
Abstract
Adolescents with ADHD show symptoms of inattention, hyperactivity, and impulsivity (American Psychiatric Association [APA], 2013). However, the disorder is frequently described as a highly heterogeneous condition (e.g., Wåhlstedt, Thorell, & Bohlin, 2009). Two sources contribute to this heterogeneity: (a) between-person (i.e., interindividual) differences and (b) within-person (i.e., intraindividual) fluctuations in symptoms. Differences between persons have been investigated with regard to ADHD symptom reports (Wåhlstedt et al., 2009), underlying neuropsychological impairments (Sonuga-Barke, Bitsakou, & Thompson, 2010), and comorbid difficulties (Taurines et al., 2010). Differences within persons have been mainly studied in the laboratory as moment-to-moment fluctuations over seconds and milliseconds in cognitive performance tests (Kofler et al., 2013) and, only recently, as observed fluctuations in symptom behavior (e.g., hyperactivity and noisiness) over the school day (Imeraj et al., 2016).
So far, however, descriptions of between-person differences in ADHD symptom expressions and analyses of their underlying structural organization (e.g., Toplak et al., 2012) are restricted to either retrospective or dispositional one-time symptom ratings that may possibly be confined by recall bias (Miller, Newcorn, & Halperin, 2009). Moreover, a paucity of research exists examining whether ADHD symptoms fluctuate within persons in natural environments from day to day, and how those symptoms are structured within individuals over time.
Within-Person Fluctuations of ADHD Symptoms
The idea of short-term within-person fluctuations in ADHD symptoms in everyday life complements well-established research findings showing that some ADHD symptoms undergo substantial within-person changes in a time frame of years and decades (e.g., Spencer, Biederman, & Mick, 2007). For example, for most individuals, overt signs of hyperactivity remit from childhood into adulthood and may appear as more subjective states such as mental restlessness, jitteriness, or impatience (APA, 2013). Following this developmental perspective, we additionally consider fluctuations in symptom severity that arise in shorter time frames, that is, from day to day. In this view, ADHD symptoms can be regarded as relatively stable, slowly changing individual differences characteristics with additional state-like components that fluctuate in shorter time frames.
Current theoretical conceptions of ADHD such as the State Regulation Model and Multiple Pathway Theories already incorporate the idea of within-person fluctuations in inattention, hyperactivity, and impulsivity in everyday life, although supporting empirical evidence from natural environments is lacking so far. The State Regulation Model considers ADHD symptoms to arise from deficits in keeping optimal states of activation (van der Meere, 2005). Building on Sanders’ cognitive-energetic theory (Sanders, 1983), it suggests that individuals’ activation levels are situation-dependent: Activation increases with high stimulus presentation rates and decreases with low stimulus presentation rates. To counteract overactivation and underactivation during task execution and thus reach optimal performance levels, individuals need to allocate extra effort. Correspondingly, performance deficits in cognitive tasks are strongest for individuals with ADHD when stimulus rates are fast (e.g., Sonuga-Barke, 2003) and slow (e.g., Scheres, Oosterlaan, & Sergeant, 2001). Accordingly, the State Regulation Model would also predict substantial within-person fluctuations in ADHD symptoms in everyday life: Higher symptom levels may be regarded (a) as self-stimulation (Johnson, Wiersema, & Kuntsi, 2009) when activation during the day is low and (b) as behavioral indicators of overactivation when activation during the day is high.
Multiple Pathway Theories on the other hand assume that several developmental influences converge upon ADHD symptoms. Today, the most influential multiple pathway theory is the Triple-Pathway Model (Sonuga-Barke et al., 2010). It postulates that distinct timing, inhibition, and delay deficits give rise to heterogeneous expressions of ADHD symptoms. This model also implies that individuals’ ADHD symptoms in everyday life are not stable over shorter time periods (e.g., hours and days) but fluctuate within individuals over time: Impulsivity is thought to evolve in situations that incorporate high demands to inhibit one’s behavior. Hyperactivity and inattention may represent behavioral attempts to attenuate the negative emotional experiences of delay where delay is unavoidable.
Thus, in sum, both theories would predict within-person fluctuations in ADHD symptoms in addition to between-person differences in everyday life depending on current stimulation level, inhibitory demands of the situation, and experiences of delay. Nevertheless, despite robust evidence from laboratory experiments supporting substantial within-person fluctuations from moment to moment in cognitive correlates of ADHD symptoms (Kofler et al., 2013) and emerging evidence for observable within-person fluctuations in symptom behavior over the school day (Imeraj et al., 2016), no empirical study has yet tested whether adolescents experience day-to-day fluctuations in ADHD symptoms in everyday life.
The Structure of ADHD Symptoms: A Between- and Within-Person Perspective
Numerous studies have investigated so far whether between-person differences in symptoms can parsimoniously be described by latent symptom factors, drawing on one-time ratings of retrospective symptom experiences (e.g., during the last week, month, year, or during childhood) or dispositional symptom experiences (i.e., symptom presence in general). However, assuming that ADHD symptoms indeed fluctuate within individuals from day to day, one-time ratings of individuals’ experiences targeting the between-person level are likely confounded by within-person fluctuations. That is, ratings may strongly be influenced by current experiences at the time when individuals provide their ratings (Brose, Lindenberger, & Schmiedek, 2013). Therefore, ADHD symptom structures that have been confirmed in prior studies based on one-time ratings likely represent a blend of structures underlying relatively stable between-person differences as well as within-person fluctuations. However, a blend of factor structures on the between- and within-person level does not necessarily inform about the structures on either of these levels as between- and within-person structures might differ from each other (cf. Leonhardt, Könen, Dirk, & Schmiedek, 2016; Molenaar, 2004). Nevertheless, factor analytic research based on one-time ratings serves as an adequate starting point for the endeavor to disentangle between- and within-person factor structures.
