
Abstract
Despite demonstrated impairments in social acceptance and behavioral conduct, children with ADHD often self-report their competence in these areas as similar to that of typically developing (TD) children (Hoza et al., 2004), a phenomenon known as Positive Illusory Bias (PIB; Owens, Goldfine, Evangelista, Hoza, & Kaiser, 2007). Although considerable research documents the existence of PIB in ADHD populations, to our knowledge, all studies have relied upon explicit self-report questionnaire measures to assess children’s self-perceptions of competence. The positive discrepancy between children’s self-perceptions and external indices (such as ratings reported by parents and teachers) of their actual social and behavioral competence is typically considered to measure PIB (Owens et al., 2007).
However, a growing literature suggests that individuals use multiple systems to process self-relevant information (Strack & Deutsch, 2014). Explicit self-perceptions reflect relatively deliberate, conscious reasoning about the self, whereas implicit associations reflect automatic activations of self-relevant evaluations that can exist outside of conscious control or awareness (Schnabel & Asendorpf, 2010). A presumption is that respondents have more conscious control over self-reports when using explicit measures than implicit measures (Greenwald, McGhee, & Schwartz, 1998). As such, implicit associations may be useful to assess children’s self-perceptions of their competence that they are less able (because they lack conscious introspective access) or less willing (because they have social desirability concerns) to report explicitly (Nosek, Greenwald, & Banaji, 2007). Assessment with implicit measures may be especially valuable when self-perceptions of competence are negative as opposed to positive, making them difficult to explicitly acknowledge.
To our knowledge, no studies have examined implicit self-perceptions of competence (or whether implicit self-perceptions are inflated relative to external indices of competence) in children with ADHD. However, children’s implicitly assessed self-esteem can diverge from their explicit reports, and consideration of both explicit and implicit self-esteem maximally predicts key interpersonal behaviors such as aggression (Sandstrom, 2011), pointing to the unique prediction offered by implicit measures. In the only study that has examined implicit associations (of any type) in an ADHD sample, Kurman, Rothschild-Yakar, Angel, and Katz (2015) found that among children with ADHD, authoritarian parenting was associated with lower implicitly, but not explicitly, measured self-esteem. Collectively, these studies suggest that implicit and explicit self-perceptions can be distinct or serve different functions, and underscore the value and feasibility of measuring implicit associations in ADHD populations.
Assessing implicit self-perceptions of competence may inform mechanisms behind PIB. Cognitive deficits have been offered as an explanation for PIB, in that delays in executive functioning development prevent children with ADHD from having the perspective-taking, self-reflection, and synthesizing abilities needed to accurately assess their own competence (Owens et al., 2007). Relatedly, most TD preschoolers have inflated views of their competence owing to their immature cognitive development, perceptions which progressively align with reality as children age; school-aged children with ADHD may be cognitively functioning on a younger level (McQuade et al., 2011). An implication is that inflated self-perceptions among children with ADHD do not result from biases in how they wish to present themselves; rather, overly positive self-evaluations are internalized and may therefore exist on an implicit, as well as explicit, level.
In support of the cognitive deficit hypothesis, children with ADHD show maturation delays in the prefrontal cortex (Barkley, 1997). Among children with ADHD, those with poorer executive functioning, cognitive fluency, and working memory have larger explicitly measured PIB in the social (although not in the behavioral) domain (McQuade et al., 2011). Some evidence suggests that as children with ADHD become older, their self-perceptions of their behavioral conduct (although not their social acceptance) become more aligned with adult-informant ratings, resulting in reductions in PIB (Hoza, Murray-Close, Arnold, Hinshaw, & Hechtman, 2010), although importantly other research finds PIB to persist among adults with ADHD (e.g., Knouse, Bagwell, Barkley, & Murphy, 2005; Lui, Johnston, Lee, & Lee-Flynn, 2013).
The self-protective hypothesis, by contrast, states that inflated self-ratings of competence reflect the desire of children with ADHD to protect their ego (Owens et al., 2007). Children with ADHD may be consciously aware of their deficits, but elect to not report them on explicit measures because of social desirability concerns. Another possibility is that children have suppressed the painful information that they have deficits from their conscious awareness, akin to ego defensiveness (Owens et al., 2007), but unconscious awareness of these deficits remains. An implication is that inflated self-perceptions should exist on an explicit level, but be substantially reduced or absent on an implicit level.
