The most common comorbid pathologies are oppositional/defiant disorder, anxiety disorders, depression, vocal movements, specific learning disorders, and aggressive behavior (Biederman et al., 1995; Friedrichs, Igl, Larsson, & Larsson, 2012; Munir, Biederman, & Knee, 1987; Reimherr, Marchant, Olsen, Wender, & Robison, 2013).
Whereas many studies of ADHD have involved children, very few have examined the adult outcome of this disorder (Ramos-Quiroga, Nasillo, Fernández-Aranda, & Casas, 2014). According to Asherson et al. (2012), many adults with ADHD may underestimate the impact of ADHD symptoms and have learned to compensate for impairments by choosing lifestyles that help compensate for symptoms, which makes it difficult to diagnose the disorder and to calculate its prevalence. Nonetheless, epidemiological data estimate the prevalence of adult ADHD to be up to 5% (Faraone & Biederman, 2005; Fayyad et al., 2007; Kessler et al., 2006). Some studies carried out with college students from the United States have also shown that approximately 2% to 8% of the population report clinically significant levels of ADHD symptoms (Weyandt & DuPaul, 2006). In fact, although the disorder is more prevalent in childhood than in other developmental periods of the individual’s life, it persists into adolescence in 50% to 80% of the cases clinically diagnosed in childhood, and into adulthood in 30% to 50% of these cases (Barkley, 1990; Biederman, 2005; Klein & Mannuzza, 1991; Weiss & Hechtman, 1993). Goldstein (1997) has even stated that 65% of children with ADHD show symptoms of the disorder into adulthood.
Gender Differences
Some studies addressed gender differences and found a higher prevalence among males (Bauermeister et al., 1995; Kessler, 2004) that is quite stable across national samples (Fayyad et al., 2007); however, other studies did not report a gender effect (Biederman et al., 2005; DuPaul et al., 2001; Murphy & Barkley, 1996) and some even found a slightly higher prevalence among adult females (Kooij et al., 2005; Serra-Pinheiro, Mattos, & Regalla, 2008). A meta-analysis by Polanczyk, de Lima, Horta, Biederman, and Rohde (2007), controlling for various method factors like informant source, found a much higher prevalence among males. The same was found in a meta-analysis of prevalence of ADHD in children and early adolescents (Gershon, 2002). A review of the literature by Nussbaum (2012) suggests that compared with males with ADHD, females with ADHD are more prone to having difficulties with inattentive symptoms than with hyperactive and impulsive symptoms, which hinders detection and early intervention among females.
Cross-Cultural Differences
The relation between ADHD and culture is not well established. Opinions differ as to whether ADHD is a universal disorder. On one hand, similar characteristics of ADHD and similar prevalence rates have been found in different countries and cultures (see Faraone, Sergeant, Gillberg, & Biederman, 2003; Fayyad et al., 2007). On the other hand, significant cross-cultural differences have appeared in various studies (see Barkley, 2003). Different reasons for cross-cultural differences in prevalence can be envisaged. First and foremost, there may be real differences in ADHD prevalence. However, there may be other reasons. For example, differences may result from differential tolerance of hyperactive behavior across cultures. Also, differences in prevalence might be attributed to methodological differences in criteria or methods used to define or assess this disorder; for example, the meta-analysis of Polanczyk et al. (2007) found that the use of informants (parents or teachers) led to higher reported prevalence rates than the use of diagnostic tests. This finding may also contribute to the higher prevalence rates among children than among adults, as other informants are less likely to be involved in their assessment. Polanczyk et al. found that after correcting for all methodological artifacts, there were only differences between Europe and North America on one hand, and Africa and the Middle East on the other hand. However, while in Europe and, especially, in North America a lot of studies have been conducted in this research area, the number of studies with regard to African and the Middle Eastern cultural groups is still scarce and there is a large variability in the results obtained in them, which underlines the need for further studies to confirm these conclusions.