Several studies based on one-time ratings confirmed that correlated factor models with distinct yet correlated symptom factors show a better fit to the phenotypic representation of ADHD than a one-factor model with only a single symptom factor (e.g., Glutting, Youngstrom, & Watkins, 2005). Correlated factor models separate either two factors of (a) hyperactivity-impulsivity and (b) inattention corresponding to two symptom lists in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; APA, 2013), or three factors of (a) hyperactivity, (b) impulsivity, and (c) inattention corresponding to three symptom lists in the International Classification of Diseases (ICD-10; World Health Organization, 1993). The correlated two-factor model has often been favored because hyperactivity and impulsivity factors are highly correlated and the model fit improves only slightly when they are separated (cf. Ullebø, Breivik, Gillberg, Lundervold, & Posserud, 2012).
Only recently, an alternative factor analytic approach—bifactor models—has been applied to understand the structure of ADHD symptoms based on one-time ratings. Bifactor models hypothesize (a) a general factor accounting for the common variance shared by all symptoms, and (b) two or three specific factors that are independent (i.e., orthogonal) from the general ADHD factor accounting for unique separable variance of inattention, hyperactivity, and impulsivity over and above the general factor. In contrast to correlated factor models that suggest interrelated but conceptually independent symptom domains, bifactor models emphasize a single core construct that underlies all ADHD symptoms while pointing to specificities of symptom domains. Mainly, two arguments have been put forward as to why bifactor models may be a better account of the underlying symptom structure: First, developmental studies reveal that the disorder frequently persists into adulthood. Nevertheless, symptom manifestations and subtype diagnoses may change with age (e.g., Willcutt et al., 2012). This suggests a generic component, which lies at the core of the disorder and is relatively stable over time, along with additional specific manifestations that may fluctuate over the life span (Martel, von Eye, & Nigg, 2012). Consistent with this view, the DSM-5 defines ADHD as a single diagnostic entity with predominantly inattentive, hyperactive-impulsive, or combined symptom presentations reflecting the current diagnostic status. Correlated factor models assume interrelated but conceptually independent symptom domains. Thus, unlike bifactor models, correlated factor models do not possess explanatory value for a generic component due to their lack of a “common core”. Second, quantitative genetic research (i.e., twin and adoption studies) point to sets of genes that influence all ADHD symptoms and other sets of genes that specifically influence one of the symptom domains (e.g., Greven, Asherson, Rijsdijk, & Plomin, 2011). A bifactor model that represents a general ADHD symptom factor as well as independent specific symptom factors may be especially well suited to account for these findings.
Indeed, during the last years, studies comparing the more traditional correlated factor models with bifactor models have reported better or at least comparable model fit for bifactor models (Willoughby, Blanton, & Family Life Project Investigators, 2015) for one-time symptom ratings across age groups (i.e., childhood to adulthood), informants (i.e., self, parent, teacher, clinicians), measures (i.e., rating scales, interviews), and populations (i.e., clinical samples, community samples; e.g., Gibbins, Toplak, Flora, Weiss, & Tannock, 2012; Gomez, Vance, & Gomez, 2018; Martel et al., 2012; Toplak et al., 2012; Ullebø et al., 2012). An open question is whether two separate (Gibbins et al., 2012; Morin, Tran, & Caci, 2016) or only one common specific factor (Caci, Morin, & Tran, 2016; Toplak et al., 2012) underlies hyperactivity and impulsivity symptoms. Because impulsivity is usually measured with fewer items, however, they may provide limited power to detect a separate specific factor for impulsivity separately from hyperactivity. Moreover, recent studies found support for incomplete bifactor models that represent not all ADHD symptom domains with specific symptom factors (Ullebø et al., 2012).
Today, intensive longitudinal designs with daily ratings of ADHD symptoms are needed to simultaneously examine both within- and between-person symptom factor structures by applying multilevel factor analyses that disaggregate within- and between-person variance. Structural accounts of within-person fluctuations would target how experiences of ADHD symptoms “travel together or covary across time” (Brose & Ram, 2012, p. 460). Thus, within-person factor models help to answer questions such as the following: Are occasions when adolescents report more difficulty sitting still co-occuring with occasions when adolescents have more difficulty engaging in activities quietly? Such associations within persons would point to an underlying hyperactivity factor. This factor would account for the covariance in hyperactivity ratings within persons that may or may not be separable from the common covariance in impulsivity and inattention ratings within persons. The average within-person factor structure from multilevel factor analyses reflects the covariance in self-reported ADHD symptoms within persons, aggregated across repeated occasions and individuals. Last, but not least, symptom ratings in intensive longitudinal studies have the advantage to yield more precise estimates of factor structures on the between-person level, compared with traditional one-time ratings, because they are less affected by retrospective bias in addition to allowing us to separate within-person and between-person variances and factor structures (Brose et al., 2013).
The Present Study
We applied an intensive longitudinal design with self-ratings of adolescents’ ADHD symptoms on eight consecutive days. Adolescents with and without ADHD diagnosis participated in the study to adequately capture the full symptom range. A widely used German ADHD self-report scale (Döpfner, Görtz-Dorten, Lehmkuhl, Breuer, & Goletz, 2008) was adapted to assess symptom presence for every day of the study.
We hypothesized that adolescents’ self-reported ADHD symptoms fluctuate substantially within persons from day to day. Furthermore, we examined the factor structure of daily ADHD symptoms disaggregating within- and between-person variance by means of multilevel confirmatory factor analyses (CFA). For both the within- and between-person level, we evaluated whether a bifactor model with a general symptom factor and specific domain factors provides a better, or equally good, account of the underlying symptom structure of daily self-reports than more traditional one-factor models and correlated factor models. Thus, the multilevel models investigated here correspond to the models targeted in previous studies drawing on one-time symptom ratings. The comparison of models, however, is exploratory in nature as this is the first study undertaking multilevel factor analyses to study ADHD symptoms in everyday life.
