
Abstract
Introduction
ADHD is a neurodevelopmental heterogeneous disorder with behavioral symptoms of inattention, hyperactivity, and impulsivity as described in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013) diagnosis of ADHD by the American Psychiatric Association (APA, 1994). The worldwide prevalence of adult ADHD has been estimated to be approximately 4% (de Graaf et al., 2008). The consequences of adult ADHD extend beyond the core symptoms of the disorder and involve impaired executive functioning, poor adaptive functioning including inadequate social performance, relationship difficulties, occupational, and educational difficulties as well as poor functioning in everyday activities (Barkley & Murphy, 2010; Biederman et al., 2006; Gjervan, Torgersen, Nordahl, & Rasmussen, 2012). There is evidence that ADHD disorder seriously affects quality of life (QoL) in many different ways (Brod, Johnston, Able, & Swindle, 2006; Safren, Sprich, Cooper-Vince, Knouse, & Lerner, 2010). Several studies have also reported highly prevalent deficits in executive function in adults with ADHD (Barkley & Murphy, 2010; Biederman et al., 2007). They have elevated risks of low occupational participation as well as poor work related performance (Barkley, Murphy, & Fischer, 2008; de Graaf et al., 2008; Gjervan et al., 2012) and poor academic achievements. And furthermore, ADHD is also associated with an increased risk of lifelong psychiatric comorbidity (Halmøy, Fasmer, Gillberg, & Haavik, 2009; Kessler et al., 2006; Torgersen, Gjervan, & Rasmussen, 2006). The most prevalent comorbid disorders are substance use disorders, affective disorders, and anxiety disorders (Fayyad et al., 2007). These impairments are indirect indications of QoL; however, the present study explores a more direct measure of QoL and its psychometric properties and validity in a sample of adult patients with ADHD.
A growing body of evidence suggests that measures of QoL in adults with ADHD is strongly affected by functional deficits (Brod, Perwien, Adler, Spencer, & Johnston, 2005; Safren et al., 2010). While generic QoL is developed to assess the impact of general health conditions, the Adult Attention-Deficit/Hyperactivity Disorder Quality of Life (AAQoL) scale is a disease-specific measure that assesses self-reported perception of the emotional and functional impact of ADHD. The literature reflects that adult ADHD is generally associated with both low disease specific (Brod et al., 2006; Matza, Johnston, Faries, Malley, & Brod, 2007; Weiss et al., 2010) and generic QoL (Adler et al., 2006; Matza, Stoeckl, Shorr, & Johnston, 2006). More specifically, untreated adult ADHD is found to have significantly lower scores than the U.S. norm on the Medical Outcomes Study 36-item short form health survey (SF-36; Ware & Sherbourne, 1992) mental component scales, that is, Vitality, Social function, Role-emotional function, and Mental Health (Adler et al., 2006). As QoL is a multidimensional concept reflecting individual perception of social, psychological, and functional aspects of health conditions, measures of QoL are increasingly being used to assess consequences of ADHD and are considered an important outcome of the disorder. Previous research suggests that ADHD symptoms are negatively correlated with generic QoL (Gjervan, Torgersen, Rasmussen, & Nordahl, 2014). There is also evidence that symptoms of inattention are a stronger mediator of QoL than hyperactivity/impulsivity (Weiss et al., 2010), although another study found no differences in QoL between the ADHD subtypes (Gibbins et al., 2010). However, the results from the study by Gibbins et al. (2010) question the validity of the hyperactive/impulsive subtype in adults. Results from some studies also indicate that QoL in adults with ADHD might be associated with deficit in executive functions (Brod et al., 2015; Stern & Shalev, 2013).
Given the heterogeneous and severe outcomes associated with ADHD, there are strong reasons to expand the scope of assessment of QoL in both clinical practice and research. So far, there are no measures capturing specific QoL consequences of adult ADHD available in Norway, and the other Scandinavian countries have only recently validated their translated versions of the AAQoL (Brod et al., 2015).
