
Abstract
Introduction
ADHD is a heterogeneous condition that may present with or without co-occurring psychiatric disorders. An early meta-analysis of comorbidity studies comparing children with and without ADHD reported mean odds ratios of other psychiatric disorders of 10.7 (95% confidence interval [CI] = [7.7, 14.8]) for conduct disorder, 5.5 (95% CI = [3.5, 8.4]) for depression, and 3.0 (95% CI = [2.1, 4.3]) for anxiety disorders (Angold, Costello, & Erkanli, 1999). Larson, Russ, Kahn, and Halfon (2011) recently analyzed parent-reported data from the 2007 National Survey of Children’s Health and found that in children aged 6 to 17 years with ADHD, 33% had one other comorbidity, 16% had two, and 18% had three or more comorbidities. Consistent with previous literature (see Barkley, 2006), the researchers found significantly higher rates of several psychiatric disorders among children with ADHD as compared with children without ADHD: conduct disorder (27% vs. 2%), depression (18% vs. 2%), and anxiety (14% vs. 1%). Disruptive behavior disorders are comorbid with ADHD roughly 50% of the time, and anxiety and depressive disorders are comorbid with ADHD approximately 25% to 30% of the time (Barkley, 2006, pp. 206-207).
Rates of comorbidities among children with ADHD vary across settings, and tend to be lower in community samples (Barkley, 2006; Bauermeister et al., 2007; Jarrett & Ollendick, 2008). Bauermeister and colleagues (2007) report the following prevalence of comorbid disorders in community and clinical settings, respectively: oppositional defiant disorder (ODD) 38.9% versus 61.2%; conduct disorder (CD) 13.2% versus 10.2%; any anxiety disorder 24.5% versus 33.5%; and any depressive disorder 9.3% versus 22.7%. However, this study did not examine the impact of specific comorbid disorders on functioning.
To meet ADHD diagnostic criteria, children must have several ADHD symptoms in multiple settings and clear evidence that ADHD symptoms interfere with or reduce the quality of social, academic, or occupational functioning (American Psychiatric Association [APA], 2013). Children with ADHD experience these impairments across academic, social, and familial contexts (Barbaresi, Katusic, Colligan, Weaver, & Jacobsen, 2007; Counts, Nigg, Stawicki, Rappley, & von Eye, 2005; Frazier, Youngstrom, Glutting, & Watkins, 2007; Hoza et al., 2005; Massetti et al., 2008; Mikami, Huang-Pollock, Pfiffner, McBurnett, & Hangai, 2007; Strine et al., 2006). When complicated by comorbidities, the functioning of children with ADHD is further strained (Counts et al., 2005; Massetti et al., 2008; Mikami & Pfiffner, 2008). Comorbid conditions are associated with poorer outcomes in academic achievement, grade retention and other school problems, delinquency, social competence, parent–child communication, and parental aggravation (Counts et al., 2005; Massetti et al., 2008; Sibley et al., 2011). Each of these studies examined only a single domain of functioning.
The functional impact of comorbidities has been found to be so significant that some have asserted that certain comorbidity profiles may represent distinct ADHD subtypes (Jensen, 2001), referred to in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) as presentations (APA, 2013, p. 60). There may be a dose-response between the presence of comorbidities and functional outcomes; Larson et al. (2011) have concluded that functioning declines in a stepwise fashion as the number of comorbid diagnoses increases. This group measured school problems, grade repetition, social competence, and parental aggravation. However, the study used parent-reported diagnoses and did not look at the impact of specific comorbid diagnoses on functional outcomes.
Kessler and colleagues (2014) report on the U.S. National Comorbidity Survey Adolescent Supplement (NCS-A). This is a large, community-based study using standardized diagnostic instruments. The study found that disruptive behavior disorders (DBD; defined in this study as CD, ODD, intermittent explosive disorder, and eating disorders) in children with DBD comorbid with ADHD accounted for the roughly half of the effect on below average grades and a third of the effect on repeating a grade, while depression and anxiety disorders had relatively little mediation of these outcomes. DBD also accounted for more than a third of the effect on school suspension, while ADHD had a direct effect of about the same amount. The direct effect of ADHD accounted for a majority of the effect on repeating a grade (68.2%) while DBD accounted for 33.9%. Although this is an important study of the impact of comorbidity on the functioning of children with ADHD, this study did not examine important areas of functioning, including peer and parent relationships and contact with the legal system.
In summary, previous research studies exhibit the following limitations: (a) focused on a single or limited number of domains of functioning, (b) considered the impact of only the most common comorbidities, (c) relied only on parent-report of diagnostic history, or (d) used participant samples that are likely to suffer from ascertainment biases (e.g., clinic-referred or convenience samples). Further, the epidemiology of ADHD continues to evolve (Centers for Disease Control and Prevention, 2010; Visser et al., 2014), suggesting that the epidemiology of conditions comorbid with ADHD and their associated impacts may also be changing over time.
