
Abstract
Introduction
ADHD is a common psychiatric disorder with childhood onset, characterized by inappropriate levels of inattention, impulsivity, and hyperactivity (Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM-5; American Psychiatric Association, 2013). Follow-up studies have documented the persistence of ADHD into adulthood, including persistence of impairing ADHD symptoms in 50% to 65% of the cases (Faraone, Biederman, & Mick, 2006). The prevalence of ADHD in adults has been estimated at 4.4% in the United States (Kessler et al., 2006). ADHD significantly interferes with several major life domains and has a negative social, academic, or professional impact (Faraone et al., 2000).
Executive functioning deficits contribute to the impairments in occupational functioning that occur in conjunction with adult ADHD (Barkley & Murphy, 2010). Executive functions correspond to higher-order, top-down cognitive processes that enable flexible, goal-directed behavior. This includes such functions as mental set-shifting, information updating and monitoring, and inhibition of prepotent responses (Miyake et al., 2000). The most consistently altered domain in ADHD is inhibition processes and switching (Barkley, 2006; Boonstra, Kooij, Oosterlaan, Sergeant, & Buitelaar, 2010). However, cognitive impairments in this population are very heterogeneous among patients, and the pathophysiological background remains unclear.
Some comprehensive theories have attempted to explain neuropsychological functioning in ADHD. One of the most prominent models was proposed by Barkley in 1997. It focuses on deficient inhibitory control as the core deficit, secondarily disrupting other executive processes and ultimately resulting in typical behavioral symptoms of ADHD. Inhibitory control involves suppressing dominant, automatic, or prepotent responses and possibly overriding them with more deliberate processes. With “the cognitive-energetic model,” Sergeant (2000) proposed that an inhibition deficit in ADHD is dependent upon the modulation of the physiological state (arousal/activation/effort) of the participant to meet task demands (Metin et al., 2016).
In the same line, hypoarousal and daytime sleepiness were recently identified as one of six future research directions and priorities by a consensus working group on sleep and ADHD (Owens et al., 2013). Arousal is a term that is used differently by different groups of scientists but more consistently refers to nonspecific activation of the cerebral cortex in relation to sleep–wake states (Oken, Salinsky, & Elsas, 2006). Dysregulation of arousal could be involved as a pathophysiological mechanism underlying attention deficit in ADHD (Benikos & Johnstone, 2009; Miano et al., 2006). Deficit in arousal modulation in ADHD has been found to be related to deficits in cognitive performance, particularly in response inhibition (Benikos & Johnstone, 2009). The few studies assessing the objective level of alertness with electrophysiological clinical procedures are inconsistent, both in ADHD children (Golan, Shahar, Ravid, & Pillar, 2004; Lecendreux, Konofal, Bouvard, Falissard, & Mouren-Simeoni, 2000; Prihodova et al., 2010) and ADHD adults. Indeed, our team recently showed (Bioulac et al., 2015) that a significant proportion of adult ADHD patients (35%) exhibit objective excessive daytime sleepiness (EDS) as measured by a short mean sleep latency on the Maintenance of Wakefulness Test (MWT), in which participants are requested to try to stay awake. A study using another objective measure of daytime sleepiness (Multiple Sleep Latency Test, MSLT), requesting participants to try to fall asleep, shows that ADHD patients’ reports of EDS are verified by a shorter sleep latency on the MSLT (Sobanski et al., 2016). Objective assessments of daytime sleepiness in ADHD are thus warranted.
In addition, ADHD patients have a higher risk of motor vehicle accidents and impaired driving performance (Barkley, Murphy, Dupaul, & Bush, 2002; Jerome, Habinski, & Segal, 2006; Reimer, Mehler, D’Ambrosio, & Fried, 2010). In the driving simulator, adults with ADHD showed significantly more erratic steering, an individual skill predisposing participants toward traffic offenses and crashes (Barkley, 2004; Barkley, Murphy, & Kwasnik, 1996). Traditional views postulate that neuropsychological deficits might contribute to the driving impairments among adults with ADHD (Barkley et al., 2002; Fried et al., 2006). Nevertheless, our recent findings showed that the sleepiest participants (MWT score < 20 min) exhibited more impaired driving performance in monotonous conditions than nonsleepy ADHD patients and controls (Bioulac et al., 2015). Therefore, objective daytime sleepiness could be a factor contributing to functional impairments in ADHD patients.
The identification of factors contributing to poor driving performance in ADHD patients is a topic of high clinical and public health importance. Up to now, however, it has remained unclear whether driving impairment with ADHD is explained by an alteration of objective daytime sleepiness (physiological level of arousal), by cognitive deficits or by both. The aim of this study was to determine the respective contribution of these factors on highway driving performance in adults with ADHD.