The AAQoL has demonstrated good responsiveness and test–retest reliability in previous studies (Matza et al., 2007; Matza, Van Brunt, Cates, & Murray, 2011). It was originally developed and validated in the United States (Brod et al., 2006) and has recently been validated in a large study including adults from 13 European countries (Brod et al., 2015). The results showed similar factor loadings between European and U.S. participants. The same was also true for the internal consistency of the scale, and discriminant validity and responsiveness. Also, the scores for each individual scale were comparable. These results suggest that the AAQoL is robust and may be used in different population settings. The convergent validity of the AAQoL was moderate to strong with the Behavior Rating Inventory of Executive Function–Adult Version (BRIEF-A) Self-Report scale (Roth, Isquith, & Gioia, 2005). This is not surprising as poor executive functioning has previously been described as a core deficit in ADHD (Barkley & Murphy, 2010; Biederman et al., 2007, Biederman et al., 2006), thus, it would be expected to affect self-reported QoL.
The AAQoL was developed from a sound theoretical model developed from both qualitative and statistical data and is commonly used to assess QoL in both clinical and research contexts. Given the well-documented effect from symptoms and function on QoL, there is a need for a Norwegian version of the AAQoL to be used for both clinical and research purposes. Therefore, we have performed a Norwegian translation of the original American version of AAQoL in agreement with the original authors.
Aim of the Study
The aim of the study was to validate the Norwegian translation of the original AAQoL and to examine and present the sample in terms of sociodemographic and clinical characteristics.
We hypothesized that results from confirmatory factor analysis would show that the Norwegian translation of the AAQoL is valid.
Method
Design
Cross-sectional data from self-report questionnaires and retrospective data from medical journals were used in the analyses.
Sample
All adults (≥ 18 to ≤ 61 years old) receiving a diagnosis of ADHD in middle Norway at the Department of Psychiatry, North-Trondelag Hospital Trust, and Tiller and Nidaros Psychiatric centers at St. Olavs Hospital in South-Trondelag during 1997 to 2013 were identified for invitation to participate in the study. After controlling for the validity of diagnoses and correctness of registrations in patient administrative systems, persons available for invitation to participate in the study were identified. A group of 233 individuals were not possible to contact due to unknown postal address. Recruitment of participants was conducted in 2009 and 2013. A total of 1,255 adult persons with confirmed ADHD were invited to participate in the study by postal mail, and 313 returned informed consents and completed self-report questionnaires including the Norwegian version of the AAQoL. The informed consent included unlimited access to medical records. Participants were excluded from the data set only when missing confirmed ADHD diagnosis or missing signed informed consent form.
Assessment and Procedures
From 1997 to May 2005, all patients older than 18 years who were to receive treatment with central stimulants in Norway had to be evaluated and approved by one of three national expert committees for hyperkinetic disorders. National guidelines were used to secure a valid diagnosis and adequate treatment. These guidelines included systematic assessment of ADHD according to the International Classification of Mental and Behavioural Disorders: Diagnostic criteria for research (ICD-10; “The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines,” 1992). Two modifications were made, allowing the inattentive subtype in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) as sufficient for the diagnosis and for the presence of comorbid psychiatric disorders. The guidelines were mandatory until May 2005.
This procedure for assessment and treatment of adult ADHD is described in earlier papers (Halmøy et al., 2009; Rasmussen & Levander, 2009; Solberg, Haavik, & Halmøy, 2015; Torgersen et al., 2006).
The Departments of Psychiatry in North and South-Trondelag continued to use the national guidelines for assessment after May 2005 with two modifications. The general Adult ADHD Symptom Checklist (Amen, 1997) was replaced by the Adult ADHD Self-Report Scale (ASRS; Kessler, Adler, Ames, Demler, et al., 2005), and the Mini International Neuropsychiatric Interview was introduced as a mandatory tool for diagnosing comorbidity. In most cases, the assessment was supplemented with additional information, such as structured diagnostic interviews, neuropsychological tests, computed tomography/magnetic resonance imaging, and electro encephalography. All relevant information about the diagnostic assessment, patient history, and treatment was documented in the medical records.
