
Abstract
The number of students in colleges and universities who have been diagnosed with attention deficit disorder or attention deficity hyperactivity disorder (ADD/ADHD) has been found to be increasing (Weyandt & DuPaul, 2010). Moreover, the inattention, hyperactivity, and impulsivity that result from ADD/ADHD were found to interfere seriously with an individual’s experience and success in academic environments (American Psychiatric Association, 2013). The most commonly used treatments to address these problems have been psychopharmaceutical drugs (i.e., stimulants), but medication of any kind can only be effective when adhered to. In the present study, we examined the adherence behaviors and the beliefs of students regarding these medications. We proposed here that a better understanding of how students choose to over- and under-adhere to their prescribed medication is necessary to provide appropriate support for these students as they progress through college or university.
Psychopharmaceutical drugs, such as methylphenidate (Concerta, Ritalin) and dextroamphetamine/amphetamine (Adderall), have been frequently prescribed to people with ADD/ADHD. The effectiveness of stimulants has been found to be lower for adults than children, with an effectiveness rate of only 50% for adults (Davidson, 2007; Greenhill, Pliszka, & Dulcan, 2002; Wilens, Spencer, & Biederman, 2000), although Safren, Duran, Yovel, Perlman, and Sprich (2007) suggested that the lower levels of effectiveness for stimulants in adults might be due to lower adherence rates. Non-adherence, or not following the instructions outlined by a prescriber, can be either intentional/purposeful (taking more or less medication than was prescribed with the intention and awareness of doing so) or unintentional (forgetting to take a medication or forgetting it was already taken that day; Lehane & McCarthy, 2007). It has been suggested that compared with children or working adults, there are some aspects of college students’ lifestyles that may make adherence particularly challenging. Extended and often irregular class and study hours may not have been accommodated by typical 4- to 6-hr fast-release tablets or 8-hr slow-release tablets (Green & Rabiner, 2012; The Physician’s Desk Reference Family Guide to Prescription Drugs, 2000). Moreover, the co-existing demands of detailed cognitive work, creative productive work, and social interaction that were required for group work may also have been challenging if medication was experienced as prioritizing some activities over others.
Pillow, Naylor, and Malone (2014) conducted perhaps the most comprehensive study on the topic of the effects of beliefs on adherence to ADHD medication in college age adults. Using Ajzen’s (1991) Theory of Planned Behavior, the authors sought to determine the influence that beliefs and attitudes, as well as subjective norms and perceived control, have on the choice to continue taking or to stop taking prescribed stimulant medication for the treatment of ADHD. The authors looked specifically at a sample of college students, between the ages of 18 and 28. These participants were divided into those who had stopped taking their prescribed medication and those who were continuing to take their medication as prescribed. Beliefs about the medication were divided into four main areas: (a) improved attention/academics (IAA), (b) loss of authentic self (LAS), (c) social self-enhancement (SSE), and (d) common side effects (CSE; Pillow et al., 2014).
Pillow et al. (2014) found that, similar to past research (McCarthy, 2014), the use of stimulant medication was seen as a trade-off, where the user is constantly balancing perceived costs and benefits. Participants who were currently taking medication believed that taking the medication would result in IAA and SSE. Those who had stopped taking their prescribed medication believed more strongly that medication would result in an LAS. That being said, if it was believed that IAA would result from medication use, some beliefs about LAS would be weighed as a trade-off, resulting in those participants continuing to take their medication. Current users were also found to have higher levels of perceived control and greater positive subjective norms than past users.
One potential weakness of the Pillow et al. (2014) study is that comparisons are made only between past and current users of medication, and no attention is paid to when and how much medication current users are taking. Whereas the topic of college students misusing stimulant medication to get high (i.e., overuse) has received increasing attention (e.g., Rabiner et al., 2009), relatively little is known about adherence rates of adults with ADD/ADHD (Caisley & Müller, 2012). However, it is widely acknowledged that many adults are frequently adjusting their medication frequency and dosages rather than following the prescribed regimen, and a better understanding of the experiences of these individuals is needed (Caisley & Müller, 2012).
