
Abstract
The “gold standard” approach for the assessment of ADHD in children is based on a multi-method, multi-informant strategy where the key informants are parents and teachers (American Academy of Pediatrics, 2011; Anastopoulos & Shelton, 2001). The collection of parent and teacher data for the assessment of ADHD became necessary with publication of the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 1994), which added assessment of impairment across settings to the diagnostic criteria. Despite the widespread use of parent and teacher data for the assessment of ADHD, it has been known for the past 25 years that parent and teacher reports correlate at a low level, ranging from .25 to .50 (Achenbach, McConaughy, & Howell, 1987; Biederman, Faraone, Milberger, & Doyle, 1993; Mitsis, McKay, Schulz, Newcorn, & Halperin, 2000; Newcorn et al., 1994). Low agreement between parent and teacher reports is the norm rather than the exception in the assessment of ADHD in children (Swanson, Lerner, March, & Gresham, 1999). Research studies have also shown that parent ratings tend to be higher than teacher ratings across clinic-referred and community samples (Antrop, Roeyers, Oosterlaan, & Van Oost, 2002; Malhi, Singhi, & Sidhu, 2008).
For a long time, discrepancy between informants was thought to be the result of measurement error (Achenbach, 2011; De Los Reyes, 2013). However, this view has not been empirically supported. An argument against the measurement error explanation is that studies have consistently shown correlations in the low to moderate range between informants, even when informants used instruments that had sound psychometric properties and similar items across informants (Achenbach & Rescorla, 2001). Low correlations between informants result even when the same factor structure explains variance in the reports of multiple informants who complete the same measure (Baldwin & Dadds, 2007; De Los Reyes, 2013). Error measurement alone does not provide a complete and parsimonious account of informant discrepancies (De Los Reyes, 2013).
Two other explanations have been offered as the cause for informant discrepancy in the reporting of children’s mental health functioning. Those are (a) informants’ unique perspectives and (b) situation specificity (De Los Reyes & Kazdin, 2005; Dirks, De Los Reyes, Briggs-Gowan, Cella, & Wakschlag, 2012; Gomez, 2007). The unique perspective explanation maintains that differences between parent and teacher reports occur because parents and teachers have different perceptions of the problem behavior (Antrop et al., 2002; Gomez, 2007; Mitsis et al., 2000; Wolraich et al., 2004). Differences in perceptions could be the result of informants having less historical knowledge of the child. For example, a teacher rating a child’s behavior at the beginning of the school year has far less information on which to base that rating than at the end, and the teacher always has less information about the child’s behavior than the parent. Differences in perceptions could also be the result of report biases or having different thresholds for viewing certain behaviors as “problems.” Two of the most frequently discussed biases are the mood congruent reporting bias and halo effect. According to the mood congruent bias, a negative mood state in the informant could lead to reporting more negative as opposed to more positive or neutral information about the child being rated (De Los Reyes, 2013). Halo effect refers to when an informant provides an inflated estimate of a given disorder (e.g., ADHD) when the child has other related disorders (e.g., oppositional defiant disorder [ODD]; Dirks et al., 2012). However, although these biases are common, they explain little of the total variance in discrepancies between informant reports (De Los Reyes, 2013; Youngstrom, Izard, & Ackerman, 1999). Research has also shown that the threshold for viewing certain behaviors as problematic can vary depending on the cultural background of the informant (Lambert et al., 1992; Weisz et al., 1988), or on the context in which the behavior is observed. For example, a teacher might rate a student’s assertive behavior as oppositional in the classroom setting but as assertive outside the classroom (Dirks et al., 2012). As such, informant discrepancies might comprise differences in the type of behaviors that are problematic in a specific context from the perspective of a particular informant that might have a different threshold for judging the behaviors (Dirks et al., 2012; Dumenci, Achenbach, & Windle, 2011).