Method
Participants
The study included 166 adolescents (90 boys; age: M = 13.15 years, SD = 1.93). Forty-seven adolescents diagnosed with ADHD (42 boys; age: M = 14.29 years, SD = 2.30) were recruited at a special ADHD school. This school has a specific approach to meet the needs of adolescents with ADHD. Adolescents recruited at this school had been diagnosed with ADHD according to ICD-10 or DSM-IV criteria and were tested for cognitive abilities that are required as a prerequisite prior to school enrollment. Among them, 36 participants were on medication for ADHD and continued their medication regimen during the study. The other 119 participants (48 boys; age: M = 12.69 years, SD = 1.55) were recruited at two regular schools. Two of these adolescents had received an ADHD diagnosis according to parental reports in the background questionnaire. All participants gave written informed consent to participate and received €10 for their participation. Detailed sample characteristics are depicted in Table 1.
Sample Background Characteristics.
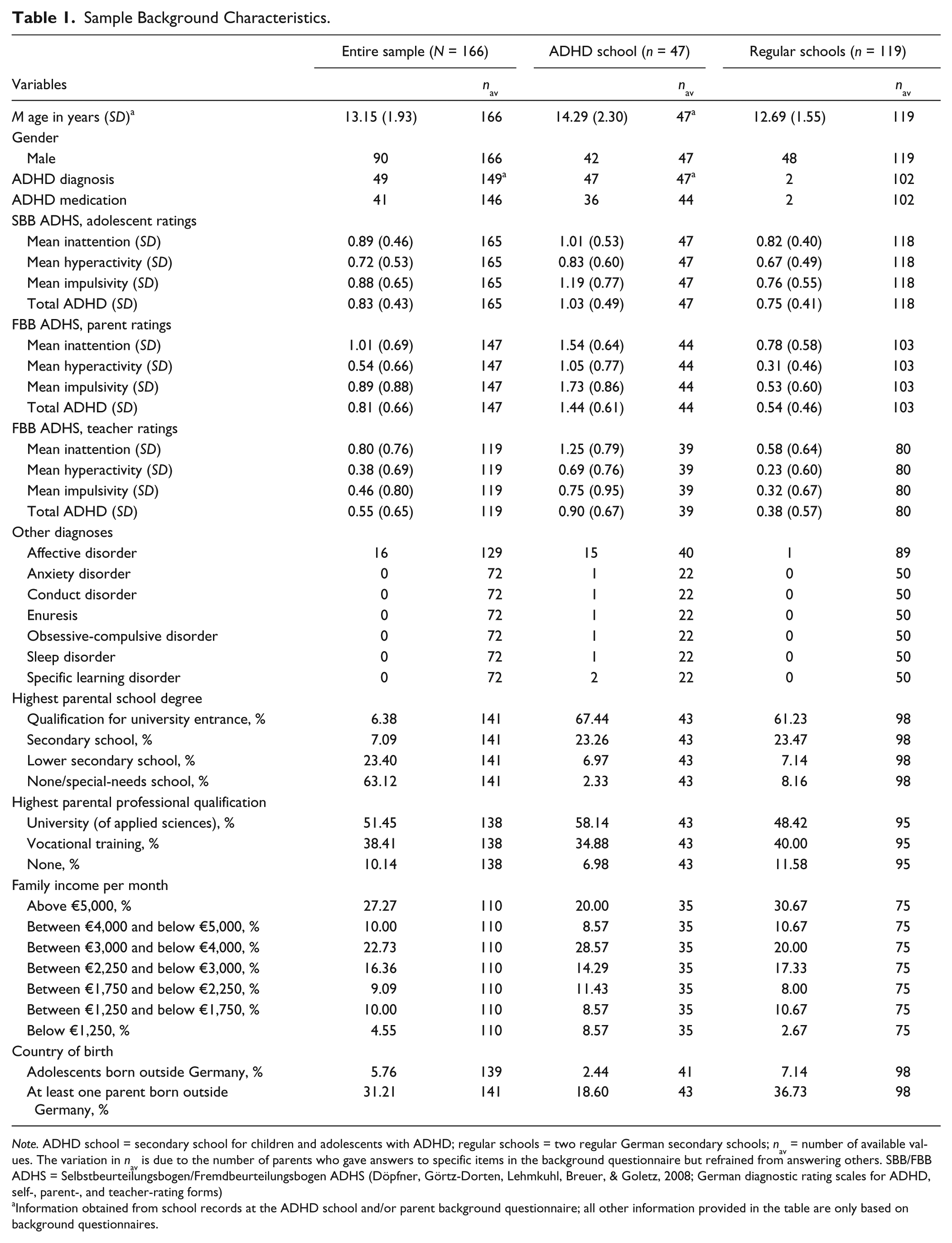
Note. ADHD school = secondary school for children and adolescents with ADHD; regular schools = two regular German secondary schools; nav = number of available values. The variation in nav is due to the number of parents who gave answers to specific items in the background questionnaire but refrained from answering others. SBB/FBB ADHS = Selbstbeurteilungsbogen/Fremdbeurteilungsbogen ADHS (Döpfner, Görtz-Dorten, Lehmkuhl, Breuer, & Goletz, 2008; German diagnostic rating scales for ADHD, self-, parent-, and teacher-rating forms)
Information obtained from school records at the ADHD school and/or parent background questionnaire; all other information provided in the table are only based on background questionnaires.
Procedure
This study was part of a larger project aiming to understand everyday experiences of adolescents, conducted at the Center for Research on Individual Development and Adaptive Education of Children at Risk (IDeA), Frankfurt, Germany. It had an intensive longitudinal design. Adolescents, their parents, and their teachers filled out background questionnaires on the first day of the study and adolescents reported daily ADHD symptoms over the phone in the evenings on eight consecutive days.
On the first study day, parents and teachers were handed out a 20-min background questionnaire and asked to hand it back filled out to the researchers the next day. Adolescents completed a 45-min background questionnaire in groups of 10 to 15 under the supervision of researchers. Adolescents also indicated a convenient time to take evening phone calls, preferably within 1 hr before bedtime. Accordingly, adolescents were called by researchers on the following eight consecutive days to answer evening diaries. In case adolescents could not be reached at the first attempt, researchers made follow-up calls until either a family member informed us the adolescents would not be available that evening or at the estimated bedtime. Overall, of a possible 1,328 daily rating occasions (166 participants × 8 study days), daily ADHD ratings from 1,264 rating occasions were obtained (95.2%). The study was approved by the local ethics committee.