The present study attempted to replicate and extend the findings of Pillow et al. (2014). We proposed here that it was important not only to distinguish between individuals who chose to take medication as prescribed and people who do not take any medication at all but also to include individuals who were partially adherent. Based on past findings (e.g., Knipp, 2006; Pillow et al., 2014) that medication was perceived as helpful for academic work but detrimental to the expression of the authentic self, we compared adherence on weekdays (when academic demands are highest) to weekends (when academic demands were reduced). We proposed that it was helpful to look at the day-to-day self-management of medication to understand what drives the decision to reduce or omit medications on weekdays and weekends during an academic semester. Specifically, we hypothesized that students would be more likely to take their medication on weekdays than on weekends, and that this difference would be driven by their beliefs and attitudes about the medication, rather than by unintentional non-adherence.
Method
Participants
The 53 participants were students from a small undergraduate liberal arts university in eastern Canada who reported having received a formal diagnosis of ADD or ADHD. All participants had been prescribed medication to treat ADD/ADHD. Medications prescribed included methylphenidate (Concerta, 26.4%; Ritalin, 13.2%), amphetamines (Adderall, 15.1%; Vyvanse, 13.2%; Dexedrine, 2%; Straterra, 4%), with 20.8% of the sample taking multiple stimulants to treat their condition, and 5.7% of the sample not answering this question.
There were 17 (32.1%) male and 36 (67.9%) female students in the sample. (The gender ratio for the entire campus at time of testing was 42% male and 58% female.) Whereas 45.3% of the students were in their first or second year of university, 45.3% were in their third or fourth year, and a further 9.4% students were in year 5 or more of a usually 4-year degree. On average, participants had received their diagnosis of ADHD at age 14.73 (SD = 4.94 years, range = 5-27 years). A majority of participants had been taking medication to treat ADHD for more than 2 years (53.8%) and had begun treatment before coming to university (60.4%). Using a 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree), participants were, on average, neutral in terms of whether it was difficult to obtain medical care for their condition in the small town where the college is located (M = 4.12, s = 1.78) and whether taking medication was too expensive while in school (M = 3.2, SD = 1.75).
Measures
The demographic information requested included gender, year of study, age of ADD/ADHD diagnosis, type of medication(s) prescribed, how long the medication had been used, and whether medication use had begun before attending university.
Four questions were used to measure adherence to gather information about past and future/intended behavior on both weekdays and weekends: Participants were asked whether they took/intended to take all their medications as prescribed (a) last Tuesday, (b) last Saturday, (c) next Tuesday, and (d) next Saturday. For each time, participants indicated whether they had (a) taken all their medication as prescribed, (b) taken only some of their medication, or (c) taken no medication. Purposeful non-adherence was also measured by asking participants to report how frequently they did not take medication “on purpose,” and unintentional non-adherence was measured by asking participants how frequently they did not take their medication because of forgetting, both on scales ranging from 1 (never) to 7 (everyday).
The beliefs participants held about prescription stimulant medication was measured using 40 items from the 50 items proposed during scale development by Pillow et al. (2014). Each item was measured on a 7-point scale ranging from 1 (very unlikely) to 7 (very likely). We calculated the Cronbach’s α if each item was deleted, and dropped the items that reduced the reliability of the scales to create four 10-item scales: (a) IAA (Cronbach’s α = .89), (b) LAS (Cronbach’s α = .88 with 2 items reverse coded), (c) SSE (Cronbach’s α = .83 with 1 item reverse coded), and (d) CSE (Cronbach’s α = .86). (Cronbach’s α for the scales in Pillow et al. were .92, .89, .90, and .83 for IAA, LAS, SSE, and CSE, respectively.) The degree to which participants judged the measured beliefs to be good or bad was also recorded.
