
Abstract
Introduction
Research shows that emotion dysregulation (ED) is a key impairment for many individuals with ADHD (Shaw, Stringaris, Nigg, & Leibenluft, 2014). Emotion regulation (ER) refers to “an individual’s ability to modify an emotional state so as to promote adaptive, goal-oriented behaviors,” and is essential to interpersonal, academic, and adaptive functioning (Shaw et al., 2014, p. 1; Thompson, 1994). As such, ED is conceptualized as (a) expressions of emotion that are excessive in relation to societal norms or situational context, (b) rapid and poorly controlled shifts in emotion (i.e., lability), and/or (c) atypical allocation of attention to emotional stimuli (Shaw et al., 2014). The prevalence of ED in clinical samples of ADHD ranges between 24% and 50% in children (Becker et al., 2006; Sjowall, Roth, Lindqvist, & Thorell, 2013; Spencer et al., 2011) and 34% and 70% in adults (Barkley & Fischer, 2010; Reimherr et al., 2005; Surman et al., 2013). However, it should be noted that prevalence estimates are significantly influenced by the definitions of ED used and the measurement of the construct (e.g., parent-report vs. self-report vs. observation). Longitudinally, ED in youth with ADHD is associated with increased psychiatric comorbidity (particularly with mood and anxiety disorders), greater social impairments, poorer quality of life, and greater academic and occupational difficulties (Althoff, Verhulst, Rettew, Hudziak, & van der Ende, 2010; Barkley & Fischer, 2010; Biederman et al., 2012; Seymour, Chronis-Tuscano, Iwamoto, Kurdziel, & Macpherson, 2014; Wehmeier, Schacht, & Barkley, 2010).
From a theoretical perspective, ED also is purported to be a core deficit in individuals with ADHD (Barkley, 1997). Barkley’s unified model of ADHD suggests that due to difficulties inhibiting a prepotent response (i.e., behavioral inhibition) and poor interference control, individuals with ADHD may be impaired in the regulation of arousal in the service of goal-directed activity (i.e., ER). As such, this theory stresses the importance of understanding ER in the context of ADHD as dysregulation of affect and motivation that can negatively affect one’s ability to complete goal-directed activity.
One form of ED of particular importance in ADHD is frustration, defined as “an affective response to blocked-goal attainment” (Leibenluft, 2011; Leibenluft, Blair, Charney, & Pine, 2003). Irritability, a mood state characterized by poor frustration tolerance is common in youth with ADHD (Leibenluft, 2011). Indeed, one study showed that 71.6% of youth with ADHD have clinically significant irritability compared with 3.2% of typically developing (TD) controls (Geller et al., 2002). While frustration is a normative affective response to blocked goal attainment, youth with increased levels of irritability display a lower threshold for frustration (i.e., low frustration tolerance). In particular, as approximately 41% of youth with ADHD also have comorbid oppositional defiant disorder (ODD), a disorder characterized by impairing irritability (Elia, Ambrosini, & Berrettini, 2008), it could be hypothesized that children with ADHD + ODD have poorer frustration tolerance than children with ADHD alone; however, the role of ODD has never been examined in relation to ADHD and frustration tolerance.
To date, there has been little empirical investigation of frustration tolerance in youth with ADHD. The only studies of frustration in youth with ADHD have been observational studies in which frustration is characterized using observer-based assessments during frustrating situations (e.g., unsolvable puzzle task, frustrating peer competition). For example, in an observational study of 6- to 11-year-old boys with and without ADHD, boys with ADHD were shown to be less effective in regulating their emotions during a frustrating peer competition than age-matched, non-ADHD comparison boys. That is, boys with ADHD displayed more signs of negative or frustrated emotion than non-ADHD comparison boys. Furthermore, in comparison with boys without ADHD, boys with ADHD demonstrated an enduring pattern of disinhibition (as measured by higher stop signal reaction time score) before and after the frustration task (Walcott & Landau, 2004). Another study of observed frustration demonstrated that 6- to 12-year-old youth with ADHD were more likely to quit a frustrating puzzle task before completion, more likely to report frustration, and less likely to engage in mood repair than non-ADHD comparison youth (Scime & Norvilitis, 2006). Increased levels of frustration and decreased task persistence by boys with ADHD have been reported during both academic and non-academic tasks (e.g., videogames, mapping task; Lawrence et al., 2002). In addition, youth with ADHD have difficulty identifying and processing negative emotions (Norvilitis, Casey, Brooklier, & Bonello, 2000; Singh et al., 1998), which may interfere with their ability to persist in goal-directed activity when frustrated.