Measures
General ADHD symptom status
In the background questionnaire, adolescents’ ADHD symptoms were assessed with a well-validated German ADHD symptom rating scale for adolescents, parents, and teachers (SBB/FBB ADHS; Döpfner et al., 2008). The measure is widely used in German-speaking countries and assesses the DSM-IV/ICD-10 symptoms for ADHD with 20 items (nine for inattention, seven for hyperactivity, four for impulsivity). Adolescents and their parents/teachers were asked to rate the presence of each symptom on a 4-point scale from 0 (not at all) to 3 (extremely).
In this study, the measure’s internal consistency was satisfactory to high across ratings of adolescents’ symptoms by adolescents, parents, and teachers. Cronbach’s α for the composite ADHD scale ranged from .85 to .96. For the inattention subscale, α ranged from .74 to .95. For the hyperactivity-impulsivity subscale, α ranged from .80 to .97, for hyperactivity from .73 to .95, and for impulsivity from .70 to .94.
Daily ADHD symptoms
Eleven items (six for inattention, three for hyperactivity, and two for impulsivity) of the original measure (Döpfner et al., 2008) were adapted for self-ratings of adolescents’ daily experiences of ADHD symptoms (e.g., I had difficulties paying attention to details today; I talked too much today). Adolescents indicated how much they had experienced each symptom that day on a 4-point rating scale ranging from 0 (not at all) to 3 (extremely). Multilevel reliability estimates (Geldhof, Preacher, & Zyphur, 2014) were computed for the entire scale and the subscales with between-person estimates (αb) referring to the reliability of individual differences in symptoms across the study period, and within-person estimates (αw) addressing the reliability of day-to-day symptom fluctuations. Reliability on the between/within-person level was .94/.66 (entire scale), .95/.59 (inattention), .87/.52 (hyperactivity-impulsivity), .90/.45 (hyperactivity), and .50/.40 (impulsivity). Please note that between-person reliability is by default higher because it is based on an aggregate of several days. The observed range of within-person reliabilities is in line with previously reported findings on adults (e.g., Tomko et al., 2014).
Data Analyses
Within-person fluctuations of daily ADHD symptoms
To assess whether adolescents’ self-reported ADHD symptoms fluctuated from day to day, we calculated the intraindividual standard deviation (ISD) and the intraclass correlation coefficient (ICC) for all symptoms. The ISD refers to each adolescent’s standard deviation in symptoms across the study days. The ICC quantifies the proportion of variability on the between-person level relative to the overall variability. Hence, small values indicate that between-person differences in symptom levels account for a small portion of the overall variability with the rest explained by within-person symptom fluctuations and residual error (Singer & Willett, 2003).
Factor structure of daily ADHD symptoms
To evaluate the factor structure of adolescents’ daily self-reported ADHD symptoms, we conducted two-level confirmatory factor analyses accounting for the multilevel structure of the diary data (i.e., repeated daily measures are nested within persons; Hox, 2010). To test whether a bifactor model with a general symptom factor and specific domain factors on both the between- and within-person level provides a better account of adolescents’ daily ADHD symptoms than more traditional factor models, the following models were estimated: Model A—a one-factor model, positing a single symptom domain underlying inattention, hyperactivity, and impulsivity (ADHD) on both levels; Model B—a correlated factor model with two factors of inattention (INA) and hyperactivity-impulsivity (HYP-IMP) on both levels; Model C—a correlated factor model with three factors of inattention (INA), hyperactivity (HYP), and impulsivity (IMP) on both levels; Model D—a bifactor model with a general factor (G ADHD) and two specific factors of inattention (S INA) and hyperactivity-impulsivity (S HYP-IMP) on both levels; Model E—a bifactor model with a general factor (G ADHD) and three specific factors of inattention (S INA), hyperactivity (S HYP), and impulsivity (S IMP) on both levels.
All models were estimated with Mplus (Version 7.11; Muthén & Muthén, 2012) using the maximum likelihood estimator with robust standard errors. For statistical identification purposes, the variance of each factor was fixed at 1 on both levels. The overall model fit was evaluated with the ratio χ2 / df, the root mean square error of approximation (RMSEA), and the comparative fit index (CFI), whereas level-specific model fit was evaluated with the standardized root mean square residual (SRMR; Beauducel & Wittmann, 2005). For χ2 / df, values below 2 were taken as good model fit (e.g., Beauducel & Wittmann, 2005). Overall model fit was assessed according to criteria defined by Hu and Bentler (1999). Nested models of ADHD symptoms were compared using Satorra–Bentler scaled χ2 difference tests (Satorra & Bentler, 2001).
Results
Within-Person Fluctuations of Daily ADHD Symptoms
Overall, adolescents rated their daily ADHD symptoms relatively low on the 0 to 3 scale, with item ratings ranging between M = 0.37 (SD = 0.67) and M = 0.84 (SD = 0.81). Mean ISD for the items ranged between 0.43 and 0.61, confirming considerable fluctuations within persons from day to day. ICCs ranged from .24 to .43 indicating that the overall variance for all items was dominated by within-person variation. All results on daily ADHD symptom ratings and within-person fluctuations are depicted in Table 2.
Descriptive Statistics and Within-Person Fluctuations of Adolescents’ Daily ADHD Symptoms.