Based off of Pillow et al.’s (2014) instrument, a measure of the perceived subjective norms of a wide range of individuals who may interact with participants was given, specifically, parents, siblings, romantic partners, best friend, classmate, physician, professors, boss, coworker, and mentor. After preliminary analyses, only the individuals who were relevant for a majority of the sample were included in analyses, namely, parents, siblings, best friend, and physician. For each person, the participant rated on a 7-point scale whether this person thought or did not think that the participant should take their ADD/ADHD medication. The participant’s desire to do what this person wanted them to do was also recorded on a 7-point scale.
Perceived behavioral control of ADD/ADHD was measured by asking participants to rate, using a 7-point scale, (a) whether they believe the condition is a biological health problem, (b) whether they believe the best way to treat symptoms is with medical care, (c) whether they believe that the symptoms are personality traits that do not need medical treatment, (d) whether it is difficult to obtain medical treatment for the condition in the university community, and (e) whether it is difficult to afford the price of the medication while in school.
Procedure
Participants were recruited from the student body via social media, the use of posters, and, most frequently, through the disability support center located on campus. This center provides services to approximately 135 students with documented diagnoses of learning disabilities and/or ADD/ADHD. All students receiving services received an email invitation to participate in an online study measuring beliefs about medication used in the treatment of ADD/ADHD. The email stated that the study was open to anyone who had a diagnosis of ADD/ADHD and had received a prescription for medication to treat this condition. We used an online survey form (via FluidSurveys), and students could complete the approximately 10-min survey at a time of their choosing. The online survey tool began with the informed consent process and ended with contact information for the researchers and the campus disability support services. Recruitment and data collection was carried out during the winter of 2015.
Results
Overall Adherence Rates
As a first set of analyses, we compared self-reported adherence and intention to adhere for four times: last Saturday, last Tuesday, next Saturday, and next Tuesday. For each time, participants rated whether they had taken all their medications as prescribed, some of their medications, or no medications. Response frequencies are presented in Table 1. Given the ordinal nature of our measure, we used the non-parametric Friedman’s test for repeated measures to compare the ranks across the four times. (Parallel parametric tests were also run and yielded equivalent results.) The ranks for the adherence rates varied significantly, with the highest adherence for next Tuesday (ranks = 2.20), followed by last Tuesday (ranks = 2.24), next Saturday (ranks = 2.67), and last Saturday (ranks = 2.89). A series of follow-up pair-wise Wilcoxon tests showed that students report being more adherent to their medications on weekdays than weekends for both the previous week (p < .001) and the coming week (p = .002), and they intend to be more adherent next Saturday than last Saturday (p = .03). Finally, they do not intend to be more adherent next Tuesday than they were last Tuesday (p = .414).
Adherence Rates.
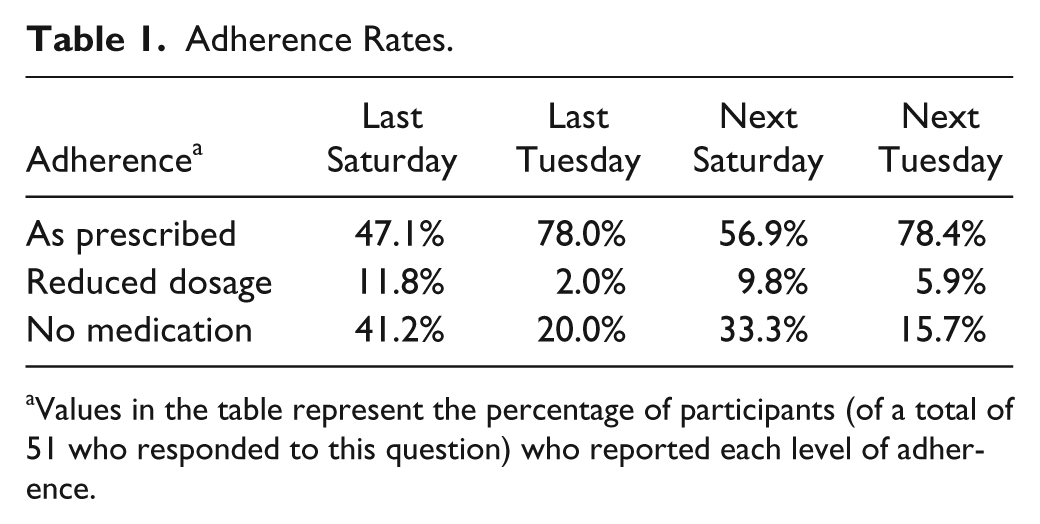
Values in the table represent the percentage of participants (of a total of 51 who responded to this question) who reported each level of adherence.