Translation Protocol
The authors of the original AAQoL (Brod et al., 2006; Brod et al., 2005) gave their permission to the translation of the AAQoL following a well outlined protocol. First, three forward translations (English to Norwegian) were performed by three independent translators, all fluent in English.
After receiving approval for this first step, a preliminary Norwegian version was submitted for back-translation (Norwegian to English) by three independent translators who were blind to the original questionnaire. These were two mental health professionals and one native English professional proofreader. When this step was approved, a second preliminary Norwegian version was prepared. The instrument was then piloted in a group of six to eight adult persons with diagnosed ADHD. A focus-group setting was used to clarify their understanding of the items of the questionnaire. Modifications were discussed in detail with the authors of the original AAQoL. All materials, versions, and comments were then sent for review by the original authors. After receiving a final approval by the authors of the original AAQoL, we prepared the present Norwegian version of the AAQoL.
Measures
Clinical variables
From the patients’ medical records, we collected information about past ADHD diagnosis and treatment history including age at first treatment with central stimulants from childhood to adulthood, and duration of central stimulant treatment in adult psychiatry. Also, past comorbid diagnoses were collected from the patient’s records. Two comorbid disorders are labeled lifetime disorders: lifetime depressive disorder and lifetime anxiety disorder. This resembles the different types of categories within depression and anxiety.
Current AAQoL
The AAQoL is a disease-specific health-related quality of life instrument specifically designed to assess self-reported, perceived QoL in adults with ADHD. The AAQoL has 29 items assessing health-related quality of life during the past two weeks among adults with ADHD. Each item is rated by patients on a 5-point Likert-type scale ranging from 1 = not at all/never to 5 = extremely/very often. The AAQoL yields a total score (based on all 29 items) and four subscale scores: Life Productivity (11 items, including getting things done on time, completing projects or tasks, remembering important things, and balancing multiple projects), Psychological Health (6 items, including feeling anxious, overwhelmed, and fatigued), Life Outlook (7 items, including perceptions that energy is well spent, people enjoy spending time with you, you can successfully manage your life, and you are as productive as you would like to be), Relationships (5 items, including tension, annoyance, and frustration in relationships). Total and subscale scores are computed by (a) reversing scores for all items except the seven items in the Life Outlook subscale; (b) transforming all item scores to a 0 to 100 point scale (1 = 0; 2 = 25; 3 = 50; 4 = 75; 5 = 100); and (c) summing item scores and dividing by the item count to generate subscale and total scores. The AAQoL allows up to three missing items for the total score, and each subscale score can be computed with up to one missing item. The original version has demonstrated satisfactory psychometric properties in earlier studies (Brod et al., 2015; Brod et al., 2006; Matza et al., 2007). Internal consistency with Cronbach’s alpha in the data set was .87 for Life Productivity, .79 for Psychological Health, .84 for Life Outlook, and .76 for Relationships.
Current ADHD symptoms
Adult ADHD Self-Report ScaleFull Edition (ASRS-v.1)
The ASRS is the World Health Organization’s self-report rating scale for adult ADHD (Kessler, Adler, Ames, Demler, et al., 2005). This scale is designed to assess current ADHD symptoms, and consists of 18 items based on the DSM-IV diagnostic criteria for ADHD. The items are measured on a 5-point Likert-type scale (0 = never/seldom to 4 = often), with a possible total range of 0 to 72. Higher scores indicate higher frequencies of symptoms and symptom load. The scale is organized in two sections, each with its own sum-score. Items 1 to 9 (part A) reflect symptoms of inattention (I), and items 10 to 18 (part B) reflect symptoms of impulsivity or hyperactivity (HI). Internal consistency with Cronbach’s alpha for ASRS in the data set was .84 on part A, and .83 on part B.
