
Abstract
Introduction
ADHD is a neurodevelopmental disorder, characterized by persistent inattention, hyperactivity, and impulsive behavior with a male preponderance of 3-4:1 (Thapar & Cooper, 2015). Prevalence estimates vary, mostly due to differences in classification, as the International Classification of Diseases–10 (ICD-10) is more strict than the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria (Polanczyk, de Lima, Horta, Biederman, & Rohde, 2007; Skounti, Philalithis, & Galanakis, 2007). The most recent global prevalence estimate is 3.4% (Polanczyk, Salum, Sugaya, Caye, & Rohde, 2015). ADHD is highly heritable and evidence supports a role for large, rare copy number variants (Akutagava-Martins, Rohde, & Hutz, 2016; Hawi et al., 2015; Jarick et al., 2014; Martin, O’Donovan, Thapar, Langley, & Williams, 2015). However, it is also being increasingly recognized that a gene–environment interaction may contribute to ADHD risk (Ficks & Waldman, 2009). For example, the serotonin transporter 5-HTTLPR (serotonin-transporter-linked polymorphic region) has been shown to moderate the effect of stress on ADHD severity (Shaw, 2015; van der Meer et al., 2015). Furthermore, recent studies have provided evidence that ADHD is associated with differential patterns of DNA methylation (an epigenetic modification) in genes relevant to children’s activity levels (Wilmot et al., 2016). As epigenomic changes are at the interface of the interaction between genes and the environment, this supports a role for a gene–environment interaction in the etiology of ADHD. Therefore, it is important to define the environmental influences that may affect the development of ADHD.
Given that the in utero environment is a critical determinant of neurodevelopmental outcome, a number of pre- and perinatal risk factors have been suggested to increase the risk of ADHD in affected children (Mill & Petronis, 2008). Building on this premise, one potential risk factor may be fetal exposure to hypertensive disorders of pregnancy (HDP). HDP are frequent gestational complications that affect 10% to 15% of pregnancies (Nelson-Piercy, 2015). HDP is an umbrella term for several hypertensive conditions of pregnancy, including chronic hypertension, gestational hypertension (GHT), preeclampsia (PE), eclampsia, and chronic hypertension with superimposed PE (Gillon, Pels, von Dadelszen, MacDonell, & Magee, 2014; Olson-Chen & Seligman, 2016).
HDP has been linked to mental and behavioral disorders in children, including ADHD (Getahun et al., 2013; Mann & McDermott, 2011; Silva, Colvin, Hagemann, & Bower, 2014). However, results in this area are inconsistent with a Swedish and a Finnish study finding no independent association between PE and ADHD (Gustafsson & Kallen, 2011; Strang-Karlsson et al., 2008). These findings highlight the need to study the effects of HDP on ADHD risk in large cohorts. The objective of the current study was to assess the association between HDP and the risk of ADHD and behavioral difficulties at the age of 7 years using a large, contemporary, representative British birth cohort.
Method
Data Source
The Millennium Cohort Study (MCS) is an ongoing survey in the United Kingdom (Connelly & Platt, 2014). The first survey was implemented in 2001/2002, when infants were 9 months of age (Dex & Joshi, 2004). Subsequent surveys were carried out when the children were ages 3 (2004/2005), 5 (2006), 7 (2008), and 11 (2012) years. Each survey was approved by the London Medical Research and Ethics Committee, and as this was secondary data analysis, no additional ethical approval was required. Permission for use of the data was received from UK Data Service (2012-2016).
Study Population
The MCS participants were selected through stratified cluster sampling. Sampling was stratified by region and electoral ward. Sample sizes were based on ward size, ethnic composition, and social disadvantage of the ward, with ethnically diverse and socially disadvantaged wards oversampled to allow for sufficient information to be collected on these groups. The detailed sampling strategy has been described elsewhere (Plewis, 2007). For the current study, data of the first (age 9 months) and fourth waves (age 7 years) were used. There were 13,363 families who participated in both waves. After the exclusion of 171 twins and triplets, the cohort included 13,192 children. The weighted population size was 13,500 children.
Exposure Measure
For the ascertainment of HDP (Wave 1), mothers were asked whether they had any problems during pregnancy which required medical attention (“Did you have any illnesses or other problems during your pregnancy that required medical attention or treatment?”). When they answered in the affirmative, categories were given for specification. Women who selected “raised blood pressure, eclampsia/preeclampsia, or toxaemia” were categorized as having HDP.