If, as has been suggested, ADHD often does not disappear after childhood and continues in adolescence and adulthood, cross-national differences in prevalence rates in adulthood may be a continuation of cross-cultural differences in prevalence in childhood. Some studies have addressed the background of cross-cultural differences in childhood prevalence. Gomez, Burns, and Walsh (2008) examined behaviors associated with oppositional defiant disorder among children of Australian, Malaysian Malay, and Malaysian Chinese parents. An item about being touchy showed a higher frequency among Malaysian parents. The authors interpret this difference as a consequence of a lower tolerance of deviant behavior by Malaysian parents. These findings suggest that cultures may well differ in their thresholds of deviance. Livingston’s (1999) results also suggest that tolerance for certain behaviors varies between cultural groups and that, in the specific case of ADHD, the attitudes of parents and relatives, clinicians, and even society at large can influence the diagnosis and medication of ADHD.
A relationship has been found between parental style and ADHD. Specifically, parents of ADHD children have been shown to demonstrate higher levels of authoritarian parenting style (Alizadeh & Andries, 2002; Alizadeh, Applequist, & Coolidge, 2007; Lange et al., 2005) and lower levels of authoritative parenting (Alizadeh, 2005). There is evidence that authoritative parenting is more widely used by European American families, where there is a high level of nurturance but clear expectations, than it is in Hispanic and African American families (Halgunseth, Cushinberry, & Bordere, 2003).
Aims and Hypotheses
The present study aims to contribute to our understanding of the continuity of ADHD in adulthood, and we believe it adds to the literature in two ways. First, we studied ADHD among young adults, whereas most studies deal with children. Second, we examined ADHD in four cultural groups (Spaniards, African American, Hispanic Americans, and European Americans), whereas most studies involve a single cultural group. In addition, we examined gender differences.
Our first hypothesis involves the similarity of ADHD symptoms across the studied samples. We expect the basic structure of ADHD to be invariant across cultural groups. The second hypothesis focuses on cross-cultural differences in ADHD scores. We expect there to be differences in the level of ADHD symptoms across cultural groups, with lower scores being found in European Americans, the group with a more prevalent authoritative parenting style, than in other cultural groups. Finally, our third hypothesis is related to gender. Here, we expect a higher prevalence rate of ADHD in males, regardless of cultural group.
Method
Participants
Participants for this study were 902 primarily young adults (nonreferred) from various high schools and universities in the United States and Spain. They came from high school (23%), junior college (24%), and university (53%). Three ethnic groups in the United States were involved: African American (n = 210), Hispanic American (n = 148), and European American (n = 306); in Spain, all participants belonged to the dominant ethnic group (White; n = 238). The ethnicity of the participants’ parents was used to determine ethnic origin; thus, if both parents of the participants with ADHD had the same ethnic origin, the participant was considered as belonging to this group. The mean age of participants was 20.39 years (SD = 4.90). The mean (SD) ages per group were 21.21 (4.51), 21.42 (3.34), 17.27 (4.11), and 20.55 (5.77) for the Spanish, African American, Hispanic American, and European American groups, respectively. The differences were statistically significant, F(3, 863) = 26.56, p < .001. Pairwise post hoc comparisons using Tukey tests showed that the Hispanic group was significantly younger than the other groups, possibly because Hispanic students are fewer in number at university in comparison with the other groups. In the overall sample, 61% were women; the percentage of women per group was 80%, 76%, 51%, and 56% for the Spanish, African American, Hispanic American, and European American groups, respectively. Therefore, the gender composition of the cultural groups was also significantly different, χ2(3, N = 902) = 43.78, p < .001.
