
Abstract
Keywords
ADHD is associated with elevated rates of comorbid depression with roughly 16% to 31% of adults with ADHD also experiencing major depressive disorder (Barkley, Murphy, & Kwasnik, 1996; Biederman et al., 2008; Biederman et al., 1993; Kessler et al., 2006; Wilens, Nierenberg, Rostain, & Spencer, 2008). In their follow-up study with a large sample of hyperactive children, Barkley, Murphy, and Fischer (2008) found that 27% developed major depression by young adulthood. Chronis-Tuscano and colleagues (2010) found that 18.4% of children diagnosed with ADHD between ages 4 and 6 reported experiencing persistent depressive episodes by age 18 compared with 1.6% of children in a healthy control group. Similarly, lifetime history of ADHD assessed in adolescence predicted increased risk of major depressive disorder through age 30 (hazard ratio = 1.81; Meinzer et al., 2013). In a recent study, Meinzer and colleagues (2015) found that childhood ADHD predicted elevated depressive symptoms compared with non-ADHD controls. Other studies reveal similar findings, which support the idea that ADHD is a risk factor for depressive disorders.
While there is an overrepresentation of comorbid depression among individuals with ADHD, less is known about the nature and development of this comorbidity (Knouse & Safren, 2010). One of the few published studies examining predictors of depression in adults with ADHD identified both behavioral avoidance and dysfunctional cognitions as mediators of the relationship between ADHD and depressive symptoms (Knouse, Zvorsky, & Safren, 2013). That study framed the question in terms of risk for depression. However, not all adults with ADHD experience comorbid depression. Just as important is the question of resiliency, or protective factors. Resiliency may be defined as the capacity to maintain a positive outcome in the face of adversity. Importantly, for an individual’s trajectory to be considered “resilient,” he or she must be confronted with critical impediments to normative developmental processes (Masten, 2001). As a developmental disorder, ADHD is just such an impediment and adults with ADHD who do not experience depression may be considered resilient to that outcome. In Knouse and colleagues’ (2013) sample, 18% of adults with ADHD were resilient to developing any comorbid depressive disorder, despite significant ADHD symptoms and related impairments. An important question to address in light of these findings is what protective factors might differentiate this resilient group? The population of adults with ADHD who have not experienced a comorbid depressive disorder is an understudied group within ADHD-depression research and identifying protective factors that make an individual with ADHD resilient to depression could inform both prevention and intervention (Luthar, Cicchetti, & Becker, 2000).
Due to the high comorbidity of depression with ADHD, the chronic nature of ADHD, and the threat of depression to successful development, the current study conceptualized resiliency as an absence of lifetime depressive disorder in spite of ADHD diagnosis. Using data from Knouse et al. (2013), which looked at potential mechanisms of risk for depression comorbidity among adults with ADHD, the current study investigated the extent to which protective factors predicted resilience to depression among this sample as evidenced by membership in a “never depressed” group of adults with ADHD. We hypothesized that a longer period of past ADHD treatment would predict resilience to depression, as prior work indicates that treatment of ADHD earlier in development may be a protective factor for the development of later comorbidity (Daviss, Birmaher, Diler, & Mintz, 2008; Wilens, Faraone, Biederman, & Gunawardene, 2003). We also hypothesized that lower levels of maladaptive cognitive and behavioral coping strategies would increase the likelihood of lifetime resilience to depression given extant literature indicating that dysfunctional cognitions, avoidant coping, and ruminative responses may be risk factors for depression (Beck, 2008; Ottenbreit & Dobson, 2008; Wisco & Nolen-Hoeksema, 2008). We also hypothesized that more severe childhood and current ADHD symptoms would predict lower likelihood of lifetime resilience to comorbid depression. In addition, we explored age, gender, race/ethnicity, negative life events and socioeconomic status as predictors of resilience, although we did not make specific predictions about these factors.
Method
Participants
Participants in this study were 77 adults who met criteria for both childhood and current ADHD (see inclusion criteria below). In all, 43% of the sample was male, and the mean age was 38 years. Race, ascertained by self-report, was 85% White, 1.2% Black, 6.5% Multiracial, and 7.8% did not disclose this information, and 9% of the participants identified as Hispanic or Latino. Self-reported levels of education indicated that 22% of participants earned a high school diploma or General Educational Development (GED), 17% had an associate’s or technical school degree, 36% earned a bachelor’s degree, 17% had a master’s degree, and 8% had a doctoral, medical, or law degree. Thirty-four percent of participants were married or had a cohabiting partner, and 25% had children. Sixty-six percent of the sample was employed.