Current sociodemographic characteristics
Information about age, gender, and level of education and occupational status were obtained from the participants using a self-report questionnaire. Occupational status refers to the individual’s source of income. The Norwegian social welfare system comprises social benefits such as unemployment benefit, sickness benefit, vocational rehabilitation, and medical rehabilitation. Due to their temporary nature, these categories are statistically pooled into one group, called temporary social benefit. Disability pension differs from temporary social benefits as it is most often a lifelong benefit obtained only when treatment and rehabilitation most likely will not enable the individual to attain a job again.
Statistical Analyses
Confirmatory factor analysis was performed by the Mplus 7.1 software, http://www.statmodel.com/ to investigate the model fit of the data from the Norwegian translation of AAQoL (Muthén & Muthén, 3463 Stoner Avenue Los Angeles, CA 90066). In addition, the IBM Statistics SPSS version 22 was used to run analyses of internal consistency and correlations and descriptive chi-square statistics and t tests.
Ethics
The study was approved by the Regional Committee for Medical and Health Research Ethics and conducted in accordance with the Helsinki declaration and Norwegian research laws.
All participants gave a signed informed consent to participate in the study
Results
Sociodemographic Characteristics
Mean age for the total sample was 33.9 years ranging from 18 to 63 (SD = 10.5).
Gender distribution in the sample showed that 185 (59.1%) women and 128 (40.9%) men participated in this study.
Educational level among the participants varied as 190 individuals (61.1%) reported junior high school as their highest level of education, and 56 (18.1%) had attained college or university. A total of 77 (25.1%) participants were receiving disability pension, and 115 (37.5%) received some type of temporary social benefit. Analyses of continuing occupational activity or studies ≥50% for the last 12 months showed that 101 individuals (38.8%) had not been in work or studies during the last year, 16 (6.2%) had been working or studying for 1 to 3 months, 27 (10.4%) for 4 to 6 months, 21 (8.1%) for 7 to 9 months, and 94 (36.2%) had been engaged in work or studies for 10 to 12 months. There were no significant gender differences in sociodemographic characteristics (Table 1).