The Project to Learn About ADHD in Youth (PLAY) is a multi-site, community-based epidemiological study of children with and without ADHD that measures the prevalence of internalizing and externalizing disorders and examines the cross-sectional impact of these comorbidities on functional outcomes. To our knowledge, this is the first community-based study to combine rigorous diagnostic assessment with a broad array of functional domains including school, peer, family, and legal outcomes using teacher, parent, and child reports to examine the differential impact of specific comorbid disorder groups. Specific hypotheses as were follows:
Method
Study Sample and Screening Procedures
PLAY is an epidemiological study that used a two-phase design to identify ADHD in elementary school-age children. The study method has been described in detail elsewhere (Wolraich et al., 2014). Briefly, teachers and parents completed ADHD screening instruments for elementary school-age children in one school district in South Carolina (SC; screening n = 4,604) and five school districts in Oklahoma (OK; screening n = 12,626), from 2003 to 2006. The grade range generally was Kindergarten through fifth grade, but a few schools in each site contained a preparatory class for 4-year-olds to get them ready for Kindergarten the following year. Of the eligible students, teachers reported on 54.3% in SC and 76.6% in OK.
Parents and teachers reported on ADHD diagnosis and medication status; teachers also completed the Vanderbilt ADHD Teacher Rating Scale (VADTRS; Wolraich et al., 2003) and, in the SC disctrict and three OK districts, the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1999). Children were considered “high screen” for ADHD if the parent or teacher reported either a prior ADHD diagnosis or use of ADHD medication, or if their teacher reported that the child had six or more symptoms in either or both ADHD dimensions (hyperactive/impulsive or inattentive) on the VADTRS and some impairment from either the SDQ (SC and initial three OK districts) or VADTRS (OK two additional districts). All other children were considered to be “low screen” for ADHD. All high-screen children and a randomly selected sample of low-screen children frequency-matched on gender were eligible to participate in the interview phase of the study.
Because the SDQ was not administered in the latter two OK districts, potential differences in impairment ratings on the SDQ and VADTRS were evaluated among the sample subset that had data on both measures. These measures were found to be in agreement (indicating intermediate impairment) for 86.5% of cases (kappa = 0.68). Therefore, data from all six school districts were used to allow for greater stability in estimating the impact of comorbidities on functional impairment based on ADHD status.
Diagnostic Data
The diagnostic interview took place approximately 1 year after screening and included the Diagnostic Interview Schedule for Children, version IV (DISC; Shaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000), reflecting diagnostic criteria for mental disorders as described in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000). Parents completed DISC modules for ADHD, generalized anxiety disorder (GAD), obsessive compulsive disorder (OCD), posttraumatic stress disorder (PTSD), major depression/dysthymic disorder, mania/hypomania, ODD, and CD in both sites. Parents in SC also completed DISC modules for separation anxiety disorder and social phobia. Children met ADHD case definition criteria if a parent reported six or more symptoms in at least one dimension with associated impairment and age of onset before age 7 years on the DISC and, to consider multiple settings and multiple informants, at least four symptoms with some impairment reported by the teacher at the screening phase. Children who were receiving medication for ADHD at the time of the interview were required to meet these criteria to be considered an ADHD case.
As previously published, the community-based prevalence estimates for OK (three school districts) and SC (one school district) were 10.6% and 8.7%, respectively (Wolraich et al., 2014). The prevalence estimates for the two additional OK school districts were not previously reported; these estimates are 7.1% (95% CI = [4.5, 11.1]) and 6.7% (95% CI = [3.7, 11.8]). Using data from all of the OK school districts reduced the overall OK community-based prevalence estimate from 10.6% to 8.6% (95% CI = [6.6, 11.1]). The number of participants with complete DISC data was 479 (75.7% of invited children) in SC and 577 (22.6% of invited children) in OK.
Demographic Data
Demographic information was collected from parents using a separate questionnaire. Some participants did not report income (SC: 6.4%; OK: 10.2%) and number of dependents (SC: 4.1%; OK: 10.0%); these indicators were imputed using multiple imputation techniques (Berglund, 2010). Race/ethnicity, presence of two adults in the household, whether the child qualified for free school lunch or was covered by Medicaid were used to derive five sets of imputed values for household income and number of dependents. Complete imputed data were used to dichotomize poverty status for participants as living below or above the 200% federal poverty level (FPL).
Functional Outcome Data
The functional impact of ADHD and comorbidities was estimated for several academic and social outcomes. During the screening process, teachers reported on performance in reading, mathematics, and written expression on the VADTRS; children whose teacher reported their academic performance as below average in two or three subjects were considered to be below average. In the DISC interview, parents reported whether their child had ever been held back a grade in school or had ever been expelled, suspended, had an in-school suspension, or been in trouble with the police. In SC only social functioning was measured by child report using the Peer Relationship, Parent Relationship, and General Self (measuring self-confidence, self-satisfaction, and self-worth) subscales of the Self-Description Questionnaire (Bryne, 1996; hereafter referred to as Marsh to distinguish from the Strengths and Difficulties Questionnaire), and by parent report using the SDQ Prosocial subscale. For social functioning outcomes, the outcome of interest was whether the child’s subscale score was in the sample’s lowest quartile.
Data Analysis
All analyses were conducted using Statistical Analysis Software (SAS)-callable SUDAAN v. 11.0.0 (RTI International; Cary, North Carolina) to account for the complex sampling design and sample weights. Sample weights were calculated to reflect differential probability of selection for inclusion in the sample and non-response among eligible participants; weighted estimates were designed to be representative of the study school districts’ populations. Weighted estimates of demographic characteristics and prevalence of comorbid disorders are presented. Inferential tests of association for weighted analyses were based on Fellegi-adjusted Wald F statistics (Fellegi, 1980).
