
Abstract
Introduction
ADHD is characterized by a persistent pattern of inattention, hyperactivity, and impulsivity, and varying degree of impairment and persistence of symptoms into mid-adolescence and adulthood for a high proportion of cases (Wilens & Spencer, 2010). ADHD in adolescence tends to be more subtle with less evident hyperactivity and high rates of psychiatric comorbidity, which often masks the disorder and makes recognition difficult (Barkley, Anastopoulos, Guevremont, & Fletcher, 1991).
Although widely varying prevalence rates have been reported, most epidemiological studies indicate that ADHD affects 4% to 7% of children and adolescents (Faraone, Sergeant, Gillberg, & Biederman, 2003; Polanczyk & Rohde, 2007). A meta-analysis that estimated worldwide prevalence of ADHD in children and adolescents reported a rate of 5.29% (Polanczyk, de Lima, Horta, Biederman, & Rohde, 2007). There are only few Indian studies on the prevalence of ADHD. In a two-stage community study of 1,578 children aged 4 to 16 years, 1.5% were diagnosed to have ADHD (Srinath et al., 2005). A small study among adolescent school children reported a prevalence of 7.2% (Juneja, Sairam, & Jain, 2014). Worldwide, boys are more likely to be affected than girls with gender ratio reported varying between 2:1 and 9:1 depending on the setting and subtype assessed (Rucklidge, 2010).
Compared with their non-ADHD peers, adolescents with ADHD experience a range of cognitive, social, and behavioral difficulties (Sciberras, Roos, & Efron, 2009). These result in a number of negative outcomes including poor academic performance (Biederman et al., 2006), increased risk of substance use disorder (Charach, Yeung, Climans, & Lillie, 2011), depression (Green, Wong, Atkins, Taylor, & Feinleib, 1999), suicide (James, Lai, & Dahl, 2004), and high rates of abuse (Cengel-Kültür, Cuhadaroğlu-Cetin, & Gökler, 2007).
Although ADHD has been recognized to be a significant public health problem owing to its prevalence, morbidity, and range of negative outcomes, there are only few studies that have looked into participants who have clinical significant symptoms of ADHD in the community without a diagnosis. It is in this background that we have studied here the self-reported prevalence of ADHD symptoms in a large sample of school-going adolescents in the state of Kerala, India. In addition, we specifically report on academic performance, psychological distress, suicidal behavior, substance/alcohol abuse, and history of sexual abuse in this population. The data for this study were collected as part of a larger study by the National Rural Health Mission (NHRM; Kerala, India), a government initiative to study patterns of substance and alcohol abuse in adolescents.
Method
Participants
We conducted a cross-sectional survey in one division of Classes (year) 8, 10, and 12 chosen randomly from 73 schools selected by cluster random sampling in the District of Ernakulam, Kerala state, India.
A total of 7,560 students (97.7% of the total of 7,740 eligible students) who were present on the day of the survey were invited to participate, of whom, 7,150 successfully completed the questionnaire. Four hundred ten (5.5%) questionnaires had to be discarded as they were found to have substantial missing items. In the sample analyzed, 3,631 (50.8%) were boys and 3,519 (49.2%) were girls with a mean age of 15.3 years (range = 12-19 years).
Design and Procedure
A self-administered questionnaire was distributed to the participants by the school junior public health nurses (JPHNs) who were trained to administer and supervise the survey and to answer any queries. To ensure privacy, students were seated sufficiently apart. The questionnaires were administered only to students who gave oral consent. Students were also told that if they required any help with regard to issues surveyed, they could approach the School JPHNs, who had received training in handling these issues. The questionnaire was initially prepared in English and translated into Malayalam (the vernacular language) and back translated to ensure that there have been no errors. Institutional ethical approval was received from the Government Medical College, Ernakulam. Information about the survey was provided to the parent–teacher association.
Questionnaire
In addition to socio-demographic data, which was in the form of checklist (age/sex/structure of family/area of residence/socio-economic status/religion/academic performance), the questionnaire included instruments that assessed the following domains:
ADHD
The Barkley Adult ADHD Rating Scale–IV (BAARS-IV)–Childhood Symptoms self-report, was used. It asks students to rate their behavior for features of ADHD between the ages of 5 and 12. The scale consists of 18 questions (nine each for features of inattention and hyperactivity–impulsivity) with Likert-type scale responses with four options ranging from never to always. The BAARS-IV Childhood Symptoms self-report scale can be scored to yield three raw scores: ADHD inattention, ADHD hyperactivity–impulsivity, and ADHD total score. The total scores thus obtained were compared with norms provided to obtain percentile scores for features of ADHD. A raw score of greater than 32 for inattention, greater than 31 for hyperactivity, and 60 and above for combined ADHD was taken as cutoff (all indicating the 99 percentile; Barkley, 2011). Although this instrument has not been validated in India, the scale has high internal consistency, good inter-observer agreement, and high test–retest reliability (Barkley, 2011).
Substance use
The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) was used to assess lifetime use of alcohol and tobacco. The ASSIST has good test–retest reliability, and high discriminative validity (WHO ASSIST Working Group, 2002).