Inclusion criteria for the study were as follows: (a) diagnosis of ADHD by an outside provider, (b) between the ages of 18 and 65 years old, (c) reported at least six of nine current inattentive symptoms and/or six of nine current hyperactive-impulsive symptoms on a telephone screen version of the Diagnostic Interview Schedule for Children (DISC; Shaffer, Fisher, & Lucas, 1997), (d) reported experiencing impairment from ADHD symptoms before age 12, (e) met the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) threshold for ADHD in childhood by retrospective report on the Kiddie Schedule for Affective Disorders and Schizophrenia–Epidemiologic Version (K-SADS; Orvaschel, 1985), and (f) on the Adult ADHD Investigator Symptom Rating Scale (AISRS; Spencer et al., 2010) confirmed a minimum six of nine inattentive symptoms and/or six of nine current hyperactive-impulsive symptoms. Exclusion criteria were (a) major sensory or motor impairment; (b) major neurological condition; (c) current psychotic disorder, pervasive developmental disorder, mental retardation, or history of bipolar disorder; and (d) inability to complete interviews and self-report questionnaires in English.
Participants were recruited through referrals from other providers and research centers in the health system where the research was conducted, from qualified participants who had participated in previous ADHD studies in the same research program, from a database of patients expressing interest in ADHD research, and from advertisements on Craigslist. After a participant contacted the study, he or she completed the DISC telephone screening addressing inclusion and exclusion criteria. Participants who passed the screening were scheduled for a 3-hr visit at the research clinic. Of 85 participants who originally passed the telephone screening and attended the study visit, eight were subsequently excluded for the following reasons: Five did not meet childhood ADHD criteria on the K-SADS, one did not meet the current ADHD symptom threshold, one was found to have a psychotic disorder, and one was found to have a history of bipolar disorder. In addition, data from two participants’ self-report measures were incomplete. Participants received US$25 and validated parking for attending the visit. Moreover, participants were provided with information about resources for adults with ADHD, treatment referrals if appropriate, and an optional letter to a treatment provider of their choice outlining the diagnostic impression from the research assessment.
Measures
Diagnostic interviews
ADHD diagnosis in childhood was established using the K-SADS Structured Interview (Orvaschel, 1985). Patients were required to endorse at least six of nine inattentive and/or six of nine hyperactive-impulsive symptoms in childhood with two or more domains of impairment. The research version of the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I; First, Spitzer, Gibbon, & Williams, 1995) was used to determine whether patients met criteria for current or past depressive disorders. Modules from the clinician version of the SCID-I were also administered to assess the presence of comorbid bipolar, psychotic, anxiety, substance use, and eating disorders.
Clinician-administered symptom rating scales
The Adult AISRS (Spencer et al., 2010) evaluated present ADHD symptoms. Participants were required to endorse at least six of nine inattentive and/or six of nine hyperactive-impulsive symptoms on both this measure and the telephone screen for inclusion in the study. In administering the AISRS, the clinician rates the severity of each of the DSM-IV symptoms on a 4-point scale from none (0) to severe (3). The AISRS outlines suggested prompts for the interviewer to use to acquire the information required to rate each item, and are embedded in the scale itself. Internal consistency was good (α = .85).
Stressful life events
Stressful life events were assessed in an interview version of the Psychiatric Epidemiological Research Institute (PERI) Life Events Inventory (Dohrenwend, Askenasy, Krasnoff, & Dohrenwend, 1978). The PERI evaluates the rate of 102 stressful life events in 10 areas within the past year. Each stressful life event is scored based on ratings from a normative sample. A total score for negative life events was used in the analysis.