Sample Characteristics (N = 313).
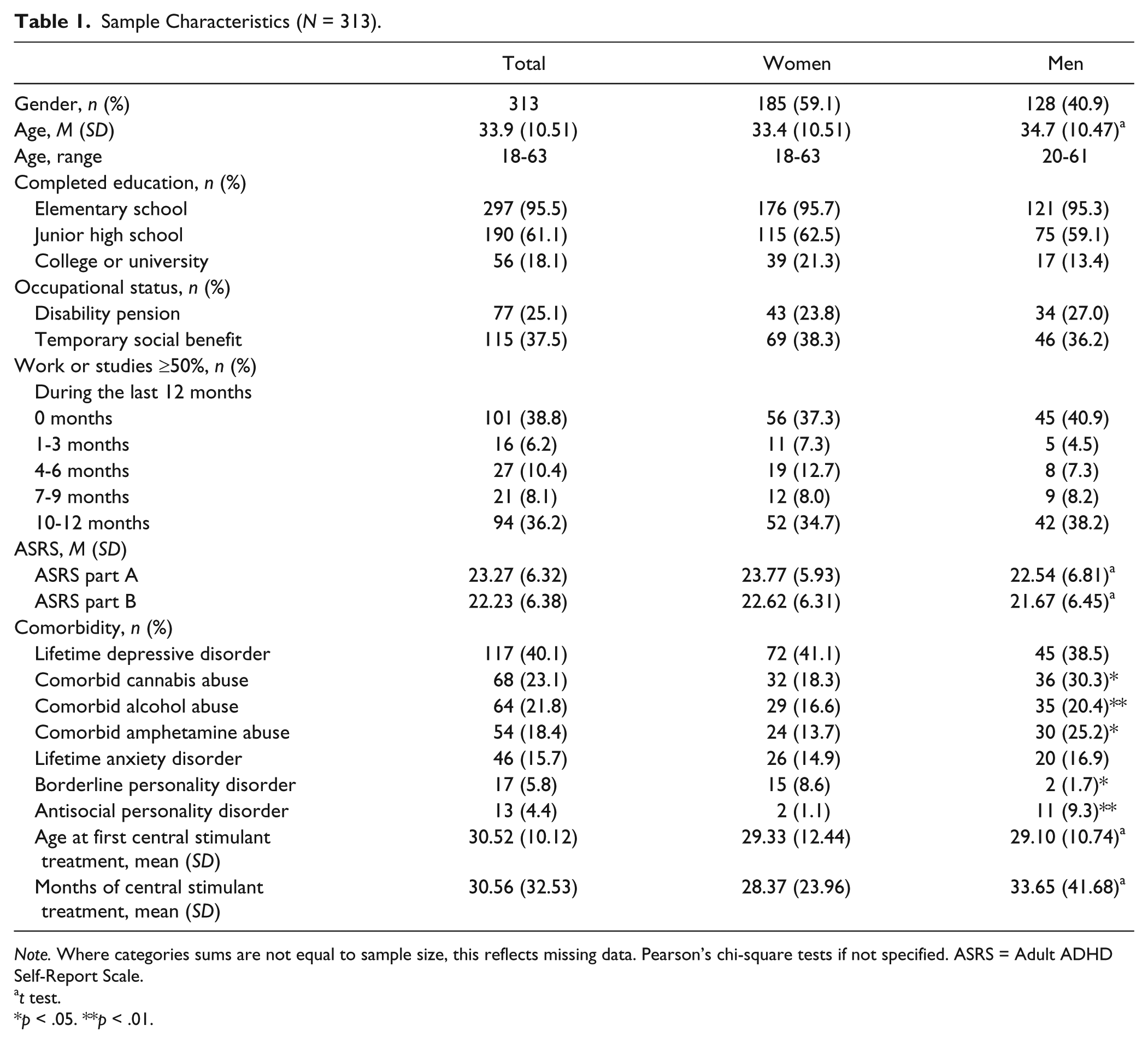
Note. Where categories sums are not equal to sample size, this reflects missing data. Pearson’s chi-square tests if not specified. ASRS = Adult ADHD Self-Report Scale.
t test.
p < .05. **p < .01.
Clinical Characteristics
ADHD symptoms
The total ASRS mean score was 46.58 (SD = 20.81) with a mean of 23.27 (SD = 6.32) for part A inattentiveness and 22.23 (SD = 6.38) for part B hyperactivity/impulsivity. We found no significant gender differences in ADHD symptoms (Table 1).
Comorbidity
Lifetime depressive disorder was the most prevalent comorbid disorder: 117 (40.1%). A total of 68 patients (23.1%) had lifetime cannabis abuse, 64 (21.8%) had lifetime alcohol abuse with significantly more men, 35 (20.4%), than women, 29 (16.6%), having the disorder (p < .01). Furthermore, 54 (18.4) had lifetime amphetamine abuse, and 46 of the participants (15.7%) had lifetime anxiety disorders. There were significant gender differences in the prevalence of borderline personality disorder (BPD) with 15 women (8.6%) versus two men (1.7%) having the disorder (p < .05), and significantly more men, 11 (9.3%), than women, 2 (1.1%), had antisocial personality disorder (p < .05) (Table 1).
Treatment history
Mean age at first central stimulant (CS) treatment in the sample was 30.52 (SD = 10.12), and total duration of CS treatment at recruitment time was 30.56 months (SD = 32.53) (Table 1).
AAQoL
The mean score for the AAQoL Life productivity scale was 50.34 (SD = 19.52). Mean score for the Psychological Health scale was 46.68 (SD = 21.17) with women having a significant lower score (p < .01) than men. Mean score for the Life Outlook scale was 52.33 (SD = 17.40), and 55.97 (SD = 20.21) for the Relationships scale, and finally 50.89 (SD = 16.46) for the total score. Cronbach’s alpha for the AAQoL subscales ranged from .76 to .87 and was .86 for the total score (Table 2). Correlations between the AAQoL scales are shown in Table 3.