Psychological distress
Kessler’s Psychological Distress Scale (K10) assessed frequency of depressive and anxiety symptoms over the past month on a 4-point Likert-type scale (Andrew & Slade, 2001). This tool has been validated to screen for common mental disorders among adolescents in developing country settings (Huang, Xia, Sun, Zhang, & Wu, 2009). Scores range from 10 to 50, with higher scores reflecting more severe symptoms.
Suicidality
Two questions were used to assess lifetime suicidality: “Have you ever thought of committing suicide in your life?” and “Have you made a suicidal attempt in your lifetime?”
Sexual abuse
Four questions modified from the Child Abuse Screening Tool–Children’s Version (ICAST-C), an instrument that has been validated in India (Zolotora et al., 2009), were asked with regard to lifetime exposure to sexual abuse: (a) Has someone misbehaved with you sexually against your will? (b) Has someone forced you to look at pornographic materials against your will? (Questions a and b—non-contact sexual abuse) (c) Has someone demanded or forced you to fondle or fondled you against your will? (d) Has someone forced you into a sexual act against your will? (Questions c and d—contact sexual abuse).
Statistical analysis
SPSS version 15 was used for all analyses (SPSS, 2006). The self-reported prevalence of symptoms of ADHD inattentive type (ADHD-I), ADHD hyperactive–impulsive type (ADHD-H), and ADHD combined type (ADHD-C) was calculated. For the purposes of further analysis, only symptoms of ADHD-C were used. Socio-demographic variables were compared between those who had symptoms of ADHD-C and those who did not, using chi-square test. Academic performance, substance use, self-reported prevalence of psychological distress, suicidality, and sexual abuse were compared between the two groups using binary logistic regression analysis. All tests were two tailed, and statistical significance was set at p < .05.
Results
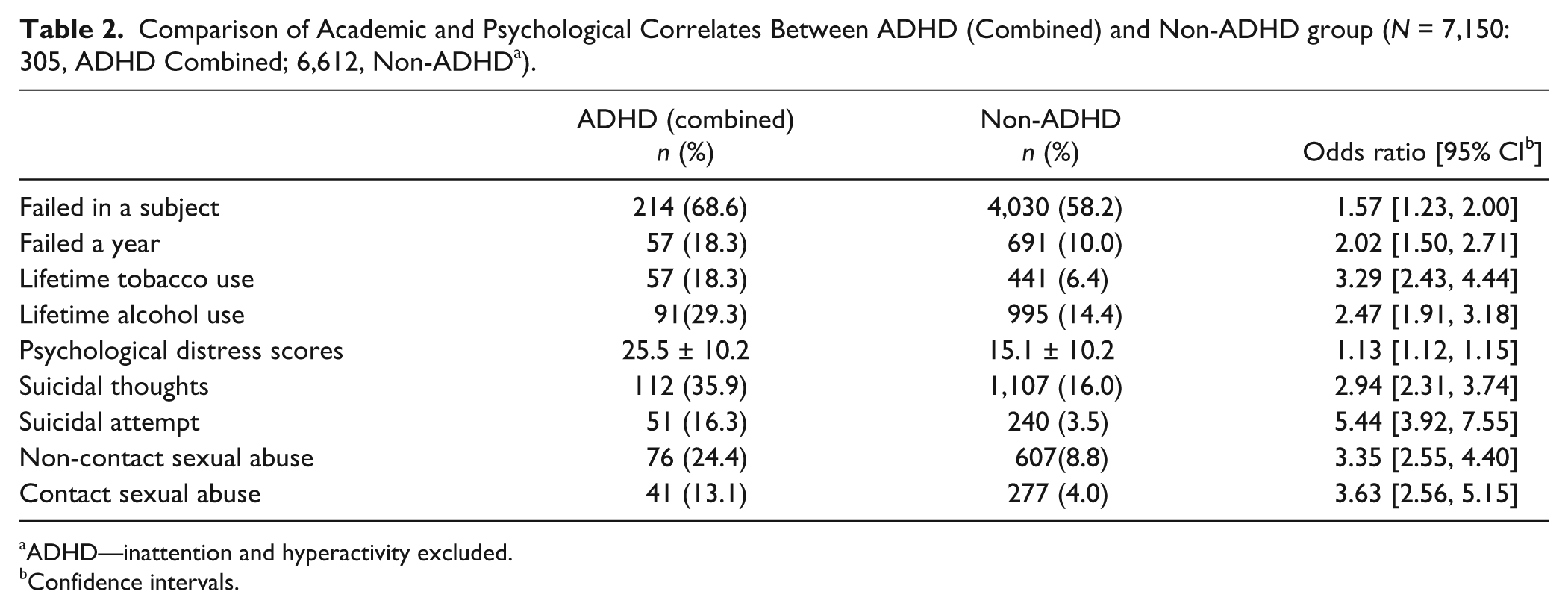
The prevalence of symptoms ADHD-I, ADHD-H, and ADHD-C are described in Table 1. The prevalence of symptoms of ADHD (all variants) in males was significantly more common than females. Students reporting ADHD-C did not differ from the non-ADHD group with regard to any of the socio-demographic variables. In the bivariate analysis, students who reported symptoms of ADHD-C had significantly higher odds of poorer academic performance (failure in subjects/year), alcohol use, tobacco use, psychological distress, suicidal thoughts, suicidal attempts, and contact and non-contact sexual abuse (Table 2).