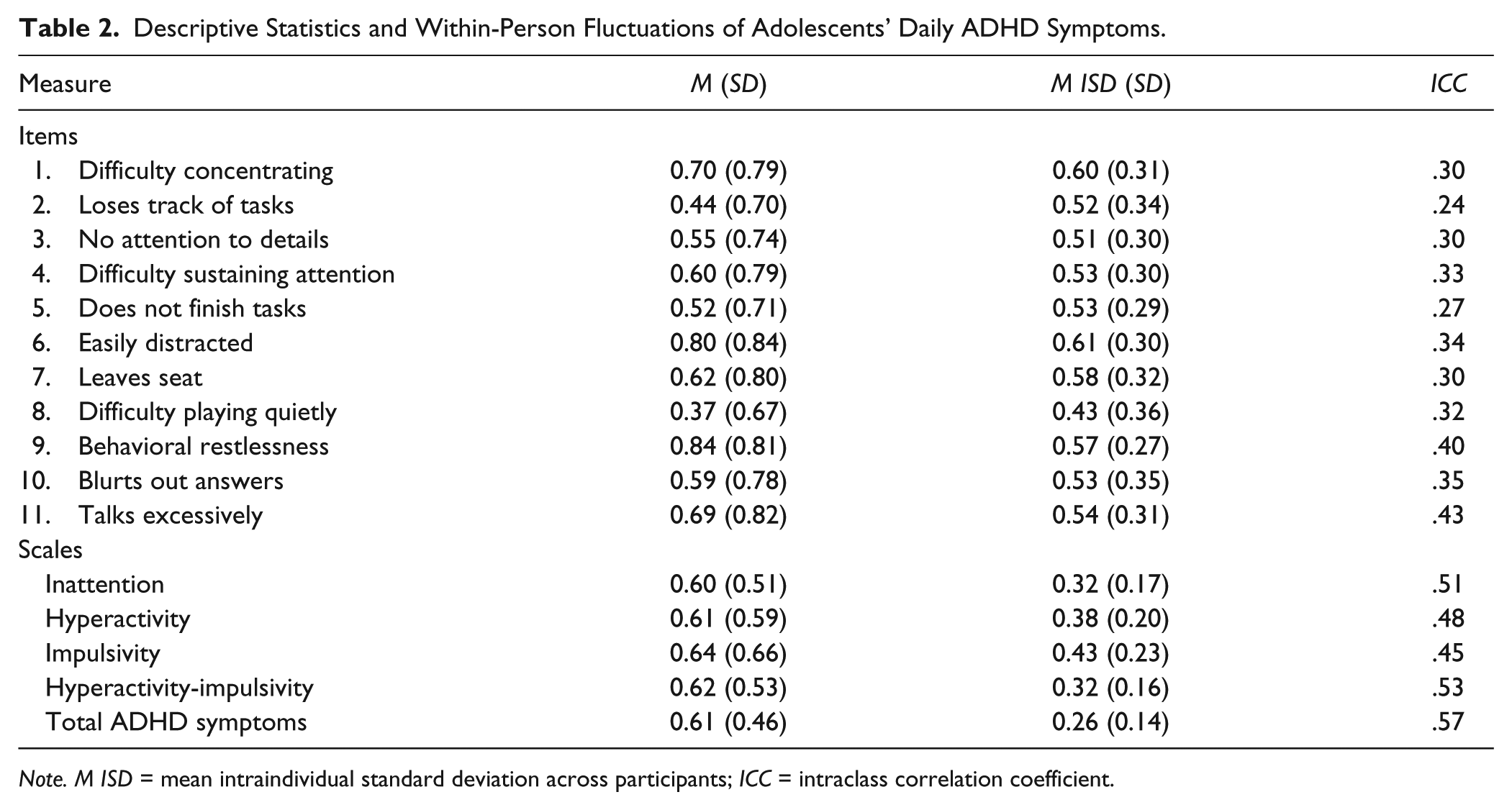
Note. M ISD = mean intraindividual standard deviation across participants; ICC = intraclass correlation coefficient.
Factor Structure of Daily ADHD Symptoms
Model selection
The one-factor model positing a single dimension underlying all ADHD symptoms on both the within- and the between-person level (Model A) did not meet all pre-defined criteria for good model fit, χ2 / df = 3.18, CFI = .87, RMSEA = .04, SRMRw/b = .04/.10 (for a summary of model fit statistics, see Table 3). The model with two correlated factors (Model B), χ2 / df = 1.99, CFI = .94, RMSEA = .03, SRMRw/b = .03/.07, and the model with three correlated factors at both levels (Model C), χ2 / df = 1.68, CFI = .96, RMSEA = .03, SRMRw/b = .03/.07, had acceptable to good fit. Comparison of nested models according to Satorra–Bentler scaled χ2 difference tests revealed that Model C had a significantly better fit than Model B.
Model Fit for Confirmatory Factor Analyses on Adolescent Daily ADHD Symptoms.
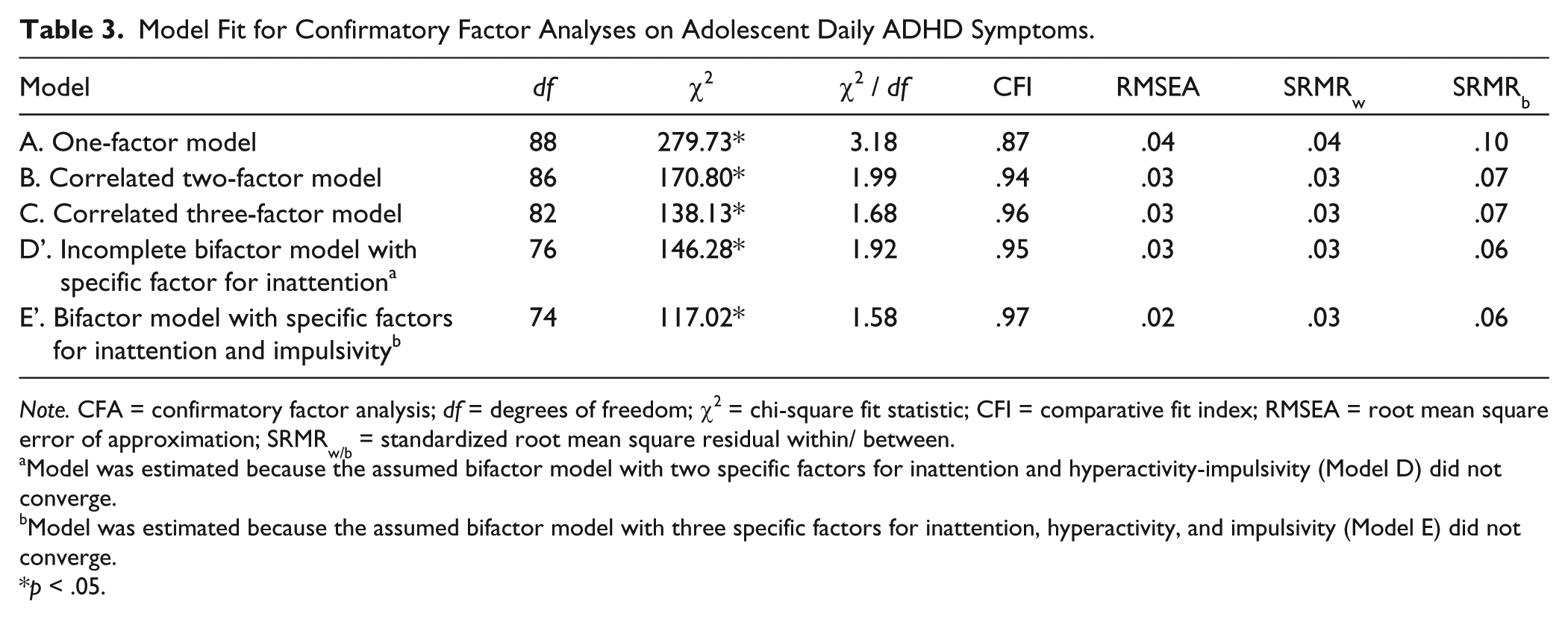
Note. CFA = confirmatory factor analysis; df = degrees of freedom; χ2 = chi-square fit statistic; CFI = comparative fit index; RMSEA = root mean square error of approximation; SRMRw/b = standardized root mean square residual within/ between.
