
Abstract
ADHD is characterized by developmentally atypical levels of inattention and/or hyperactivity and impulsivity (American Psychiatric Association [APA], 2013). Although once believed to be a disorder specific to childhood, it is now apparent ADHD persists into adolescence and adulthood in the majority of cases (Biederman et al., 2010). Prevalence estimates suggest approximately 4.4% of adults between the ages of 18 and 44 years meet criteria for ADHD (Kessler et al., 2006). Furthermore, the patterns of impairment and underachievement commonly associated with ADHD in childhood (DuPaul & Langberg, 2014) persist into adulthood (Molina et al., 2009). For example, in comparison with young adults without ADHD, those with ADHD attain lower levels of educational and occupational achievement (Biederman et al., 2008; Kuriyan et al., 2012). Young adults with ADHD also report poorer interpersonal skills (Shaw-Zirt, Popali-Lehane, Chaplin, & Bergman, 2005), more relationship problems (Canu & Carlson, 2007), and lower overall quality of life (Canu & Carlson, 2007; Shaw-Zirt et al., 2005).
Importantly, many individuals diagnosed with ADHD in childhood continue to experience significant impairment into adulthood, even when symptoms of ADHD have remitted to below the diagnostic threshold (Willoughby, 2003; Wolraich et al., 2005). One theory designed to explain why impairments persist or increase even after the remittance of ADHD symptoms is the cognitive-behavioral therapy (CBT) model described by Safren, Sprich, Chulvick, and Otto (2004; Figure 1). In this model, the underlying deficits that characterize ADHD (i.e., attention, inhibition, and self-regulation) lead to repeated failures and underachievement. Over time, these experiences lead to the development of negative thought patterns, low self-concept, and symptoms of anxiety and depression, in a cyclical pattern. These symptoms of anxiety and depression in turn result in an increased likelihood of future impairment (e.g., “I am no good at this and will fail anyway so why try?”). Therefore, even in the absence of persistent ADHD symptoms, past underachievement would continue to affect future functioning through increased negative cognitions and internalizing symptoms.

A cognitive-behavioral model of ADHD.
The Safren et al. (2004) model suggests that as individuals with ADHD age and experience underachievement, they begin to develop dysfunctional cognitions and beliefs. These negative cognitions often take the form of negative judgments about self-worth or value, reflecting a low self-concept. Some examples of negative thoughts related to self-concept include, “I am a loser” and “I always screw up” (Safren et al., 2004, p. 351), and adolescents with ADHD have been found to exhibit lower self-concept as related to their academic abilities in comparison with their peers (e.g., Major, Martinussen, & Wiener, 2013). However, as shown in Figure 1, these negative cognitions are not proposed to be directly related to impairment, but instead, lead to impairment through the eventual development of symptoms of anxiety and depression.
The temporal association outlined in the CBT model of ADHD is supported by research showing that depressive disorders typically develop several years after the onset of ADHD (Daviss, 2008). Indeed, the developmental literature suggests that rates of internalizing disorders among young adolescents with ADHD do not differ significantly from rates among young adolescents without ADHD (Bagwell, Molina, Kashdan, Pelham, & Hoza, 2006; Ruchkin, Lorberg, Koposov, Schwab-Stone, & Sukhodolsky, 2008). However, in emerging adult populations such as college students with ADHD, significantly higher levels of comorbid internalizing disorders relative to peers without ADHD have been reported (e.g., Chronis-Tuscano et al., 2010; Heiligenstein & Keeling, 1995). Some of the most rigorous evidence is provided by Anastopoulos et al. (2015), who conducted a large, multi-site study of an emerging adult college population using a multi-method, comprehensive assessment (including clinical interviews) to diagnose both ADHD and comorbid disorders. In a sample of 443 emerging adults (M age = 18.2), 32.3% of students with ADHD met criteria for a depressive disorder, compared with only 5.4% in the comparison group, and 28.6% met criteria for an anxiety disorder, compared with 3.6% in the comparison group. Studies using dimensional measures have also found higher rates of depressive and anxiety symptoms in college students with ADHD compared with those without ADHD (Rabiner, Anastopoulos, Costello, Hoyle, & Swartzwelder, 2008; Richards, Rosen, & Ramirez, 1999). These studies support the CBT model of ADHD, as they demonstrate internalizing symptoms are developing over time in many individuals with ADHD. However, less is known about whether these symptoms are then leading to future impairment, above and beyond the existing negative influence of ADHD symptoms.
To date, longitudinal studies examining the implications of comorbid internalizing symptoms in ADHD samples have largely focused on depression-specific outcomes, such as more severe psychopathology and increased risk for suicidal ideation (e.g., Chronis-Tuscano et al., 2010). Furthermore, this research has largely been limited to individuals who meet full criteria for Major Depressive Disorder or Dysthymia (e.g., Biederman et al., 2008). The CBT model of ADHD postulates that past underachievement leads to negative cognitions and symptoms of depression and anxiety, and these individuals may or may not meet full criteria for a depressive or anxiety disorder. Furthermore, it is unknown whether these symptoms are associated with impairment broadly, or if the increased impairment is limited to depression-related impairment (e.g., hospitalization and suicidal ideation). Given the high rates of internalizing symptoms during emerging adulthood, college seems to be an ideal developmental period to study the dimensional effect of comorbid symptoms on functional impairment.