Evidence for the self-protective hypothesis comes from findings that when children with ADHD receive experimentally manipulated positive feedback, they deflate their explicit self-reports of competence, making their self-reports closer to their actual performance, thereby reducing their PIB (Diener & Milich, 1997; Ohan & Johnston, 2002); TD children do not show this pattern. It is thought this result occurs because children with ADHD explicitly report inflated self-ratings of competence for the purpose of appearing more capable, but when the threat of not appearing competent is reduced, they report their competence accurately. Consistent with this idea, Emeh and Mikami (2014) found that critical feedback given by parents to their children in a naturalistic observation was associated with larger PIB regarding social competence for children with ADHD, but not for TD children. In addition, positive associations are also found between PIB and measures of social desirability among children with ADHD, but not TD children (Ohan & Johnston, 2011).
Hypotheses
Based on significant literature documenting PIB when self-perceptions are measured explicitly, we predicted that explicit self-ratings of social and behavioral competence would not differ between children with ADHD and TD children, but that children with ADHD would have lower external indices of actual competence. As no study to our knowledge has examined implicit PIB, we assessed two competing hypotheses based on cognitive deficits and self-protection in determining whether children with ADHD demonstrate inflated self-perceptions of competence (relative to external indices of competence) when self-perceptions are measured implicitly.
Method
Participants
Participants were 78 children ages 6.8 to 9.8 from suburban and rural areas in Southeastern United States. Twenty-three met criteria for ADHD (13 boys), and 55 were TD (26 boys). Children were 81% White, 4% Black, 4% Asian, 3% Latino, and 8% were mixed/more than one race. The average family income was US$101,375. Participants were taking part in a larger investigation testing interventions for social problems in ADHD (Mikami et al., 2013). From this larger investigation, all participants with ADHD and a randomly selected subsample of the TD children were enrolled.
Children with ADHD had at least six of nine symptoms of hyperactivity/impulsivity or inattention endorsed as occurring “often” or “very often” on the Child Symptom Inventory (Gadow & Sprafkin, 2002) by parents and teachers. Because the larger study focused on social problems, parents and teachers needed to report that children had social impairment using a scale modified from Dishion and Kavanagh (2003). ADHD diagnosis was confirmed on the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Aged Children (K-SADS; Kaufman et al., 1997) administered to parents, which is keyed to Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000). Most (18 of 23) children with ADHD fit the Combined Type, and five were Inattentive Type. Oppositional Defiant Disorder (n = 12) and internalizing comorbidities (n = 11) were prevalent. Children receiving medication for ADHD (n = 10) remained on the same dosage/schedule for the study duration and were included as there is no evidence that medication improves children’s accuracy in their self-rated competence (Ialongo, Lopez, Horn, Pascoe, & Greenberg, 1994).
TD children could not have more than three symptoms of inattention or hyperactivity/impulsivity endorsed by parent or teacher (and less than five ADHD symptoms total), had minimal social difficulties, and did not meet criteria for any disorder on the K-SADS. Exclusionary criteria for all participants were Pervasive Developmental Disorder or Full Scale IQ below 80 on the Wechsler Abbreviated Scale of Intelligence (Wechsler, 1999). ADHD and TD groups did not differ in gender ratio, age, ethnicity, or family income (see Mikami et al., 2013, for further details about the sample).
Procedure
All procedures were approved by an institutional review board. Parents and teachers provided consent, and children assented. At a lab visit, children completed the measure of explicit self-perceptions of competence. Parents (in lab) and teachers (via mail) rated the child’s actual competence. Afterward, all children (ADHD and TD) were enrolled together in a 2-week summer program, which is described extensively in Mikami et al. (2013). During the summer program (on various days), participants completed the measure of implicit self-perceptions of competence. Short-term behavioral treatment in a summer program does not change explicit PIB (Mikami, Calhoun, & Abikoff, 2010); therefore, we did not expect that our summer program would affect implicit self-perceptions.
Measures
Self-perception profile for children (SPPC)
The SPPC (Harter, 1985) is the measure most commonly used to assess PIB in the ADHD literature (Owens et al., 2007). Research assistants read the Social Acceptance (six items) and Behavioral Conduct (six items) subscales to children in individual interviews. Items describe two kids (e.g., “some kids find it hard to make friends; other kids find it’s pretty easy to make friends”). Children select the description with which they identify, and report whether the description is “really true” or “sort of true,” resulting in a score for each item on a 4-point metric. Although the SPPC was intended for children aged 8 and older, it has been used successfully with younger children with ADHD (Ohan & Johnston, 2002); omitting the participants younger than age 8 in our sample did not change results. Internal consistencies in our sample were .70 for Social Acceptance and .85 for Behavioral Conduct subscales. Higher scores indicated higher explicit self-perceptions of social and behavioral competence.