Unfortunately, there are a number of limitations of the extant literature examining frustration in youth with ADHD. First, none of the existing studies of frustration in youth with ADHD have considered the role of comorbid ODD. Given high rates of comorbidity between ADHD and ODD, and the role of irritability (and therefore low frustration tolerance) in ODD, examination of frustration in ADHD youth with and without comorbid ODD is critical to understanding frustration tolerance in youth with ADHD. An additional limitation is that there have been few investigations of the behavioral correlates of frustration in youth with ADHD. That is, the majority of studies have relied on observational methodologies (i.e., studies in which child behavior is coded using observational coding systems) rather than the use of behavioral tasks to probe frustration. Observational methodologies may be subject to rater bias and therefore more objective means of probing frustration such as task persistence should be examined. Furthermore, in comparison with observational paradigms that may not reliably elicit frustration, behavioral tasks such as the Mirror Tracing Persistence Task (MTPT) used in this study have been shown to reliably elicit frustration in participants and to be predictive of difficulties with ER including substance use disorders and borderline personality disorder (BPD), as well as substance use treatment drop out (Daughters et al., 2005; Leyro, Zvolensky, & Bernstein, 2010). A final limitation is that a number of prior studies of frustration in youth with ADHD have included exclusively boys (Hoza, Pelham, Waschbusch, Kipp, & Owens, 2001; Lawrence et al., 2002; Walcott & Landau, 2004), which may not generalize to girls with ADHD.
The goal of the current study was to examine frustration tolerance in youth ages 10 to 14 years with and without ADHD using a behavioral task. We hypothesized that youth with ADHD would have lower frustration tolerance than their non-ADHD comparison peers. Furthermore, we sought to examine the role of comorbid ODD on MTPT performance in youth with ADHD. Therefore, we compared MTPT performance in youth with ADHD and ODD (ADHD + ODD, n = 12) with those with ADHD without ODD (ADHD – ODD, n = 23). We also examined ODD as a moderator in the relationship between ADHD and frustration tolerance.
Method
Participants
Participants included 67 youth between the ages of 10 and 14 years with (n = 37) and without (n = 30) Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994) ADHD. The age range of 10 to 14 years was chosen due to the larger aims of the study (i.e., to examine the relationship between ER and depressive symptoms in youth at an age when depressive symptoms are likely to emerge; Seymour et al., 2012). Participants were recruited through mailings to pediatricians, schools, and community centers in the Washington DC metropolitan area, as well as university employees and families who had previously been seen in the laboratory. For inclusion in the study, youth were required to (a) be between the ages of 10 and 14 years, (b) be fluent in English so that they could understand and complete questionnaires; and (c) have at least one residential parent/guardian who was willing to participate and could complete the measures in English. Youth were excluded if there was evidence of mental retardation (estimated IQ <70) or evidence of psychosis, bipolar disorder, or pervasive developmental disorders (PDD).
For inclusion in the ADHD group, youth had to meet full DSM-IV criteria for ADHD according to evidence-based assessment procedures (i.e., parent-report on a semi-structured clinical interview and parent and teacher completion of ADHD rating forms; Pelham, Fabiano, & Massetti, 2005). For inclusion in the non-ADHD comparison group, youth could not have more than three total symptoms of DSM-IV ADHD or clinically significant impairment according to combined parent and teacher report. Participant characteristics are presented in Table 1.
Participant Demographic and Clinical Characteristics (n = 66).

Note. Results presented as M (SD) or as percent (n). Total ADHD, inattention, hyperactivity/impulsivity are based on parent and teacher report on the Disruptive Behavior Disorders Checklist and clinician report on the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children–Present and Lifetime Version (K-SADS-PL). The mean for WISC scaled scores is 10. WISC-IV = Wechsler Intelligence Scale for Children–4th edition; ODD = oppositional defiant disorder; MTPT-C = Mirror Tracing Persistence Task–Computerized Version.