The number of students with ADHD pursuing higher education has risen dramatically in the past 30 years, with current prevalence estimates for ADHD in college settings ranging from 5% to 8% (DuPaul, Weyandt, O’Dell, & Varejao, 2009; Wolf, Simkowitz, & Carlson, 2009). Most students pursuing a college degree fall in the age range of 18 to 25 years of age, which has been described as “emerging adulthood” (Arnett, 2000). This time period has been proposed to be a unique developmental stage for adults, marked by exploration and change in terms of employment, higher education, romantic relationships, and identity (Arnett, 2000). For many emerging adults, attending college represents one of these critical developmental changes in which individuals are faced with challenges such as a significant decline in external supports (e.g., parental supervision, teacher support) and an increase in environmental demands (e.g., academic independence, financial responsibility, maintaining personal health; Fleming & McMahon, 2012). These changes are particularly difficult for emerging adults with ADHD to navigate, and many experience significant impairment in the years following the transition to college (Weyandt et al., 2013). Relative to their non-ADHD peers, college students with ADHD have significantly lower GPA, are more likely to be placed on academic probation, and are less likely to graduate (e.g., Advokat, Lane, & Luo, 2011; Blase et al., 2009; Weyandt & DuPaul, 2013). However, it is not clear what role the development of comorbid internalizing symptoms has on the functioning of college students with ADHD as no longitudinal studies testing this association exist. Given that ADHD symptoms can also negatively affect functioning in college (Bruner, Kuryluk, & Whitton, 2015; Lewandowski, Lovett, Codding, & Gordon, 2008; Rabiner et al., 2008), to fully evaluate the CBT model of ADHD, it would be important to control for the trajectory of ADHD symptoms.
Accordingly, the present study uses a multi-method approach to evaluate the pathway to impairment proposed by the Safren et al. (2004) model. Specifically, we tested whether prior year GPA (i.e., past achievement/underachievement) affects future self-reported functional impairment through a negative self-concept (i.e., negative cognitions) and the subsequent trajectory of depressive and anxiety symptoms. Consistent with a developmental approach, this association was evaluated controlling for baseline self-reported functional impairment as well as changes in ADHD symptoms. In this study, we used prior year GPA as a measure of past achievement and a broad (i.e., multiple domain) self-report measure of functional impairment. Because many universities and colleges use GPA as a metric to judge the quality of applicants and their potential for future academic success, as well as the academic progress of current students, pathways leading from prior GPA to future impairment are a highly relevant area of study. We hypothesized that consistent with the Safren et al. model, negative cognitions and symptoms of anxiety and depression would act as serial mediators of the association between prior achievement (i.e., past-year GPA) and future impairment, above and beyond symptoms of ADHD.
Method
Participants
Participants were undergraduate students enrolled in a large public university in Virginia. For the current study, 139 students initially expressed interest in the study and completed the phone screen. In all, 101 families were eligible based on the phone screen, 94 completed the inclusion/exclusion evaluation, and 68 met full study-inclusion criteria and were enrolled. We limited the sample for the current study to full-time students (those taking ≥ 9 credit hr; N = 62), and 59 of these participants completed all the primary study measures examined in this study. In comparing the demographic characteristics of those participants for whom full data were available with those without complete data, no differences were found for age, gender, ethnicity, year in school, parent education level, family income, and ADHD medication status (ps > .05). Similarly, no differences were found for ADHD subtype, symptoms of ADHD, anxiety, depression, negative self-concept, GPA, or functional impairment ratings (ps > .05).
The final sample of 59 participants included in this study ranged in age from 17 to 30 years (M = 19.90, SD = 2.75 years), and 32 (54.2%) were male. Forty-two participants (71.2%) self-identified as Caucasian; the remaining were six African American (10.2%), six Hispanic (10.2%), and five multiracial (8.5%). Twenty-seven participants (45.7%) were in their first year of college, with remaining participants in their second (n = 13; 22.0%), third (n = 11; 18.6%), or fourth (n = 8; 13.6%) year. Based on procedures described below, 30 participants (50.8%) were diagnosed with Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) ADHD, Predominantly Inattentive presentation, and 29 (49.2%) were diagnosed with ADHD, Combined Presentation. Thirty-five participants (59.3%) were taking medication for ADHD, and four (6.8%) were taking medications for other psychological disorders. Fifty participants (84.7%) had received an ADHD diagnosis prior to the study.