Model was estimated because the assumed bifactor model with two specific factors for inattention and hyperactivity-impulsivity (Model D) did not converge.
Model was estimated because the assumed bifactor model with three specific factors for inattention, hyperactivity, and impulsivity (Model E) did not converge.
p < .05.
The estimation of both the bifactor model with two specific factors (S INA, S HYP-IMP) at both levels (Model D) and the bifactor model with three specific factors (S INA, S HYP, S IMP) at both levels (Model E) resulted in non-admissible solutions. Closer inspection unveiled the reason for these estimation problems to most probably lie in overfactoring related to S HYP-IMP (Model D) and S HYP (Model E), which had little variance left at both levels after accounting for G ADHD. Therefore, S HYP-IMP (Model D) and S HYP (Model E) were removed at both levels and incomplete versions of the models were estimated (cf. Ullebø et al., 2012). Both the incomplete bifactor model with S INA at both levels (Model D’), χ2 / df = 1.92, CFI = .95, RMSEA = .03, SRMRw/b = .03/.06, and the incomplete bifactor model with S INA and S IMP at both levels (Model E’), χ2 / df = 1.58, CFI = .97, RMSEA = .02, SRMRw/b = .03/.06, had good to acceptable fit. Overall, model fit for Model E’ was slightly better than for Model D’. However, as daily impulsivity was measured with only two items and bifactor models define specific factors to be uncorrelated with each other and with the general factor, factor loadings for S IMP in this model had to be constrained to equality at either level for identification purposes. Therefore, interpretability of the incomplete Model E’ with S INA and S IMP is limited. The model fit of the bifactor model with only S INA (Model D’) and the correlated three-factor model (Model C) were very similar. Thus, model interpretation for both models are presented in the following section.
Model interpretation
Correlated three-factor model interpretation for daily ADHD symptoms
On both levels, all symptoms had significant, positive loadings on the respective hypothesized factors of INA, HYP, and IMP (see Table 4). Overall, factor loadings were lower on the within- than on the between-person level. For INA, standardized factor loadings ranged from 0.34 to 0.60 on the within-person level, and from 0.65 to 0.98 on the between-person level. For HYP, loadings ranged from 0.45 to 0.48 on the within-person level, and from 0.80 to 0.91 on the between-person level. The relatively small range of factor loadings for all three indicators of HYP indicates that they are similarly important expressions at both levels. For IMP, loadings for the two indicators were 0.39 and 0.56 on the within-person level, and 0.59 and 0.98 on the between-person level. Therefore, especially with regard to the between-person level, the item tapping excessive talking dominated IMP.
Standardized Factor Loadings of the Correlated Three-Factor Model and the Incomplete Bifactor Model With Specific Inattention Factor for Adolescent Daily ADHD Symptoms on the Within-Person and Between-Person Level.