Method and Materials
Population
ADHD patients were recruited from the attentional disorders outpatient clinic at the Department of Child and Adolescent Psychiatry, University of Bordeaux (France), according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria. Childhood and chronic course of ADHD symptoms from childhood to adulthood were established by a board-certified psychiatrist who carried out a clinical evaluation and administered a semi-structured diagnostic interview (Conners’ Adult ADHD Diagnostic Interview for DSM-IV [CAADID]; Epstein, Johnson, & Conners, 2000). We used the Conners’ Adult ADHD Rating Scales (CAARS; Conners & Jett, 1999). In addition, the French version of the Wender Utah Rating Scale (Ward, Wender, & Reimherr, 1993) and the Brown Questionnaire were employed to qualify the ADHD symptoms of our patients. Patients filled out the Epworth Sleepiness Scale (ESS; Johns, 1991) to assess subjective daytime sleepiness (EDS). We excluded all patients with any clinically relevant medical or psychiatric condition including current mood or psychotic disorders, and substance abuse within 1 year prior to screening, shift work, and long-term treatment with benzodiazepine. Comorbid psychiatric disorders were assessed with the Mini International Neuropsychiatric Interview (MINI 5.0.0. DSM-IV; Sheehan et al., 1998). All patients were withdrawn from psychostimulant medication for a minimum of 72 hr before starting the study and were without other psychotropic medication for a minimum of 1 month.
Healthy control participants were recruited among the general population. We excluded participants with any psychiatric disorders plus any complaint of sleep disorders (reported on the Basic Nordic Sleep Questionnaire [BNSQ]; Partinen & Gislason, 1995) and subjective EDS based upon the ESS (score > 10). The presence of nocturnal sleep-disordered breathing (apnea–hypopnea index [AHI] > 10/hr) and periodic limb movements (PLM; index > 15/hr) were ruled out through ambulatory polygraphy, which included an electromyography (EMG) channel on the anterior tibialis muscle of each leg. ADHD symptoms were ruled out in the control population with the Adult ADHD Self-Report Scale (ASRS; 18 items; Adler et al., 2006) and the CAARS self-evaluation.
All the participants possessed a driving license and had attended secondary education up to Grade 9. All participants provided written informed consent, and the local ethical committee (consultative committee for the protection of persons participating in biomedical research, Comité de Protection des Personnes [CPP] Sud-Ouest et Outre Mer III) approved the study, which was registered as a clinical trial (ClinicalTrials.gov identifier: 2009-A01276-51). The participants were compensated with 100 euros for their participation.
Study Design
Patients and controls were instructed to maintain a regular sleep–wake schedule in the 3 days preceding the 1-hr driving session on simulator at 5:00 p.m. at laboratory. Then, a nocturnal polysomnography (PSG) was administered, followed the next day by a 4 × 40-min MWT and a battery of neuropsychological tests (Figure 1). All neuropsychological tests were administered at the same time of day for all participants. We ensured that participants had not practiced the neuropsychological tests used for this study 1 year prior to participation to minimize any learning effect.

Overview of protocol design.
Sleep Recordings
PSG
The following parameters were monitored: electroencephalogram (EEG; F3/A2, C3/A2, O2/A1, from the 10–20 international electrode placement system), electrooculogram, chin and leg electromyogram, electrocardiogram, and body position. Respiration was monitored with a nasal cannula and thoracic and abdominal belts. Oxygen saturation was recorded by pulse oximetry. Sleep and respiratory events were manually scored by an experienced sleep technician in 30-s epochs according to the recommendations of the American Academy of Sleep Medicine (AASM) Manual for the scoring of sleep and associated events (Iber, Ancoli-Israel, Chesson, & Quan, 2007; Rechtschaffen & Kales, 1968).
MWT
Four 40-min MWT trials were performed at 10:00 a.m., 12:00 p.m., 2:00 p.m., and 4:00 p.m. as recommended by the AASM practice parameters (Littner et al., 2005). The room was shielded from external light, and the only light source (10 lx) was positioned behind the patient’s head. The test was administered by an experienced sleep technologist: EEG (C3/A2, O2/A1) and an electromyogram and electrooculogram were recorded. Patients and control participants were video monitored throughout the test. They were not allowed to use any artificial strategy to stay awake, such as moving continuously or singing. They were asked to fight against sleepiness in a soporific condition. Data were manually scored in 30-s epochs according to the recommendations of AASM (Iber et al., 2007). Sleep onset was defined as the first epoch of greater than 15 s of cumulative sleep in a 30-s epoch. The test was ended after three continuous epochs of Stage N1 or one epoch of any other sleep stage to avoid interfering with the sleep homeostasis process (Littner et al., 2005). As recommended by the AASM practice parameters (Littner et al., 2005), patients who did not sleep during a trial were assigned a value of 40 min. The mean sleep latency of the four MWT trials was then calculated.