Self-report questionnaires
Current ADHD symptom severity was measured by the Current Symptoms Scale (CSS; Barkley & Murphy, 2006). The CSS prompts participants to rate the occurrence of each of the DSM-IV items on a 4-point scale (0 = never or rarely to 3 = very often). Internal consistency in this sample was good (α = .86). Current depressive symptom severity, measured using the 21-item Beck Depression Inventory (BDI; Beck, Ward, Mendelson, Mock, & Erbaugh, 1961), had excellent internal consistency (α = .92). Dysfunctional beliefs were measured using the 40-item version of the Dysfunctional Attitudes Scale (DAS; Beck, Brown, Steer, & Weissman, 1991). Participants ranked each statement on a Likert-type scale from totally agree to totally disagree. Lower scores on the DAS indicate greater agreement with dysfunctional beliefs. Avoidance was assessed using the Cognitive-Behavioral Avoidance Scale (CBAS; Ottenbreit & Dobson, 2004). Participants read 31 statements providing ways that a person might deal with real-life situations. They were asked to rate how true the statement is for how they would typically respond (1 = not at all true for me to 5 = extremely true for me). The items span cognitive/behavioral and social/nonsocial dimensions of avoidance. Internal consistency of the DAS and CBAS in this sample was excellent (both αs = .94). Negative automatic thoughts were measured using the Automatic Thoughts Questionnaire (ATQ; Hollon & Kendall, 1980), which asks participants to mark on a 5-point scale (0 = not at all to 4 = all the time) how frequently a given thought occurred to them over the last week. The ATQ maintained excellent internal consistency (α = .98). Anxiety symptoms were measured using the Beck Anxiety Inventory (BAI; Beck & Steer, 1993), which prompts participants to designate how much they have been troubled by a particular symptom during the past week. Participants rated their response on a 0 to 3 scale (0 = not at all to 3 = severely). Internal consistency was good (α = .85). Ruminative thoughts were measured using the Ruminative Response Scale (RRS; Treynor, Gonzalez, & Nolen-Hoeksema, 2003). The RRS asks patients to rate on a 4-point scale (0 = never to 3 = always) how often they think or do each listed item when they feel sad or depressed. The RRS maintained excelled internal consistency (α = .93). Finally, participants approximated in years the total length of time they had received treatment (defined as any modality) for ADHD in their entire lifetime.
Procedure
All study procedures were reviewed and approved by the Institutional Review Board at Massachusetts General Hospital. Participants first completed informed consent procedures and signed the approved consent form. The clinician administered the K-SADS structured interview followed by the AISRS, the PERI Life Events Scale, and the SCID-I depressive disorder and other modules. Participants completed self-report measures on a laptop computer via the Questionnaire Development System software. Participants completed all of these measures on the computer following the interview portion of the visit.
Plan of Analysis
We used a three-step analytic strategy to identify factors associated with resilience to depression in our participants. Each step listed below is an increasingly rigorous test of possible relationships between predictors and resilience to depression (see Figure 1 for additional explanation and graphical representation of the analytic strategy):
We used logistic regression to determine whether each independent variable predicted membership in the group of participants who never met criteria for depression (group labeled “Resilient” in Figure 1) versus those with current or past (lifetime) depression (all participants represented in the “Depression” column in Figure 1). Independent variables for each analysis were as follows: severity of childhood ADHD symptoms (K-SADS), severity of current ADHD symptoms (AISRS and CSS) dysfunctional attitudes (DAS), negative automatic thoughts (ATQ), rumination in response to sad moods (RRS), avoidant cognitive and behavioral coping strategies (CBAS), years of past ADHD treatment, age, gender, race/ethnicity, socioeconomic status, stressful events in the past year (PERI), and substance abuse and comorbid anxiety disorders. In each analysis, we controlled for current ADHD symptom severity as measured by the AISRS and gender but no differences in outcomes were noted. Thus, we report results without these covariates.
For variables that significantly predicted resilience versus lifetime depression in Step 1, we repeated logistic regression analyses only among participants who were not currently depressed (n = 37 past depressive disorder only; n = 14 no history of depressive disorder). In other words, we tested whether each independent variable predicted membership in the group of participants who never met criteria for depression (group labeled “Resilient” in Figure 1) versus those with past depression only (all participants represented in the top portion of the “Depression” column in Figure 1). We did this to rule out the possibility that the inclusion of currently depressed participants was driving results observed in Step 1. Again, we controlled for ADHD symptom severity and gender in each analysis and they had no effect, and thus results without covariates are reported.
For predictors surviving Steps 1 and 2, we repeated the logistic regression analysis in Step 2 controlling for current depressive symptoms as measured by the BDI. We did this to further ensure that observed relationships with lifetime depression could not be accounted for by any current subthreshold depressive symptoms.