Prevalence of Self-Reported ADHD Symptoms.

Comparison of Academic and Psychological Correlates Between ADHD (Combined) and Non-ADHD group (N = 7,150: 305, ADHD Combined; 6,612, Non-ADHD a ).
ADHD—inattention and hyperactivity excluded.
Confidence intervals.
Discussion
The prevalence rates of self-rated ADHD symptoms in our sample were 4.3% for ADHD-C, 1.8% for ADHD-H, and 1.4% for ADHD-I with a male predominance. Even though we did not do a diagnostic confirmation, the prevalence rates of ADHD symptoms in our sample is similar to the 5.29% rate found in the largest meta-regression analysis of ADHD prevalence to date (Polanczyk et al., 2007). There are many other studies reporting widely varying prevalence rates ranging from 1% to 20% (Faraone et al., 2003). In comparison with other Indian studies, the rate of ADHD in our sample is higher than the rate of ADHD of 1.5% reported from a community sample (Srinath et al., 2005), where a clinical diagnosis of ADHD was made but lower than the rate of 7.2% reported from a small adolescent school sample (Juneja et al., 2014). This variance in prevalence rates of ADHD could be owing to the methodological differences across studies (Polanczyk et al., 2007). Our finding of male predominance replicates finding from various studies across the world (Polanczyk et al., 2007; Polanczyk & Rohde, 2007; Staller & Faraone, 2006). The male preponderance in ADHD mirrors what is seen for other neurodevelopmental disorders such as autism spectrum disorder and intellectual disability.
Although the cross-sectional nature of our study precludes any conclusion with regard to causality, our students reporting ADHD symptoms had a number of negative correlates. The poor academic performance in our adolescents who reported ADHD symptoms have been reported prior (Barkley et al., 1991; Biederman & Faraone, 2005; Biederman et al., 2006). Deficits of attention, subtle impairments of intelligence, and other psycho-social vulnerabilities have been postulated to act additively to contribute to the poor academic performance among ADHD participants (Biederman & Faraone, 2005; Biederman et al., 2006).
Our students who had ADHD symptoms had a three-fold risk of tobacco use and two-fold risk of alcohol use, which is similar to findings in a meta-analytic review, which showed youth with ADHD showed substantially higher likelihood of cigarette smoking (2.4×) and substance use disorder (1.5×; Charach et al., 2011). Multiple studies from across the world have also reported high prevalence of alcohol and nicotine use/abuse in ADHD patients (Biederman & Faraone, 2005; Biederman et al., 2006; Couwenbergh et al., 2006). These findings are so robust that researchers are increasingly focusing on theories of shared family, genetic, and neurobiological vulnerabilities, which could be contributing to the higher risk, in addition to the traditional theories of “impulse dysregulation” and “self-medication” (Faraone & Biederman, 2004). High level of psychological distress and suicidality found in our ADHD participants adds to already existing evidence with regard to the link between ADHD, depression (Green et al., 1999), and suicidality (James et al., 2004). ADHD symptoms reporting students self-reported high rates of contact and non-contact sexual abuse. Studies have shown high rates of ADHD (22.2%) have been diagnosed in children exposed to abuse (Cengel-Kültür et al., 2007). The negative correlates that we identified in our students with ADHD symptoms are similar to findings from studies that also diagnosed ADHD, indicating that self-reported ADHD symptoms could be as disabling as ADHD. Furthermore, this interaction between ADHD symptoms, poor academic performance, substance use, psychological distress, abuse, and suicidality could form a developmental matrix of risk for future pathology.
The findings reported here should be evaluated in light of its strengths and limitations. The strengths of the study include that this is one of the largest studies on self-reported ADHD symptoms in an adolescent population from India. Structured instruments were used for assessments where possible. Many of the correlates of ADHD symptoms being reported have been examined for the first time from a community sample in India. The study had several limitations. First, we are reporting symptoms of ADHD that cross the diagnostic threshold based only on the self-reported responses of the students. No diagnostic interview or information from other sources was collected to confirm the diagnosis. Second, formal validation exercise of the instruments used was not performed on the sample population. Finally, our findings from Kerala may not be easily generalizable to students from other regions in India or other countries with varying cultural differences.
To conclude, the findings that self-reported ADHD symptoms in adolescents from Kerala, India, are not uncommon and are associated with number of negative correlates similar to studies in participants with diagnosis of ADHD have wider public health implications. There is, thus, a need for methodologically rigorous studies to further explore this area. In the meanwhile, the study adds evidence to the continuing need to sensitize all stakeholders of the need for early comprehensive intervention to manage this disabling disorder with lifelong implications.
Footnotes
Acknowledgements
We wish to thank Mr. Ajaya Kumar and team who helped with the data entry.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was partly funded by National Rural Health Mission (Kerala), India.