Logistic regression models and odds ratios (ORs) were used to evaluate the effect of comorbid disorders on school and social outcomes after controlling for sex, race, poverty status, and site. In total, 44 participants of other racial/ethnic minority groups (not African American, American Indian, or Hispanic) were excluded from the logistic models due to small size.
Results
Sample demographics are presented by ADHD status and site (Table 1). In total, 479 participants in SC and 577 participants in OK completed all DISC modules. Distribution of sex was similar between the two sites; however, there were some racial/ethnic and income differences.
Demographic Characteristics by PLAY Study Site, Stratified by ADHD Case Definition Status (Weighted Percentage).
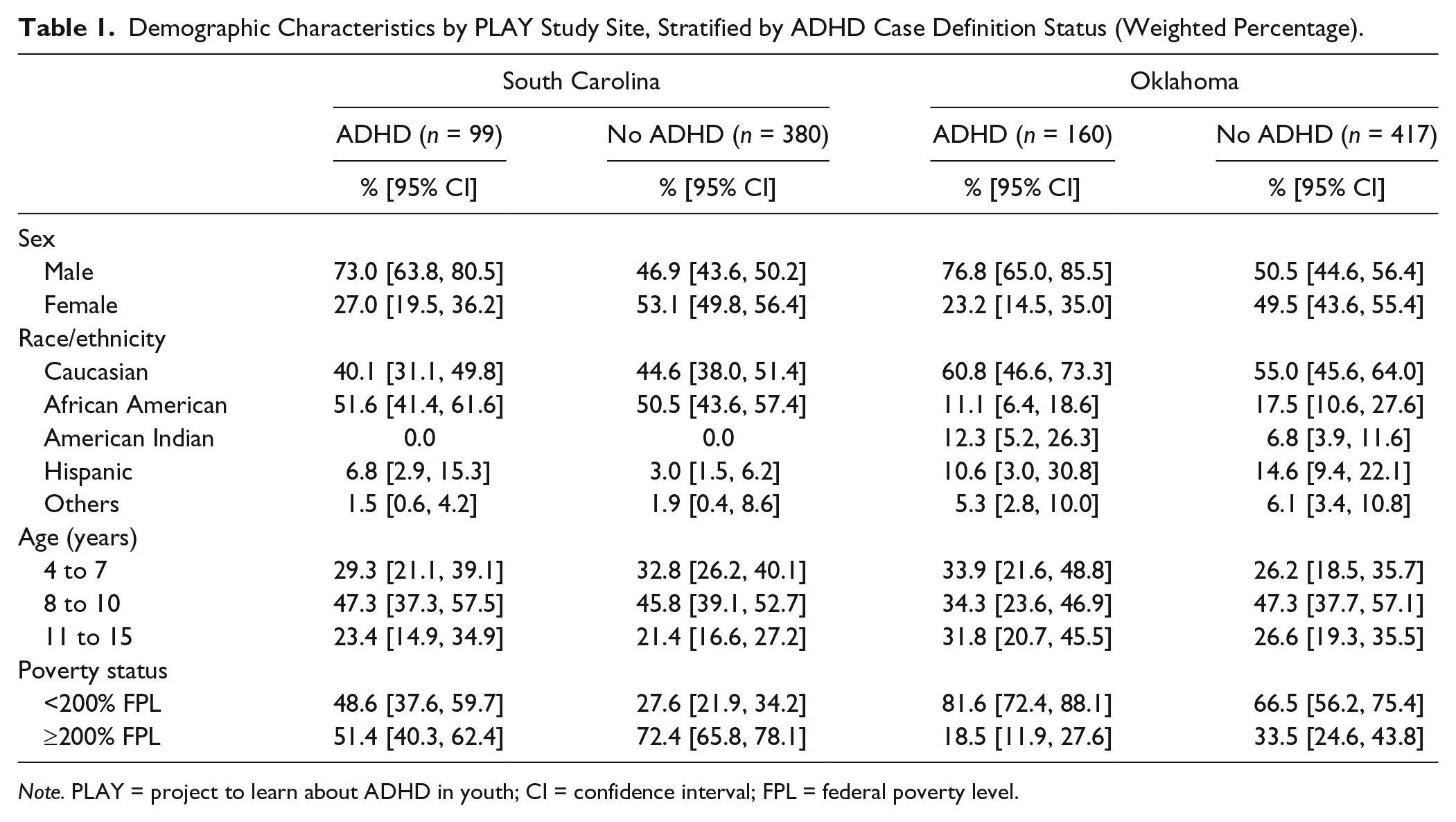
Note. PLAY = project to learn about ADHD in youth; CI = confidence interval; FPL = federal poverty level.