Two ADHD participants were missing WISC-IV scores.
n = 24 and 20 for ADHD and Control groups, respectively.
Five participants (three Controls and two ADHD) were missing MTPT-C data due to technical errors.
Procedures
Participants were screened via telephone to determine initial eligibility and, if eligible, were scheduled for a single assessment session at the University of Maryland College Park. Written parent consent and child assent were obtained prior to participation. During the assessment, parents completed (a) a diagnostic interview about the youth’s past and current ADHD symptoms, (b) rating scales assessing the youth’s ADHD and disruptive behavior disorder (DBD) symptoms and functional impairment, and (c) a demographics questionnaire. Youth completed (a) a brief IQ screen using the Wechsler Intelligence Scale for Children, 4th Edition (WISC-IV) Block Design and Vocabulary subtests (Wechsler, 2003) and (b) a computerized behavioral task of frustration tolerance. Youth with ADHD who were taking stimulant medication were allowed to remain on their medication on the day of testing (for ethical reasons), but for diagnostic purposes, questions were asked about their behavior off medication. For the larger aims of the study, information was also collected from parents and youth about depressive symptoms and ER. Youth were paid US$25 for their participation and parents were offered a free workshop offered by the first author on “Parenting Adolescents.”
With parental permission, rating scales were sent to the teacher who spent the most time with the child and knew him or her the best. In total, teacher ratings were available for 66% (n = 44) of the sample, and there was no difference between groups on the presence of teacher ratings, χ2(1, N = 67) = 0.02, p = .89. If teacher data were unavailable, the ADHD diagnosis was made using clinician assessment and parent-report of school performance and difficulties, incorporating prior report cards and school records when available. Teachers received US$10 upon completion of these scales.
Assessment of parent and youth demographic information
Parents were asked to complete a basic demographic information form inquiring about parent and/or youth sex, age, ethnicity/race, income level, and medication status.
Assessment of youth ADHD
Parents/guardians were interviewed using the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children–Present and Lifetime Version (K-SADS-PL; Kaufman et al., 1997), a semi-structured diagnostic interview assessing current and lifetime diagnoses of ADHD. The K-SADS-PL has well-established reliability (Ambrosini, 2000) and has been shown to be highly related to the Child Behavior Checklist and Conners’ Parent Rating Scale scores (Kaufman et al., 1997). Interviews were conducted by the first author who was extensively trained in the administration of the K-SADS, and who met weekly with a licensed clinical psychologist (the senior author) for supervision. Interviews were recorded for supervision purposes, and discrepancies were discussed by the clinical team until agreement was reached.
Parents and teachers also completed the DBD symptom checklist (Pelham, Gnagy, Greenslade, & Milich, 1992) that assesses ADHD, ODD, and conduct disorder (CD) symptoms on a scale from not at all to very much. Symptoms rated as occurring pretty much or very much were considered present to a clinically significant degree. Internal consistency for the DBD in this sample was adequate to high on the ADHD (α = .95), ODD (α = .90), and CD (α = .74) scales. Total ADHD symptoms (r = .92, p < .001), total inattentive symptoms (r = .94, p < .001), and total hyperactivity/impulsivity symptoms (r = .90, p < .001) as rated by parents and teachers on the DBD were highly correlated with the clinical interview (i.e., K-SADS). Parents and teachers were requested to report on the youth’s typical behavior while not actively medicated for ADHD.
As required for a Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000) diagnosis of ADHD, cross-sectional impairment was measured using the parent and teacher versions of the Children’s Impairment Rating Scale (CIRS; Fabiano et al., 2006). On the CIRS, informants assess the youth’s level of impairment and need for treatment across multiple domains, including peer/sibling relations, self-esteem, academic achievement, and parent–child relations as well as an overall rating of impairment. Ratings are made on a 7-point scale, with scores above the midpoint indicating clinically significant impairment. The CIRS has demonstrated concurrent validity with other established measures of youth impairment and accurately discriminates between youth with ADHD and non-disordered youth (Fabiano et al., 2006). Internal consistency for both parent- and teacher-rated CIRS in this sample was high (α = .95 and .88, respectively).