Procedure
The study was approved by the university Institutional Review Board (IRB), and student participants signed informed consent and their parents/guardians provided verbal consent. The inclusionary criteria included attendance at the university where the research was being conducted and meeting full DSM-IV diagnostic criteria for ADHD, Predominantly Inattentive Type (ADHD-I) or ADHD, Combined Type (ADHD-C). Diagnosis was determined through separate administration of Part 1 and Part 2 of the Conners’ Adult ADHD Diagnostic Interview for the DSM-IV (CAADID; Epstein, Johnson, & Conners, 2000; Epstein & Kollins, 2006) to students and their parent/guardian. The CAADID assesses both current and childhood symptoms and impairment, as well as age of onset and pervasiveness of symptoms across time. Part 1 of the interview provides a detailed history, and Part 2 is the ADHD diagnostic interview.
Strict diagnostic inclusion criteria were adhered to in this study. Specifically, parents/guardians had to endorse at least six symptoms in an ADHD domain on the CAADID as present and impairing during childhood for a student to be included. Furthermore, the student and their parents/guardians had to endorse a total of six symptoms in a domain as currently present and impairing on the CAADID. For documentation of current ADHD symptoms, we allowed parent interview data to be supplemented with student self-report and vice versa. However, both the parent and student had to endorse a minimum of four symptoms in a domain as currently present and impairing for supplementation to occur. Flyers describing the study were included in the orientation packets of all incoming freshman, e-mailed to all students currently receiving ADHD accommodations, and posted in the Disability Services Office, at Student Health, and in all university dorms. The flyers stated that students with difficulties with attention and concentration and/or students with a diagnosis of ADHD were eligible to receive a free diagnostic evaluation. Students completed baseline measures at the start of the school year (T1) and follow-up measures at the end of the school year (T2; 9 months post-baseline) and received a nominal monetary reimbursement for their time and effort completing the ratings at both time points.
Measures
Negative self-concept
The Sense of Inadequacy Scale from the Behavior Assessment System for Children–Second Edition: Self-Report of Personality–College Version (BASC-2: SRP-College Version; Reynolds & Kamphaus, 2004) was used to measure negative self-concept. This measure, which was normed on a sample of 706 college students between 18 and 25 years of age, is designed to assess the frequency or intensity with which an individual engages in a range of internal thoughts and external behaviors. The BASC-2: SRP-College Version consists of 185 total items, which are rated on either a 4-point rating scale (1 = never; 2 = sometimes; 3 = often; 4 = almost always) or as true/false. Completion of the measure results in the formulation of 16 individual scales for which t scores are calculated. The t scores between 60 and 69 are considered to be in the borderline clinical range, and t scores of 70 or higher are considered to be clinically significant. The Sense of Inadequacy Scale examines the endorsement of attitudes or beliefs reflecting a general difficulty or inability to succeed or to achieve. Higher scores reflect more negative perceptions of individual abilities, and, thus, a more negative self-concept. The scale is made up of nine items. Examples of items include “Even when I try hard, I fail,” “I fail at things,” and “I never quite reach my goal.” Scores on this subscale from T1 were used in the mediation models. Five-week test–retest reliability for the Sense of Inadequacy Scale is strong (ρ = .73, Intraclass Correlation Coefficent [ICC] = .84; Nowinski, Furlong, Rahban, & Smith, 2008), and there is evidence for both convergent and discriminant validity (Nowinski et al., 2008). Internal consistency was acceptable (α = .73).
Anxiety and depression
To measure symptoms of anxiety, the Anxiety Scale of the BASC-2: SRP-College Version (Reynolds & Kamphaus, 2004) was used. The Anxiety Scale examines endorsements of frequent fears or worries, including specific (e.g., tests) and nonspecific (e.g., the future) events. Depression was measured using the Depression Scale of the BASC-2: SRP-College Version (Reynolds & Kamphaus, 2004). The Depression Scale measures endorsements of thoughts related to depressive symptoms, such as feelings of anhedonia and hopelessness. Scores on the Anxiety and Depression scales collected at T1 and T2 were used in the mediation model. As with the Sense of Inadequacy Scale, t scores on the Anxiety and Depression scales between 60 and 69 are considered to be in the borderline clinical range, and t scores of 70 or higher are considered to be clinically significant. There is evidence for the 5-week test–retest reliability of the Anxiety Scale (ρ = .84, ICC = .93) and the Depression Scale (ρ = .65, ICC = .62; Nowinski et al., 2008). Furthermore, there is evidence for convergent validity of the BASC Anxiety Scale (Schwanz, Palm, Thackray, & Hill-Chapman, 2009) and the BASC Depression Scale (Nowinski et al., 2008) with commonly used measures of anxiety and depression such as the State-Trait Anxiety Inventory (STAI; Spielberger & Gorsuch, 1983) and the Adult Self-Report (Achenbach & Rescorla, 2003). Internal consistency for the Depression and Anxiety scales in this sample was good (α = .81 and α = .85, respectively).