Outcome Measures
For the assessment of ADHD (Wave 4), parents were asked whether a doctor or health professional had ever told them that their child had ADHD (“Has a doctor or health professional ever told you that [cohort child’s name] had any of the following problems?”). If the answer for ADHD was “yes,” the child was considered to have ADHD.
Parent-reported behavioral difficulties were assessed through the Strength and Difficulties Questionnaire (SDQ), a validated behavioral assessment tool for children aged 4 to 17 years (Stone et al., 2015). The questionnaire is subdivided into five subscales: Emotional Problems, Conduct Problems, Hyperactivity, Peer Problems, and Prosocial Behaviors. Each subscale consists of five questions, whereby each answer takes on a value between 0 and 2. The total difficulties score is generated by adding up the values of the first four scales, leading to a possible score between 0 and 40, where higher scores indicate an increasing level of behavioral difficulties. Children were considered to have “behavioral difficulties” if they received a score higher than Goodman’s widely used cutoff point of 17. This cutoff corresponds to the top 10% of scores and is considered to be clinically relevant based on a large U.K. survey (Goodman, Ford, Corbin, & Meltzer, 2004; SDQInfo, 2013).
The SDQ subscale assessing hyperactivity issues was used as the third outcome measure. Possible hyperactivity scores ranged from 0 to 10, with higher scores indicating higher levels of hyperactivity. The cutoff at 7 points was used to determine “signs of hyperactivity” according to the same survey assessment (SDQInfo, 2013).
Potential Confounders
Potential confounders were chosen based on previous literature. Demographic and socioeconomic variables included the following: infant sex (Sciberras, Ukoumunne, & Efron, 2011), family’s poverty status (Hjern, Weitoft, & Lindblad, 2010), ethnicity (Getahun et al., 2013), maternal age at birth (Khalil, Syngelaki, Maiz, Zinevich, & Nicolaides, 2013), single parenthood (Hjern et al., 2010), and maternal education (Pastor & Reuben, 2008). Pregnancy- and delivery-related factors included maternal smoking (Gustafsson et al., 2010) and alcohol consumption during pregnancy. Further influences included parity (“first born” vs. “not first born child”; Ananth & Basso, 2010), preterm delivery (Bhutta, Cleves, Casey, Cradock, & Anand, 2002), and small for gestational age (SGA; Lahti et al., 2006), defined as birthweight below the 10th customized percentile. Variables assessing the maternal health status were gestational diabetes, prepregnancy body mass index (Rodriguez et al., 2008), depression (Lesesne, Visser, & White, 2003), and mental disorder.
Statistical Analysis
Crude and adjusted logistic regression models were used to examine the association between HDP and ADHD and SDQ scores. First, univariate analyses were conducted to examine the association between HDP and each of the three outcome measures. Each potential confounder was separately tested and included into the final models if it changed the association between HDP and ADHD by at least 10%. As none of the variables fulfilled the criteria, a more inclusive cutoff point of 5% was used. Maternal age and poverty status were below the 5% mark (3.7% and 4.8%, respectively), but were still included as found to be important based on previous literature, and had an effect on the association when included in the model together (Hjern et al., 2010; Mann & McDermott, 2011). To adjust for the disproportionate stratified sampling design, survey weights were used for all the analyses. Plewis has previously shown that the first survey weights did not differ materially from the combined sample and loss to follow-up weight at age 7 years. Therefore, the first survey weights were used in the present study (Plewis, 2007). When weighted, the sample is representative of children born in the United Kingdom in the year 2000/2001 (Plewis, 2007). Variables were included in the statistical models as presented in Table 1. Analyses were repeated with stratification by infant gender and parity.
Overall Characteristics of the Study Population and in Relation to HDP.