According to the situation specificity hypothesis, disagreements between informants reflect differences in expectations and demands present in specific settings. For example, the behavioral demands in the classroom are quite different from the demands at home. Different behavioral demands result in different types of behaviors and differences in degree or intensity of behaviors. Under this perspective, discrepancies between parents and teachers are the result of differences in observable behavior. The situation specificity hypothesis has received empirical support. There is greater agreement between informants rating children’s behavior in the same environment (e.g., school setting) compared with informants rating children in different settings (e.g., school and home; Achenbach et al., 1987). Also, observational and laboratory studies conducted in school and summer camp settings have provided support to the notion that informant discrepancies are to a large extent the result of differences in child behavior across settings (De Los Reyes, Henry, Tolan, & Wakschlag, 2009; Hartley, Zakriski, & Wright, 2011).
Clinicians, who often face the dilemma of determining whether or not a child meets diagnostic criteria for ADHD in the context of discrepant parent and teacher reports, need more information to better understand the reasons for the discrepancy. For a specific child, the clinician can obtain most of this information by interviewing the parents. For example, the clinician can ask the parents about their own psychological functioning, get the child’s school history, inquire about the child’s behavioral and emotional functioning at home and at school, evaluate the quality of the parent–teacher relationship, and assess the child’s academic performance by reviewing grade report card and test scores (Barkley, 2015).
At a more global level, the clinician can also benefit from knowing about factors that affect parent–teacher reporting in general. For example, are there any child or family factors that are linked to parent–teacher discrepancies in the reporting of child mental problems (Wender, 2004)? Little research has been conducted to identify factors related to this cross-source discrepancy, with some notable exceptions (De Los Reyes et al., 2009). Identifying factors contributing to parent–teacher discrepancy could be useful for clinical practice. It might shed some light on the “informants’ unique perspectives versus situation specificity” hypotheses.
The purpose of this study is to investigate factors related to parent–teacher discrepancy scores derived from a widely used rating scale for measuring symptoms of ADHD. Specifically, the study investigates how children’s (a) demographic characteristics, (b) psychiatric comorbidity, (c) academic performance, and (d) cognitive and academic achievement scores are related to parent–teacher discrepancy scores of symptoms of ADHD. The study is unique in that it examines the relationship between parent–teacher discrepancy scores and several demographic and clinically relevant factors in the context of an ADHD evaluation, in a large clinic-referred sample.
The following research questions were examined:
Method
Participants and Setting
The sample of children and adolescents (see Table 1) was derived from a database of 1,722 consecutive referrals for diagnostic assessment to a specialized center for the management of ADHD located in a pediatric hospital in a large city in the Northeastern section of the United States. Children were referred to the center by parents, teachers, or primary care physicians. Typical reasons for referral included excessive hyperactivity, inattention, impulsivity, noncompliance, conduct problems, and academic difficulties. Participants for this study were the 1,364 participants for whom both parents and teachers had completed the ADHD-IV rating scale.
Demographic and Sample Characteristics (N = 894).

Note. The sample size varied between measures due to missing data and the need to use different measures for some of the children. SES = socioeconomic status; WIAT = Wechsler Individual Achievement Test.
Sample Characteristics
Demographic information and sample characteristics for the children included in the study is provided in Table 1. The average age of participants was 9.56 years. Most of the sample was male and Caucasian. The most common comorbid diagnoses were ODD and generalized anxiety disorder (GAD). The sample had a large percentage of children who had a history of special education support, many of whom had special education for learning problems, and/or who had failed a grade. The average estimated IQ score was slightly above the 50th percentile and the average reading and math scores were slightly below the strict average level of 100.
Measures
ADHD Rating Scale, Fourth Edition, Home and School Version (ADHD-RS-IV, Home, School)
Ratings of symptoms of ADHD were obtained from parents and teachers using the ADHD-RS-IV (DuPaul, Power, Anastopoulos, & Reid, 1998). Each of the 18 items is rated on a 4-point scale ranging from 0 (never or rarely), 1 (sometimes), 2 (often), to 3 (very often). The ADHD-RS-IV is comprised of 18 items adapted from the symptom list for ADHD in the DSM-IV. Factor analytic studies have indicated that the nine-item inattention factor (I) and the nine-item hyperactivity/impulsivity factor (H-I) of this instrument closely correspond to the two-dimensional structure in the DSM-IV (DuPaul, Anastopoulos, et al., 1998; DuPaul et al., 1997). This measure has adequate reliability and validity (DuPaul, Power, McGoey, Ikeda, & Anastopoulos, 1998). This study uses the age and gender normed T scores for analyses, because these are the scores that are commonly used in clinical decision making (Anastopoulos & Shelton, 2001).