Overall functional impairment
Participants completed the Barkley Functional Impairment Scale (BFIS; Barkley, 2011), which assesses psychosocial impairment in 15 domains of major life activities, at T1 and at T2. The BFIS is a norm-referenced measure (N > 1,200) with high internal consistency (α = .97; Barkley, 2011) and 2-week test–retest reliabilities range from .47 to .72, according to domain (Barkley, 2011). Participants rated impairment in each major life activity on a 10-point Likert-type scale ranging from 0 (not impaired) to 9 (severely impaired). A total impairment score (sum of all 15 domains of functioning) was examined in the present study (α = .96). Total impairment scores may range from 0 to 135. The mean impairment score in this sample was 50.14 (SD = 23.32) at T1 and 47.58 (SD = 24.58) at T2, respectively. Scores on this measure collected at T2 were used as an outcome measure in the two mediation models, and T1 was controlled as a covariate.
Prior year GPA
Participants’ GPA was used as a measure of academic achievement and was coded based on a system developed and refined in past work with adolescents and young adults (Molina et al., 2009). Prior GPA was evaluated at baseline. For freshmen participants, GPA from their senior year of high school was used in the analyses. Similarly, for sophomores, juniors, and seniors, GPA from the prior academic year was included in the analyses. For all students, A = 4.0, B = 3.0, C = 2.0, D = 1.0, and F = 0.
Analytic Plan
The primary aim of this study was to test the indirect and direct pathways between a history of past underachievement and later functional impairment. Accordingly, serial mediation was used, as it assumes “a causal chain linking the mediators, with a specified direction of causal flow” (Hayes, 2012, p. 14). For example, prior academic underachievement may contribute to a more negative self-concept, which leads to increases in symptoms of anxiety or depression, which ultimately contributes to increased functional impairment (i.e., prior GPA → T1 negative self-concept → T1 depressive/anxious symptoms → T2 depressive/anxious