Implicit Association Test (IAT)
The IAT is a computerized reaction time test with strong psychometric properties (Greenwald et al., 1998) where participants sort target stimuli into superordinate categories to assess the relative strength of associations between concepts. Research assistants administered the social competence and behavioral competence IATs in counterbalanced order. For the social competence IAT, words were used as stimuli for the categories self (me, myself, I) versus others (them, her, him), and three pictures of peer-accepted children versus three pictures of peer-rejected children were used as stimuli for the categories accepted versus rejected. Research assistants first ensured that children understood which stimuli represented each category before administering the critical trials.
Children were instructed to press the left button when they saw either words that represented the self or pictures that represented acceptance (self + accepted pairing), and to press the right button when they saw either words that represented others or pictures that represented rejection (others + rejected pairing). Signs with the words and pictures were placed next to the button that children were to press when they saw these stimuli. Then, pairings were reversed so that self was associated with rejection and others associated with acceptance. Conditions were counterbalanced so half the children paired self with rejection first and half with acceptance first, as is standard practice. An analogous design was used for the behavioral competence IAT, except that pictures depicting well-behaved versus misbehaving children were used.
It is presumed that participants make classifications more quickly when pairings are congruent with their automatic associations in memory (i.e., one should be faster when self is paired with accepted, vs. with rejected, if one has positive implicit social self-competence). A D score was calculated representing the mean response time for the block of self + accepted/well-behaved (and others + rejected/misbehaving) minus the mean response time for the block of self + rejected/misbehaving (and others + accepted/well-behaved), divided by the standard deviation of all blocks (Greenwald, Nosek, & Banaji, 2003). Larger D values, calculated separately for social and behavioral competence IATs, indicate higher implicit self-perceptions of social and behavioral competence.
Note that we made recommended modifications to the standard IAT to make it suitable for children with low attention spans and reading levels (Thomas, Burton Smith, & Ball, 2007). Specifically, we used pictures as stimuli, placed the pictures/words that represented each category next to the associated button as a reference, and reduced the number of trials in each block from 180 to 144. These modifications make the IAT suitable for children as young as age 4 (Cvencek, Greenwald, & Meltzoff, 2011), and all reflect common variations of IATs (e.g., IAT studies often vary in number of trials, use of word vs. picture stimuli). In addition, we added a practice IAT in which children classified stimuli into the target categories self versus others paired with the categories adults versus kids (using pictures of adults and children, respectively), to help children become accustomed to the task. Inclusion of a practice task is also common in IAT studies.
Given the novelty of these specific IATs, a series of checks were conducted to evaluate design choices. To ensure the stimuli reflected the categories of interest, we first piloted the pictoral stimuli by collecting 29 images from the Internet and image databases that exemplified the target categories (accepted, rejected; well-behaved, misbehaving). When pictoral stimuli involved multiple people (e.g., a child being bullied by peers), a red circle was drawn around the child intended to represent the category of interest. A pilot sample of 15 adults and two children, none of whom were participants in the final sample, sorted all images into the target categories, and the three images most frequently associated with each category were retained. All pictoral stimuli and full details on IAT design are available from the first author.
Furthermore, to check the suitability of the IAT with this sample, we examined several well-validated indicators that participants were able to successfully complete the task. Encouragingly, most participants completed the IAT with acceptable accuracy rates of at least 70%, a criteria suggested by Greenwald et al. (2003). On average, both TD children and children with ADHD classified more than 90% of stimuli accurately (TD: M = 95%, SD = 4; ADHD: M = 91%, SD = 7). Although there was significant difference between groups, t(75) = 2.74, p = .01, d = .70, this difference is not likely to be practically meaningful given that both groups performed with high accuracy and only four children (one TD, three ADHD) responded to more than 30% of IAT trials incorrectly. 1
There was also comparability between TD and ADHD children in their response latencies. Based on scoring recommendations made by Greenwald et al. (2003), trials taking longer than 10,000 ms were deleted, a 600 ms penalty was added to the response latency of incorrect responses (to account for differences in response latencies and error rates based on speed), and data were truncated such that latencies less than 300 ms were changed to 300 ms and latencies greater than 5,000 ms were changed to 5,000 ms. After these standard procedures, response latencies of children with ADHD (M = 2,332.99, SD = 911.84) did not differ from those of TD children (M = 2,073.70, SD = 730.92), t(75) = −1.29, p = .20, d = .31, again supporting the suitability of this task for this sample (though participants did show more variability than is typical 2 ).