AAQoL Scores (N = 313).

Note. AAQoL = Adult Attention-Deficit/Hyperactivity Disorder Quality of Life.
t test.
p < .01.
Correlations Between the AAQoL Scales.
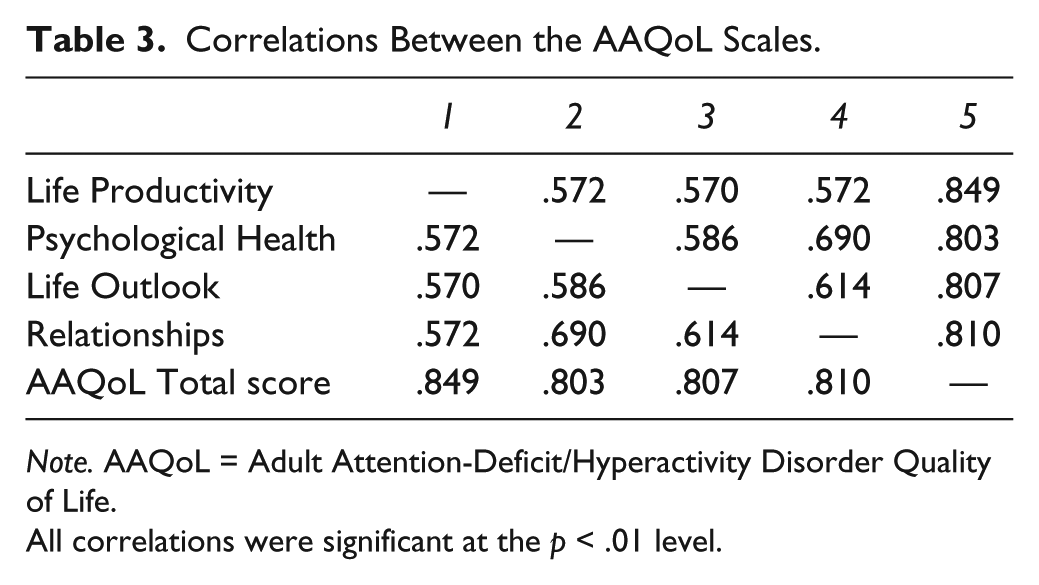
Note. AAQoL = Adult Attention-Deficit/Hyperactivity Disorder Quality of Life.
All correlations were significant at the p < .01 level.
Confirmatory factor analysis
To examine the properties of the translated AAQoL, we applied confirmatory factor analysis. No changes were made in the original number of domains and their related items.
The chi-square test of model fit provided a value of 863.179 with 371 degrees of freedom (df) and p = .0000. Estimation of the goodness of fit of the model showed that the root mean square error of approximation (RMSEA) estimate was 0.069 with 90% confidence interval (CI) = [0.069, 0.075]. Furthermore, we found that the comparative fit index (CFI) was .873 and the Tucker–Lewis index (TLI) was .821.
Results from two-tailed correlations showed moderate to robust relationships between all AAQoL scales and the ASRS I and HI. The correlations between ASRS I and the Life Productivity scale were −.713 (p < .01) and −.651 (p < .01) for the AAQoL total score (p < .01). The correlation between ASRS HI and the Psychological Health scale was −.488 and −.529 for the AAQoL total score. The total range for correlations between AAQoL and ASRS I were −.713 to −.433 and −.529 to −.342 for ASRS HI (Table 4).
Pearson Two-Tailed Correlations Between ADHD Symptoms and AAQoL Scales.