Neuropsychological Tests
Neuropsychological battery comprised the following:
The computerized Test of Attentional Performance (TAP) was administered to evaluate various aspects of attention. Three subtests were selected: Vigilance, Alertness, and Flexibility. For each task, mean reaction time (RT) on correct responses and total number of omission errors (number of missed targets) were recorded (Zimmermann & Fimm, 2009).
The Conners’ Continuous Performance Test II (CPT II) is basically a test of sustained attention and impulsivity. The dependent measures were mean RT for hits, which measure the response execution process; the number of omission errors (missed targets) from the failure to respond to target letters (i.e., non-Xs), which assesses sustained attention; and the number of commission errors (false hits) made when responses are given to nontargets (i.e., Xs), which assesses response inhibition (Conners, 2000).
The Useful Field of View (UFOV) is a computer-based test of visual attention and processing speed involving detection and localization of briefly presented targets throughout the visual field. For each subtest, the score is the stimulus exposure time (ms) required for the participant to achieve 75% accuracy in responding (Ball & Owsley, 1993).
The Digit Symbol Substitution Test (DSST), a component of the Wechsler Adult Intelligence Scale, is frequently used to measure associative ability and speed information processing. The dependent measure was the number of correct responses (Wechsler, 1981).
The Trail Making Test (TMT) A and B: TMT-A time is considered as a measure of processing speed, while TMT-B time is viewed as an index of flexibility. The dependent variables are the number of seconds needed to complete the sequence and the number of correct responses for Part B and an interference index (Part A/Part B; Reitan & Wolfson, 1985).
The Wisconsin Card Sorting Test (WCST) is a widely used task assessing cognitive flexibility via set-shifting. Dependent measures were the number of categories achieved and the number of perseverative errors (Heaton, 1981).
The Stroop Color-Naming Test is a classical neuropsychological test that measures the ability to inhibit competing responses in the presence of salient conflicting information. The difference score between RTs of named colors on the incongruent card and the one of the neutral card, and the difference score between the number of errors of named colors on the incongruent card and that of the neutral card were calculated to represent interference indices (Stroop, 1935).
Finally, the Tower of London (TOL), a task of planning ability, was given. Dependent measures were total number of moves, total problem-solving duration, and number of correct solutions in minimum number of moves (Shallice, 1982).
Simulated Driving Test
Participants performed a 60-min task in a driving simulator (Oktal®) composed of a simplified car cockpit with a car seat, a steering wheel with force feedback, a manual gearbox, pedals, and three display monitors (19 inches, see Figure 2). The monitors were viewed from a distance of about 60 cm. The three monitors were positioned side by side to create a driving scene that subtended a total of 130 degrees horizontal × 30 degrees vertical of visual angle. A left and right mirrors displayed in the visual provided a view behind the vehicle. The visual scene was rendered and updated at a rate of 60 Hz by the SCANeR™ studio software running on a computer. The scene displayed normal traffic conditions (infrequent vehicles) on a closed-loop highway to reproduce real driving conditions as accurately as possible. Participants were instructed to maintain a constant legal speed (130 km/hr [80 miles/hr]) and not to cross the lane borders. During the task, the vehicle’s speed and the lateral position of the vehicle from the center of the road were continuously recorded. The software calculated the standard deviation of the lateral position (SDLP, cm), which measures the weaving of the car during the driving session (Bioulac et al., 2015; Ramaekers, 2003; Verster, Taillard, Sagaspe, Olivier, & Philip, 2011). The number of inappropriate line crossings (ILCs) during the driving session was also computed (Davenne et al., 2012; O’Hanlon, Vermeeren, Uiterwijk, van Veggel, & Swijgman, 1995; Philip et al., 2005; Sagaspe et al., 2008). An ILC was scored when the driver crossed a lateral highway lane knowing that no overtaking maneuver was possible in this scenario.

Oktal driving simulator.
Statistical Analyses
Quantitative variables were expressed as mean ± standard deviation (SD), and qualitative variables were expressed as relative frequency.
Between-group comparisons with the Mann–Whitney U Test for continuous variables or Chi-Square Test (χ2) for categorical variables were used to compare demographic, clinical, and polysomnographic characteristics and neuropsychological test performance in adult patients with ADHD versus healthy controls.
For regression analyses, all variables (demographic, clinical characteristics, and neuropsychological performance) associated with driving performance (SDLP and ILC) on the simulator in ADHD patients were initially examined separately using univariate models. Multivariate logistic regression analyses using a binary driving performance variable based upon the median as the outcome variable were performed for all variables that showed a significant association with SDLP or ILC in univariate models. Reverse order of scores was entered in the model when appropriate to obtain an odds ratio > 1.