Table 2 presents the prevalence of psychiatric disorders in children with and without ADHD stratified by study site. Although ADHD prevalence was similar across sites, the prevalence of most other disorders was higher in OK than in SC in both ADHD and non-ADHD groups. Prevalence was several times higher for many comorbid disorders in the ADHD group than the non-ADHD group in both sites, although confidence intervals were wide for many estimates. In SC, 54.7% of children with ADHD had at least one other disorder, and 22.4% had two or more, compared with 12.5% in the non-ADHD group having any disorder other than ADHD, F(1, 475) = 55.6, p < .001, and 2.7% having two or more disorders, F(1, 475) = 30.7, p < .001. In OK, 64.8% of children with ADHD had at least one other disorder, and 32.5% had two or more additional disorders, compared with 21.7% of the non-ADHD group having any disorder, F(1, 565) = 26.5, p < .001, and 8.4% having two or more disorders, F(1, 565) = 11.6, p < .001. Children in OK were significantly more likely to have one or more conditions other than ADHD than children in SC, 25.3% versus 16.0%; F(1, 1042) = 5.5, p = .02. There were no cases of mania in the SC cohort, although three children did meet criteria for hypomania, while in the OK sample six children met criteria for mania, and six met for hypomania. Children with major depressive disorder, dysthymic disorder, mania, and hypomania were grouped during further analyses and are presented as “mood disorders.”
Weighted Prevalence of DSM-IV Disorders Among Children With and Without ADHD Based on DISC-IV Criteria, by PLAY Study Site, and ADHD Case Definition Status.
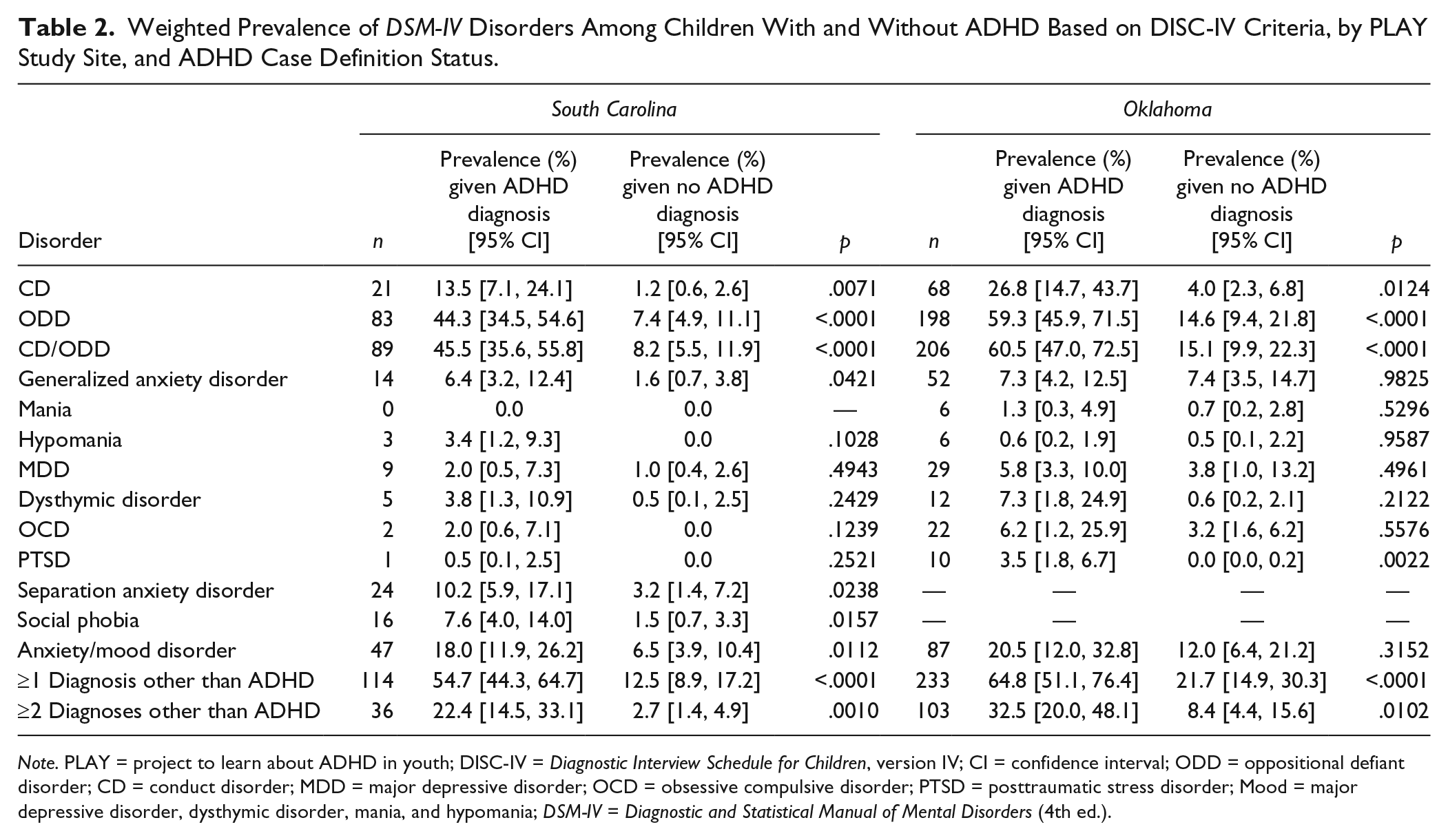
Note. PLAY = project to learn about ADHD in youth; DISC-IV = Diagnostic Interview Schedule for Children, version IV; CI = confidence interval; ODD = oppositional defiant disorder; CD = conduct disorder; MDD = major depressive disorder; OCD = obsessive compulsive disorder; PTSD = posttraumatic stress disorder; Mood = major depressive disorder, dysthymic disorder, mania, and hypomania; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.).