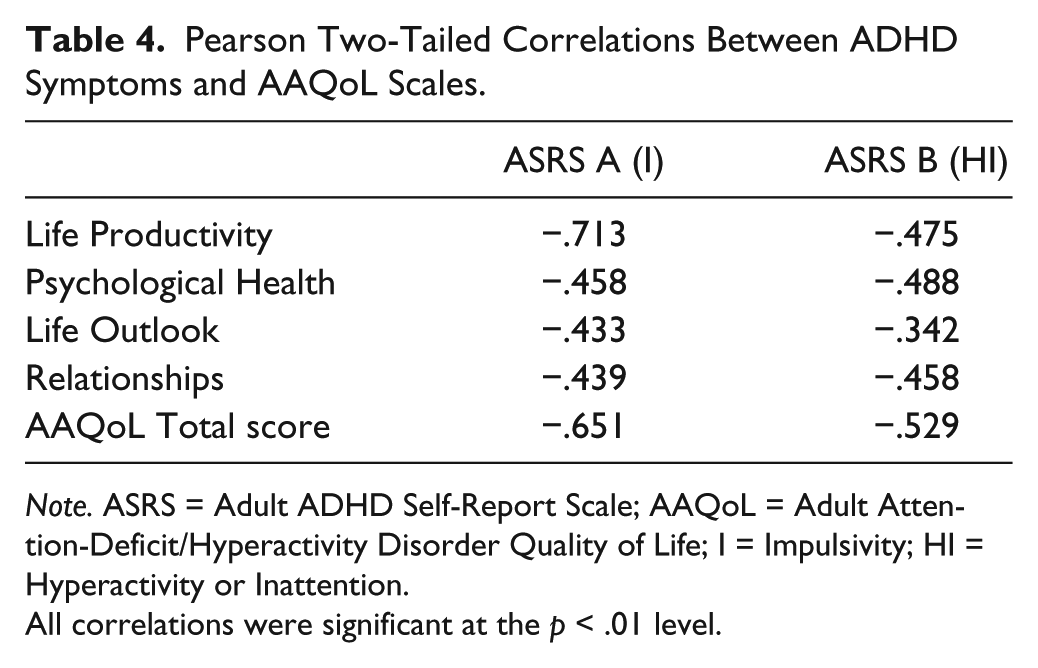
Note. ASRS = Adult ADHD Self-Report Scale; AAQoL = Adult Attention-Deficit/Hyperactivity Disorder Quality of Life; I = Impulsivity; HI = Hyperactivity or Inattention.
All correlations were significant at the p < .01 level.
Discussion
The major finding in this study was that the Norwegian translation of the AAQoL showed good psychometric properties and initial indications of validity. Results from the analyses of the model fit between data from the translation and the original AAQoL provided evidence that the Norwegian version of AAQoL was valid for the sample in the current study. Our findings also correspond well with the mean scores from the original AAQoL (Brod et al., 2006) as well as findings in European patients (Brod et al., 2015). The conducted analyses resulted within the acceptable range for model-fit indicators and proper internal consistency for all scales. The RMSEA estimate was optimal and the CFI value was close to optimal while the TLI value was too small to be considered optimal although acceptable (Schreiber, Nora, Stage, Barlow, & King, 2006). Internal consistency by Cronbach’s alpha was acceptable and comparable to the original AAQoL and results from the other European versions (Brod et al., 2015; Brod et al., 2006).
To establish whether the Norwegian version of AAQoL would reflect ADHD related impairments, we examined convergent validity of the translated AAQoL (Zeller & Carmines, 1980). Convergent validity was supported by moderate to strong correlations between ADHD symptoms and all scales in the translated AAQoL. This suggests that the AAQoL scores are negatively associated with specific ADHD symptoms as was expected.