The alpha risk threshold was set at p = .05. All analyses were performed using the SPSS statistical software package (PASW® Statistics 18).
Results
Population
Forty-nine ADHD patients were recruited; however, two patients did not agree to participate, and one patient was not eligible (owing to a major depressive disorder). Forty-six ADHD patients were included, but six ADHD patients exhibited cybersickness on the driving simulator, and the PSG was not correctly recorded for another ADHD patient.
The sample thus consisted of 39 ADHD patients (Mage = 36.2 ± 9.0 years, range = 20-52 years, male = 18, years of education = 13.7 ± 2.7) and 18 age-, gender- and educational-level-matched healthy controls (Mage = 37.2 ± 10.1 years, range = 20-52 years, male = 8, years of education = 14.4 ± 2.3). Among the 39 ADHD patients included in the present study, 20 (50%) had comorbid anxiety disorders (past or present) and 24 (60%) had a history of mood disorder but no current mood disorder. Twenty-seven (70%) presented with ADHD of the mixed subtype and 12 (30%) with the inattentive subtype.
Table 1 represents comparisons of demographic and clinical characteristics, and driving performance and neuropsychological test performance between ADHD patients and control groups.
Demographic and Clinical Characteristics, and Driving Performance and Neuropsychological Test Performance (M ± SD) in Adult Patients With ADHD and Healthy Controls Groups.

Note. Statistical significance (p values) for between-groups comparisons with Mann–Whitney U Test for continuous variables or Chi-Square Test (χ2) for categorical variables. Sleep can be broken down into four distinct stages: N1, N2, N3 and rapid Eye Mouvement (REM). n = effectives; CAARS = Conners’ Adult ADHD Rating Scales; ESS = Epworth Sleepiness Scale; MWT = Maintenance of Wakefulness Test; REM = rapid eye movement; API = apnea–hypopnea index; PLM = periodic limb movements; SDLP = standard deviation of the lateral position; ILC = inappropriate line crossings; TAP = Test Battery for Attentional Performance; RT = reaction time; CPT = Continuous Performance Test; UFOV = Useful Field of View; DSST = Wechsler Digit Symbol Substitution Test; TMT = Trail Making Test; TOL = Tower of London; WCST = Wisconsin Card Sorting Test.
Sleep Recordings
PSG
ADHD patients and controls slept, respectively, 403 ± 42.6 min versus 399.8 ± 42.2 min (NS) during the night prior to the MWT. Sleep efficiency was not significantly different between the groups (84.9 ± 8.7 vs. 84.5 ± 7.5). In ADHD patients, the mean AHI was 5.2 ± 6.5/hr, and the mean index of PLM was 4.8 ± 12.4/hr. Three ADHD patients had an AHI above 10/hr, and four ADHD patients had a PLM index > 15 events/hr. One patient had both indices above the pathologic cut-off. Finally, no difference appears on parameters of sleep macroarchitecture in controls versus ADHD patients (sleep latency = 17.7 min ± 14.6 vs. 16.9 min ± 26.4, Mann–Whitney U Test = 0.826, ns; Stage N1 = 7.7% ± 3.4 vs. 6.9 ± 3.1, Mann–Whitney U Test = 0.807, ns; Stage N2 = 51.2% ± 7.8 vs. 48.8 ± 8.9, Mann–Whitney U Test = 0.876, ns; Stage N3 = 21.9% ± 6.6 vs. 22.8 ± 9.1, Mann–Whitney U Test = −0.052, ns; Stage REM = 19.2% ± 5.6 vs. 21.4 ± 6.8, Mann–Whitney U Test = −1.476, ns; Table 1).
MWT
ADHD patients displayed a significantly shorter mean sleep latency on the MWT than controls (25.4 ± 9.7 min vs. 39.0 ± 2.0, p < .001).
Simulator Driving Test
ADHD patients had higher steering variability (SDLP) than controls (40.5 ± 11.2 vs. 31.9 ± 6.4, p < .01) and higher number of ILC than controls (39.1 ± 31.6 vs. 23.9 ± 29.9, p < .05; Table 1).
Neuropsychological Tests
Compared with controls, ADHD patients presented deficits in vigilance performance, alertness performance, shifting attentional performance, sustained attention, visual perceptual threshold, speed of information processing, and executive functioning, notably inhibition (Table 1).
Predictors of Driving Performance in ADHD Patients
The median of steering variability (SDLP) on the simulator in the group of ADHD patients was 37.998 cm. Nineteen ADHD patients were categorized as having poor highway driving performance.
For multivariate logistic regression analysis, continuous variables entered in the model were as follows: MWT mean sleep latency (reverse order), number of correct responses on DSST, number of commission errors on CPT, interference index (on correct responses) on Stroop task, and number of perseverative errors on WCST. The model was adjusted for age, gender, educational level, ADHD severity (CAARS), history of anxiety disorders, and history of major depressive disorder.