Given the mixed results concerning the comparison of future intentions and past behavior, it is likely that non-adherence occurs due to planned behavior, rather than forgetting. This conclusion is supported by the strong relationship between the purposive non-adherence question and non-adherence last Saturday (r = .43, p < .001), and last Tuesday (r = .36, p = .013). In contrast, the correlations between missing medication due to forgetting and non-adherence last Saturday (r = .19, p = .19) and last Tuesday (r = .07, p = .63) were relatively small.
Beliefs and Adherence
Ratings on a 7-point scale indicated that overall, students believed that ADD/ADHD is a biological health problem (M = 5.74, SD = 1.52), where medical care was the best treatment (M = 5.15, SD = 1.42) rather than a personality trait that did not require medication (M = 2.43, SD = 1.45). The stronger the belief that ADD/ADHD is a biological health problem, the less likely the student was to be non-adherent (Spearman correlations ranging from −.44, p = .005, to −.37, p = .02, across the four times of measurement). In contrast, people who strongly believe that the symptoms of the condition are personality traits that do not require medication are more likely to be non-adherent (Spearman correlations ranging from .42, p = .007, to .28, p = .08, across the four times of measurement).
The inter-correlations between the four belief scales are shown in Table 2. As can be seen, SSE is highly correlated with both improved academic achievement (IAA) and with LAS. CSE is correlated only with LAS. Finally, IAA and LAS are not related. To look at the relationship between scores on each belief scale (IAA, LAS, SSE, and CSE), we combined the adherence self-ratings for the two weekday ratings and then for the two weekend ratings, and created binary measures for each. Thus, given the small number of individuals who were partially adherent, particularly on weekdays, we collapsed two categories and identified one group of individuals who took all their medications as prescribed (the adherent group), and a second group who took no medication or less medication than prescribed (the non-adherent group) on those 2 days. We then carried out a series of t tests comparing the means of these two groups on the four belief scales. These results are shown in Table 3. (Because of missing data, the number of people included in each analysis varies.) Results show that on weekdays, SSE, LAS, and to some extent IAA are all important in determining whether one is adherent or not. In contrast, on weekends, neither IAA nor SSE is significantly related to adherence status, though it should be noted that SSE has a medium effect (η2 = .07) and may have reached significance with a larger sample.
Pearson Correlations Showing Relationship Between Belief Scales.