In SC, several internalizing disorders were significantly more common among those with ADHD: generalized anxiety disorder, F(1, 475) = 5.9, p < .05; separation anxiety disorder, F(1, 475) = 5.5, p < .05; and social phobia, F(1, 475) = 9.8, p < .05. The presence of any anxiety/mood disorder was also significantly higher among children with ADHD, F(1, 475) = 10.3, p < .05. In OK, the only internalizing disorder that was significantly more common among children with ADHD was PTSD, F(1, 565) = 26.3, p < .001. For both sites, prevalence of comorbid behavioral disorders (CD and ODD) was very high among those with ADHD and although these disorders were the most common disorders among the non-ADHD group, CD and ODD were significantly more common among those with ADHD: SC, F(1, 475) = 56.0, p < .001; OK, F(1, 565) = 34.4, p < .001.
In both sites, ADHD prevalence was higher among those below 200% FPL: SC, 14.4% versus 6.4%, F(1, 191) = 11.6, p < .001; OK, 10.3% versus 4.9%, F(1, 75) = 6.3; p < .05. The prevalence of having any other disorder was also higher among those below 200% FPL: SC, 30.3% versus 10.2%, F(1, 205) = 18.5, p < .001; OK, 30.5% versus 14.6%, F(1, 99) = 6.3, p < .05. Pooled logistic regression models revealed that the site indicator was not statistically significant in its association with the prevalence of another psychiatric disorder after adjustment for 200% FPL, and this was also the case for generalized anxiety disorder specifically. These findings suggest that socioeconomic differences between sites explained much of the site variations in disorder prevalence, including the differences in prevalence of generalized anxiety disorder.
Table 3 presents results related to academic performance and disciplinary actions. Children with no disorder (nSC = 322; nOK = 291) were compared with children with the following mutually exclusive disorder categories: ADHD alone (nSC = 42; nOK = 50); ADHD plus CD or ODD with or without an anxiety or mood disorder (CD/ODD; nSC = 47; nOK = 102); ADHD plus anxiety/mood disorder without CD/ODD (nSC = 10; nOK = 8); CD/ODD without ADHD regardless of anxiety or mood disorder (nSC = 42; nOK = 104); and anxiety/mood disorder without ADHD or CD/ODD (nSC = 16; nOK = 22).
Logistic Regression of Diagnostic Categories on Functional Outcomes Among the PLAY Participants, Pooled Across Study Sites.
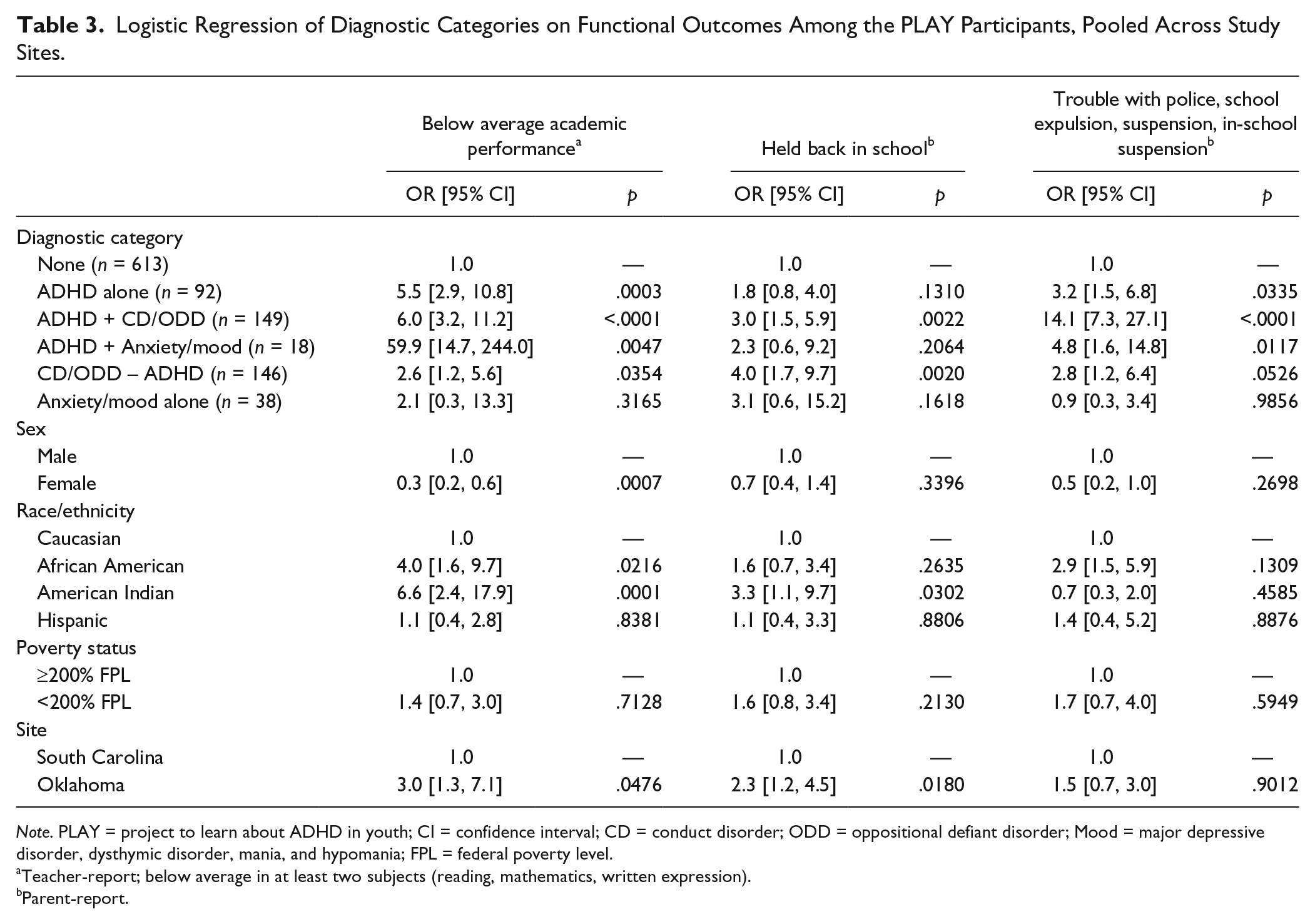
Note. PLAY = project to learn about ADHD in youth; CI = confidence interval; CD = conduct disorder; ODD = oppositional defiant disorder; Mood = major depressive disorder, dysthymic disorder, mania, and hypomania; FPL = federal poverty level.
Teacher-report; below average in at least two subjects (reading, mathematics, written expression).
Parent-report.
In pooled analyses, academic performance was significantly worse for children with any of the disorders except for anxiety/mood disorder alone when compared with children without a disorder. Children with ADHD combined with an anxiety/mood disorder had the largest OR for below average academic performance, but a wide confidence interval as a result of small sample size warrants caution when interpreting this estimate. Separate models were fit to determine differences in the academic performance between diagnostic categories using different comparison groups. Children with ADHD and comorbid anxiety/mood disorder were significantly more likely than children with ADHD alone to have below average academic performance (OR = 10.8, 95% CI = [2.4, 49.1]). Children with ADHD and comorbid CD/ODD were somewhat more likely than those with CD/ODD without ADHD to have below average academic performance (OR = 2.3, 95% CI = [1.0, 5.7]; p = .06).