In ADHD patients, a risk of poor highway driving performance (SDLP) was multiplied by 1.13—95% confidence interval (CI) [1.03, 1.24], p < .05—per minute less on sleep latency on the MWT. Independently, a risk of poor driving performance was multiplied by 2.68 (95% CI [1.05, 6.82], p < .05) per additional error on the Stroop interference index.
Table 2 describes the risk factors associated with high SDLP in ADHD patients.
Multivariate Logistic Regression Results for Prediction of Poor Highway Driving Performance on Simulator Based Upon Median (SDLP > 37.998 cm) in Adult Patients With ADHD.
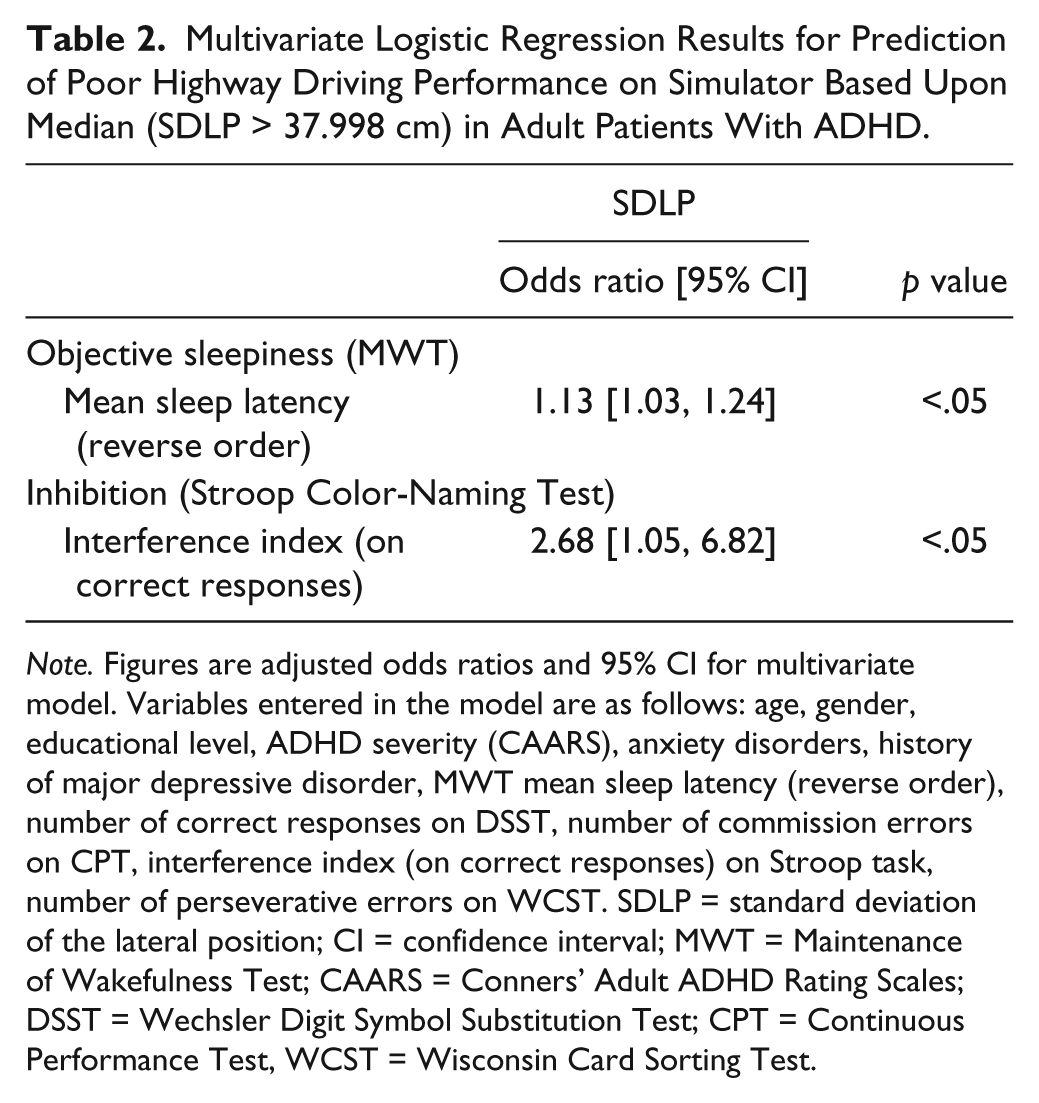
Note. Figures are adjusted odds ratios and 95% CI for multivariate model. Variables entered in the model are as follows: age, gender, educational level, ADHD severity (CAARS), anxiety disorders, history of major depressive disorder, MWT mean sleep latency (reverse order), number of correct responses on DSST, number of commission errors on CPT, interference index (on correct responses) on Stroop task, number of perseverative errors on WCST. SDLP = standard deviation of the lateral position; CI = confidence interval; MWT = Maintenance of Wakefulness Test; CAARS = Conners’ Adult ADHD Rating Scales; DSST = Wechsler Digit Symbol Substitution Test; CPT = Continuous Performance Test, WCST = Wisconsin Card Sorting Test.