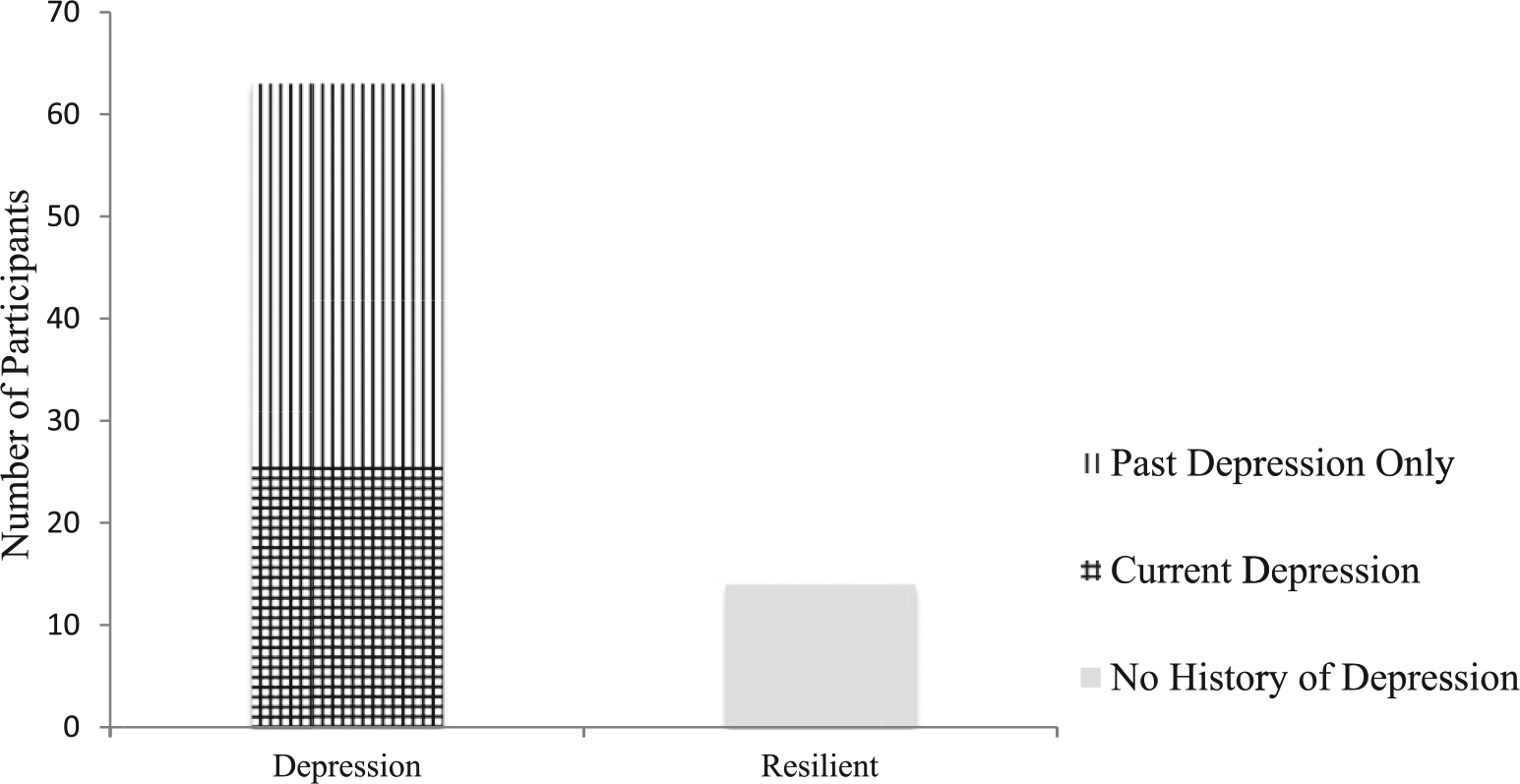
Participants by depression group.
We used ORs to capture the association between each potential predictor and resilience to depression. We report the regression coefficient (b), as a parameter estimate of the increase in the log odds of resilience to depression occurring per unit increase in the value of the potential predictor.
Results
Descriptive Statistics
Table 1 illustrates the overall descriptive statistics for the predictor variables we investigated. Table 2 reports descriptive statistics for significant predictors at Step 1 (see “Plan of Analysis” section) separately for each of three groups of adults with ADHD—resilient (n = 14), past depressive disorder only (n = 37), and current depressive disorder (n = 26). Note, however, that our analyses predicted group membership and did not involve comparing the mean scores on these measures across groups and that these descriptive statistics are provided for illustrative purposes only.