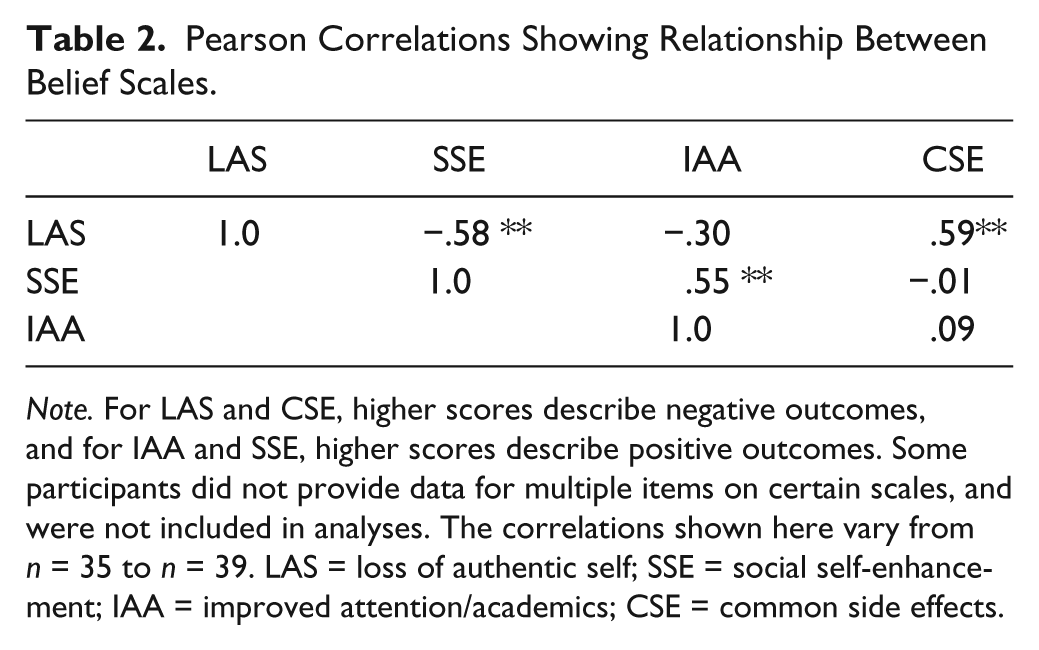
Note. For LAS and CSE, higher scores describe negative outcomes, and for IAA and SSE, higher scores describe positive outcomes. Some participants did not provide data for multiple items on certain scales, and were not included in analyses. The correlations shown here vary from n = 35 to n = 39. LAS = loss of authentic self; SSE = social self-enhancement; IAA = improved attention/academics; CSE = common side effects.
Comparing Adherence Groups on Beliefs About Medication Outcomes.
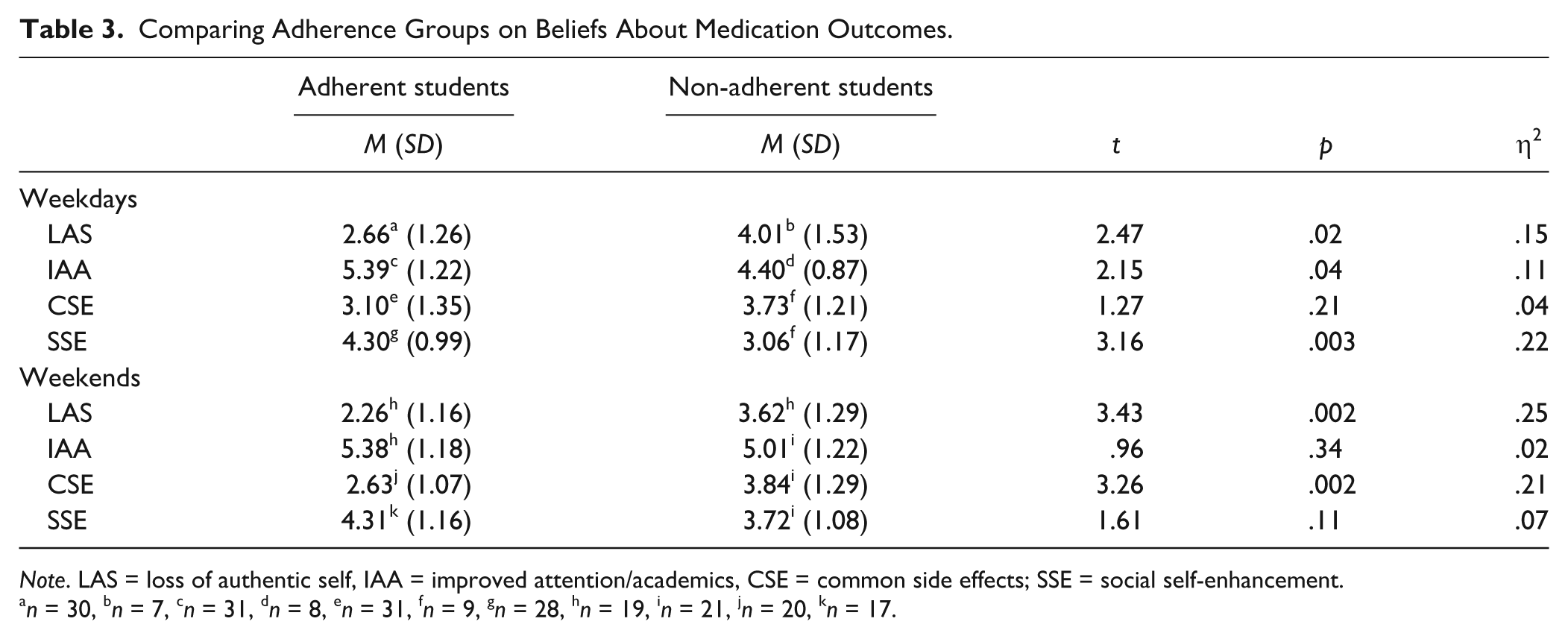
Note. LAS = loss of authentic self, IAA = improved attention/academics, CSE = common side effects; SSE = social self-enhancement.