The median of ILC on the simulator in the group of ADHD patients was 30. Twenty ADHD patients were categorized as having poor highway driving performance.
For multivariate logistic regression analysis, continuous variables entered in the model were as follows: MWT mean sleep latency (reverse order), sleep efficiency, RTs on TAP flexibility, number of correct responses on DSST, total problem-solving time on TOL, number of perseverative errors on WCST, and selective attention on UFOV. The model was adjusted for age, gender, educational level, ADHD severity (CAARS), history of anxiety disorders, and history of major depressive disorder.
In ADHD patients, a risk of poor highway driving performance (ILC) was multiplied by 1.13 (95% CI [1.02, 1.25], p < .05) per minute less on sleep latency on the MWT. Independently, sleep efficiency was associated with lower risk of ILC: 0.90 (95% CI [0.81, 0.99], p < .05).
Table 3 describes the risk factors associated with ILC in ADHD patients.
Multivariate Logistic Regression Results for Prediction of Poor Highway Driving Performance on Simulator Based Upon Median (ILC > 29.5) in Adult Patients With ADHD.
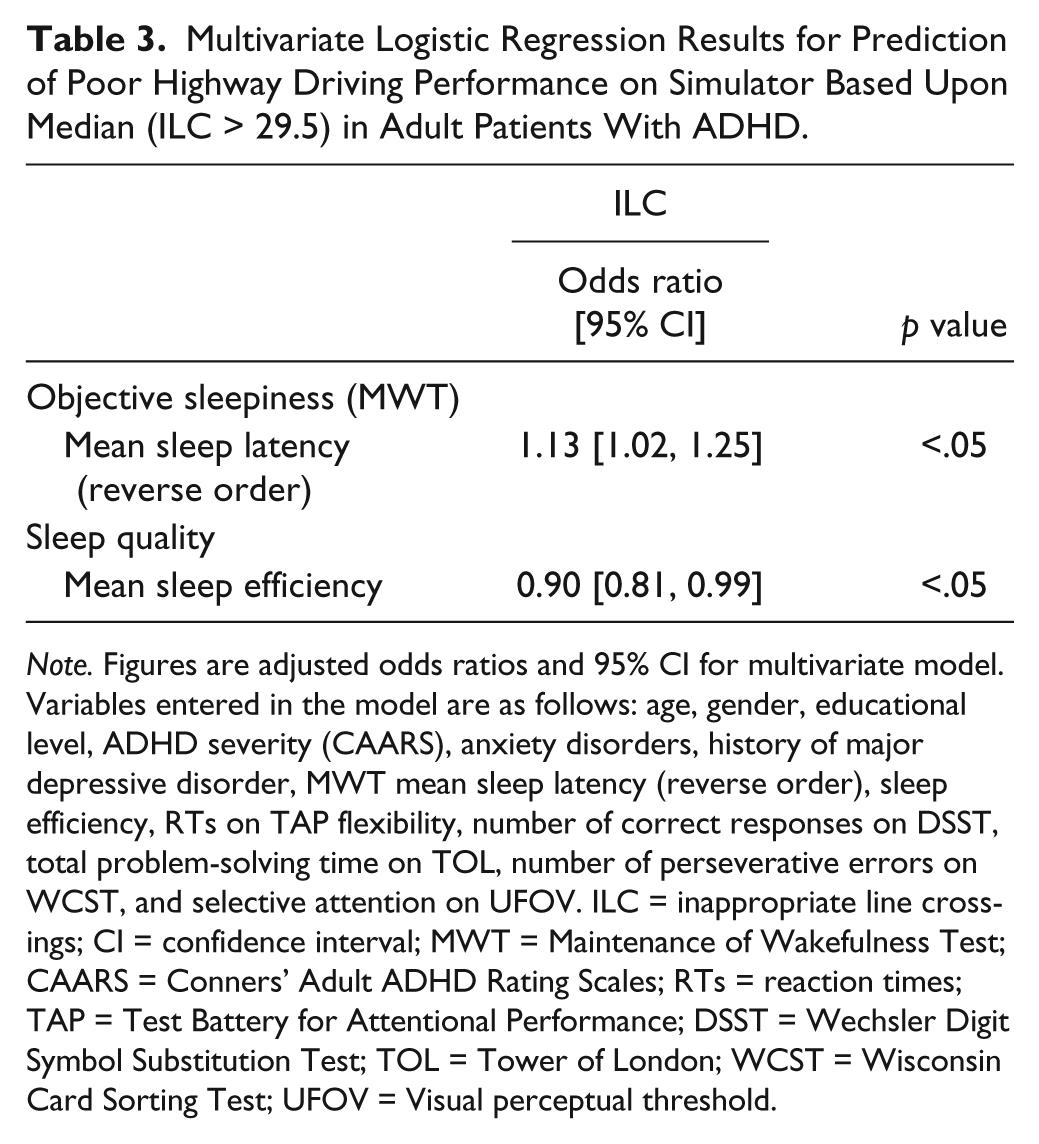
Note. Figures are adjusted odds ratios and 95% CI for multivariate model. Variables entered in the model are as follows: age, gender, educational level, ADHD severity (CAARS), anxiety disorders, history of major depressive disorder, MWT mean sleep latency (reverse order), sleep efficiency, RTs on TAP flexibility, number of correct responses on DSST, total problem-solving time on TOL, number of perseverative errors on WCST, and selective attention on UFOV. ILC = inappropriate line crossings; CI = confidence interval; MWT = Maintenance of Wakefulness Test; CAARS = Conners’ Adult ADHD Rating Scales; RTs = reaction times; TAP = Test Battery for Attentional Performance; DSST = Wechsler Digit Symbol Substitution Test; TOL = Tower of London; WCST = Wisconsin Card Sorting Test; UFOV = Visual perceptual threshold.
Discussion
This study demonstrates for the first time that poor highway driving control in adults with ADHD is predicted independently by objective daytime sleepiness and inhibition deficit.
We confirm in this study that compared with controls, adults with ADHD had higher attention deficits, were slower, and made more errors on executive tasks. The neuropsychological difficulties we found are similar to those in previous studies on adults with ADHD (Riccio, Wolfe, Romine, Davis, & Sullivan, 2004; Seidman et al., 2004) with an inhibition deficit, one of the most consistently altered domains in ADHD (Advokat, 2010; Barkley, 1997, 2006; Boonstra et al., 2010; Boonstra, Oosterlaan, Sergeant, & Buitelaar, 2005; Hervey, Epstein, & Curry, 2004).