Covariates
Demographic covariates
Demographic variables were ethnicity and socioeconomic status (SES; see Table 1). Ethnicity was determined based on parent report. The SES for this sample, as determined by the Four-Factor Index of the Social Status (Hollingshead, 1975), was 1% in Category I (laborers), 7% in Category II (machine operators), 22% in Category III (skilled craftsman, clerical, and sales workers), 28% in Category IV (small business owners, technicians), and 42% in Category V (major business owners, professionals).
Comorbidity
Comorbidity variables were externalizing and internalizing disorders (see Table 1). The presence of a comorbid externalizing disorder (i.e., ODD or conduct disorder [CD]) or internalizing disorder (i.e., separation anxiety disorder [SAD], GAD, social phobia [SOPHOB], specific phobia [SP], panic disorder [PD], major depressive episode [MDE], dysthymia [Dys], or bipolar disorder [BD]) was assessed using the parent version of the Diagnostic Interview for Children and Adolescents, DSM IV Version (DICA-IV; Reich, Leacock, & Shanfeld, 1995).
The DICA-IV is a semi-structured diagnostic interview designed to evaluate symptoms of child psychopathology using DSM-IV criteria. The interview procedure for this instrument measures number of symptoms, symptom duration, age of onset, and level of functional impairment according to setting or situation (e.g., at home, at school, making or keeping friends). Doctoral-level psychologists and advanced doctoral students in psychology trained in the administration of the DICA-IV administered this measure and each interview was audio recorded. Approximately, 20% of the total interviews (i.e., 346 audiotapes) were randomly selected and scored by another trained clinician to determine inter-rater agreement, which was based on whether the two raters agreed on diagnostic status. The kappa coefficients were as follows: ODD = .84, CD = .77, MDE = .82, dysthymic disorder = .73, GAD = .83, SAD = .87, SOPHOB and SP = .61. Each of the composed K statistics was above the acceptable range for agreement on diagnostic interview data (Hartman, 1982).
Academic performance
Academic performance variables were (a) history of special education for academic problems, (b) history of grade failure, and (c) homework performance. History of special education for academic problems and history of grade failure were based on parent report. Homework performance was assessed using the Homework Problems Checklist (HPC; Anesko, Schoiock, Ramirez, & Levine, 1987). The HPC was used to provide information regarding parent perceptions of children’s homework-related problems.
The HPC is a 20-item checklist that requires parents to rate the presence and severity of homework problems. It has high internal consistency (α = .91; Anesko et al., 1987). The HPC has been shown to be reliable for students with behavioral disorders (Foley & Epstein, 1993). The HPC has been shown to have a moderate to high correlation with parent ratings of inattention, but low correlations with teacher reports of inattention, learning problems, and study skills (Power, Werba, Watkins, Angelucci, & Eiraldi, 2006). Raw scores from the HPC were used due to the unavailability of norms for the entire grade range used in this study.
Cognitive ability and academic achievement
Cognitive ability was estimated using one of the Wechsler Intelligence Tests: Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler, 1999), Wechsler Abbreviated Scale of Intelligence, Second Edition (WASI-II; Wechsler, 2001), Wechsler Preschool and Primary Scale of Intelligence–Revised (WPPSI-R; Wechsler, 1989), Wechsler Intelligence Scale for Children (WISC), Wechsler Intelligence Scale for Children, third edition (WISC-III; Wechsler, 1991), Wechsler Intelligence Scale for Children, fourth edition (WISC-IV; Wechsler, 2003) or Wechsler Adult Intelligence Test–Third Edition (WAIS-III; Wechsler, 1997). For the WASI and WASI-II, the estimated full-scale IQ score was based on the combined score of the Vocabulary and Block Design subtests. The full-scale IQ score was used for the WPPSI-R, the WISC-III, or the WISC-IV. The WASI and WASI-II are strongly correlated (Wechsler, 2001), and the other Wechsler Intelligence Scales used in the study are strongly correlated with the WASI (Wechsler, 2011).