symptoms → T2 functional impairment). Separate serial mediation models were run for depression and anxiety symptoms as mediators. Baseline functional impairment (T1) and change in ADHD symptoms from T1 to T2 were controlled for as covariates in both models. Process modeling strategies, as recommended by Hayes and Preacher (2010) were used to assess the mediation pathway. The PROCESS macro for SPSS (Hayes, 2012) allows for testing of serial mediation models including both direct and indirect effects. For smaller samples, bootstrapping tests of mediation are recommended over other tests of mediation such as Baron and Kenny (1986), because bias-corrected bootstrapped estimates of the confidence intervals (CIs) for indirect effects do not assume normality of the distribution of sampled indirect effects (Preacher, Rucker, & Hayes, 2007). For this study, 95% CIs are considered significant if they do not include zero and 10,000 replications (bootstrapping tests) were used.
Results
Participant age, gender, race, employment status, living status, and current and childhood treatments including medication were not significantly correlated with functional impairment outcome and are not considered further. Correlations between all predictor, mediator, and outcome variables are displayed in Table 1. T1 functional impairment, ADHD symptoms, prior year GPA, negative self-concept, and symptoms of depression and anxiety were each significantly associated with T2 overall impairment.
Means, Standard Deviations, and Intercorrelations of Predictor, Mediator, and Outcome Variables.
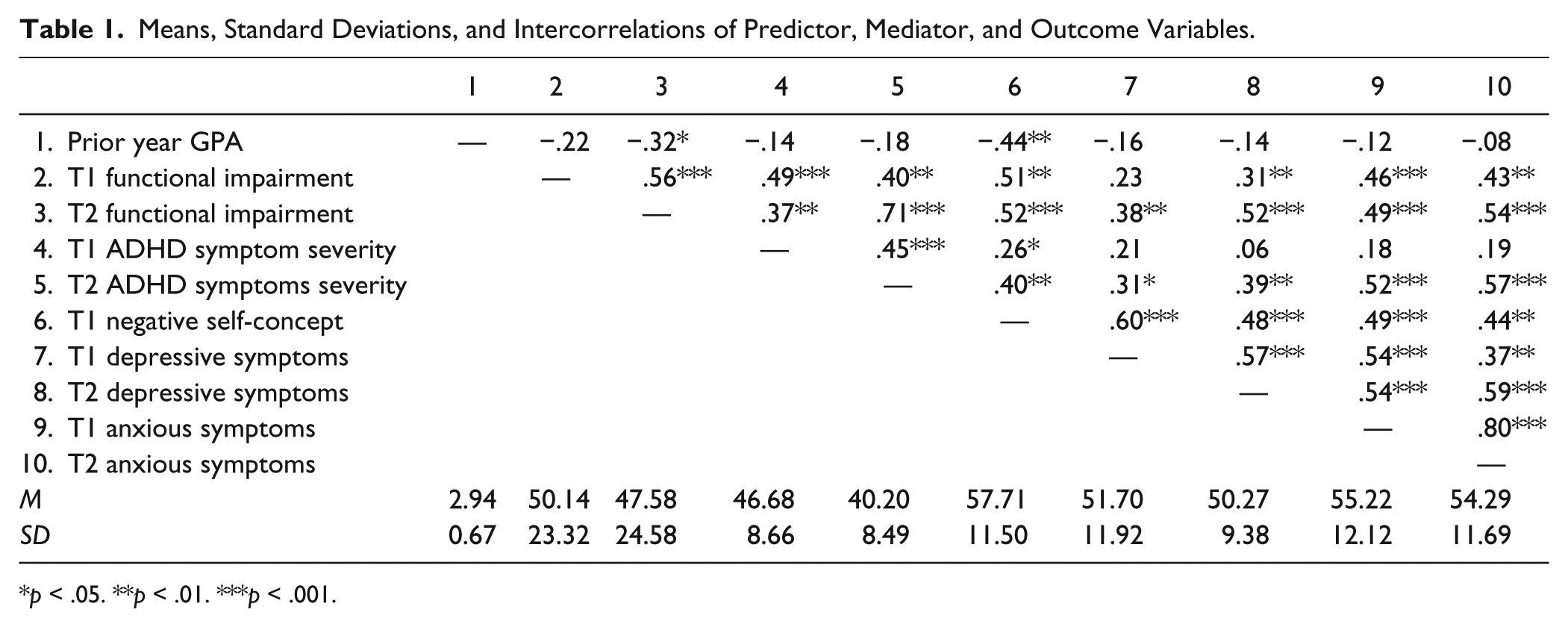
p < .05. **p < .01. ***p < .001.
Serial Mediation Analyses
Two separate mediation analyses were conducted to test the serial mediators for GPA predicting later functional impairment (see Figures 1 and 2). Anxiety and Depression at T1 and T2 were included as the mediators after T1 negative self-concept.
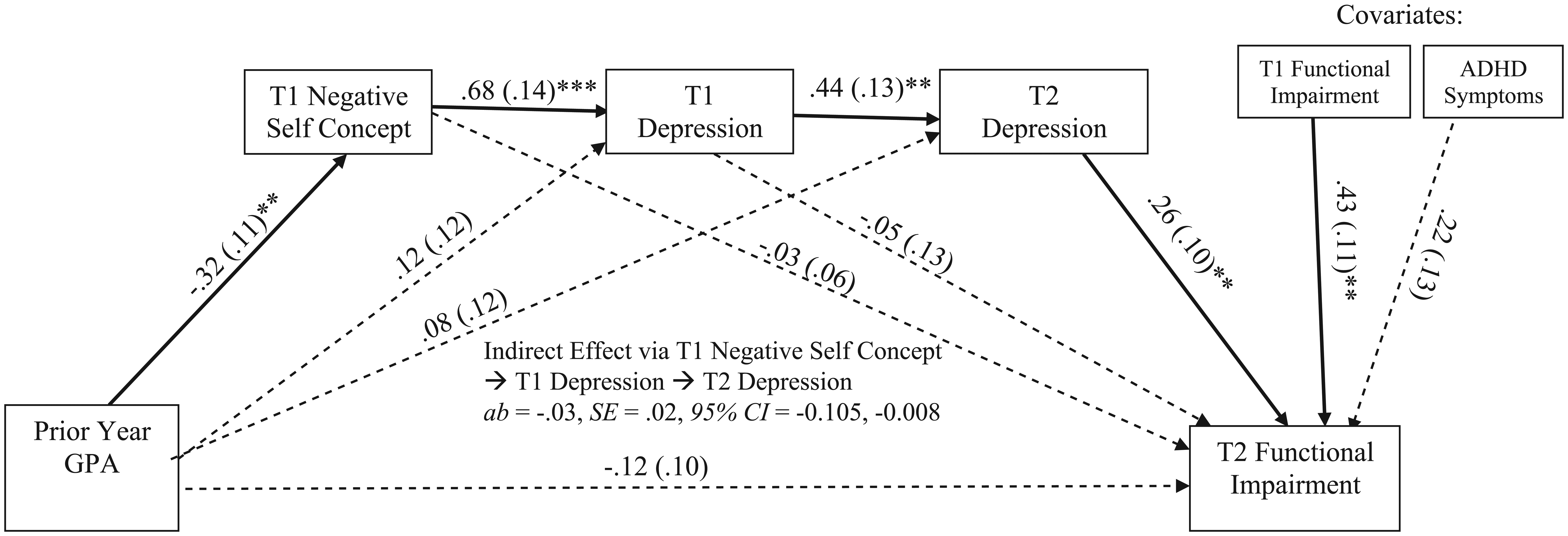
Indirect effects model of prior year GPA predicting T2 functional impairment via T1 negative self-concept leading to T1 depression to T2 depression.