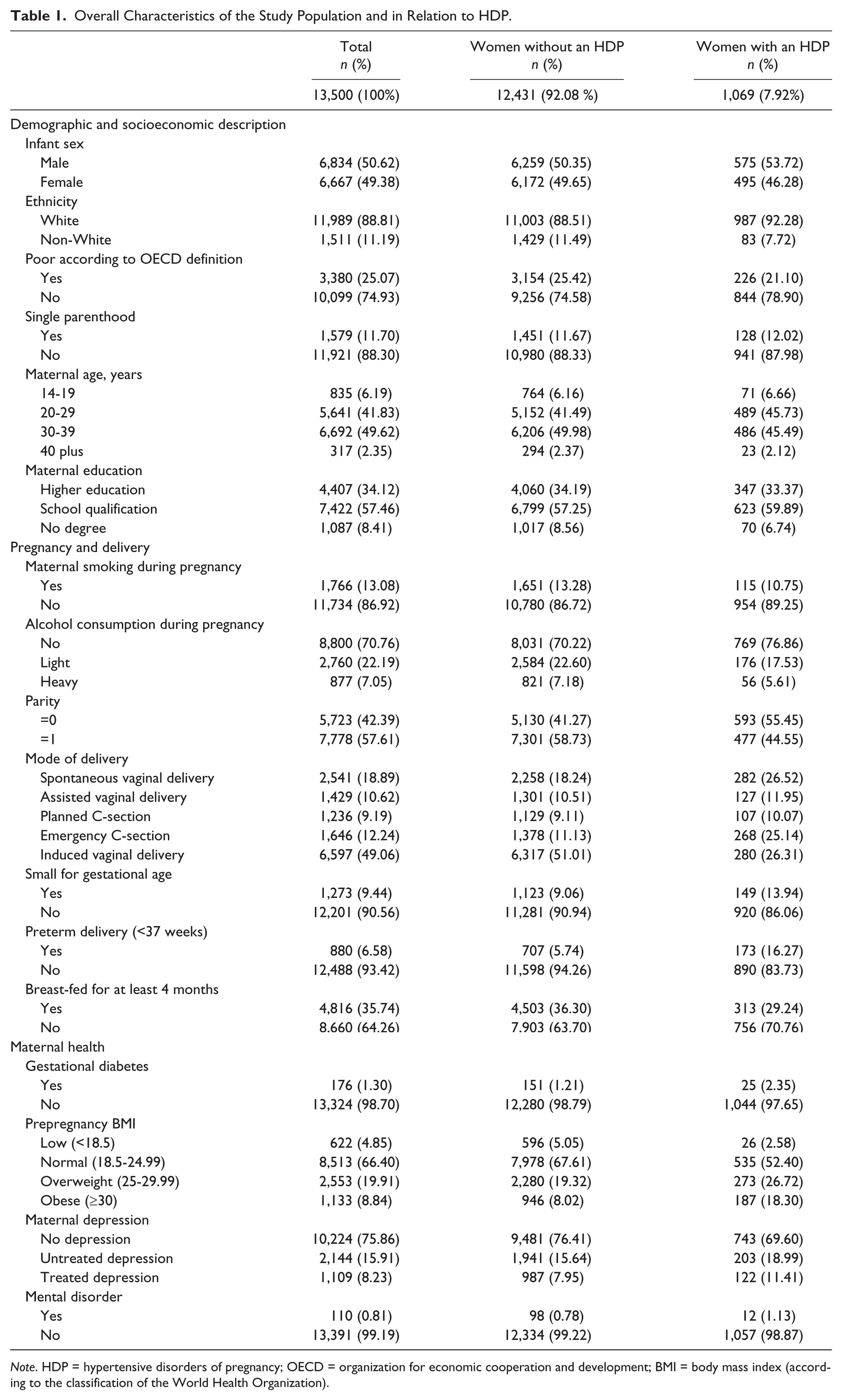
Note. HDP = hypertensive disorders of pregnancy; OECD = organization for economic cooperation and development; BMI = body mass index (according to the classification of the World Health Organization).
Several sensitivity analyses were performed to assess the strength of the observed associations. Regression models were repeated for the outcome of ADHD only, excluding (a) preterm births (<37 weeks gestation), (b) preterm and early term births (all births before 39 gestational weeks), (c) SGA infants, (d) offspring of women with prepregnancy chronic hypertension, and (e) offspring of women with depression. We repeated the analysis adjusting for birthweight instead of SGA. To assess the potential mediating effect of the mode of delivery and breast feeding, the variables were individually added into the final model; p < .05 was considered statistically significant. Analyses were performed using SAS 9.4.