Diagnoses of ADHD were made by counting symptoms endorsed by either parents or teachers as occurring to a clinically significant degree on either the K-SADS or DBD (“or” rule; Shemmassian & Lee, 2016). Furthermore, youth in the ADHD group were required to display cross-situational impairment as measured by parent or teacher report of overall impairment on the CIRS (Fabiano et al., 2006). When teacher ratings were unavailable, only parent DBD and clinician K-SADS ratings were used to count symptoms; however, parent-report about school behavior, prior report cards, and school records were used to establish cross-situational impairment. Diagnoses of ODD were made by counting symptoms (i.e., four out of eight) endorsed by parents as occurring to a clinically significant degree on either the K-SADS or DBD. Descriptive data for all scales are presented in Table 1.
Assessment of frustration tolerance
Frustration tolerance was assessed using a well-validated computerized measure of psychological distress tolerance, the Mirror Tracing Persistence Task–Computerized Version (MTPT-C; Strong et al., 2003). During this task, participants are instructed to trace the outline of a star (Figure 1) using the computer’s mouse (i.e., red dot shown in Figure 1). To elicit frustration, the mouse is programmed to move the cursor in the reverse direction of participant movement. For example, if the participant moves the mouse to the left, the red dot moves to the right. Furthermore, if the participant moves the red dot outside of the star’s lines or stalls for more than 2 s, a loud noise sounds and the red dot returns to the starting position. Participants can quit the task at any point but are told that their monetary prize is dependent upon how they do on the task. The primary outcome (i.e., frustration tolerance) is measured dichotomously (i.e., quit vs. no quit). In addition, total errors and median distance were recorded to assess participant skill on the task. Total task time is a maximum of 5 min depending on quit time. As a manipulation check, before and after the task, participants rated their current irritability, frustration, anxiety, difficulty concentrating, and bodily discomfort on a scale of 0 to 100. The MTPT-C has been shown to be a valid measure of psychological distress tolerance (i.e., the ability to persist in goal-directed activity when experiencing psychological distress) in adults engaged in smoking cessation (Brown, Lejuez, Kahler, Strong, & Zvolensky, 2005), abstinence from drugs and alcohol (Daughters et al., 2005), treatment of eating disorders (Anestis, Selby, Fink, & Joiner, 2007; Waller, Corstorphine, & Mountford, 2007), and cessation of self-harm behaviors in individuals with BPD (Gratz, 2003). Prior studies of distress tolerance in adolescents (using a modified distress tolerance task) have shown that lower levels of distress tolerance have been associated with higher levels of internalizing symptoms in females, and externalizing behaviors including ADHD and ODD both cross-sectionally and longitudinally (Cummings et al., 2013; Daughters et al., 2009).
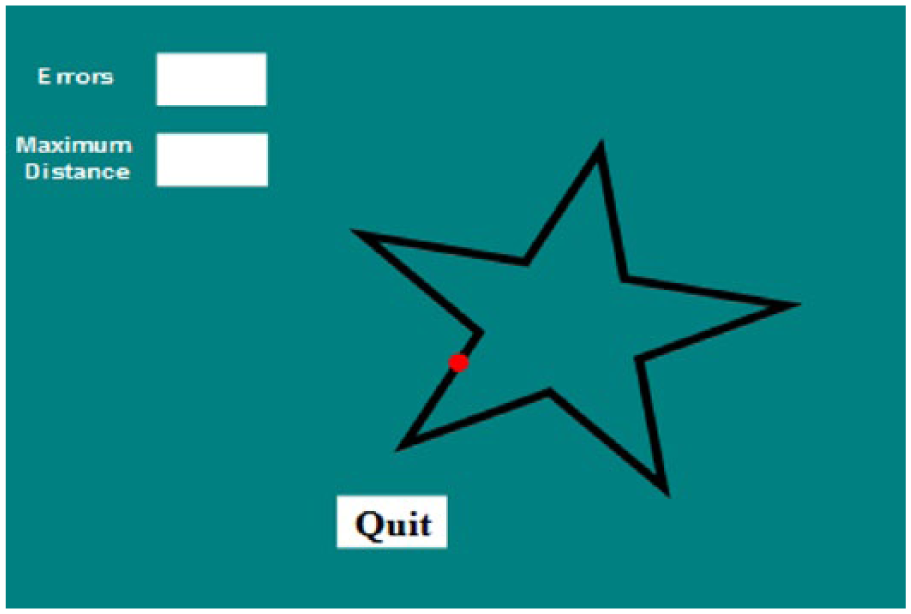
Display for MTPT-C.