Instruments
The ADHD construct was measured by the Inattention and the Hyperactivity/Impulsivity scales, form A, of Caterino’s Adult ADHD Scale (CAADS; see Caterino, Gómez-Benito, Balluerka, Amador-Campos, & Stock, 2009, for a detailed explanation of the development process of the scale; Gómez-Benito & Balluerka, 2000, have described a Spanish version). Each of the two scales (Inattention and Hyperactivity/Impulsivity) is composed of nine items that fit the behavioral criteria of the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000): 314.00 for diagnostic category of Inattention and 314.01 for Hyperactivity/Impulsivity. Both English and Spanish versions showed good psychometric properties (Caterino et al., 2009; Gómez-Benito & Balluerka, 2000).
Each item describes a symptom; severity is evaluated on a 3-point scale: 0, if it hardly describes the behavior of the participant; 1, if it describes this behavior to a certain degree; and 2, if it describes this behavior to a large degree. Moreover, each item has to be answered with regard to three areas: “at home,” “at work or at school,” and “in other areas of society”; the sum of the scores in the three areas constitutes the score for that item (ranging from 0 to 6).
Procedure
The evaluation procedure was approved by the heads of the educational centers that collaborated in the study. All the participants received oral and written information about the aims of the study. Once the research team had explained the aims of the research, the participants were invited to participate voluntarily and anonymously. It was made clear to them that all data would remain confidential, and that participation would in no way affect their academic results. After obtaining the written consent of the participants, copies of the scale were distributed in classrooms by a member of the research team or by a classroom instructor. Participants were allowed to complete their form at their own pace and were informed that they had the freedom to leave the study if they wanted to. Refusal rates were below 5%.
Data Analysis
The data analysis comprised two parts. The first part examined the cross-cultural adequacy of the instrument (structural equivalence) and the comparability of the scores (score comparability). The examination of structural equivalence started from an exploratory factor analysis that was conducted in each group. An instrument is taken to measure the same psychological construct if factor loadings show a high correspondence across cultures. The correspondence of factors, obtained in different cultures, was evaluated by Tucker’s (1951) phi coefficient. We compared the correspondence in a pairwise manner (given that four cultural groups were involved, six comparisons could be computed). In each comparison, a cultural group was chosen as the target and the factor loadings of the other cultural group were rotated so as to maximize the similarity with the target. A value of Tucker’s phi higher than .90 is considered as evidence for factor similarity (Van de Vijver & Leung, 1997).
Structural equivalence is not in itself sufficient for making numerical score comparisons across cultures. Score comparability was thus examined by testing the presence of DIF (Differential Item Functioning, also labeled item bias), using linear regression. For each of the two scales, a set of multiple regression analyses was conducted. Three dummy variables were created to represent the four cultural groups. The total score for each scale (i.e., the sum of the item scores of the scale) was centered on the sample mean to avoid multicollinearity. In each equation, the item score was the dependent variable, and the dummy variables, the centered total score, and the interactions between this score and dummies were the independent variables. Stepwise regression was used. The first step estimated the effect of total score, the second step added the effect of the three dummy variables, and the last added the effect of the three interaction terms. The change in R2 between the three regression models assesses the relative importance of adding the block variables. The increment in R2 between the first two steps assesses the main effect of the group variable and, if sufficiently large, suggests uniform DIF (Mellenbergh, 1982), which indicates that the affected item is consistently more endorsed across all levels of the total score in at least one cultural group. Moreover, the R2 increment from the second to the third step assesses the effect of the interactions between group and score variables and, if sufficiently large, indicates nonuniform DIF, which means that group score differences depend on score level. In line with common practice to examine both significance and effect size of bias effects, we computed the size of the change in the determination coefficient in hierarchical regression, f2 (Cohen, 1988); Values of .02, .15, and .35 are considered small, medium, and large effects, respectively.
As for the second part of the analysis, the aim was to investigate cultural differences between the four groups regarding the two dimensions of ADHD, as well as the effect of gender on them. A MANCOVA was carried out with Inattention and Hyperactivity/Impulsivity as dependent variables (factor scores), with cultural group (four levels) and gender (two levels) as factors, and with age as a covariate to control for confounding sample differences.