Results
Descriptive Results
A total of 18,552 families participated in the first wave survey. Of these, 13,363 families participated in the fourth wave survey, including 13,192 singleton births. When this was weighted, it produced an effective sample size of 13,500. Characteristics of the weighted study sample with regard to HDP are presented in Table 1. HDP were reported by 1,069 (7.9%) women. Alcohol and tobacco intake during pregnancy was reported by 29.2% and 13.1%, respectively, whereas the consumption of both was lower in women with HDP. Primiparae women were more likely to have HDP than multiparae women (55.5% vs. 44.5%). Gestational diabetes was reported by 1.3% of the women, with almost twice the occurrences in mothers who reported HDP versus those who did not (2.4% vs. 1.2%). About 28.8% of mothers were overweight or obese before pregnancy; this proportion was larger in HDP women (45% vs. 27.3%). Maternal depression was present in 24.1%, and those who reported HDP were more likely to have treated (11.4% vs. 8%) and untreated depression (19% vs. 15.6%) as compared with women with no HDP. More details are summarized in Table 1.
Data on ADHD status were obtained from 13,420 (99.4%) participants and reported in 166 children (1.2%). The SDQ and hyperactivity scores were available on 13,178 (97.6%) and 13,228 (98.0%) children, respectively. An abnormal SDQ score was present in 857 (6.5%) children. The Hyperactive subscale showed abnormal results for 1,602 children (12.1%). Prevalence of abnormal SDQ and hyperactivity scores were more than sevenfold among children with an ADHD diagnosis, compared with the ones without (Figure 1).
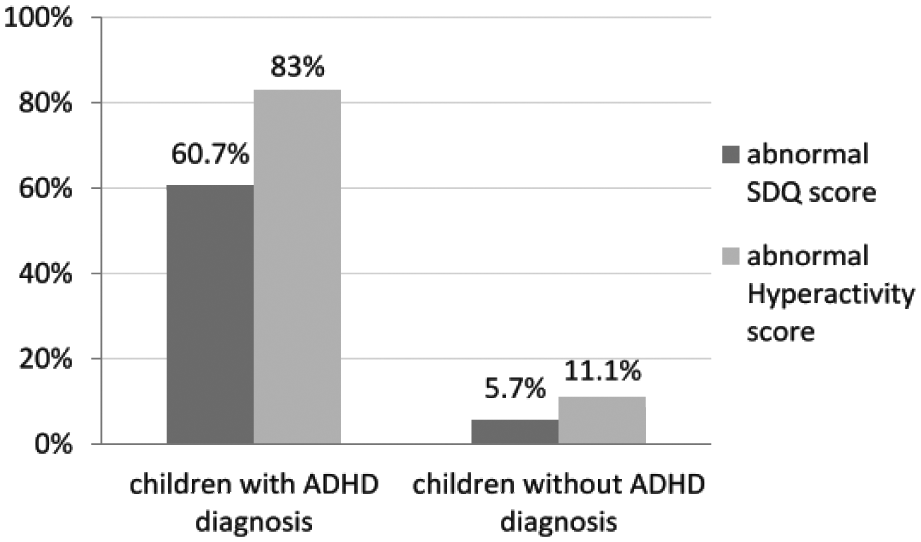
Abnormal SDQ/hyperactivity score among children with and without ADHD diagnosis.
Results from the logistic regression analyses on the association between HDP and ADHD, abnormal SDQ, and hyperactivity scores are displayed in Table 2. There was a significant association between HDP and ADHD in both crude (odds ratio [OR] = 1.89, 95% confidence interval [CI] = [1.11, 3.20]) and adjusted analyses (OR = 1.78, 95% CI = [1.03, 3.07]). There was no evidence to support an association between HDP and the risk of abnormal SDQ scores in either the crude (OR = 0.96, 95% CI = [0.72, 1.29]) or adjusted analysis (OR = 0.94, 95% CI = [0.69, 1.29]). There was a small, but nonsignificant, association between maternal HDP and the risk of abnormal hyperactivity scores (adjusted OR = 1.22, 95% CI = [0.97, 1.53]).
Logistic Regression for the Association Between HDP and Behavioral Outcomes in Children.