The academic achievement covariates (see Table 1), specifically, basic reading and math skills, were assessed using standard scores from two subtests of the Wechsler Individual Achievement Test (WIAT). Because the current sample is derived from assessments spanning 7 years, participant data include scores from either the original WIAT (Wechsler, 2001) or the second edition of the test (WIAT-II; Wechsler, 1992). The Basic Reading and Numerical Operations subtests from the first version of the WIAT, or the Word Reading and Numerical Operations subtests from the WIAT-II were used to assess academic performance. These corresponding subtests of the WIAT and the WIAT-II are strongly correlated (WIAT-II; Wechsler, 2001). Internal consistency estimates and test–retest correlations for these subtests are above .85 (Wechsler, 2001). In this study, data from word/basic reading (n = 827) and numerical operations (n = 818) were used.
Procedures
The current project utilized data from an existing database that was derived from psychological assessments of children referred to an ADHD evaluation and treatment center. Parents were asked for their consent and children were asked for their assent. The Institutional Review Board of the pediatric hospital approved the research procedures for the study. Questionnaire packets were mailed to parents and teachers several weeks prior to the family’s appointment at the center. On the day of the assessment, one member of the clinical team administered the DICA-IV and an unstructured interview in which parents were asked to report on their child’s age, ethnicity, gender, history of grade failure, and special education, whereas another clinician administered the child measures (e.g., cognitive and achievement testing).
Statistical Analyses
Given that parent scores tend to be higher than teacher scores (Antrop et al., 2002; Malhi et al., 2008), we chose deviations from parent ratings on the ADHD-RS-IV as a measure of split or “discrepancy.” We used percentile scores instead of raw scores for calculating the split between parent and teacher ratings because (a) percentile scores are the scores which clinicians routinely use in making diagnostic decisions (Anastopoulos & Shelton, 2001) and (b) a goal of this article was to assess factors that might help clinicians reconcile parent–teacher discrepancies while sorting out clinical data in the context of clinical care.
The average discrepancy between parent and teacher total scores for the sample was 10.8 (SD = 19.3). Discrepancies ranged from teachers being 66 percentile points higher than the parents, to parents being 88 percentile points higher than the teachers.
Given the relatively small number of ethnic and racial minority children in the data set, data from all ethnic and racial minority children were collapsed under the “minority” category. Similarly, given that the majority of children did not receive special education services, receipt of special education services was collapsed into a yes or no variable based on whether or not the classification was for academic problems, without any distinction based on classification. In predicting discrepancy scores, multiple regression analyses were employed. Because multiple comparisons were made, a smaller p = .01 level of significance was used for all analyses.
To determine which factors are related to the parent–teacher discrepancy (Aim 1), a series of multiple regression equations were used to predict the discrepancy score from each group. This set of analyses was used to predict the discrepancy in parent–teacher total scores.
To determine the relevant weight of significant predictors in predicting the parent–teacher difference score (Aim 2), a multiple regression equation was used to predict the discrepancy score with the predictors being the covariates, which were significant in the analyses for Aim 1 and their multiplicative interaction terms.
To determine how participants for whom parents reported the higher presence of ADHD symptoms, participants for whom teachers reported the higher presence of ADHD symptoms, and participants for whom parents and teachers reported a comparable level of ADHD symptoms differed from each other (Aim 3), the sample was divided into three groups. These were (a) “Average Difference” group (participants whose agreement was within 1 standard deviation [19.3] of the mean [10.8] parent–teacher difference score), (b) “Teacher High” group (participants for whom the teacher reported higher levels of ADHD symptoms than the parent and the difference was more than one standard deviation below the mean difference score; difference score < −8.5), and (c) “Parent High” group (participants for whom the parent reported higher levels of ADHD symptoms than the teacher and the difference was more than one standard deviation above the mean difference score; difference score > 30.1). ANOVA was used to compare the three groups and any significant differences were further explored using post hoc Tukey’s T tests.