Results
The results are divided into two parts. The first part deals with the analysis of the psychometric properties and focuses on the analysis of internal consistencies, the similarity of the psychological meaning of the construct among the different groups involved, and the lack of bias of the items measuring the construct between the mentioned groups. The second part aims to examine the differences among cultural and gender groups in the two dimensions of ADHD.
Psychometric Properties
In all the groups, a two-factor solution was obtained, distinguishing between the Inattention and Hyperactivity/Impulsivity indicators. The values of internal consistency of the two factors were .79 and .76, respectively, for the whole sample. The values of Cronbach’s alpha ranged between .73 and .81 for Inattention, and between .70 and .81 for Hyperactivity/Impulsivity across the cultural groups. In neither analysis was the value of alpha increased by deleting any item, indicating the relevance of the indicators in the measure of the respective constructs.
Table 1 shows the loadings of the two factors for their corresponding items and with respect to the four groups studied. The values of the Tucker’s phi coefficients for the six possible comparisons between the groups ranged between .98 and .99 for Inattention, and between .96 and .99 for Hyperactivity/Impulsivity. All values were much higher than .90, suggesting equivalence of factor structures. It was concluded that the two-factor structure for the ADHD items of the CAADS replicated well across all cultural groups and, therefore, the first hypothesis was confirmed.
Item Loadings of Each Group for Inattention and Hyperactivity/Impulsivity.

Table 2 shows the results of the DIF analyses that were conducted per scale, based on the factors of the previous analysis. The analysis of the Inattention scale showed that five out of nine items were significantly biased (p < .05); more specifically, all these items showed a uniform bias (significant effect of culture), two of these also showed a significant nonuniform bias (significance of interaction term). We also examined the effect sizes; the f2 associated with cultural group ranged from .001 to .035 and the values for the interaction ranged from .001 to .009; by common standards these are negligible to small effect sizes. A similar pattern was obtained for Hyperactivity/Impulsivity; six out of nine items reached significance (p < .05) for the main effect and one item for the interaction. The values of f2 ranged from .004 to .040 for the main effect and from .001 to .012 for the interaction. Again, the effect sizes were negligible to small. We concluded that no items showed sufficiently large bias to be discarded.
R2, Significance of Change in R2, and Effect Size for Inattention and Hyperactivity/Impulsivity Items.
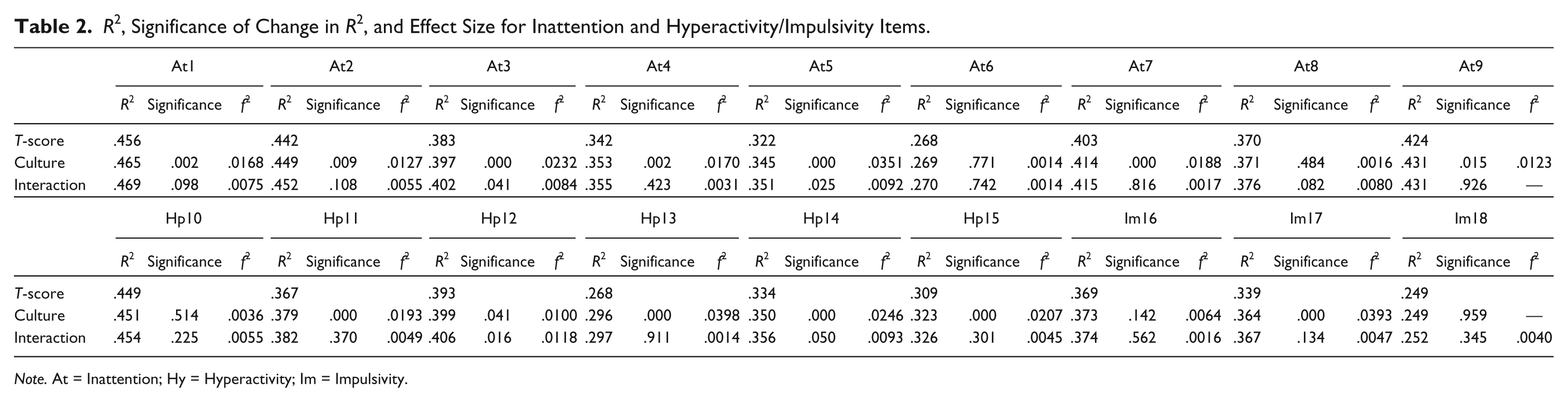
Note. At = Inattention; Hy = Hyperactivity; Im = Impulsivity.