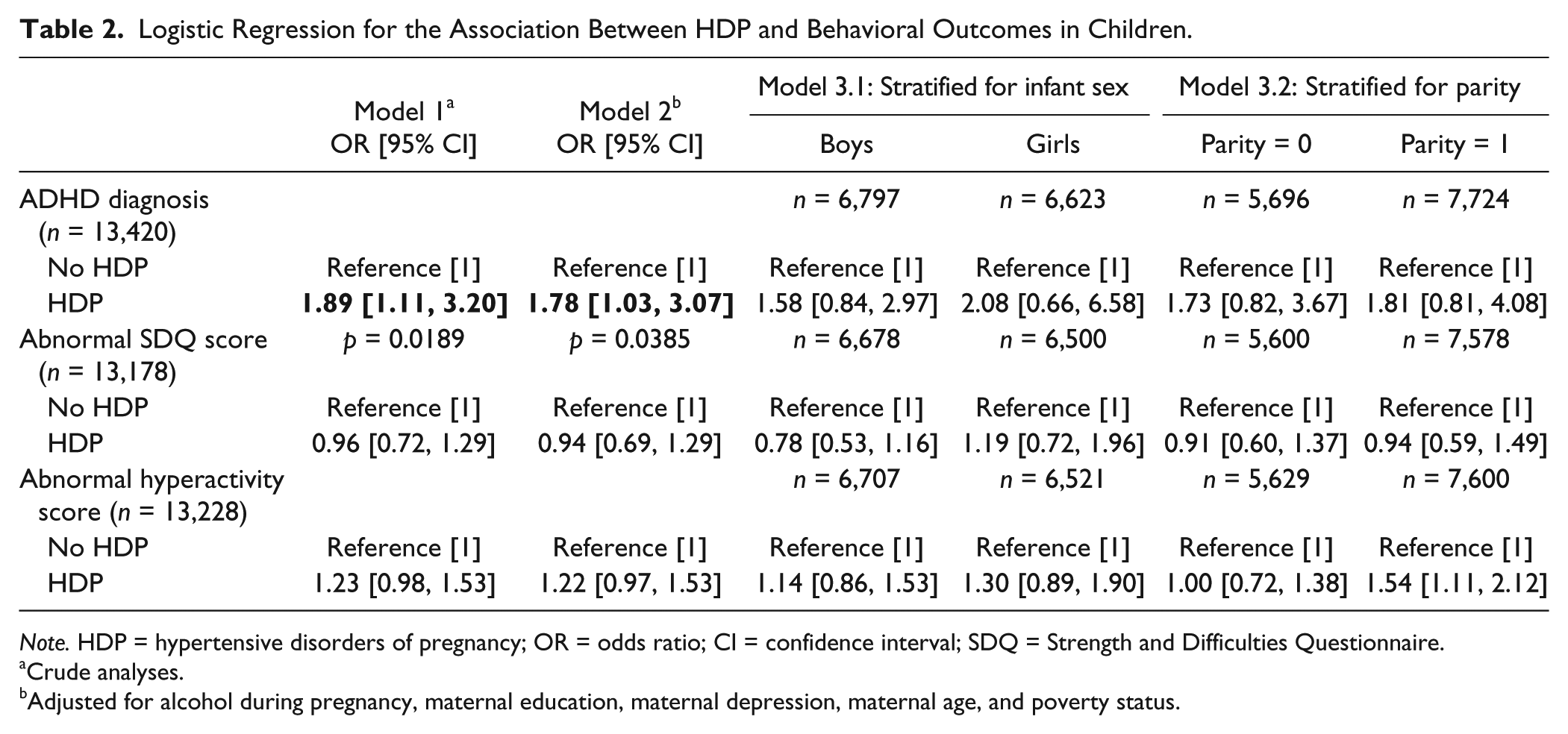
Note. HDP = hypertensive disorders of pregnancy; OR = odds ratio; CI = confidence interval; SDQ = Strength and Difficulties Questionnaire.
Crude analyses.
Adjusted for alcohol during pregnancy, maternal education, maternal depression, maternal age, and poverty status.
The stratified analyses by infant sex showed that the association for all outcomes seemed to be stronger for girls than for boys, but these effects by sex were not significantly different (χ2 for heterogeneity p = .68; Table 2). In the stratified analyses for parity (Table 2), the association between HDP and ADHD, and HDP and increased hyperactivity, seemed to be increased in multiparae women, while there was no association with an abnormal SDQ score. Multiparae women had a significant association between HDP and an abnormal hyperactivity score (OR = 1.54, 95% CI = [1.11, 2.12]), but the interaction was not statistically different (χ2 for heterogeneity p = .07).