Data from five participants (three controls, two ADHD) were unusable on the MTPT-C due to technical errors. Youth with missing data did not differ from those with MTPT-C data in terms of age F(1, 65) = 1.32, p = .26; sex, χ2(1, 67) = 0.74, p = .39; ethnicity, χ2(1, 67) = 0.15, p = .70; or ADHD status χ2(1, 67) = 0.51, p = .48.
Data Analytic Plan
All analyses were conducted using IBM SPSS Statistics 23. First, to ensure the task elicited frustration, paired t tests were conducted on pre- and post-task reports of emotion (e.g., overall dysphoria, frustration). Next, partial correlational analyses, controlling for group differences in race/ethnicity (due to differences between the groups, see Table 1), were conducted to examine the relationship between the dependent variable (i.e., quit/no quit on the MTPT-C) and demographic variables, ADHD symptoms, and impairment within the entire sample.
To examine group differences in errors and median distance achieved on the frustration task as well as irritability, general linear model (GLM) ANOVA were conducted. Primary analyses to compare groups (ADHD vs. TD, and ADHD + ODD vs. ADHD – ODD) on frustration tolerance (i.e., quit status) were conducted using logistic regressions. Cox and Snell R-squared are reported for model fit. To test the moderating effect of ODD on frustration tolerance in youth with ADHD, the PROCESS macro in which all predictors are mean centered prior to analysis was employed (Hayes, 2012). For moderation analysis, latency to quit (continuous variable) rather than quit versus no quit was used as the dependent variable (i.e., to avoid having all dichotomous variables in the model). For all analyses significance was set to p < .05.
Results
Manipulation Check
To confirm that the MTPT-C elicited distress, a manipulation check was conducted on emotion ratings before and after the task. Using paired t tests, the manipulation check showed that all participants had an increase in dysphoria following the MTPT-C (mean before = 43.37 ± 51.90; mean after = 89.98 ± 68.59), t(61) = −8.24, p < .001, and in particular an increase in frustration (mean before = 14.53 ± 20.17; mean after = 44.90 ± 34.32), t(61) = −7.16, p < .001.
Correlational Analyses
First, we examined the relationship between frustration tolerance on the MTPT-C and demographic variables within the entire sample. Within the entire sample, MTPT-C quit status (i.e., quit vs. no quit) was not significantly related to any demographic variables including child sex (r = .14, p = .29), child age (r = −.17, p = .18), or child race (r = .00, p = .98).
Given that diagnostic groups differed on child race/ethnicity (Table 1), partial correlations controlling for child race were used to examine the relationship between MTPT-C quit status and ADHD symptoms and impairment. All partial correlations are presented in Table 2. MTPT-C quit status was significantly related to ADHD diagnosis (r = .28, p = .02), total ADHD symptoms (r = .28, p = .03), and total inattentive symptoms (r = .30, p = .02), but not hyperactive/impulsive symptoms (r = .21, p = .11) or ODD diagnosis (r = .13, p = .32). MTPT-C quit status was also significantly related to both parent-reported overall impairment (r = .28, p = .03) and teacher-rated overall impairment (r = .32, p = .04).
Partial Correlations Controlling for Group Differences in Child Race/Ethnicity Within the Whole Sample (n = 67).