The fact that inattentiveness was somewhat stronger associated with low AAQoL scores is recognizable in results from earlier studies indicating that attention complaints are associated with several generic QoL aspects, such as problems with social functioning, role-emotional function, and vitality (Scholtissen-In de Braek, Hurks, van Boxtel, Dijkstra, & Jolles, 2011). In line with this, a study by Weiss and colleagues suggests that symptoms of inattention are a stronger mediator of ADHD-specific QoL than hyperactivity/impulsivity (Weiss et al., 2010). However, research also suggests that there may be no difference in QoL between ADHD subtypes (Gibbins et al., 2010), and there is a growing body of research suggesting that adult ADHD is generally associated with both disease-specific and generic QoL (Adler et al., 2006; Brod et al., 2006; Matza et al., 2007; Matza et al., 2006). Furthermore, in a recent study by our own group (Gjervan et al., 2014), we found that ADHD symptoms were differentially related to different aspects of generic QoL. The issue related to what symptom groups affects QoL in which way is still understudied and therefore unclear; thus, further research is needed to better understand this particular relation.
The scores from the subscales and the total score of the Norwegian AAQoL were only marginally different from previously reported scores from the original version (Brod et al., 2015; Brod et al., 2006). Conclusively, the scores from the Norwegian version of the AAQoL are comparable with both U.S. and European scores. This opens for researchers to compare results from studies across countries. The results show that the present sample is characterized by substantial impairment in quality of life and everyday function.
The prevalence rates of functional impairment and psychiatric comorbidity in the sample is recognizable from previous epidemiological findings (Kessler, Adler, Ames, Barkley, et al., 2005; Kessler et al., 2006; Kessler, Chiu, Demler, Merikangas, & Walters, 2005). Analyses of demographical variables indicated that the sample was considerably impaired in terms of poor educational and occupational outcomes. The association between ADHD and these impairments has also been reported elsewhere (Barkley & Murphy, 2010; Barkley et al., 2008; Biederman et al., 2008; de Graaf et al., 2008; Gjervan et al., 2012). In line with previous studies (Halmøy et al., 2009; Kessler, Chiu, et al., 2005; Torgersen et al., 2006), we also found high prevalence numbers for psychiatric comorbidity. Mood and substance use and anxiety disorders were the most prevalent disorders. The impact of comorbidity on functional outcome is still somewhat understudied. However, previous research suggests a relationship between psychiatric diagnoses of comorbidity and low occupational activity in adults with ADHD (Halmøy et al., 2009; Sobanski et al., 2007).
Limitations
There is a risk of gender bias in the results as there are considerably more women than men in the sample. This may have negatively affected the representativeness of our results by possible gender-related skewness in some results. Because of the relatively low response rate, the study also represents a risk of biased results. However, the present sample had recognizable symptom levels and prevalence of comorbidity as well as impaired function when compared with samples in the reviewed literature. The clinical characteristics for the total sample are in line with previous epidemiological studies, and we only found gender differences in symptoms for comorbid substance abuse and borderline personality disorder and antisocial personality disorder. This was expected as these comorbid disorders are generally associated with gender differences. Also, one cannot overlook the possibility of recruitment bias in the sample as all participants were self-selected. However, the sample was recruited from a clinical population and is very well assessed as both the diagnosis of ADHD and comorbid diagnoses were established by experienced clinicians using established diagnostic guidelines when starting treatment, and in retrospect, by a specialist in adult psychiatry experienced in assessing and treating adult ADHD. The systematic assessment and high quality of diagnoses contributes to the external validity of the results.
Implications
The Norwegian version of the AAQoL is the first validated specific measure of QoL for adult ADHD in Norway. This gives both clinicians and researchers the opportunity to extend the assessment and exploration of functional and psychological impairment in Norwegian adults with ADHD. The high degree of impairment in QoL and associated function suggests that these aspects should receive more attention in the assessment and treatment of ADHD. Further studies should examine the clinical utility of the AAQoL and whether there are subgroup differences in adults with ADHD. Also, the previously reported differential associations between ADHD symptoms and generic QoL aspects should be further investigated with ADHD specific QoL measures. Finally, the validity of the Norwegian version of AAQoL should also be examined in other samples.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author has received noncommercial financial support from Oslo University Hospital in Norway through the ADHD research network in Norway in connection with the present project.