One of the main results is that inhibitory control deficit proves to be a risk factor for poor highway driving performance in ADHD. This confirms and extends previous work showing that ADHD individuals at high risk for poor driving behavior might be distinguishable from other ADHD individuals on neuropsychological deficits, notably inhibitory control (Fried et al., 2006). Similarly, a study (Barkley et al., 2002) identified correlations between impairments in inhibition capacity and accident frequency, and between interference control impairment and traffic violations. These findings confirm that such a deficit might contribute to the effects of ADHD on functional ability in everyday life such as driving. Interestingly, our predictive model shows that inhibitory control deficit measured by the Stroop task better explains poor highway driving control in adults with ADHD than more basic cognitive attentional components (vigilance, alertness, sustained attention) measured by neuropsychological tests.
Independently, another main result of this work is that level of alertness is an associated risk factor of poor highway driving in ADHD participants. Sleepiness due to behavioral sleep restriction, sleep disorders, or induced by pharmacological treatment has deleterious effects on simulated and real driving performance (Banks, Catcheside, Lack, Grunstein, & McEvoy, 2005; Philip et al., 2013; Philip et al., 2008; Pizza, Contardi, Ferlisi, Mondini, & Cirignotta, 2008; Pizza, Contardi, Mondini, Trentin, & Cirignotta, 2009; Sagaspe et al., 2010). In addition, sleepiness has been identified as one of the major causes of traffic accidents and fatal crashes (Blazejewski, Girodet, Orriols, Capelli, & Moore, 2012; Connor, Whitlock, Norton, & Jackson, 2001; Philip & Sagaspe, 2011; Philip et al., 2010; Pizza et al., 2010). In a previous experimental study, our team showed that a significant proportion of adults with ADHD exhibited objective EDS that affects simulated driving performance (Bioulac et al., 2015). These findings demonstrate that objective daytime sleepiness plays a key role in ADHD driving impairment independent of cognitive deficits. As objective daytime sleepiness may play a role in ADHD, one of the strengths of our study is that we controlled for the effects of physiological arousal via an objective measure of sleepiness (MWT) to assess the impact of neuropsychological deficits on functional activity in everyday life. Our study proves that ADHD individuals do not suffer from a unique inhibition deficit that accounts for all functional and real-world impairments. Because there is growing evidence for a particular phenotype of ADHD suffering for objective daytime sleepiness (Bioulac et al., 2015; Reimer, D’Ambrosio, Coughlin, Fried, & Biederman, 2007), taken together, these results highlight the need for more stringent prevention, screening, and treatment of sleepiness in ADHD objectively measured by electrophysiological clinical method.