Results
Examination of Aim 1
The correlation between ADHD-RS-IV parent and ADHD-RS-IV teacher was .24. The regression equation using ethnicity and SES and their multiplicative interaction as predictors was a significant predictor of parent–teacher discrepancies in ADHD-IV total scores (F = 6.38, p < .001). Table 2 shows that at the p = .01 level of significance, only ethnicity was a significant predictor in the final model (t = −2.46, p = .01). Specifically, there was a greater discrepancy between parent and teacher reports for ethnic minority families than for Caucasian families, with parents reporting fewer symptoms relative to teachers. In addition, there was a trend toward significance for the interaction between ethnicity and SES, with the ethnicity related differences in parent–teacher discrepancy scores increasing as SES increases.
Predicting Parent–Teacher Discrepancy in ADHD-IV Total Score Using Demographic, Comorbidity, Academic Performance, and Cognitive Ability/Academic Achievement Predictors (Aim 1).
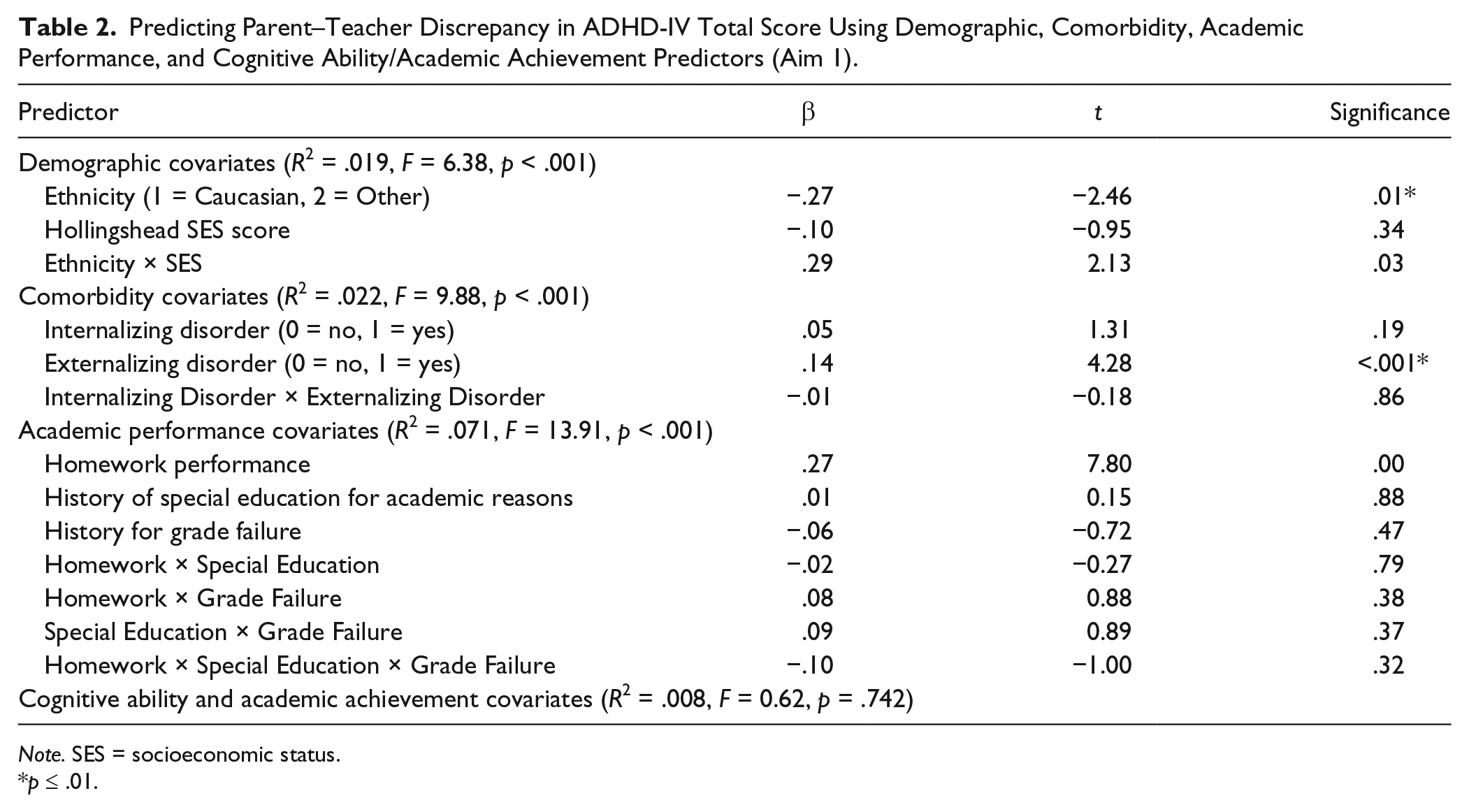
Note. SES = socioeconomic status.
p ≤ .01.