Cultural and Gender Differences in ADHD
The multivariate effects in the MANCOVA showed statistically significant results for cultural group and age—Wilks’s Lambda for cultural group = .958, F(6, 1622) = 5.830, p < .001, and Wilks’s Lambda for age = .971, F(2, 811) = 12.004, p < .001. However, the corresponding effect sizes were small (η2 = .021 for cultural group and .029 for age). The univariate analyses revealed that the multivariate significant differences were primarily due to the Inattention scale, which showed a significant group difference, F(3, 812) = 9.650, p < .001. The effect of age (covariate) on Inattention was also significant, F(1, 812) = 23.943, p < .001. Both effect sizes were small (cultural group: η2 = .034; age: η2 = .029). With respect to the Hyperactivity/Impulsivity scale, a borderline significance was found for cultural group, F(3, 812) = 2.393, p = .067, with a negligible η2 = .009; for age, although the effect was statistically significant, F(1, 812) = 7.012, p = .008, the size was also negligible (η2 = .009). No significant effect was found for gender, Wilks’s Lambda = .998, F(2, 811) = 0.864, p = .422; the interaction between gender and culture was just significant, Wilks’s Lambda = .985, F(6, 1622) = 2.106, p = .050. Effect sizes associated with such effects were very small (gender: η2 = .002; interaction: η2 = .008). The univariate interaction was significant for Inattention, F(3, 812) = 2.819, p < .050, η2 = .010, and bordered on significance for Hyperactivity, F(3, 812) = 2.258, p = .080, η2 = .008. The interaction was mainly due to the Hispanic group, which was the only one in which females scored higher than males; although not significant, the same pattern was found for Hyperactivity. This finding may also explain why no main effect was found for gender.
The results of the post hoc analyses for cultural differences are shown in Tables 3 and 4. Means and standard deviations per group are given in Table 3, which shows at a glance that for both factors, the highest scores are obtained by the Hispanic American group and the lowest by European Americans.
Means (and Standard Deviations) of the Groups for Inattention and Hyperactivity/Impulsivity.

Mean Differences, (Significance), and Effect Size for the Pairwise Mean Comparison Between the Groups for Inattention and Hyperactivity/Impulsivity.