Sensitivity Analyses
Sensitivity analyses were performed within the fully adjusted model to evaluate possible impacts of additional variables, using the main outcome ADHD (Table 3). The exclusion of preterm births (Model 4a), both preterm and early term infants (Model 4b), or SGA infants (Model 5) did not change the results materially. The exclusion of chronic hypertensive women (Model 6) led to a slight decline in the association (OR = 1.68, 95% CI = [0.96, 2.94]), which was no longer statistically significant. The exclusion of women with depression (Model 7) led to a slight increase in the relationship between HDP and ADHD (OR = 2.15, 95% CI = [1.05, 4.43]). Adjusting the model for birthweight instead of SGA did not change the results materially.
Sensitivity Analyses Using Logistic Regression for the Association Between HDP and ADHD.
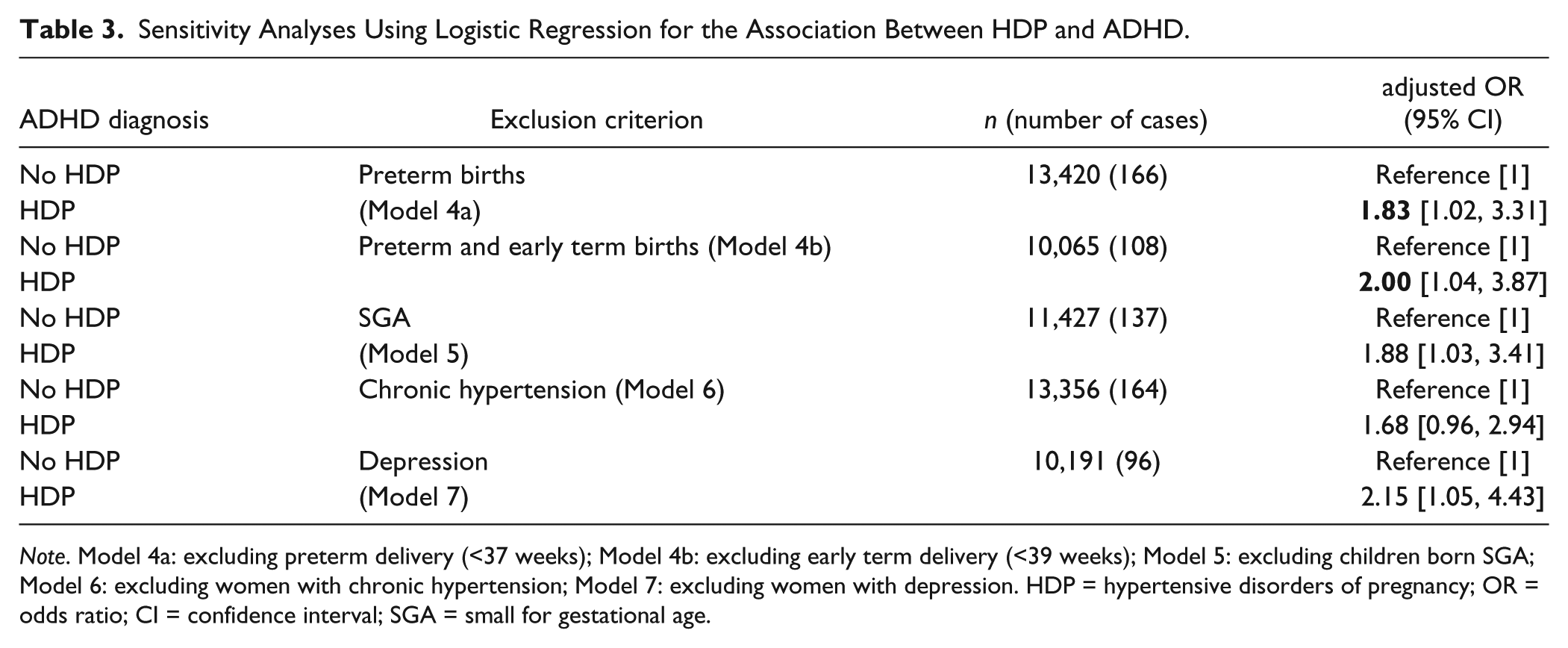
Note. Model 4a: excluding preterm delivery (<37 weeks); Model 4b: excluding early term delivery (<39 weeks); Model 5: excluding children born SGA; Model 6: excluding women with chronic hypertension; Model 7: excluding women with depression. HDP = hypertensive disorders of pregnancy; OR = odds ratio; CI = confidence interval; SGA = small for gestational age.