Note that we reran the main analyses using different variants of the IAT score to increase confidence in the robustness of our findings. Specifically, data were reanalyzed using (a) raw IAT scores (generated before response latencies were truncated and penalties were added), (b) IAT scores before response latencies were truncated but after penalties, (c) IAT scores after penalties and when response latencies were truncated but not transformed, and (d) after penalties and with truncated and transformed IAT scores. Results were consistent in all cases.
External index of competence
Parents and teachers independently completed an adult-informant version of the Social Acceptance and Behavioral Conduct subscales on the SPPC about the child’s competence in these areas (Harter, 1985). The format is parallel to the SPPC but includes three questions per subscale. The subscale mean for each domain was computed; higher scores indicate higher child social and behavioral competence. In the PIB literature, it is common for parents and teachers to complete this measure as an external indicator of the child’s actual competence to which the child’s self-reports on the SPPC are compared (Hoza et al., 2004; Hoza et al., 2010). Internal consistencies were high for both informants and subscales (αs = .89-.95). Parent and teacher ratings were correlated (social acceptance: r = .52, p < .01; behavioral conduct: r = .68, p < .01). Because of the moderate to strong associations between parent and teacher ratings, we computed the mean of the parent and teacher reports of the child’s competence in social and behavioral domains to obtain a more reliable estimate than a single report, and considered these as external indices of children’s social and behavioral competence.
Calculation of PIB
Following the tradition in the PIB literature, explicit PIB was calculated by subtracting the standardized score of the adult-informant index of competence from the standardized score of the child’s self-report on the SPPC (De Los Reyes & Kazdin, 2005). Implicit PIB was calculated by subtracting the standardized score of the adult-informant index of competence from the standardized score of the child’s IAT D score. We note that as an alternative, Laird and Weems (2011) proposed a regression model to calculate PIB. However, because this study examines a novel type of PIB, using an implicit measure, we used the standardized discrepancy score for a more intuitive interpretation of results.
Results
Descriptive Statistics
All children had complete data on explicit and implicit self-perceptions of competence and on parent ratings of competence. For two children missing teacher ratings of competence, parent ratings (instead of the mean of parent and teacher ratings) were used as the external index of competence. Variables were roughly normally distributed with no outliers exceeding 3 SDs from the mean for any variable, with the exception of adult-informant ratings of behavioral competence for which there was one outlier 3.2 SDs below the mean. Changing this to a value of exactly 3 SDs below the mean did not alter results, so we left it untransformed.
As displayed in Table 1, adult-informant reports were modestly associated with child self-perceptions of competence. Children’s explicit and implicit self-perceptions of competence were uncorrelated; however, variable relations are common among implicit and explicit measures of a construct, depending on moderators like social desirability (Nosek, 2005).
Correlations Between Study Variables.