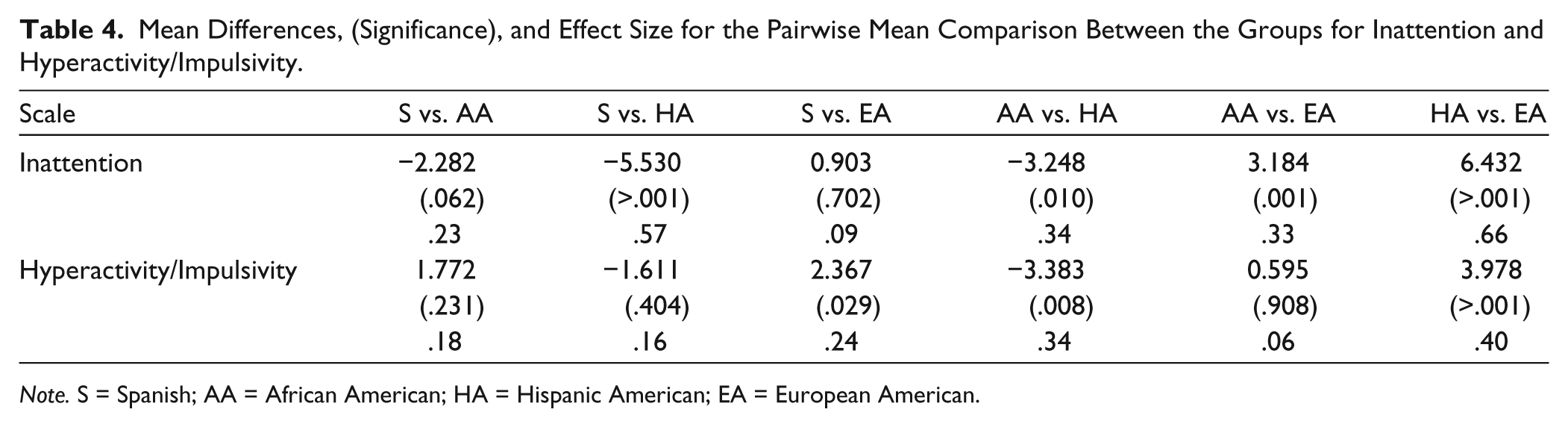
Note. S = Spanish; AA = African American; HA = Hispanic American; EA = European American.
Table 4 shows the mean differences between the six possible comparisons, as well as the corresponding significance and effect size (estimated by means of Hedges’s g) of these differences. Four of the six comparisons are significant in Inattention, as the Hispanic American group achieved significantly higher scores than did all other groups, with effect sizes of moderate to high magnitude. For its part, the European American group not only achieved significantly lower scores than did the Hispanic American group but also scored lower than the Spanish group, although in this case with a low to moderate effect. With respect to the Hyperactivity/Impulsivity scale, three of the six comparisons are significant, all with effect sizes of low to moderate magnitude. The Hispanic American group scored significantly higher than the other two American groups, while scores in the European American group were lower than those in both the Hispanic American and Spanish groups. In sum, the lowest score for both the Inattention and Hyperactivity/Impulsivity subdomains of ADHD was found in European Americans. This result confirms our second hypothesis.
The relationship between age and the two dimensions of ADHD is depicted in Figure 1. A decline of symptoms was observed with advancing age, slightly more pronounced for Inattention. The correlation between age and each of the dimensions of ADHD is −.20 for Inattention and −.12 for Hyperactivity/Impulsivity; both are statistically significant (p < .05) but of small effect size (Cohen, 1988).
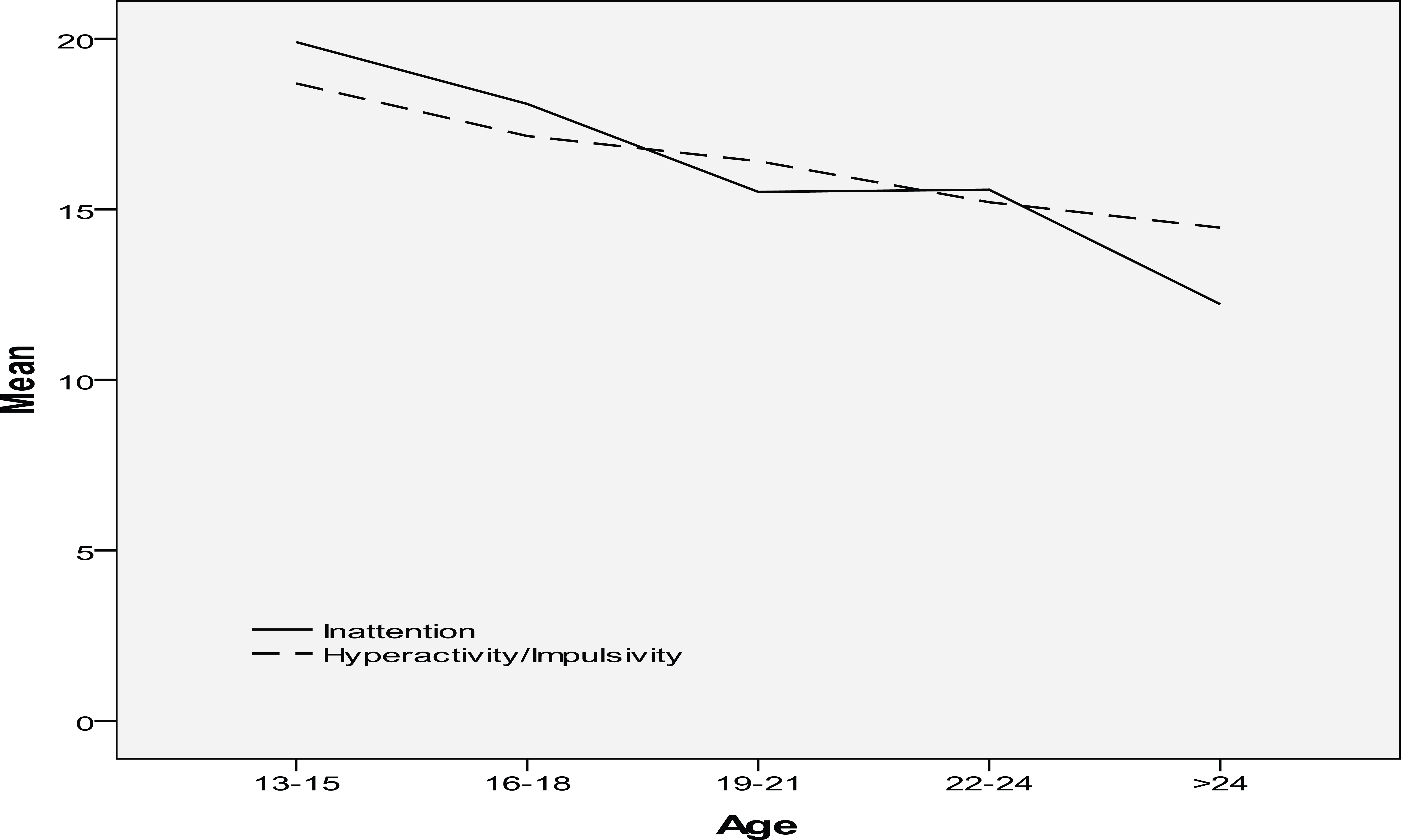
Means of Inattention and Hyperactivity/Impulsivity dimensions as a function of age.