Obstetric mode of delivery and breast feeding were added to the fully adjusted model to assess a potential mediating effect on the association between HDP and ADHD. Mode of delivery appeared to explain a small part of the association, reducing the OR slightly (OR = 1.68, 95% CI = [0.95, 2.97]). Breast feeding did not change the association materially (OR = 1.78, 95% CI = [1.03, 3.07]).
Discussion
The aim of this study was to investigate the association between HDP and ADHD at 7 years of age. HDP was associated with an almost twofold increased risk of ADHD after controlling for a range of potential confounders. However, there was no association with overall behavioral difficulties or high hyperactivity scores in children, as measured by the SDQ.
There is little research about the impact of HDP on the development of behavioral difficulties in children. Mann and McDermott (2011) reported a 20% increased odds of ADHD in children exposed to PE, using a multiyear cohort of more than 140,000 children from the United States. This small association, compared with our observed association, could potentially be explained through differences in ADHD definitions, as the DSM classification used in their study is more inclusive than ICD classification which is generally used for diagnosis in the United Kingdom (Taylor et al., 2009). This interpretation would explain the ameliorated effect of HDP on the hyperactivity outcome as measured by the SDQ. It is possible that the effect of HDP on ADHD may increase with the severity of behavioral difficulties and hyperactivity in children. Another U.S. study reported a 34% increased odds of ADHD in relation to PE, using California’s health system specific guideline for ADHD diagnosis, which again, is more inclusive than the ICD definition of ADHD (Getahun et al., 2013). An Australian study found PE to be associated with a 20% to 40% increased risk of ADHD in both boys and girls in several statistical models (Silva et al., 2014). These results support the larger association for girls compared with boys found in the current study, though both findings were not statistically significant.
Conversely, a Swedish study reported no association between PE and ADHD and mental and behavioral disorders (Gustafsson & Kallen, 2011). The study examined several perinatal risk factors, including maternal age, smoking, and PE, and found weak associations with ADHD. The discrepancy between Gustafsson and Kallen’s findings and the present study may be related to different cohort age, as their study population was born between 1986 and 1996, compared with 2001 and 2002 in the present study. It could also be related to the definition of the exposure, where they examined the effect of PE on ADHD, while we examined the effect of HDP.
As HDP are likely to influence gestational age and mode of delivery, the effects of these variables were tested in sensitivity analyses. Some studies reported that preterm births and being SGA were positively associated with ADHD (Bhutta et al., 2002; Lahti et al., 2006). In our study, however, excluding preterm births, preterm and early term births and SGA babies from the logistic models did not have a material effect on the association between HDP and ADHD. The risk factors and the pathophysiology of chronic hypertension and newly developed hypertension during pregnancy (GHT, PE) differ. Therefore, we performed a sensitivity analysis excluding chronic hypertensive women, which lead to a slight decrease of the association. This suggests that chronic hypertension may explain some of the association, but that pregnancy specific conditions are responsible for the majority of the relationship. Similarly, adjusting for the potential mediating effect of mode of delivery partly explained the observed association.
Strengths and Limitations
This study has several strengths. First, we used a large prospectively collected data set, which includes representative information on a contemporary U.K. population. The prospective design reduces the chance of recall bias of participants. Second, we had access to a wide range of variables, allowing for the adjustment of many potential confounders, including maternal age, depression, and smoking, among others. Third, we were able to include the previously validated and well-established SDQ score measure as an additional outcome, providing a more comprehensive study of the impact of HDP on ADHD and child behavior. The abnormal SDQ score is linked with 15-fold increased odds of psychiatric disorders (Goodman, 2001). Therefore, the study of the SDQ measure may have allowed us, indirectly, to examine psychiatric outcomes that were not specifically measured in the study cohort. Fourth, the response rates in the first and fourth wave of the MCS were 82% and 72%, respectively (Hansen, Jones, Joshi, & Budge, 2010), which provides a high generalizability of the findings. Similarly, outcomes were reported for the great majority of the sample (>97%).