Descriptive Statistics for Predictors and Covariates in Logistic Regression Analyses.

Note. BDI = Beck Depression Inventory; PERI = Psychiatric Epidemiological Research Institute; K-SADS = Kiddie Schedule for Affective Disorders and Schizophrenia; AISRS = Adult ADHD Investigator Symptom Rating Scale; CSS = Current Symptom Scale (ADHD symptom self-report); ATQ = Automatic Thoughts Questionnaire; DAS = Dysfunctional Attitudes Scale; CBAS = Cognitive-Behavioral Avoidance Scale; RRS = Ruminative Response Scale.
Descriptive Statistics for Significant Predictors at Step 1 by Depression Status Group.
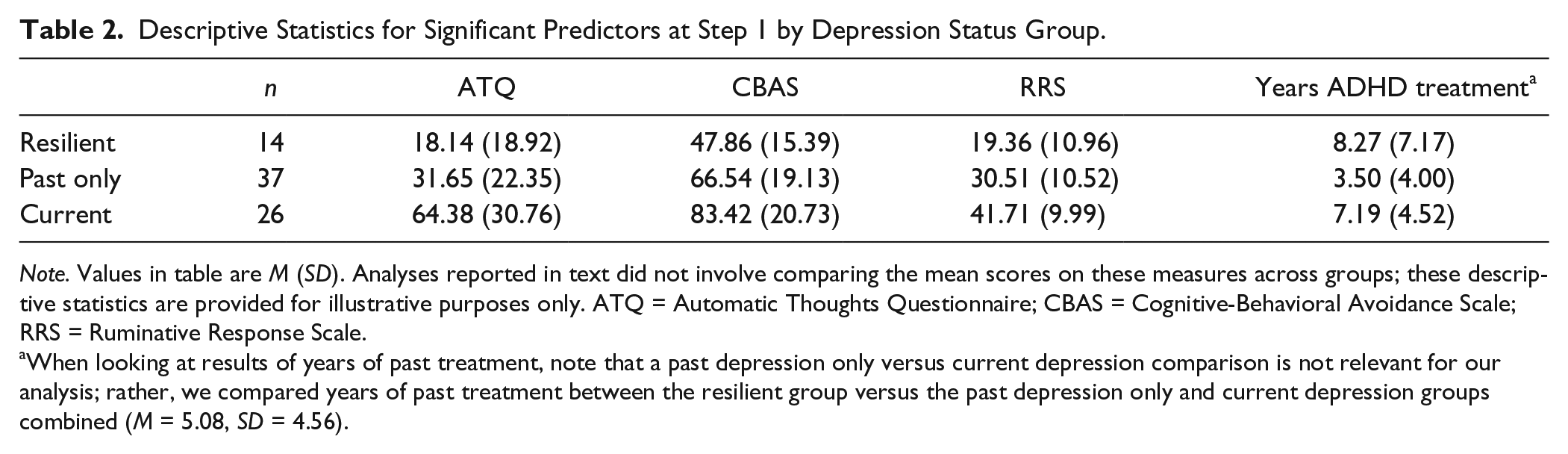
Note. Values in table are M (SD). Analyses reported in text did not involve comparing the mean scores on these measures across groups; these descriptive statistics are provided for illustrative purposes only. ATQ = Automatic Thoughts Questionnaire; CBAS = Cognitive-Behavioral Avoidance Scale; RRS = Ruminative Response Scale.
When looking at results of years of past treatment, note that a past depression only versus current depression comparison is not relevant for our analysis; rather, we compared years of past treatment between the resilient group versus the past depression only and current depression groups combined (M = 5.08, SD = 4.56).
Logistic Regression Results
Below, we present results from the series of logistic regression analyses described in the “Plan of Analysis” section, grouping our results according to each predictor of resilience.
Predictors: Demographics and life events
Age, socioeconomic status (Hollingshead, 1975), as well as stressful life events in the past year (PERI Negative Event score) were not significant predictors of lifetime depression in the entire sample (Step 1 in “Plan of Analysis” section). In a chi-square analysis, the categorical independent variables of gender and race (coded as Black, White, Biracial, and Other) were not significant predictors of lifetime depression.
Predictors: Severity of ADHD symptoms
We conducted separate logistic regression analyses using total childhood ADHD symptom scores from the K-SADS, current symptom scores from the self-report CSS, and current symptoms from the AISRS. We also tested hyperactive-impulsive and inattentive symptom scores separately for both CSS and AISRS measures as possible predictors of lifetime depression. None of these measures of symptom severity significantly predicted lifetime resiliency to depression.