Discussion
ADHD is an important focus for both researchers and practitioners. This is mainly due to the prevalence of the disorder, the high persistence throughout life, the social relevance of the dysfunction, the increased medication rates, and the unfinished debate about the cultural and/or neurobiological background of ADHD. The present study addressed the question of to what extent ADHD symptoms, as measured by the Inattention and the Hyperactivity/Impulsivity scales of the CAADS (Caterino et al., 2009), vary across cultures (Spaniards, African American, Hispanic Americans, and European Americans) and gender. The literature is inconclusive on both issues.
Equivalence of the psychological meaning of the construct among the groups is required before any cross-cultural comparison can be made. Therefore, the study examined the equivalence of the used measure to assess ADHD symptoms at the structural and item levels. The main conclusion of this first part of our analysis is that the data supported the structural equivalence of the two dimensions of ADHD across the four cultural groups involved (in line with our first hypothesis). The bidimensional factor construct we observed is well established in the literature, both among children and adults, and both in self-ratings and other ratings (Bauermeister, Canino, Polanczyk, & Rohde, 2010; Rohde et al., 2005). The subsequent confirmation of equivalence at the item level represented additional support for the validity of the group comparisons. Item bias of ADHD instruments has never been addressed; therefore, our study provides relevant information about the validity of cross-cultural comparisons involving CAADS, which has been taken for granted in previous studies.