The regression equation using comorbid internalizing and externalizing disorders and their multiplicative interaction as predictors was a significant predictor of parent–teacher discrepancies in ADHD-IV total scores (F = 9.88, p < .001). Only externalizing disorders was a significant predictor in the final model (t = −4.28, p < .001). Specifically, there was a greater discrepancy between parent and teacher reports for children who had a comorbid externalizing disorder than for children who did not have a comorbid externalizing disorder, with parents reporting more ADHD symptoms than teachers for children with a comorbid externalizing disorder (see Table 2).
The regression equation using homework performance, history of special education for academic reasons, and grade failure and their multiplicative interactions as predictors was a significant predictor of parent–teacher discrepancies in ADHD-IV total scores (F = 13.91, p < .001). Only homework performance was a significant predictor in the final model (t = −7.80, p < .001). Specifically, there was a greater discrepancy between parent and teacher reports for children who showed more homework problems at home than for children who had fewer homework problems, with parents reporting more ADHD symptoms than teachers for children with greater levels of homework problems at home (see Table 2).
The regression equation using IQ and math and reading achievement scores and their multiplicative interactions as predictors was not a significant predictor of parent–teacher discrepancies in ADHD-IV total scores (F = 0.62, p = .74).
Examination of Aim 2
To determine the relative weight of the predictors that were significant predictors of the parent–teacher difference score in the prior analyses (ethnicity, comorbid externalizing disorder, and homework problems), a multiple regression equation was run using three predictors and their multiplicative interaction terms to predict the parent–teacher discrepancy score. The regression equation was a significant predictor of parent–teacher discrepancies in ADHD-IV total scores (F = 21.04, p < .001). As shown in Table 3, both comorbid externalizing disorder (t = 3.13, p < .01) and homework performance (t = 4.06, p < .001) were significant predictors of the parent–teacher difference scores. Ethnicity was no longer a significant predictor when comorbid externalizing disorder and homework performance were also included as predictors in the same model (t = 0.10, p = .92). Specifically, there was a greater discrepancy between parent and teacher reports for children who showed more homework problems, with parents reporting higher levels of ADHD symptoms than teachers. In contrast, the presence of a comorbid externalizing disorder was associated with less disagreement between parents and teachers, when the presence of homework problems was taken into account.
Predicting Parent–Teacher Discrepancy in ADHD-IV Total Score Using Predictors Which Were Significant in Prior Analyses (Aim 2).

p < .01. **p < .001.
Examination of Aim 3
To determine how participants for whom parents reported higher presence of ADHD symptoms (Parent High) differed from participants for whom teachers reported higher presence of ADHD symptoms (Teacher High), and how both groups differed from participants for whom parents and teachers reported a comparable level of ADHD symptoms (Average Difference), ANOVAs were calculated for Parent ADHD-IV Total Score, Teacher ADHD-IV Total Score, and each of the covariates used in Aim 1. ANOVAs were significant for Parent ADHD-IV Total Score, F(2, 1361) = 369.9, p < .001; Teacher ADHD-IV Total Score, F(2, 1361) = 613.5, p < .001; SES, F(2, 983) = 8.2, p < .001; comorbid externalizing disorders, F(2, 1361) = 18.6, p < .001; and homework problems, F(2, 1277) = 70.8, p < .001.