The first model tested whether negative self-concept and depression over time (entered as serial mediators) mediates the relationship between prior year GPA and later functional impairment (T2), after controlling for baseline functional impairment (T1) and ADHD symptom severity as covariates in the model. Specifically, this model tested the following causal chain: prior year GPA → negative self-concept (T1) → depression (T1) → depression (T2) → functional impairment (T2). A total effect from prior year GPA to T2 functional impairment was not present (c = −.12, SE = .10, p = .26), primarily due to a strong and significant association between T1 and T2 functional impairment (b = .56, SE = .10, p < .001), and current mediation guidelines are clear that an indirect effect may exist in the absence of a direct effect (see Hayes, 2012; Preacher et al., 2007). In line with this possibility, and as shown in Figure 1, the total indirect effects of the serial mediators were significant (p < .001). Examination of the specific indirect effects shows that there was a significant indirect effect of the serial mediators, ab = −.03, SE = .02, 95% bootstrap CI = [−.105, −.008] (see Figure 1) indicating that negative self-concept and depression from T1 to T2 serve as serial mediators of the effect of prior year GPA on later functional impairment (T2). An examination of the specific path coefficients demonstrated that prior year GPA was negatively associated with negative self-concept (T1), which positively predicted T1 depression, which in turn positively predicted T2 depression, and depression (T2) was positively associated with functional impairment (T2). No mediation was found for negative self-concept (T1) alone in that the indirect effect of prior GPA → negative self-concept (T1) → functional impairment (T2) was nonsignificant, ab = −.02, SE = .04, 95% CI = [−.120, .060], but only significant when considered in the indirect path with T1 depression → T1 depression as serial mediators. Similarly, no mediation was found for depression (T1) alone in that the indirect effects of prior GPA → depression (T1) → functional impairment (T2) was nonsignificant, ab = −.01, SE = .03, 95% CI = [−.022, .106], as well as the indirect effects of prior GPA → negative self-concept (T1) → depression (T1) → functional impairment (T2) was nonsignificant, ab = −.01, SE = .04, 95% CI = [−.109, .042].
The second model tested whether negative self-concept and anxiety over time (entered as serial mediators) mediates the relationship between prior year GPA and later functional impairment (T2), after controlling for baseline functional impairment (T1) and change in ADHD symptom severity as covariates in the model. Specifically, this model tested the following causal chain: prior year GPA → negative self-concept (T1) → anxiety (T1) → anxiety (T2) → functional impairment (T2). As depicted in Figure 3, although prior GPA demonstrated an effect to negative self-concept (T1) that predicted anxiety (T1) and this predicted later anxiety (T2), only a marginally significant effect was present from anxiety (T2) to functional impairment (T2), b = .23, SE = .17, p = .11. Furthermore, examination of the specific indirect effects shows that there was not a significant indirect effect of the serial mediators, ab = −.02, SE = .03, CI = [−.120, .002] (see Figure 2) indicating that negative self-concept and anxiety over time do not serve as serial mediators of the effect of prior year GPA on later functional impairment (T2), unlike the depression model.
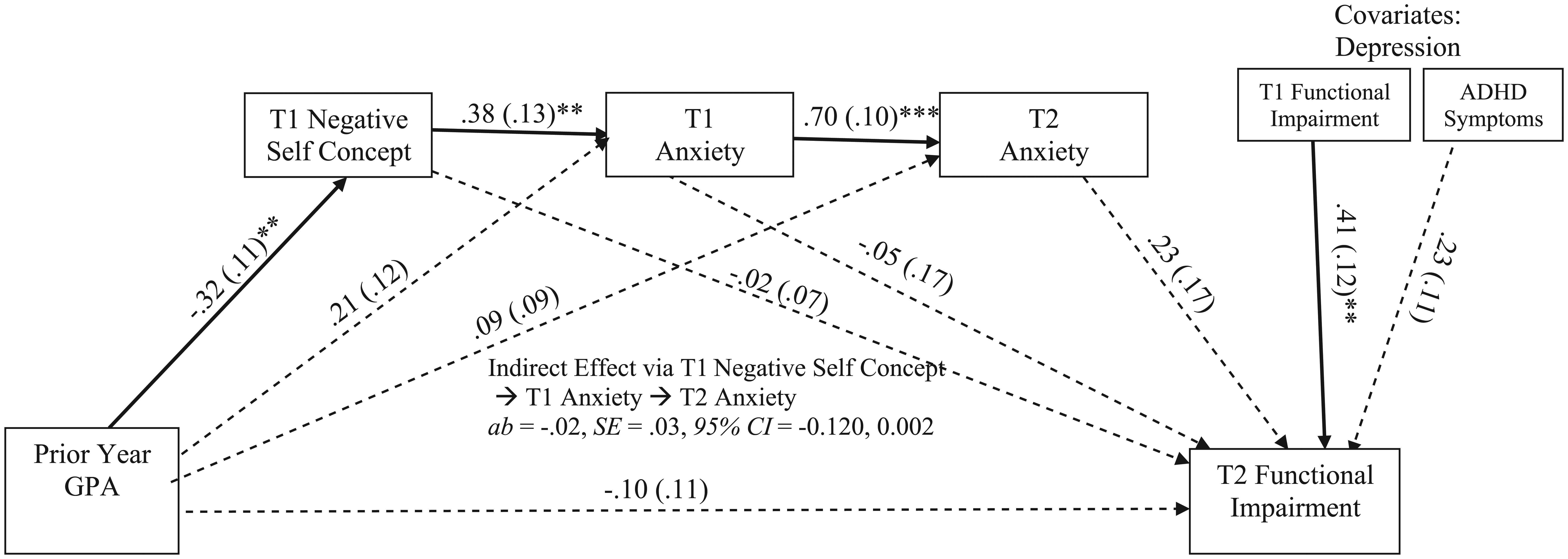
Indirect effects model of prior year GPA predicting T2 functional impairment via T1 negative self-concept to T1 anxiety to T2 anxiety.