Regarding the effect of culture, the results showed a lower level of ADHD in the European Americans than in the rest of the cultural groups, which confirms our second hypothesis. There are several potential explanations for this difference. Cross-cultural differences in authoritative parenting style could be relevant. This parenting style is more common among European American parents and is associated with more tolerance of deviant child behavior than is authoritarian parenting, together with more warmth and less power assertion by parents (Hinshaw, Zupan, Simmel, Nigg, & Melnick, 1997; Hurt, Hoza, & Pelham, 2007; Mikami, Jack, Emeh, & Stephens, 2010). We can therefore conclude that the construct is shared among the studied groups and that there are small, yet consistent cross-cultural differences in mean scores. We concur with Rohde et al. (2005), who stated that taking into account cultural aspects to better understand a disorder is not the same as defining it as a culture-specific construct. The equivalence of the instrument suggests that, at least across our four samples, ADHD has a well-established core that is identical across the samples. This is concordant with our view that ADHD is a complex disorder whose clinical manifestation involves the coincidence of several risk factors, some of them of biological and genetic nature, whereas others are environmental and psychosocial; among the latter, parenting styles and the relative degree of tolerance for behavior may be relevant. These findings point to the importance of considering cultural factors for professionals working with ADHD in schools, families, or other social contexts.
We also addressed gender differences. Contrary to our hypothesis, we did not find a gender effect. This finding has been observed before (though not consistently) and might be due, according to Biederman et al. (2005), to the sampling of nonreferred samples, because the majority of the studies that observe more ADHD in males are comprised of clinical samples. It is also possible that our findings are mainly a consequence of the unexpected pattern of gender differences in the Hispanic group in which females, if anything, tended to score higher. This has also been found by Rohde et al. (1999) and by Serra-Pinheiro et al. (2008). Furthermore, the meta-analysis of Simon, Czobor, Bálint, Mészáros, and Bitter (2009) reported that gender differences are less pronounced in adults than in children. All these results highlight the need for future studies on the course of the disorder between the genders and the impact on referral rates at different development stages (Asherson et al., 2012).
Finally, our findings provided tentative evidence for symptom decline over time of the two dimensions of ADHD, which is in line with the literature (Barkley, 1998; Biederman, Mick, & Faraone, 2000; Biederman et al., 2010; Faraone, 2000; Polanczyk et al., 2007). The explanation of this phenomenon is not clear. It could be related to the transition from educational to occupational environments (with their usually lower requirements vis-à-vis attentional and inactivity demands), so that the symptoms of the disorder are less evident. Another explanation might be that in adults, there is a greater social acceptance and tolerance of ADHD-type behaviors than in children. The choice of one’s work or recreational activities that compensate for the deficits associated with the disorder may also be relevant. Finally, the remission could be due to the fact that the norms of DSM-IV are made for children and have not been properly adapted for adults; Barkley (1997) and Faraone (2000) have argued that symptom decline in ADHD may reflect the developmental insensitivity of the DSM-IV rather than the natural history of ADHD.
In sum, the results support that ADHD, as measured by the CAADS, is comparable among the four cultural groups involved in this study and has a similar psychological meaning for all of them. However, there are cross-cultural differences in the two dimensions of ADHD. Specifically, European Americans show lower levels of the disorder than do the rest of the cultural groups, which might be related with their authoritative parenting style. We concur with Faraone et al. (2003) that ADHD is not “an American condition.” Our study suggests that ADHD cannot be seen out of its context of occurrence, although future studies would be needed to establish which cultural factors have a bearing on its observed prevalence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Spain’s Ministry of Economy and Competitiveness (Grant PSIC2012-32275), and by the Agency for the Management of University and Research Grants of the Government of Catalonia (Grant 2014SGR1139).