Post hoc Tukey’s tests were conducted for the significant ANOVAs. Not surprisingly, the results shown in Table 4 indicated that Parent ADHD-IV Total Scores were significantly lower for the Teacher High group than for either of the other two groups (Average Difference or Parent High) and that Teacher ADHD-IV Total Scores differed among the three groups in the expected direction (Teacher High > Average Difference > Parent High). Post hoc analyses indicated that participants in the Parent High group were of significantly higher SES than either participants in the Teacher High group or the Average Difference group, whereas the latter two groups were not significantly different from each other. Tukey’s tests indicated that participants in the Teacher High group were significantly less likely to have a comorbid externalizing disorder than participants in the Parent High group or participants in the Average Difference group, whereas the latter two groups were not significantly different from each other. Last, participants in the Teacher High group had fewer parent-reported homework problems than participants in either the Average Difference or the Parent High groups, whereas the latter two groups did not differ from each other. See Table 4 for further details of these analyses.
Differentiating Between Children Whose Teachers Report Higher Levels of Symptoms, Children Whose Parents Report Higher Levels of Symptoms, and Children Whose Parents and Teachers Report Similar Levels of Symptoms (Aim 3).

Note. WIAT = Wechsler Individual Achievement Test. *p < .01. **p < .001.
Discussion
This study sought to identify factors that contribute to parent–teacher discrepancy in the reporting of symptoms of ADHD in clinic-referred children. The sample composition, including age (9.7 years), gender ratio (74% male), ethnic/racial ratio (74% Caucasian), and ADHD subtype composition (37.4% inattentive subtype), was in general similar to other previous study samples (e.g., Lahey et al., 1994; Newcorn et al., 1994). When predicting parent–teacher discrepancy from demographic variables, we found discrepancy between parents and teachers, with teachers reporting higher levels of symptoms for ethnic minority children than for non-minority children. When the extreme groups were examined, SES mattered more than ethnicity. The group in which parents reported higher levels of symptoms than did teachers was of significantly higher SES than participants in the other two groups (see Table 4). The finding regarding ethnic minority children is not unexpected as teachers often rate ethnic minority children and in particular, African American children, as being more symptomatic than Caucasian children (e.g., Reid, Casat, Norton, Anastopoulos, & Temple, 2001), suggesting that reporters’ unique perspectives, and not situation-specific differences, underlie this finding. The second finding regarding SES might be an artifact of the sample given that most children in the study were Caucasian from relatively high-income households (see Table 1). Further studies with a more economically and ethnically diverse sample would more adequately clarify these relationships.
When predicting parent–teacher discrepancy from comorbidity covariates, there was a greater discrepancy between parent and teacher reports for children who had a comorbid externalizing disorder, with parents reporting higher levels of symptoms of ADHD than teachers. Participants whose teachers reported higher levels of symptoms of ADHD than their parents did were significantly less likely to have a comorbid externalizing disorder. The first finding regarding comorbid externalizing disorders is most likely accounted for by the fact that most of the children in the sample were referred by their parents. Parents are more likely to seek help for children who have comorbid externalizing problems (such as oppositional and defiant behavior at home) than for children who do not present comorbid problems (Eiraldi, Mazzuca, Clarke, & Power, 2006). As seen in Table 1, 34% of the children met criteria for an externalizing disorder based on the parent semi-structured interview. This finding is also consistent with the informants’ unique perspective, as oppositional defiant symptoms were most often reported by parents and therefore, parents who are seeing their children being oppositional might also be more likely to perceive their children’s ADHD symptoms as more severe. The finding regarding teachers is consistent with the view that teachers tend to have a lower threshold for identifying problems that affect their ability to teach, such as disruptive behavior exhibited by children with ADHD, than for other problems that do not affect their ability to teach, such as learning disabilities or internalizing disorders, and also suggests that it is differing perspectives, rather than situational differences in behavior, that underlie this finding.
We also found that when parents reported homework problems at home, they also reported higher levels of symptoms of ADHD than teachers did. Looking at the extreme, groups showed that when teachers reported higher levels of symptoms of ADHD than parents, parents reported fewer homework problems. It is not known whether teachers would have reported more homework problems along with higher levels of symptoms of ADHD, if a teacher measure of homework problems were used. However, given that the burden of managing homework completion falls entirely on parents, it is likely that the findings would not have been different if a teacher measure of homework completion were also used. In contrast to the findings regarding ethnicity and externalizing problems, the finding that homework performance differences is related to parent–teacher discrepancies supports the situation specificity hypothesis, as it is probably driven by the effects that specific behaviors have upon the home and school context.