Below average academic performance was more common in the OK sample, 32% versus 16% in SC; F(1, 1042) = 16.5, p < .001. Academic performance was significantly better among girls compared with boys. Both African Americans and American Indians were significantly more likely to be in the below average group compared with Caucasian children; Hispanic and Caucasian children were statistically similar on this academic outcome. This racial difference was carried by children with ADHD in SC, where 58% of racial/ethnic minority children with ADHD were below average versus 29% of Caucasian children with ADHD: F(1, 475) = 8.8, p < .01, and to a lesser extent in OK, where 77% of racial/ethnic minorities with ADHD versus 61% of Caucasians with ADHD were below average (not statistically significant). Also of interest is that poverty status was associated with academic performance only among racial minorities in SC, F(1, 178) = 24.9, p < .001; poverty was not associated with academic performance in OK.
Children with CD/ODD without ADHD were four times more likely to be held back in school than children without any disorder; children with CD/ODD and ADHD were three times more likely to be held back than children with no disorder. Being in trouble with police, school expulsion, or suspension was more common among all disorder groups except anxiety/mood disorder alone compared with children without a disorder. This association was largest for ADHD comorbid with CD/ODD; the association was also statistically significant for children with ADHD alone, ADHD and an anxiety/mood disorder, and CD/ODD alone. Children with ADHD and comorbid CD/ODD were significantly more likely than children with ADHD alone (OR = 4.3, 95% CI = [1.8, 9.8]) and CD/ODD alone (OR = 5.1, 95% CI = [2.1, 12.4]) to have trouble with police, school expulsion, or suspension. Children in OK were significantly more likely to be held back a grade, 21% in OK versus 8% in SC; F(1, 1042) = 13.3, p < .001.
Table 4 presents SC-specific logistic regression analyses on child-reported peer and parent relations and general self-scores as well as the parent-reported SDQ prosocial scale, modeling the likelihood of having a score in the lowest quartile. The analyses were conducted with data from SC only, as OK did not administer the Marsh instrument. Low peer relations (lowest quartile) were at least three times more likely among children with CD/ODD either alone or in combination with ADHD, as compared with children without a disorder; low peer relations were marginally significant for ADHD alone. Children with ADHD plus CD/ODD were more than twice as likely as those without any other disorder to report low parent relations scores. No diagnostic category was associated with scores in the lowest quartile on the Marsh general self-concept scale. Consistent with the nature of CD/ODD, parents of children with CD/ODD alone or comorbid with ADHD were at least four times more likely to report low prosocial behaviors compared with children without a disorder.
Logistic Regression of Diagnostic Categories on Lowest Quartile of Marsh (Child-Report) and SDQ (Parent-Report) Subscales From the South Carolina PLAY site.