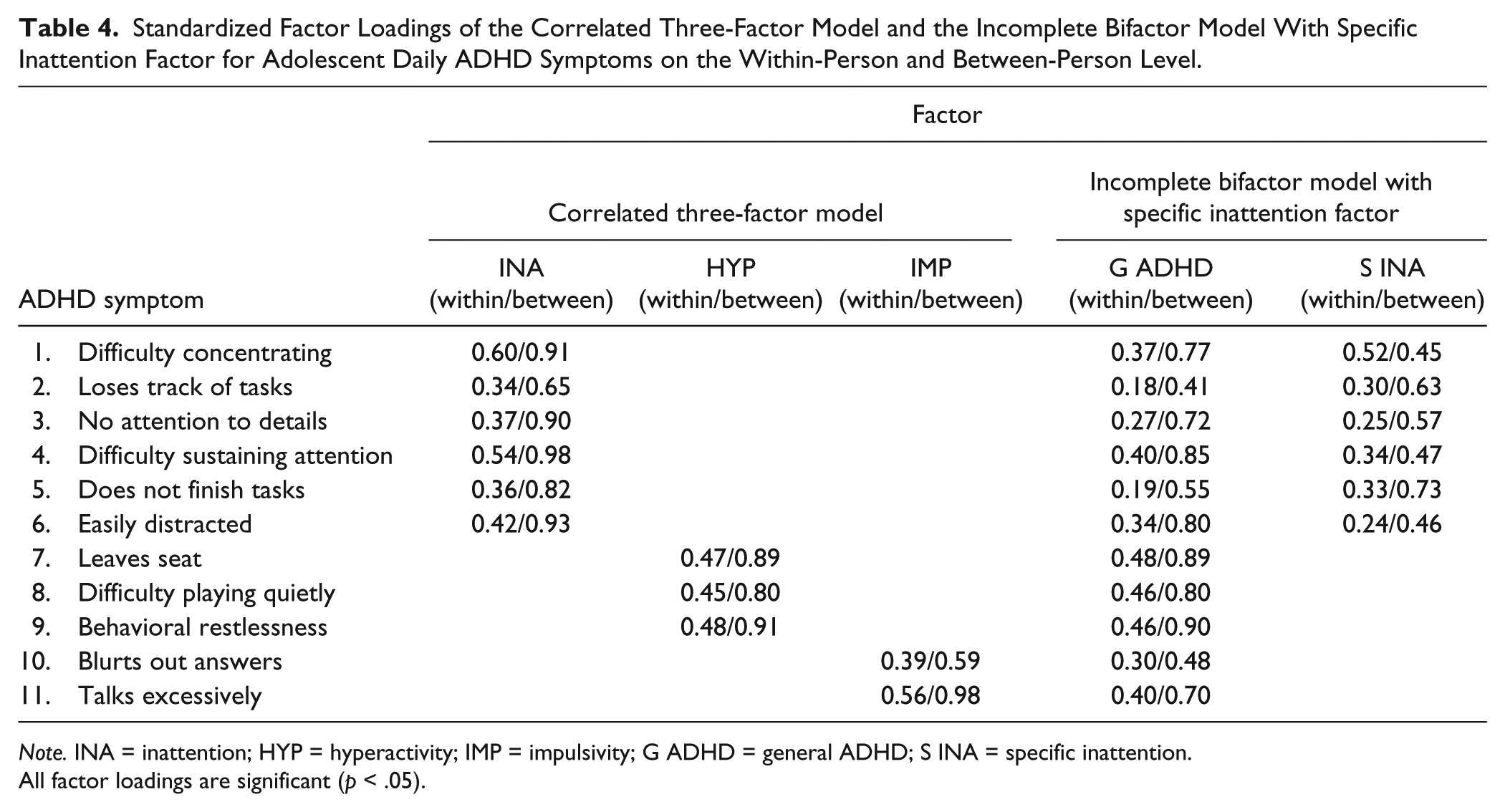
Note. INA = inattention; HYP = hyperactivity; IMP = impulsivity; G ADHD = general ADHD; S INA = specific inattention.
All factor loadings are significant (p < .05).
Correlations on the within-person level between INA and IMP (r = .40, p < .001) were moderate, for INA and HYP (r = .71, p < .001), and HYP and IMP (r = .69, p < .001) they were large. On the between-person level, the pattern of factor correlations was similar with the relatively smallest correlation between INA and IMP (r = .50, p < .001), and large correlations between INA and HYP (r = .83, p < .001), and HYP and IMP (r = .73, p < .001).
Incomplete bifactor model (Model D’) interpretation for daily ADHD symptoms
All daily symptoms loaded significantly on their respective factors (G ADHD and S INA) on both levels. Overall, factor loadings were higher on the between-person level for both G ADHD and S INA. On the within-person level, standardized factor loadings for G ADHD ranged from 0.18 to 0.48. For S INA, standardized factor loadings ranged from 0.24 to 0.52 with a balanced number of symptoms having either higher loadings on G ADHD or on S INA. On the between-person level, standardized loadings for G ADHD ranged from 0.41 to 0.90 and for S INA they ranged from 0.45 to 0.73 with four out of six items having lower loadings on S INA than on G ADHD.
In sum, adolescents’ daily ADHD symptoms can be represented equally well by a two-level correlated three-factor model and an incomplete bifactor model. The latter involves a strong G ADHD factor underlying all symptoms as well as a meaningful S INA factor both at the within- and the between-person level.
Discussion
This intensive longitudinal study showed that adolescents’ self-reported ADHD symptoms fluctuate substantially within persons from day to day. Thus, this is the first study to demonstrate substantial within-person fluctuations from day to day to be a common phenomenon in adolescents’ experiences in everyday life. The study extends previous findings from laboratory and school settings. These studies showed moment-to-moment fluctuations in computerized cognitive performance tests in individuals with ADHD (Kofler et al., 2013) and observed symptom fluctuations over the school day (Imeraj et al., 2016). Therefore, the present finding of substantial symptom fluctuations from day to day refines our understanding of ADHD symptoms in adolescence: It provides evidence for current ADHD theories that proposed the idea of within-person fluctuations in inattention, hyperactivity, and impulsivity in addition to differences in symptom levels between persons. Notably, for all items within-person fluctuations accounted for a considerable part of the total item variability as indicated by ICCs between .24 and .43. This means that up to 76% of the overall variance in daily ADHD symptoms cannot be attributed to between-person variance that was at the center of research so far. Thus, ADHD symptoms incorporate a strong dynamic dimension or state-like component that fluctuates from day to day around relatively stable individual differences (i.e., traits) in adolescents with and without ADHD diagnosis.
The substantial within-person fluctuations we found indicate that previous structural characterization of ADHD symptoms may have confounded between- and within-person variance in one-time symptom ratings. By disaggregating these types of variance, our study allows for a more differentiated view on the ADHD symptom structure that accounts for the dynamic nature of symptoms. Both a two-level factor model with three correlated factors (inattention, hyperactivity, impulsivity) and a two-level bifactor model with a general ADHD symptom factor and a specific inattention factor provided acceptable to good accounts of the structure underlying daily symptom ratings on the between- and within-person level.
Our finding that among the more traditional two-level factor models, the model with three correlated factors on both levels (Model C) fitted better than both the one-factor model (Model A) and the model with two correlated factors (Model B) underscores previous notions that it may be necessary to distinguish between hyperactivity and impulsivity (Wolraich & Lambert, 2003)—at least when not simultaneously emphasizing a general underlying ADHD component. To strengthen the finding that hyperactivity and impulsivity are separable within a correlated factor model approach on the between- and within- person level, however, future studies should include a larger number of items (e.g., items intermediately considered for DSM-5; Tannock, 2013), and use objective methods of assessment (e.g., actigraphy; Gawrilow, Kühnhausen, Schmid, & Stadler, 2014).