When the three significant predictors (ethnicity, comorbid externalizing disorder, and homework performance) were jointly entered into a regression equation, comorbid externalizing disorder (t = 3.13, p < .01) and homework performance (t = 4.06, p < .001) emerged as significant predictors of the parent–teacher difference scores, whereas ethnicity was no longer a significant predictor. These findings suggest that homework problems, closely followed by externalizing behavior problems, are the most important factors associated with parent–teacher discrepancy in the reporting of symptoms of ADHD. Regarding the “informants’ unique perspective versus situation specificity” hypotheses, the findings that homework problems were a key predictor of discrepancy seem to provide support for the “situation specificity” hypothesis (De Los Reyes & Kazdin, 2004). Parents expect their children to respect rules and do well in school; the onus placed on parents is to ensure that children meet these expectations. When children are not able to meet these expectations, their parents rate them as more symptomatic. Teachers, however, expect their students to stay on task and not disrupt the class. The demand placed on teachers is that they teach all students, regardless their individual circumstances. When students are not able to meet these expectations, they are rated as more symptomatic. In contrast, the finding that children with comorbid ODD were rated by parents as more symptomatic provides support for the unique perspective theory, suggesting that there may be a halo effect of children who are showing one type of disruptive behavior in the home setting, oppositional defiant behavior, are also perceived as showing more of another type of disruptive behavior, hyperactive, impulsive behavior. However, our study has a significant limitation in drawing any conclusions about the relative merit of the informant perspective versus the situation specificity hypothesis, because it did not include observational data of children’s behavior in the home and school setting; therefore, any conclusions regarding the individual perspective versus the situation specificity hypothesis must be considered preliminary and tested further with observational behavioral data.
Our study has some additional limitations. The findings regarding the effects of homework problems in parent–teacher discrepancy in the reporting of symptoms of ADHD is limited by the fact that a teacher measure of homework problems was not used. Ethnic minority families in the sample were primarily of African American descent, so the findings are not generalizable to other ethnic or racial groups. Also, most participants were of Caucasian and middle or upper-middle-class background. Non-Caucasians and lower SES participants were underrepresented.
The analyses using the ADHD RS-IV were conducted on percentile scores and not on raw scores. This approach was chosen because ADHD RS-IV percentile scores, rather than raw scores, are most often used by clinicians when making diagnostic decisions, as they allow comparison with normative behavior for children of similar age and gender; and, the goal of our study was help guide clinical decision making when clinicians are faced with discrepant information. Given that our sample was a clinic-referred sample, and is, therefore, biased toward having higher levels of symptoms than would be found in a population-based study and has a distribution that is positively skewed relative to the population mean, the use of percentile scores has the advantage that it reduces reliance on the mean. However, although it has merit of not heavily depending on nominal distribution and incorporates information about normative behavior by age and gender, there is a disadvantage in that percentile scores are not evenly spaced relative to raw scores. For example, a 1% change in score may be several points or a single point in raw score, depending on the relative frequency of that particular raw score.
As found in other studies (e.g., Swanson et al., 1999), the agreement between parents and teachers in the reporting of symptoms of ADHD in this sample was very low (.24). The clinical implications for the study are that clinicians should interpret discrepant information between parents and teachers as reflective of the child behavior in “that particular context” (Roberts, Milich, & Barkley, 2015, p. 55), while being aware that particular characteristics of the child, such as their ethnicity and whether they are oppositional at home, are also likely to influence parents’ perception of the severity of their children’s ADHD symptoms.
In summary, parent–teacher discrepancy on the reporting of symptoms of ADHD is likely to occur when the child has significant homework problems closely followed by externalizing behavior problems. No source of information should be seen as more valid or accurate than any other source, but it is important that reporters’ ratings of overall severity of ADHD symptoms are supplemented by specific behavioral details, such as that obtained during behavioral observations or a semi-structured interview, for the clinician to discern the extent to which differences in impairment in different settings, rather than differences in informant perspective, are leading to discrepant results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.