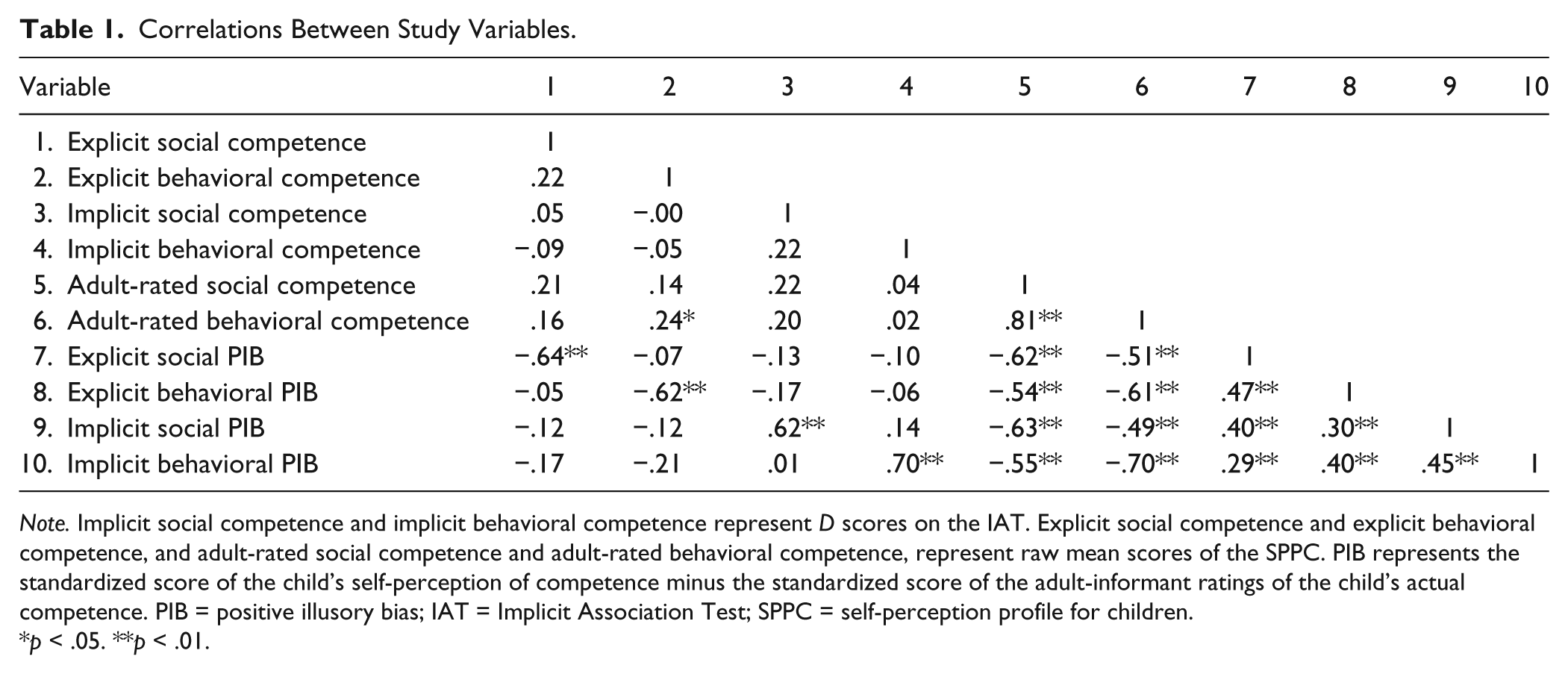
Note. Implicit social competence and implicit behavioral competence represent D scores on the IAT. Explicit social competence and explicit behavioral competence, and adult-rated social competence and adult-rated behavioral competence, represent raw mean scores of the SPPC. PIB represents the standardized score of the child’s self-perception of competence minus the standardized score of the adult-informant ratings of the child’s actual competence. PIB = positive illusory bias; IAT = Implicit Association Test; SPPC = self-perception profile for children.
p < .05. **p < .01.
Self-Perceptions and PIB
Table 2 contains analyses showing that children with ADHD and TD children did not differ in their explicit self-reports of social or behavioral competence. Adult informants rated children with ADHD as having lower social and behavioral competence, relative to TD children. As such, independent-samples t tests suggested that children with ADHD had larger explicit social and behavioral PIB scores than TD children, as expected.
Differences in Competence Between Children With ADHD and TD Children.

Note. Implicit social competence and implicit behavioral competence represent D scores on the IAT. Explicit social competence and explicit behavioral competence, and adult-rated social competence and adult-rated behavioral competence, represent raw mean scores of the SPPC. PIB represents the standardized score of the child’s self-perception of competence minus the standardized score of the adult-informant ratings of the child’s actual competence. TD = typically developing; CI = confidence interval; PIB = positive illusory bias; IAT = Implicit Association Test; SPPC = self-perception profile for children.
p < .05. **p < .01.
Table 2 also shows that children with ADHD and TD children did not differ in their implicit self-perceptions of social or behavioral competence. Because adult informants rated children with ADHD as having low competence, this resulted in children with ADHD having larger implicit social and behavioral PIB scores than TD children.
One issue with calculating PIB via discrepancy scores is that this method obscures whether PIB in the ADHD group is solely driven by lower levels of actual competence found in children with this condition. To address this concern, we recalculated PIB as the standardized discrepancy between children’s self-perceptions of competence and parent ratings of child competence. Then, we reconducted analyses assessing ADHD–TD group differences in PIB when controlling for teacher ratings of competence. In all cases (for both explicit and implicit PIB, in the social and behavioral domains), ADHD–TD group differences remained significant, suggesting that findings may persist above and beyond the tendency for children with ADHD to have lower actual competence.