Some limitations of this study should be considered. First, although the main outcome definition was based on the parent report of a doctoral diagnosis, data were anonymized, and thus, it was not possible to validate reported diagnosis. It is possible that parents were influenced by social desirability and stigma connected to an ADHD diagnosis. The prevalence found in this study is slightly lower compared with the findings of another U.K. survey (1.2% vs. 1.6%; Green, McGinnity, Meltzer, Ford, & Goodman, 2005). This and the larger variation to a recent global estimate at 3.4% may both be explained by a difference in the included ages (diagnosis at age 7 vs. up to age 10 and 18 years, respectively; Polanczyk et al., 2015). Different disorder classifications, as well as cultural and country specific influences, such as the acceptance of the disorder or targeted screening programs, might influence prevalence estimates. Second, information collected through the SDQ relied on the subjective evaluation of parents, though the scale has been widely used and found to be valid and reliable to screen for mental health problems (Bourdon, Goodman, Rae, Simpson, & Koretz, 2005; Goodman, 2001). Third, the exposure definition did not distinguish between the different hypertensive conditions, such as PE, but was rather assessed as an umbrella term. This was due to lack of data on specific hypertensive disorders in the MCS. This led to a limited comparability with other studies, which often focus on one specific hypertensive disorder. The sensitivity analyses, excluding chronic hypertensive women, were performed to partly adjust for this and to look at women with a newly developed hypertensive disorder during pregnancy only. As the current study found a clear association between HDP and ADHD in general, further research is required to determine whether a specific type of HDP is driving the association, and whether the association is specific to ADHD. Fourth, similar to all observational research, we cannot rule out the possibility that the observed association is due to unmeasured environmental factors, such as hypertension medication or genetic residual confounding. It should be noted, however, that there was a limited material impact on the observed association after adjusting for a wide range of confounders. Fifth, as the first survey took place 9 months after delivery, it was not possible to account for the time of onset and severity of the condition, and may have been subject to recall bias. However, it has been found that self-reported information on HDP was accurate from 2 months to 27 years after delivery (Falkegard, Schirmer, Lochen, Oian, & Acharya, 2015; Gresham et al., 2015). Although the reported prevalence of HDP in the current study (7.9%) was similar to a national estimate of HDP for the same years (7%; Government Statistical Service, 2002), misclassification of the exposure cannot be ruled out. Sixth, heritability of ADHD could not be controlled for, as information on family history was not available.
Potential Mechanisms
The molecular basis of the link between HDP and ADHD is an important question for future research. Interestingly, neuroanatomical alterations in the cerebellum, temporal lobe, brain stem, and right and left amygdalae have been described in children from pregnancies complicated by PE (Ratsep et al., 2015). Furthermore, neuroanatomical alterations in these regions have been implicated in ADHD (Schneider, Retz, Coogan, Thome, & Rosler, 2006). The causative molecular basis of these changes will be important to identify; however, the maternal inflammatory pathway may be a leading candidate in this regard. For example, it has recently been shown that activation of effector T-lymphocytes and maternal interleukin-17a (IL) in the fetal brain in response to maternal immune activation leads to behavioral disturbances and an abnormal cortical phenotype in affected offspring (Choi et al., 2016). Given the increased prevalence of circulating IL-17-producing T-lymphocytes in PE (Darmochwal-Kolarz et al., 2012; Toldi, Rigo, Stenczer, Vasarhelyi, & Molvarec, 2011), it is tempting to speculate that maternal IL-17 dysregulation in HDP may be the molecular link between HDP and an increased risk of ADHD in affected offspring.
Conclusion
The findings of this study suggest that children who were exposed to HDP are at higher risk of ADHD by age 7 years, even after adjusting for several potential confounders. Further research is needed to understand the possible mechanisms involved in the association. A more distinct analysis of the hypertensive conditions might help to understand the biological factors involved in this association.
Footnotes
Authors’ Note
Stefanie Böhm designed the study, performed the statistical analysis, and drafted the initial manuscript. Eileen A. Curran supervised the statistical analysis, interpreted the results, and reviewed and revised the manuscript. Louise C. Kenny conceptualized the study, interpreted the results, and reviewed and revised the manuscript. Gerard W. O’Keeffe conceptualized the study, interpreted the results, and reviewed and revised the manuscript. Deirdre Murray interpreted the results and reviewed and revised the manuscript. Ali S. Khashan conceptualized and designed the study (with Stefanie Böhm), supervised the statistical analysis, interpreted the results, and reviewed and revised the manuscript. All authors approved the final version to be submitted and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. This study was con-ducted by S.B. as part of her student research placement at the Irish Centre for Fetal and Neonatal Translational Research (INFANT), University College Cork, Ireland.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was part funded by the Irish Centre for Fetal and Neonatal Translational Research (INFANT; Science Foundation Ireland funded centre, Grant 12\RC\2272).