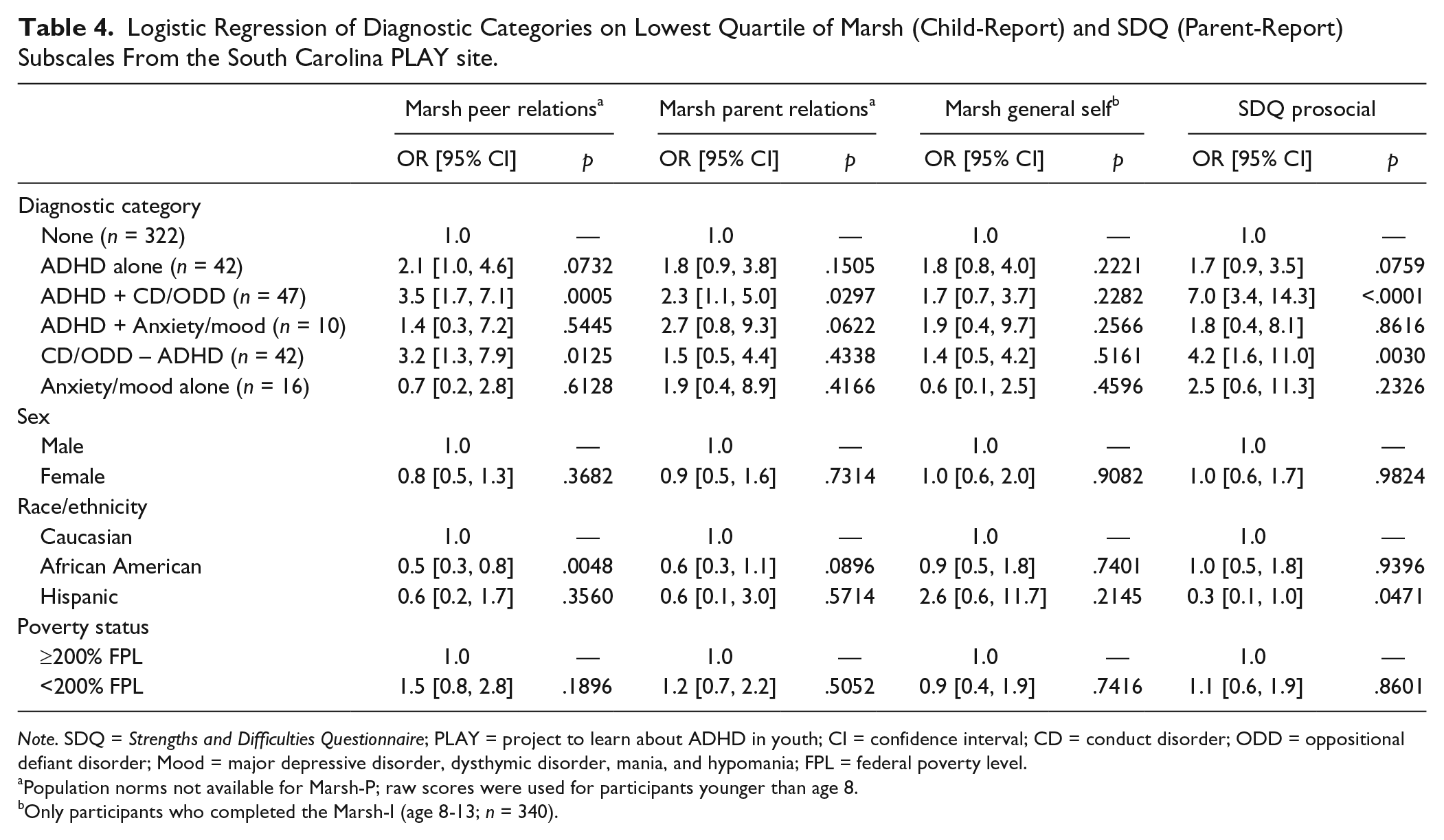
Note. SDQ = Strengths and Difficulties Questionnaire; PLAY = project to learn about ADHD in youth; CI = confidence interval; CD = conduct disorder; ODD = oppositional defiant disorder; Mood = major depressive disorder, dysthymic disorder, mania, and hypomania; FPL = federal poverty level.
Population norms not available for Marsh-P; raw scores were used for participants younger than age 8.
Only participants who completed the Marsh-I (age 8-13; n = 340).
Discussion
As expected, CD and ODD were the most prevalent comorbid disorders among children with and without ADHD, followed by anxiety disorders and mood disorders. Consistent with prior research, the majority of children with ADHD had at least one psychiatric comorbidity. The rate of having a comorbidity among children with ADHD was at least four times higher in SC and three times higher in OK than that of the respective non-ADHD groups. A child with ADHD is significantly more likely to have another psychiatric disorder. This ratio is similar to previous studies described earlier, and supports the idea that rates of comorbidities among children with ADHD are not changing significantly over time.
Although estimates of individual comorbid disorders were generally higher among OK children, these site differences did not reach statistical significance. However, the overall prevalence of having one or more comorbid disorder was significantly higher in OK, which was statistically accounted for by a larger percentage of children living below 200% FPL in OK, as was the higher prevalence of generalized anxiety disorder.