Discussion
The purpose of this study was to longitudinally evaluate the pathways outlined by the cognitive-behavioral model of adult ADHD (Safren et al., 2004) in a sample of college students with ADHD. The primary aim was to determine whether negative self-concept and associated changes in symptoms of anxiety and depression longitudinally mediated the association between prior academic achievement and later levels of impairment. Overall, the results of this study provide support for the validity of the cognitive-behavioral model of adult ADHD. Specifically, in this sample of college students with ADHD, negative self-concept and symptoms of depression fully mediated the association between prior GPA and self-report of overall functional impairment more than a year later. Although not statistically significant, the magnitude of the association between anxiety and functioning was similar to that of depression, and the lack of statistical significance may have been associated with sample size and power to detect effects. Notably, as outlined in the cognitive-behavioral model of ADHD (see Figure 1), prior GPA was not directly associated with symptoms of depression but was significantly associated with self-concept, which in turn led to depressive symptoms. In terms of clinical implications, these finding suggest that negative self-concept is an important precursor to depressive symptoms in emerging adults with ADHD and should be assessed along with depressive symptoms. Furthermore, given that the association between depression and impairment held even when controlling for changes in ADHD symptoms, it seems likely that interventions for college students with ADHD will need to include cognitive strategies to counter maladaptive thinking patterns.
It is important to note that the measure of impairment used in this study taps difficulties with multiple areas of life, such as daily responsibilities, relationships with friends and family, maintaining physical health, academic functioning, and driving. As noted in the introduction, previous studies examining the impact of depression in ADHD samples have focused on depression-specific outcomes such as increased suicidal ideation. Although such measures are undoubtedly meaningful, it is also critical to consider functioning more broadly. These findings indicate that depressive symptoms in college students with ADHD may affect multiple distinct aspects of functioning. Indeed, symptoms of depression predicted overall functioning, whereas there was not a significant direct path from prior year GPA to overall functioning. These findings are congruent with past research showing that the emotional and social functioning of college students is more predictive of attrition than is academic functioning (Gerdes & Mallinckrodt, 1994).
It is important to acknowledge that emerging adults with ADHD who attend college are a unique group, by virtue of the fact that they have functioned at a high-enough level in high school to be accepted by a college or university. However, although they may be functioning relatively well compared with young adults with ADHD who are not attending college, they are certainly not functioning as well as their non-diagnosed peers. For instance, in the present sample, 70% of participants had received a D or an F in a core class during the second academic semester (T2). In addition, 54% endorsed clinical levels of anxiety or depression symptoms on the BASC-2, suggesting that many might meet criteria for an internalizing disorder. Finally, although the mean overall impairment score on the BFIS suggests minimal impairment (M = 50.14, SD = 23.32 on a scale from 0 to 135), a more detailed examination of individual domain scores (which range from 0 to 9) reveals that participants reported significant impairment in multiple domains of functioning. For example, the mean impairment score was 6.11 (SD = 2.49) in the Educational Activities domain and 5.68 (SD = 2.52) on the Organization of Daily Responsibilities domain, respectively. Accordingly, although college students with ADHD are clearly a unique group, there is evidence of impairment in the sample in multiple domains of functioning.
Clinical Implications and Future Directions
These findings have several potential implications for ADHD interventions focused on emerging adults and college students. Adolescents with ADHD are at risk for developing negative self-concepts (Major et al., 2013), and the findings from this study link a negative self-concept to the development of symptoms of anxiety and depression. Evidence-based treatments commonly used to treat ADHD in childhood (e.g., pharmacological interventions, behavioral parent training, school interventions) do not directly target either comorbid internalizing symptoms or negative self-concepts. Furthermore, CBT intervention efforts with younger children and adolescents that have focused mostly on changing maladaptive cognitions have largely been ineffective in improving both ADHD symptoms and impairment (Antshel & Olszewski, 2014). In contrast, there is accumulating evidence for the effectiveness of CBT for adults (Knouse & Safren, 2010) and college students (Anastopoulos & King, 2015) with ADHD. This provides evidence that targeting maladaptive cognitions and associated symptoms of anxiety and depression in individuals with ADHD is important, but several important unanswered questions remain.