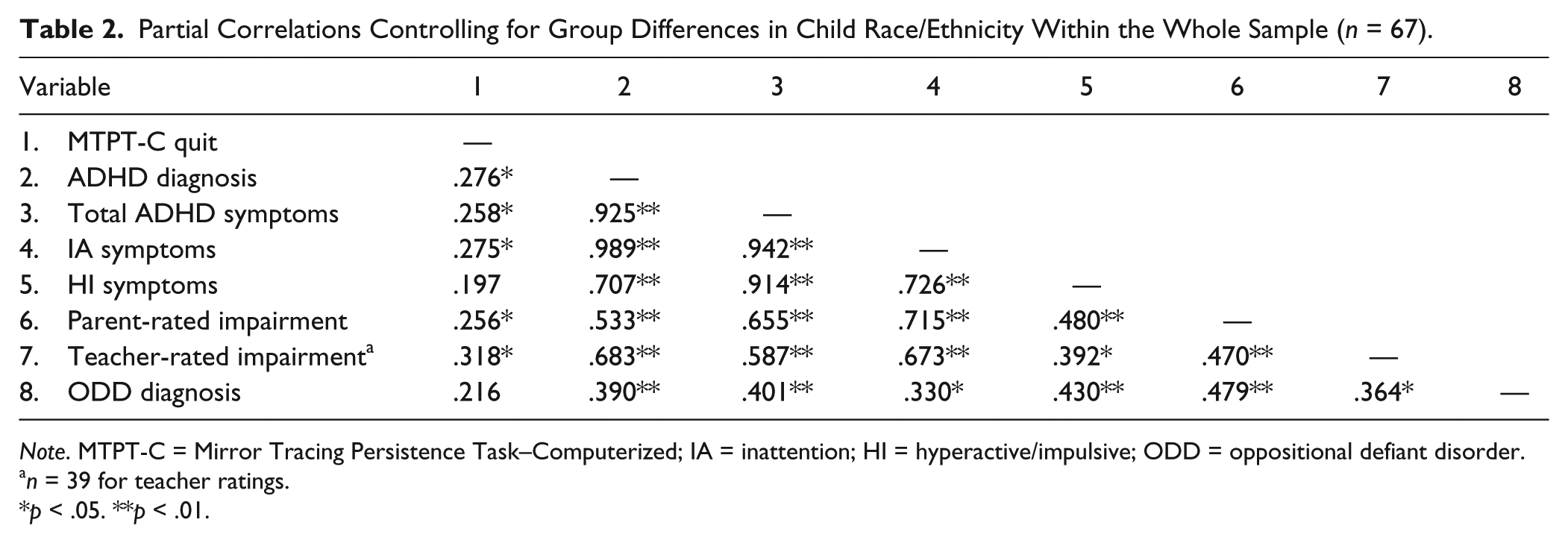
Note. MTPT-C = Mirror Tracing Persistence Task–Computerized; IA = inattention; HI = hyperactive/impulsive; ODD = oppositional defiant disorder.
n = 39 for teacher ratings.
p < .05. **p < .01.
Group Differences
Comparisons between the ADHD and Control Group on MTPT-C variables are presented in Table 1. There were no significant group differences on number of errors made on the task, F(1, 60) = 0.01, p = .95, or median distance achieved on the task, F(1, 60) = 0.88, p = .35, demonstrating no group differences in skill. Furthermore, youth with ADHD did not demonstrate a greater change in self-reported frustration compared with non-ADHD youth, F(1, 61) = 2.62, p = .11. However, youth with ADHD were significantly more likely to quit the task than control participants (odds ratio [OR] = 3.32, Wald χ2 = 4.07, p = .04; Table 2). Eighty three percent of the ADHD participants quit the task compared with 59% of non-ADHD control participants (Figure 2). In fact, youth with ADHD had 24.74 times increased odds of quitting compared with non-ADHD participants.

Differences in frustration tolerance in children with ADHD and non-ADHD controls.
Next, we compared MTPT performance in youth with ADHD + ODD (n = 12) with those with ADHD – ODD (n = 23). Groups did not differ on number of errors made on the task F(1, 33) = .02, p = .89, or median distance achieved on the task, F(1, 33) = 2.19, p = .15. Moreover, there were no differences in frustration tolerance (quit vs. no quit) between ADHD + ODD and ADHD – ODD groups (OR = 1.05, Wald χ2 = .003, p = .96).
Finally, we examined ODD as a moderator in the relationship between ADHD and latency to quit. ODD did not moderate the relationship between ADHD and MTPT latency to quit (Table 3, Figure 3).
Linear Model Predictors of MTPT Latency to Quit.

Note. Model R2 = .046. ODD = oppositional defiant disorder.
MTPT = Mirror Tracing Persistence Task.

Examination of ODD as a moderator in the relationship between ADHD and MT time to quit; Note. ODD = oppositional defiant disorder.