Children with ADHD with or without CD/ODD had higher odds of below average teacher-rated school performance than children without a disorder. The odds for ADHD alone and ADHD plus CD/ODD were both roughly twice that of CD/ODD alone. The odds for ADHD plus anxiety/mood were highest among the disorder groups for below average school performance. This estimate lacks precision; however, the lower end of the CI was greater than the upper end of CIs for other disorder groups. These data do not support the previous report of a stepwise decline in functioning for the addition of CD/ODD to ADHD for the academic performance outcome (Larson et al., 2011), although our data do support the conclusion that there may be increased impairment with the addition of anxiety or depression to ADHD. Due to the wide confidence intervals among children with ADHD and anxiety/mood disorders, the finding should be further examined by future studies.
To our knowledge, this is the first study to use community-based data to investigate the relationship between ADHD, comorbid disorders, and their impact on broad, cross-sector functional outcomes. These data extend our knowledge of the impact of comorbid psychiatric disorders on the functioning of children with ADHD and, if replicated, can inform policies, programs, and practices for children with ADHD. Specifically, our findings suggest that children with ADHD, particularly those with comorbid anxiety or depression, could benefit from psychoeducational testing and, if indicated, classroom accommodations, interventions, and support to improve academic performance. Children with ADHD and comorbid CD or ODD could also be targeted for interventions to prevent school dropout and involvement in legal systems. Consistent with the nature of the disorders, children with CD or ODD also have problems with peer and parent relations and have low prosocial scores. Early intervention with evidence-based parent training and skills training for children in this very high risk population may be particularly important, due to the high associated personal and societal costs and the demonstrated benefits of these interventions on family and peer functioning (Pelham & Fabiano, 2008; Thomas, 2010).
The only categories associated with being held back in school were CD/ODD either alone or comorbid with ADHD, which had similar rates of grade retention. Our findings suggest similar risk of grade retention across these two groups, with a slightly greater magnitude of risk for those with CD/ODD. Oppositional and behavior problems associated with CD/ODD may confer a slightly greater risk for being held back in school than the problems with executive functioning found in children with ADHD. This finding is somewhat inconsistent with the findings from the NCS-A (Kessler et al., 2014); the NCS-A showed ADHD responsible for 68.2% of the effect on repeating a grade; DBD, as defined in that study, were responsible for 33.9%; and for below average grades, 48.8% was attributable to DBD while ADHD accounted for 21.9%. Thus, in both studies DBD were associated with poor academic functioning, at times being more important than ADHD effects.
Children with ADHD were significantly more likely to get into trouble with police or be suspended/expelled from school. Children with ADHD and comorbid CD/ODD had the greatest odds of this outcome. In contrast to the previous finding regarding academic performance, this finding is consistent with the stepwise decrease in functioning found by Larson et al. (2011).
These results reveal that although the impact of ADHD and comorbidities on functioning is consistently negative, the relationship is complex. ADHD appears most strongly related to poor academic performance, while CD/ODD may be more strongly associated with disciplinary action or being held back in school. Although these data provide some support for the notion that psychiatric comorbidity impacts functioning in a stepwise fashion, the results vary by type of outcome variable. In addition, race was a significant covariate in several of the functional outcome models. More research is needed with larger samples to better understand the relationship between race, co-occurring psychiatric conditions, and school-related functional outcomes.
Limitations of this study include a lack of power to detect differences among certain disorder groups due to small sample size in those groups. Recruitment bias could have affected results; however, there were no statistically significant differences in demographics between the weighted proportions in the sample interviewed and the demographics of the school district as a whole. Another possible limitation is the use of parent and teacher reports of outcomes, rather than school or other administrative data that may be more accurate. This could lead to potential informant bias. To include multiple informants in the diagnostic algorithm, teacher screens performed up to a year prior to the diagnostic assessment were used, which could also possibly introduce bias if the child’s symptoms changed during this time. However, given that ADHD is a chronic disorder, and there is not likely to have been a systematic bias in one direction or another, it is unlikely this would have an impact on the findings. Finally, the study did not have a measure to address learning and language disorders although these conditions are common comorbidities (Bauermeister et al., 2007; Pelham & Fabiano, 2008) and may play a role in school performance. Strengths of this multi-site study include the use of two-stage epidemiological methods for obtaining racially diverse community-based samples of children with enhanced case finding, use of well-validated DSM-based measures, the use of multiple informants for diagnoses and functional outcomes, and the examination of multiple functional outcome domains.
In conclusion, more than half of the elementary-aged children with ADHD had a comorbid psychiatric disorder in this multi-site, community-based study of ADHD. Having ADHD alone or in combination with other psychiatric disorders significantly increased the risk of poor outcomes across multiple functional domains. Future analyses of the data from this epidemiological cohort of children can be used to better understand the longitudinal impact of ADHD and comorbid psychiatric disorders on the functional outcomes of children with ADHD. Collectively, these findings can be used to inform prevention and intervention efforts for the estimated 5.1 million U.S. children with a current ADHD diagnosis (Visser et al., 2014).
Footnotes
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The lead author has received research support from Vanguard Research Group through a grant from Otsuka Pharmaceuticals.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centers for Disease Control and Prevention through cooperative agreements U50/CCU622315-02 and U84/CCU422516-02 and contracts 200-2006-18912 and 200-2006-18949.