Predictors: Cognitive and behavioral coping
Frequency of negative automatic thoughts as measured by the ATQ was found to be a significant predictor of lifetime depression versus no history of depression in adults with ADHD (b = .05, OR = 1.05, p = .008). Thus, lower self-reported frequency of automatic negative thoughts was associated with lifetime resiliency to depression. However, when we tested ATQ as a predictor of past depression only versus resilience (Step 2), the results of the logistic regression analysis were marginally significant (b = .04, OR = 1.04, p = .06). When BDI score was entered first into this logistic regression analysis (Step 3), ATQ was no longer a significant predictor (b = .04, OR = 1.04, p = .15). Dysfunctional attitudes measured using the DAS were also tested as predictors of lifetime resilience but results were not significant.
Cognitive and behavioral avoidant coping as measured by the CBAS was a significant predictor of lifetime depression (b = .08, OR = 1.08, p = .001). In addition, results in the sample of those not currently depressed were significant (b = .07, OR = 1.07, p = .005). Finally, when BDI was initially entered into this analysis, CBAS remained a significant predictor (b = .60, OR = 1.06, p = .01). Thus, a less avoidant coping style was associated with resilience to depression above and beyond current depressive symptoms.
We measured ruminative responses using the RRS, and found that it too was a significant predictor of lifetime depression among all participants in our sample (b = .13, OR = 1.14, p = .001) and among participants who were not experiencing depression at the time of the study (B = .11, OR = 1.11, p = .01). To control for depressive symptoms further, when BDI was first entered into our logistic regression analysis (b = .14, OR = 1.14, p = .02), RRS remained a significant predictor (b = .1, OR = 1.10, p = .01). Participants who reported being less likely to ruminate in response to sad moods were less likely to have experienced a depressive episode in their lifetimes.
Years of past treatment for ADHD
We analyzed participants’ self-reported years of past treatment for their ADHD as a predictor of lifetime depression. Results in the entire sample were significant (b = −.11, OR = 0.90, p = .049) and suggest that the more years of past treatment for ADHD a participant has received, the less likely he or she had experienced a comorbid depressive disorder. Results were also significant (b = −.16, OR = 0.85, p = .014) among adults with ADHD who were not currently depressed and remained so when controlling for current depressive symptoms (b = −.14, OR = 0.87, p = .04). Participants who had more years of treatment for their ADHD were more likely to have maintained resiliency to comorbid depression despite their ADHD.
Discussion
Our results identify potential protective factors which may promote resilience to developing comorbid depression among adults with ADHD. We found that adults with ADHD who are less engaged in ruminative thinking patterns and cognitive-behavioral avoidance when feeling sad and those with more extensive ADHD treatment histories were more likely to be resilient to depression comorbidity. Furthermore, predictors that might be expected to increase risk for depression—severity of recent negative life events and severity of ADHD symptoms—were not predictors of resilience in this sample.
Consistent with the broader depression literature, specific behavioral and cognitive coping factors were significant predictors of ADHD and depression comorbidity. Participants’ self-reported tendency to ruminate when feeling depressed and the extent to which they reported coping with stressors by cognitive and behavioral avoidance were significantly related to depression-ADHD comorbidity—even among participants who were not currently depressed and when accounting for any subclinical depression symptoms. Our results are consistent with extensive prior research showing that the tendency to respond to depressed moods by ruminating is a risk factor for depression (Nolen-Hoeksema, 2000). Rumination is associated with more negative cognitive bias, impaired concentration, and inhibition of adaptive coping behavior and interpersonal problem solving (Wisco & Nolen-Hoeksema, 2008). Relatedly, an avoidance-motivated coping style itself is a hallmark of depression whereby adults respond to stressors in ways which enable them to escape immediate negative affect rather than resolving problems long term, which also reduces access to possible sources of reinforcement (Ferster, 1973; Ottenbreit & Dobson, 2004). Rehashing negative events and avoiding uncomfortable situations are behaviors that may lead to depression and lower levels of these responses may constitute protective factors to ADHD-depression comorbidity.