From a neurobiological standpoint, on one hand, our results support the well-known hypothesis that the behavioral disturbances of ADHD are the result of an imbalance between noradrenergic and dopaminergic systems in the prefrontal cortex involved in executive functions (Genro, Kieling, Rohde, & Hutz, 2010; Russell, 2002). On the other hand, waking systems (i.e., orexin, histamine), which promote arousal and maintain wakefulness (Alexandre, Andermann, & Scammell, 2013), could play a role in the pathophysiology of ADHD. Particularly, our result of a wake dysregulation (i.e., objective sleepiness) adding to the core inhibition deficit in ADHD corroborates the hypothesis of alterations in the hypocretin/orexin neurotransmitter system in this disorder (Cortese, Konofal, & Lecendreux, 2008).
Furthermore, recent studies show behavioral, cognitive, and neurobiological links between ADHD and narcolepsy, a syndrome characterized by hypothalamic orexin dysregulation (Nishino, Ripley, Overeem, Lammers, & Mignot, 2000). Both executive control of attention deficit and sleepiness occur in this syndrome, with the former being explained by the severity of objective sleepiness (Bayard, Croisier Langenier, Cochen De Cock, Scholz, & Dauvilliers, 2012) and with the latter being particularly elevated in those patients with a childhood history of ADHD (Modestino & Winchester, 2013). In line with this, our findings thus confirm the interest to explore the role of the orexin system in the pathophysiology of ADHD (Cortese et al., 2008).
All together, these findings support new pharmacological options that might significantly improve alertness and cognition of sleepy patients with ADHD, and consequently improve their quality of life. The wake-promoting action of modafinil coupled with its beneficial effects on inhibition response in adults with ADHD (Turner, Clark, Dowson, Robbins, & Sahakian, 2004) may have a direct beneficial action on real-life abilities.
Considering the neuropsychological models of ADHD, our results seem more in line with the alternative “dual-process” models (Metin et al., 2016; Nigg & Casey, 2005; Sergeant, 2000; Sonuga-Barke, 2003; Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005). The latter emphasize the dynamic interplay of bottom-up-driven factors such as activation, arousal, alerting, motivation, reward, and temporal processing with top-down cognitive control processes in explaining the findings of ADHD impairment on executive functions. ADHD patients have difficulty applying effort to maintain an optimal activation state during difficult, challenging, or monotonous conditions. Difficulties regulating the activation state are further reflected in an functional magnetic resonance imaging (fMRI) study showing that ADHD patients showed higher activation than controls in default mode network regions during task items with extreme event rates (fast and slow) requiring mental effort. The activity of these regions, which is normally suppressed during effortful task performance, suggests state regulation deficits in ADHD necessary to optimize task engagement (Metin et al., 2015). Future simulated driving tasks in fMRI could verify how this disruption of default mode network attenuation can be related to inhibition deficits and sleepiness affecting driving performance, as found in the current study.
It is important to note that our driving task was a monotonous highway scenario possibly inducing decreasing arousal in addition to low workload (Jackson, Kleitman, & Aidman, 2014; Pattyn, Neyt, Henderickx, & Soetens, 2008). The fact that inhibitory control deficit is a predictor of performance on this task strongly suggests that top-down cognitive control is necessary to recruit additional resources. Further studies will be needed to better understand the respective and complementary role of physiological arousal and cognitive control on driving tasks differing in executive components of ADHD.
Several methodological limitations need to be considered. First of all, this study had a small sample size that limits the generalizability of the findings. Our sample of ADHD individuals was selected on their high educational level, implying that neuropsychological deficits may be not representative of the general adult ADHD population. Indeed, deficits in executive functioning are known to be associated with lower academic achievement, irrespective of ADHD status (Biederman et al., 2006). Another limitation is the lack of objective assessment at home before the laboratory experiment. Nevertheless, no rebound of sleep (slow-wave sleep [N3]) appears during the night of PSG suggesting that the participants were not in sleep restriction during the previous nights.
In conclusion, this is the first study to show that not only the severity of an inhibitory control deficit but also the severity of objective sleepiness contribute independently to highway driving impairment in adults with ADHD. Our findings provide new insights into the pathophysiological mechanisms by which highway driving is disrupted in ADHD patients. A clinical evaluation of objective daytime sleepiness is a key element regarding driving risk in ADHD, a major public health issue. Further studies are needed to explore whether medications that promote wakefulness could improve the functional abilities of sleepy adults with ADHD.
Footnotes
Acknowledgements
We would like to thank Dr. Astrid Claret who participated in the inclusion of some patients.
Authors’ Note
This study was supported by a call from Bordeaux University Hospital (SOMTDAH CHUBX 2009/17).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.