Discussion
Consistent with previous literature, children with ADHD, but not TD children, had inflated explicit self-perceptions relative to adult ratings of their competence; that is, they demonstrated explicit PIB. This was attributable to the fact that children with ADHD and TD children did not differ in their explicitly reported self-perceptions of competence, but children with ADHD were rated lower by adult informants in their actual competence. Intriguingly, a similar pattern was found on the implicit measures. Children with ADHD also had larger implicit PIB related to social and behavioral competence compared with TD children, because they did not differ from TD children in their implicit self-perceptions of competence despite receiving lower ratings of competence from adult informants.
The self-protective hypothesis has been the leading explanation for PIB (Owens et al., 2007). However, children with ADHD in the current study demonstrated larger PIB than TD children on both implicit and explicit measures, suggesting that inflated self-competence may not be solely attributable to children having blocked painful perceptions of ineptitude from conscious awareness, or desiring to appear competent to others. Rather, our results suggest that children with ADHD may be unaware of their social and behavioral deficits on an implicit measure thought to reflect associations that reside largely outside of conscious control or awareness and to be relatively free from the effects of social desirability.
If inflated self-perceptions do operate on an implicit level, one implication is that PIB may be at least partially explained by cognitive deficits. Future research might examine whether, within the ADHD population, children with better developed prefrontal cortices demonstrate less implicit as well as explicit PIB. In addition, if implicit PIB is related to cognitive deficits, then implicit (along with explicit) PIB may decrease with age. Unfortunately, the narrow age range and the small ADHD sample size in our study precluded testing these possibilities. Furthermore, it is also possible that repeated defensiveness and seeking of self-protection on an explicit level could lead to changes in implicit perceptions over time; this possibility should be examined in subsequent research.
The novelty of the IAT to measure self-perceptions of competence among children with ADHD is both a strength and a limitation of this study. Our results shed light on a previously untested research question: whether PIB exists on an implicit level for children with ADHD. However, we cannot be certain that the IAT accurately measured children’s implicit self-perceptions given this is the first evaluation, especially because the nature of ADHD and its associated cognitive deficits may have led to variable responding and lower reliability on the IAT. Relations between implicit and explicit measures vary considerably as a function of moderator variables (see Nosek, 2005), making it difficult to determine whether the absence of an implicit–explicit correlation reflects a true null finding or a limitation of the specific implicit task to capture the construct of interest. It will be important in future work to show that implicit PIB predicts expected outcomes and to further establish the psychometrics of the measure. That said, there have literally been hundreds of IAT studies at this point, including many assessing self-concept in ways similar to the current study, and involving young children as participants (Baron & Banaji, 2006; Greenwald, Poehlman, Uhlmann, & Banaji, 2009). We followed standard procedures for adapting the task for children and examined numerous alternate scoring options to check the robustness of our findings—all of which yielded consistent results.
Other limitations are that, although we considered self-protection and cognitive deficits as explanations for PIB, the mechanisms behind these explanations (e.g., self-presentation desires or cognitive functioning) were not measured. In addition, whereas children with ADHD demonstrate explicit PIB in multiple domains (e.g., social, behavioral, academic, athletic; Owens et al., 2007), this study only investigated social and behavioral PIB. Furthermore, although it is standard in the PIB literature for adult-informant reports to compose the external index of children’s actual competence, this leaves open the possibility that adults may have inaccurately rated children’s competence. Finally, the ADHD group was small, which prevented exploration of results by ADHD subtype or comorbidities (known to be associated with explicit PIB; Owens et al., 2007).
Despite these limitations, the current study is the first to suggest that children with ADHD may display PIB on an implicit level as well as an explicit level and contributes to our understanding of this phenomenon. Explicit PIB has clinical significance, in that it may uniquely portend later maladjustment (Jia, Jiang, & Mikami, 2015) and predict children receiving less benefit from empirically supported behavioral interventions for ADHD (Mikami et al., 2010). Understanding implicit PIB may provide more insights into, or a way of addressing, PIB in ADHD populations.
Footnotes
Acknowledgements
We would like to thank the participating families and many graduate and undergraduate research assistants who contributed to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding to the second author from National Institute of Mental Health Grant 1R21 MH091486.