n = 30, bn = 7, cn = 31, dn = 8, en = 31, fn = 9, gn = 28, hn = 19, in = 21, jn = 20, kn = 17.
Subjective Norms
Participants were asked to rate their perception of how much different people in their lives wanted them to take their medication as prescribed, and then rated whether they wished to follow these people’s recommendations. Of the categories of people rated, there were five categories that were relevant for at least 30 participants: Parent 1, Parent 2, sibling, best friend, and doctor/physician. Because the correlation between Parents 1 and 2 was very high (r = .75), we used only the rating for Parent 1 for subsequent analyses. Table 4 presents the results of a series of t tests comparing the adherent and non-adherent groups. Because most of the means are positive, this indicates that others were viewed on average as wanting the student to take medication, and students were relatively willing to follow these recommendations. On weekdays, the adherent and non-adherent groups were particularly different in terms of their perception of their siblings and their physicians’ opinions. In contrast, on weekends, the adherent group perceived parents, siblings, best friends, and physicians as being more positive about medication taking than did non-adherent students, but when weighted views were compared, only ratings of parents and physicians’ views were significantly different between the two groups of students. (However, effect sizes for both sibling [η2 = .08] and friend [η2 = .11] are relatively large, and may have been significant with a larger sample.)
Comparing Adherence Groups on Perceived Views and Weighted Views of Important Others.
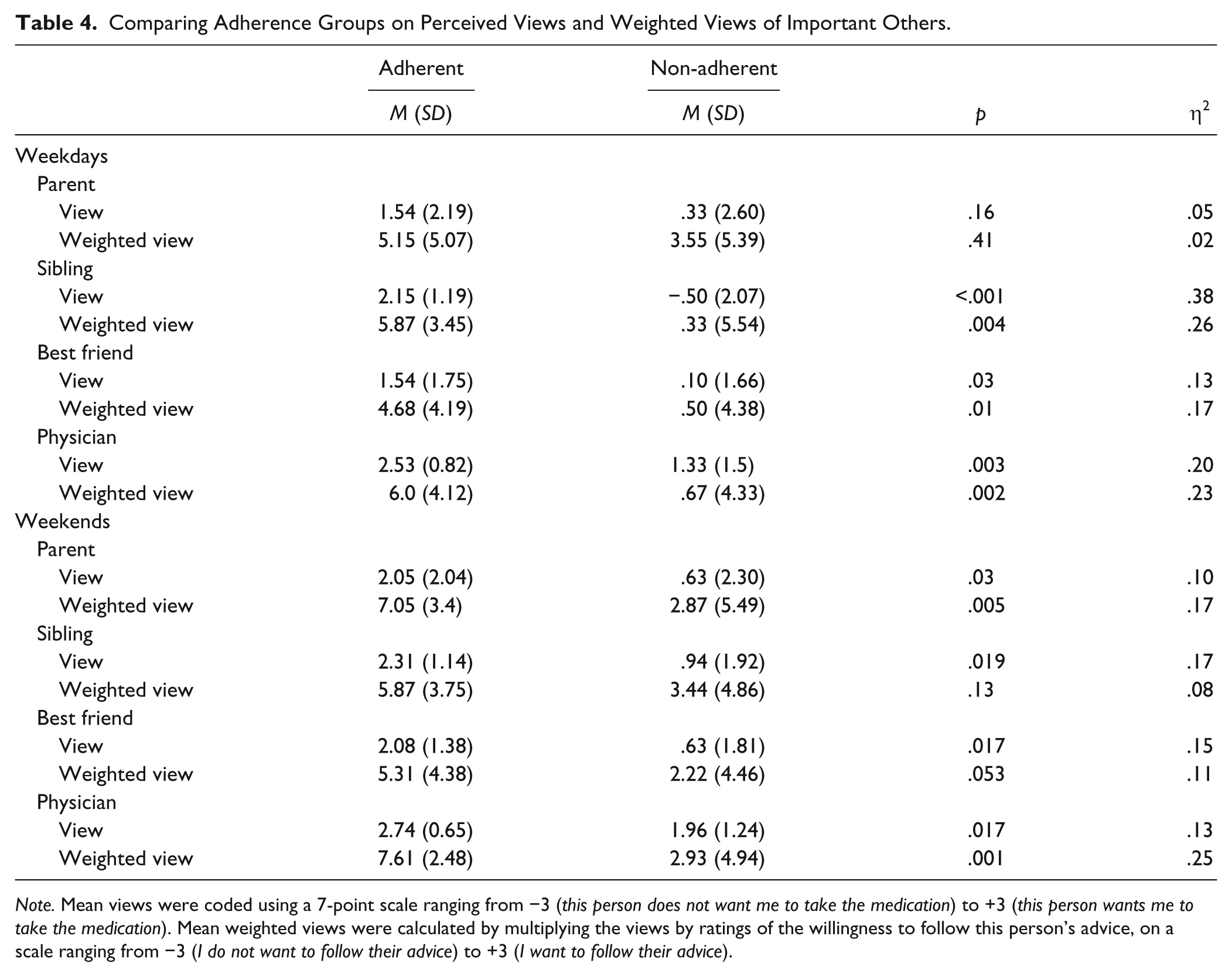
Note. Mean views were coded using a 7-point scale ranging from −3 (this person does not want me to take the medication) to +3 (this person wants me to take the medication). Mean weighted views were calculated by multiplying the views by ratings of the willingness to follow this person’s advice, on a scale ranging from −3 (I do not want to follow their advice) to +3 (I want to follow their advice).
Discussion
Past research has clearly established that many college students medicated for ADD/ADHD are not taking their medication as prescribed. By asking participants to rate their adherence on both weekdays and weekends, both past and future, we were able to extend these findings in interesting ways. First, we established that students are more likely to be adherent on weekdays than weekends, and there is a tendency to anticipate higher rates of adherence for the upcoming weekend than the past weekend. At first glance, these results could be due to weekend schedules being less routine leading to more forgetting. However, correlations between adherence levels and participants’ self-ratings of why they miss medication dosages suggest strongly that students are actively managing their medication intake (as proposed by Caisley & Müller, 2012), rather than simply forgetting dosages. For the most part, when they take less medication than prescribed, it is because they choose to do so—not because they forgot or because this was recommended by their physician.
In follow-up analyses, we investigated the role of beliefs in deciding whether or not to take medication as prescribed. We had expected that students who took their medication as prescribed (particularly on weekdays) would do so mostly because they believed the medication would lead to enhanced academic performance (IAA). Although this was true, the belief that the medication improved social skills (SSE) and did not lead to an LAS was also significant. A different pattern of results was obtained on weekends where the belief that the medication leads to an LAS and to side effects (CSE) distinguish the adherent and non-adherent groups.