Discussion
This study was the first to examine frustration tolerance, assessed using a computerized behavioral task, in youth with ADHD compared with youth without ADHD. Furthermore, it was the first study to examine the role of ODD in relation to frustration tolerance in youth with ADHD.
Our main finding was that youth with ADHD demonstrated lower levels of frustration tolerance (i.e., measured as the tendency to quit a frustrating behavioral task) compared with non-ADHD control youth regardless of comorbid ODD. Our results parallel observational studies of frustration, which have shown that, compared with TD youth, youth with ADHD are less effective in regulating their emotions and persisting in the face of frustration than their TD peers (Scime & Norvilitis, 2006; Walcott & Landau, 2004). Interestingly, we did not find that youth with ADHD reported greater levels of perceived frustration with this task compared with their TD peers as has been found in other studies (Scime & Norvilitis, 2006). This may be because youth in our study were asked to self-report on their affective state rather than have the affective state characterized by an independent observer. That is, youth with ADHD may be less aware of their internal affective states or be less valid reporters of those states (Smith, Pelham, Gnagy, Molina, & Evans, 2000; Zucker, Morris, Ingram, Morris, & Bakeman, 2002). Indeed, many studies using the MTPT-C find no correlations between quit status and self-reported emotional reactivity suggesting that MTPT-C measures tolerance of frustration in the moment while self-report measures likely tap trait-related frustration reactivity (Ameral, Palm Reed, Cameron, & Armstrong, 2014; McHugh et al., 2011). It may be that the primary difference in youth with ADHD compared with TD youth lies in the regulation of the behavioral response to frustration rather than in the subjectively rated intensity of the emotion itself. In addition, as affective responses can be affected by medication, it should be noted that some of the children with ADHD were taking stimulant medication during the task (n = 25), which may have altered their perception of task frustration. Furthermore, our results do not suggest that a skills deficit contributed to decreased frustration tolerance in youth with ADHD more so than their peers as there were no group differences in skill on the MTPT-C.
Our main finding is also interesting when considered in the context of the ADHD reward processing literature. Specifically, we found that despite being told that their reward was dependent upon their performance during the frustrating task, youth with ADHD were more likely to quit the task. This result is interesting in light of neuroimaging results that have shown that individuals with ADHD demonstrate hypoactivation of the ventral striatum during reward anticipation indicating that the salience of anticipated rewards is diminished in ADHD (Scheres, Milham, Knutson, & Castellanos, 2007; Strohle et al., 2008). For youth with ADHD, if anticipated rewards are less meaningful, it may negatively affect their ability to persist in the wake of goal-directed behavior when frustrated. For example, the ability to complete a frustrating task such as homework may not be worth the reward of getting a good grade or earning a reward at home for youth with ADHD. In fact, Sagvolden, Johansen, Aase, and Russell (2005) have suggested that due to dopamine hypofunction, youth with ADHD have deficits in the processing of reward cues, which likely contributes to the fact that behavioral symptoms of ADHD often appear resistant to operant conditioning. Alternatively, it may be that, for youth with ADHD, their dysregulated frustration response results in increased engagement of limbic regions, facilitating sensitivity to affective information at the expense of the engagement of cortical systems necessary for regulatory control, making it difficult to engage in goal-directed activity (Oei et al., 2012). Of course, both of these hypotheses require additional testing in youth with ADHD.
Given the high rates of comorbidity between ADHD and ODD, we compared frustration tolerance in youth with ADHD with and without comorbid ODD. Results showed no group differences in frustration tolerance. Furthermore, moderation analyses showed that ODD does not moderate the relationship between ADHD and frustration tolerance. Taken together, our results suggest that the difficulties that youth with ADHD have with frustration tolerance are likely independent of ODD. While these findings may reflect low power to detect this effect, they could also suggest that a lower threshold for frustration in youth with ADHD is more related to core characteristics of ADHD such as inattention, hyperactivity, and impulsivity rather than the associated features of oppositionality, anger, and irritability. Indeed, we found a positive relationship between frustration tolerance and total inattentive symptoms such that youth with higher levels of inattention were more likely to quit the task than those with lower levels of inattention. Surprisingly, we did not find a relationship between hyperactive/impulsive symptoms and frustration tolerance within our sample. It may be that in the wake of frustration, youth with ADHD “tune out” the aversive frustrating stimuli and give up on a task rather than persist, which can greatly impair their academic functioning. Additional research is needed to further explore the relationship between inattention and hyperactive/impulsive symptom dimensions and frustration tolerance.