First, it is currently unclear when in development failure experiences begin to have a detrimental impact on the self-concepts of adolescents with ADHD and when a negative self-concept spills into clinical symptoms of depression and anxiety. Longitudinal studies tracking the development of self-concept in ADHD could inform when cognitive strategies might be most usefully incorporated into ADHD interventions. One possibility is that negative self-concepts do not develop until later adolescence because a significant portion of children with ADHD exhibit a positive illusory bias (PIB) and may not be aware of their deficits or that their performance is worse than their peers (Hoza, Pelham, Dobbs, Owens, & Pillow, 2002; Owens, Goldfine, Evangelista, Hoza, & Kaiser, 2007). Alternatively, it may be that prior to adolescence, youth with ADHD have not yet experienced “enough” failure experiences and underachievement to have developed a pervasive negative self-concept. As failure experiences accumulate, there may be a “tipping point” in adolescence when self-concept suffers, and the path to the development of symptoms of anxiety and depression is initiated. Furthermore, it may be the case that this tipping point occurs later in development for some individuals, with the effects of this shift observed first during emerging adulthood.
An alternate theory may be that a PIB does extend into adulthood, but perhaps exists only in limited areas. Research on PIB in adults has demonstrated that adults with ADHD overestimate their competence with regard to driving abilities (Knouse, Bagwell, Barkley, & Murphy, 2005); however, there is no other compelling evidence that suggests that adults with ADHD overestimate their academic skills or functioning broadly. In fact, there is evidence that adults with ADHD rate their overall impairment levels significantly higher (worse) than the ratings of their impairment provided by spouses or close friends (Barkley, Knouse, & Murphy, 2011). Thus, it seems more likely that adults with ADHD are more cognizant of their own difficulties than children or adolescents with ADHD.
Second, it is unknown whether the development of comorbid symptoms of anxiety and depression can be prevented or minimized by including cognitive strategies into behavioral interventions implemented during adolescence. Most CBT research with children and adolescents with ADHD has focused on short-term outcomes, and future studies could be designed to assess for long-term preventive effects. Furthermore, there has been almost no intervention research focused on high school students with ADHD (see Evans, Langberg, Egan, & Molitor, 2014, for an exception), and it seems likely that self-concept and negative thoughts would increase in salience during this late adolescent period. Regardless, it seems likely that a purely behavioral approach would not be successful in a college student with ADHD population, given the high rates of comorbid depression and anxiety. Specifically, college students with ADHD and comorbid internalizing symptoms would likely struggle with apathy and lack of motivation to implement new behavioral strategies.
Specific to the Safren et al. model, the findings from this study have the potential to be extended by evaluating the remaining pathways described by the model. For instance, the model suggests that negative self-concept and symptoms of anxiety and depression contribute to impairment by interfering with the use of compensatory strategies (e.g., organizational techniques, prioritizing) used to manage ADHD symptoms. This was not evaluated in the current study, and future research in college samples might use a measure such as the Learning and Study Strategies Inventory (LASSI; Weinstein & Palmer, 2002) to evaluate the impact of depression and anxiety on academic skills and strategies.
Limitations
There are several limitations to the current study that should be noted. First, the sample size in the current study was moderate and replication of the findings in other college samples is needed. Second, the measures utilized in this study were almost exclusively self-report, with the exception of prior year GPA. Although this is a common assessment strategy for college students and adults with ADHD, a multi-informant measurement is considered optimal, particularly for the assessment of impairment (Sibley et al., 2012). Third, it could be argued that past-year GPA too narrowly measures past failure/underachievement as conceptualized by the Safren et al. (2004) model. Future research could improve on this by utilizing additional measures of past academic success or achievement such as high school ranking, college entrance exam scores, or number of failing grades experienced per year. In addition, it may be useful to gather measures related to student’s perceptions of what constitutes underachievement or failure, because these perceptions may not always correspond exactly with external assessment of academic success such as grades, class rankings, or exam scores. Another limitation is the college student sample used in this study, which inherently limits the generalizability of the findings. The degree to which the results will generalize to a population of young adults with ADHD who are not attending college is unknown. Finally, no control group was collected, and it is important to acknowledge that that CBT model may not be unique to college students with ADHD.
Conclusion
Overall, the findings from this study support the pathways outlined by the Safren et al. (2004) cognitive-behavioral model of impairment for adults with ADHD. The development of a negative self-concept leading to depressive symptoms seems to be important in explaining the recurring cycle of impairment witnessed in individuals with ADHD, above and beyond the trajectory of ADHD symptoms. The findings from this study suggest that interventions for college students with ADHD will need to include both cognitive and behavioral strategies (e.g., Anastopoulos & King, 2015) and that behavioral only approaches are unlikely to be successful.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.