In interpreting these results, two main issues should be recognized. The first is the relationships between SSE and the other four types of beliefs associated with the medication. The belief that the medication improves social skills (SSE) tended to co-occur with (a) the belief that it did not lead to a loss of self (LAS) and (b) the belief that it improves academic performance (IAA). These findings might point to the particularly social and collaborative nature of academics in a liberal arts university setting. Students may recognize that the ability to work effectively with others on group projects and in study groups is an essential part of academic success.
The second issue is the active weighing of costs and benefits of the medication that students are constantly carrying out. IAA and SSE were related to higher adherence on weekdays but not on weekends. This suggests that academic success is perceived as being beneficial enough to take medication on weekdays, but on weekends, the costs of CSE and LAS outweigh the importance of academic success. By the same token, the negative aspects of the medication (LAS and CSE) are outweighed on weekdays by the salience of IAA and SSE.
The results also indicate the importance of people in students’ lives when it comes to adherence rates. Generally, students believed that the people in their lives wanted them to take their medication, and this was particularly true for adherent students. It is intriguing to note that parents seem to play a stronger role in determining adherence on weekends than on weekdays. Moreover, the weighted means for physicians and parents show particularly strong effect sizes on weekends. Thus, when students wish to follow the recommendations of authority figures, the influence of these authority figures is considerable, and can outweigh the temptation to miss medications on weekends. On weekdays, however, the weighted means for siblings, friends, and physicians are all relatively strong predictors of adherence. One interesting possibility here is that if siblings and friends are perceived as providing an honest opinion of one’s social abilities, (and social abilities are perceived as important to academic success), then these individuals’ views outweigh the temptation to miss medications during weekdays.
In any case, friends, family members, and physicians have an opportunity to increase adherence through positive encouragement. Even people who are not seen every day maintain an influence on the way that students take their medication.
Although this study offers many intriguing findings, it remains that these results are based on a small sample from a single small liberal arts university, and replication is needed before interventions to improve adherence are justified. Of course, given the limited power afforded by the small sample size, the coherent pattern of significant findings is notable. Further limitations include the use of self-reports to measure adherence, as well as the fact that the various measures used were all obtained using the same method, namely a single online survey. Finally, in the present study, we used a simple, specific self-report question to measure non-adherence behaviors and general self-reported measures have often been found to overestimate adherence levels. However, when highly specific questions about recent and limited time spans are used, as was done here, self-reports have been found to be accurate (Hertzog, Park, Morrell, & Martin, 2000), and predictive of clinical outcomes (Jerant, DiMatteo, Arnsten, Moore-Hill, & Franks, 2008; Stirratt et al., 2015).
Future research in this area could benefit not only from a larger sample but also from following students’ management of their medication across an entire term using multiple indicators. One could hypothesize that levels of adherence on weekends, in particular, would increase during particularly busy times during the term. It would also be of great interest to do an analysis of how medication is managed across different types of academic tasks (term papers, tests, in-class presentations) and academic disciplines (e.g., sciences, humanities, fine arts). Finally, it would be valuable to measure actual outcomes of medication use, using both objective measures (i.e., grades) and subjective ones (e.g., feelings of accomplishment, self-esteem and self-efficacy). University environments bring their own unique set of demands and challenges, and at the same time present a great time of transition for young adults. It is important to better understand university students’ changing beliefs about medication, not only as a window into their adherence behaviors in the future but also as a way to understand the role of beliefs and social norms on purposive non-adherence.
In summary, these results replicate past findings that college students are constantly making conscious decisions to adjust the dosages of their stimulant medication. The decision process used to make these adjustments is based partly on the views of important others, but also on a complex weighing of the costs and benefits of the drug. Whereas perceived side effects and LAS decrease adherence, perceived enhanced academic performance and enhanced social skills increase adherence. Our findings extend existing research to show that both adherence levels and the relative influence of the factors that predict adherence change across the week. These exploratory results suggest interesting pathways for future research to further understand how young adults actively and consciously make decisions about when and how to take prescription medications for ADD/ADHD.
Footnotes
Acknowledgements
The authors wish to acknowledge the staff at the Meighen Centre for Learning Assistance and Research at Mount Allison University for support in recruiting participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.