Duration of past treatment for ADHD was also associated with resilience to depression. Our findings are consistent with the idea that treatment of ADHD earlier in development may limit later comorbidity. Some studies suggest this may also be true for later substance use problems (Wilens et al., 2003). Likewise, preliminary research indicates that pharmacotherapy for adolescents with ADHD may have a protective effect against subsequent major depressive disorder (Daviss et al., 2008). Our results also support the notion that given the long-term chronicity of ADHD, longer lasting management of ADHD symptoms via treatment may have a protective effect for later depression comorbidity. Comprehensive treatment that is informed by an understanding of the protective mechanisms that constitute resiliency to comorbid depression (e.g., active coping) may prevent depression among adults with ADHD. Notably, empirically supported cognitive-behavioral treatments for adult ADHD teach clients active coping skills to compensate for ADHD-related deficits (Safren, Perlman, Sprich, & Otto, 2005; Solanto, 2011), which are consistent with cognitive-behavioral approaches to depression. Future studies should examine whether skills-based treatments for ADHD have an impact on subsequent resilience to depression as well.
Interestingly, while our measure of automatic negative thoughts survived initial logistic regression analyses, it was not a significant predictor of lifetime depression in adults who were not currently depressed. In addition, the measure of dysfunctional attitudes was not a significant predictor of resilience. Notably, these instruments measure the content of participants’ thoughts. In contrast, the RRS, which was found to be a significant predictor of lifetime depression in adults not currently diagnosed with depression, measures the frequency of ruminative processes. Because ruminative thought process may serve an avoidance function (Wisco & Nolen-Hoeksema, 2008), this result is consistent with our findings for cognitive and behavioral avoidance. Thus, as supported by prior depression literature (Jacobson, Martell, & Dimidjian, 2001), the content of thoughts may be less clinically important than a focus on the function of ways of thinking and behaving when working with adults with ADHD at risk for depression. Clinicians may wish to address ruminative response styles and avoidant coping in their clients with ADHD rather than targeting negative content per se (Knouse & Mitchell, 2015).
While we hypothesized that severity of ADHD symptoms would predict risk for depression co-occurrence, our analysis of severity of ADHD symptoms did not yield significant results. Further research is needed to investigate whether this finding is reliable and replicable. It may be the case that the cardinal symptoms of ADHD (e.g., inattention and hyperactivity/impulsivity) do not necessarily drive the relationship between ADHD and depression. Instead, it is quite possible that the associated impairment resulting from these symptoms accounts for the increased prevalence of depression among adults with ADHD. Of interest, given that anxiety disorders were not exclusionary, and negative thoughts and avoidance are often symptoms of anxiety conditions, our findings may offer potential fodder for research on factors that might promote resilience to comorbid anxiety disorders. Furthermore, anxiety and anxiety disorders themselves may also be possible mediators between ADHD and risk for depression—a question that warrants further study.
Notably, our cross-sectional results will need to be replicated in prospective longitudinal studies to further support the idea that protective factors at Time 1 lead to beneficial outcomes at Time 2. Although our analyses controlled for the possible influence of concurrent depressive symptoms (i.e., BDI score) on candidate protective factors, we cannot rule out the possibility that past depression accounted for, for example, lingering avoidant coping styles rather than the idea that these vulnerability factors were present from an earlier time point. Note, however, that the years of past ADHD treatment variable is less vulnerable to this particular interpretational difficulty. Importantly, our results cannot necessarily be generalized to the population at large because our sample did not have a high degree of racial and ethnic diversity. Additional research should incorporate racially and ethnically diverse populations. Finally, given that bipolar disorder was an exclusion criterion, our results do not necessarily extend to the depressive phases of the disorder and our findings should be interpreted accordingly.
While we know there is an increased risk for depression in adults with ADHD, less is known about the underlying factors that promote resiliency to depression in this population. Longer duration of ADHD treatment and lower levels of both self-reported rumination when feeling depressed and coping with stressors through avoidance were significantly related to lifetime resilience to depression among adults with ADHD—even among those not currently depressed. Prospective studies are needed to further investigate causal relationships among these factors. However, given that the broader depression literature provides strong support for these processes in the development of depression, clinicians should consider working to bolster active coping skills to prevent depression in people with ADHD.
Footnotes
Author Note
Ms. Oddo is now in the Department of Psychology at Virginia Commonwealth University, 806 West Franklin Street, Richmond, VA 23284, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ms. Oddo was supported by a University of Richmond Undergardaute Summer Research Fellowship and Dr. Knouse was funded by a University of Richmond Faculty Summer Research Fellowship.