In addition to the correlated three-factor model, the bifactor model approach represented a good fit to the data on the between- and within-person level. This alternative approach generally is in line with (a) the proposition of a generic component of ADHD in addition to specific symptom manifestations (Martel et al., 2012), and (b) quantitative genetic studies indicating both genes that influence all symptom domains simultaneously as well as genes that influence separate specific symptom domains (e.g., Greven et al., 2011). The incomplete two-level bifactor model underscores that both general ADHD and specific inattention components are essential for fully elucidating symptom experience in terms of between-person differences and within-person fluctuations from day to day. We found that the hyperactivity and impulsivity items loaded strongly on the general symptom factor and there was too little variance left for modeling respective specific factors. This result resembles findings for one-time symptom ratings of primary school children (Ullebø et al., 2012). The specific inattention factor on the between-person level in this study suggests that there are adolescents who stably experience high levels of only inattention symptoms, underscoring the plausibility of the ICD-10 diagnosis of attention deficit disorder without hyperactivity (F98.8). Moreover, for the within-person level, our results suggest that on days with high levels of specific inattention symptoms, adolescents may not necessarily experience general ADHD symptoms and vice versa. Overall, our study presents a promising starting point for a nuanced understanding of ADHD symptom heterogeneity between and within individuals. More research is needed to replicate these findings and better understand which structural model best captures the symptom clustering on both the between- and within-person level.
Limitations of the Present Study and Related Directions for Future Research
The present study has several limitations. First, almost all adolescents diagnosed with ADHD were male. Thus, we could not compare factor structures in subsamples of male and female adolescents with versus without ADHD, respectively. However, we do not assume that the factor structures should differ between adolescents with and without ADHD diagnosis because ADHD is commonly regarded as a dimensional construct with symptoms differing in strength but not in kind between individuals with versus without diagnosis (Coghill & Sonuga-Barke, 2012). Furthermore, the few studies that have explicitly addressed the question of differences in ADHD factor structures between male and female participants have found either factorial invariance (Gibbins et al., 2012) or only minor differences in structural parameters (Ullebø et al., 2012) for one-time symptom ratings. Nonetheless, other studies have reported that female participants are more frequently affected by the inattentive subtype of ADHD than male participants (e.g., Biederman et al., 2002). Therefore, we recognize the need for future intensive longitudinal studies that investigate with adequate sample sizes whether inattention is related to hyperactivity and impulsivity similarly across gender within and between persons. Second, the between-person reliability over the eight study days was good for the entire scale as well as the subscale for inattention and hyperactivity, but was not satisfactory for the impulsivity subscale. Furthermore, reliabilities of day-to-day changes in ADHD symptoms were moderate—both for the entire scale and for all subscales. However, between-person reliabilities are by default higher than within-person reliabilities because they are based on aggregates of several days. Moreover, the reported within-person reliabilities are comparable with those previously reported for a measure of daily impulsivity (Tomko et al., 2014). Nevertheless, future research should aim at improving measurement accuracy and consider a greater pool of items to select reliable subsets, particularly for the impulsivity subscale. The underrepresentation of impulsivity and hyperactivity items in this study made it difficult to draw clear conclusions about whether specific factors of impulsivity and hyperactivity do possibly underlie daily symptom ratings. The use of only two impulsivity items was especially critical: A bifactor model with a specific impulsivity factor was not testable due to the model not being saturated without placing an additional constraint on the model (i.e., equality of factor loadings for both items on the specific inattention factor on both levels). Better and more daily hyperactivity and impulsivity items will allow to draw conclusions about whether specific factors of both hyperactivity and impulsivity possibly underlie daily symptoms.
Clinical Implications and Implications for Future ADHD Research
The present findings have important implications for both assessment and intervention in ADHD. First, the results imply that systematic within-person fluctuations in ADHD symptoms may be important to complement the description of an individual’s symptom status. Thus, clinicians should routinely conduct repeated assessments in the diagnostic process as already implicitly suggested in diagnostic guidelines by notions of context-specific symptom levels within a given setting (APA, 2013). Second, to derive individually tailored interventions that effectively reduce symptoms in adolescents’ everyday life, clinically oriented research should investigate antecedents, correlates, and consequences of enhanced symptoms in everyday life. Particularly, we suggest intensive longitudinal research conducted over representative study periods with multiple assessments per day integrating repeated self-reports, physiological assessments, and observed behavior. This research should investigate which situations are associated with particularly low or high activation, high inhibitory demands, or are experienced as overly delaying. These situations may give rise to high symptom levels, negative emotional experiences, or problematic social interactions (Sonuga-Barke et al., 2010; van der Meere, 2005). Such knowledge about possibly person-specific antecedents, correlates, and consequences of high symptom levels in everyday life would pave the way for interventions delivering elements of cognitive behavioral treatment, medication, or a combination thereof, depending on environmental demands and current symptom levels. Tailored interventions may provide effective treatment options for patients experiencing negative side effects or non-response to classic fixed-dose medication regimens (Storebø et al., 2015) and reduce the total amount of medication intake.
Conclusion
Adolescents show substantial and systematic fluctuations in ADHD symptoms from day to day. This questions one-time assessments and calls for a more intensive diagnostic process with repeated reports by adolescents and also clinicians, teachers, and parents. Furthermore, this study lays the groundwork for investigating individual context-dependent and potentially time-varying antecedents, correlates, and consequences of daily ADHD symptoms as it has established ADHD symptoms as a within-person phenomenon. Moreover, the findings of the present study highlight the need for interventions to account for fluctuations in symptoms from day to day.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Center for Individual Development and Adaptive Education of Children at Risk (IDeA), funded by the Federal State Government of Hessen (LOEWE initiative), and by the Robert Bosch Foundation, Stuttgart, Germany.