Our results should also be examined in relation to prior studies of distress or frustration tolerance in youth with ODD. For example, a longitudinal study of distress tolerance in community sample of pre-adolescents (ages 9-13) found that greater persistence on a behavioral distress tolerance task at Year 1 was associated with lower levels of ADHD symptoms at Year 4, but increased levels of ODD symptoms at Year 4, suggesting a positive association between frustration tolerance and ODD symptoms (Cummings et al., 2013). In contrast, ODD was not related to frustration tolerance (i.e., quit status) in our sample. It should be noted that the distress tolerance task used by Cummings et al. (2013) was different from the one used in this study, which may have contributed to differential results. In addition, study design (i.e., Cummings et al. being a longitudinal study vs. this cross-sectional study) may have contributed to different findings.
Moving forward, behavioral frustration tolerance tasks should be used to probe the neural circuitry involved in low frustration tolerance in youth with ADHD. Frustration is a complex affective response that involves the interaction of multiple neural circuits involved in ER including (a) core limbic regions (amygdala [AMG], insula, and orbitofrontal cortex [OFC]) in circuit with reward regions (ventral striatum particularly nucleus accumbens [NAcc]) involved in the assessment of emotional/reward salience and generation of emotion responses, (b) frontal cortical (dorsolateral prefrontal cortex [dlPFC]) regions in circuit with dorsal striatal regions involved in the cognitive control of emotional responses, and (c) regions involved in the interface between emotional and cognitive control circuitry (especially those related to attentional control) including the medial prefrontal cortex (mPFC) and anterior cingulate cortex (ACC; Abler, Walter & Erk, 2005; Haber & Knutson, 2010; Ochsner & Gross, 2005; Ochsner et al., 2009; Phillips, Drevets, Rauch, & Lane, 2003; Phillips, Ladouceur, & Drevets, 2008). Research has shown that deficits within these three circuits are associated with ED in youth with ADHD (Shaw et al., 2014). In TD youth, frustration is associated with increased dorsal and ventral mPFC recruitment suggesting the importance of “top-down” engagement of cognitive and attentional resources to assist in ER. Taken together, research in TD individuals suggests that frustration produces increased activity in both limbic and cognitive control regions, but decreased activity in reward anticipation centers. However, despite demonstrating difficulties with frustration tolerance, there has been no examination of the neural basis of low frustration tolerance in youth with ADHD. It may be that for youth with ADHD, an increased affective response in core limbic regions coupled with poor regulatory control in prefrontal regions results in a decreased threshold for frustration.
A number of limitations should be noted. First, our sample size is small, which may have limited our power to detect findings. Second, we characterized frustration using a singular behavioral task that may not adequately capture such a complex affective response. Moving forward, studies assessing frustration in youth with ADHD should consider a multimodal assessment of frustration (e.g., observational, behavioral, physiological assessment, neuroimaging).
Clinically, the results of this study suggest the importance of addressing poor frustration tolerance in youth with ADHD in treatment. To date, none of the evidence-based treatments for ADHD (i.e., stimulant medication, behavioral parent training) directly target affective responses in youth with ADHD (American Academy of Pediatrics, 2000; Wolraich et al., 2011); however, it could be argued that stimulant medication indirectly targets affective responding via assistance with executive functioning an integral aspect of ER. Although behavioral interventions may help decrease frustration tolerance by setting external parameters on a child’s behaviors, more treatments that target parental socialization of emotions within their youth need to be employed with youth with ADHD (Graziano & Garcia, in press). In fact, using frustrating behavioral paradigms during treatment could allow parents to act as in vivo coaches to their youth’s negative affective responses (Chronis-Tuscano et al., 2014). Biofeedback in which youth receive real-time measures of their own physiological reactivity may also be helpful in making youth with ADHD more attuned to their frustration levels.
Footnotes
Acknowledgements
The authors would like to thank Thorhildur Halldorsdottir, Kristian Owens, and Talia Sacks for all their assistance with the collection of data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.