
Abstract
For children living in the United States, ADHD is among the most pressing mental health concerns (Merikangas et al., 2010) and a primary cause for referral to psychological services (Nock, Kazdin, Hiripi, & Kessler, 2006), with a prevalence in the United States of 11% across the life span (Centers for Disease Control and Prevention [CDC], 2011). Classified as primarily Inattentive, Hyperactive, or Combined types, ADHD is characterized by persistent deficits in attention (e.g., inability to attend to a particular task for a sustained period of time, poor ability to ignore distractions), hyperactivity (i.e., fidgeting, frequent motion), and impulsivity (e.g., interrupting during conversation, blurting out answers at school). Children with ADHD show marked difficulty adhering to developmentally appropriate behavior patterns across multiple major settings (i.e., at school, at home, or with peers). These symptoms, in turn, correlate highly with impaired functioning in academic (DuPaul, McGoey, Eckert, & VanBrakle, 2001) and social (Nijmeijer et al., 2008) settings, and increased risk for negative life trajectories, characterized by high school dropout and loss of employment (Barkley, Fischer, Smallish, & Fletcher, 2006). The high prevalence rate, combined with severe consequences that manifest across the life span, make identification and delivery of effective treatments for ADHD an urgent national priority.
Evidence-Based Treatments for ADHD
Recommendations for evidence-based treatment historically have been driven by national task forces (e.g., American Psychological Association [APA] Division 12 Task Force on Evidence-Based Treatments; Chambless et al., 1998) and rely on criteria that require, for instance, a particular number of randomized controlled trials (RCTs), implemented by multiple research teams, with additional requirements regarding rigor and quality of design and execution. For ADHD, two broad categories of treatment options have been identified, according to these criteria, as evidence based: pharmacologic treatment, most commonly with some form of stimulant medication, and nonpharmacologic, or psychosocial, interventions.
Medication
Stimulant medication is currently the most common treatment in the United States, with an estimated one out of every 25 children in the United States (roughly 4.4%) receiving some form of stimulant medication for ADHD (Castle, Aubert, Verbrugge, Khalid, & Epstein, 2007). Stimulant medication provides strong and often rapid reduction of both inattentive and hyperactive core symptoms of ADHD, and the current evidence base shows medication to be strongly supported for reduction of those symptoms (Attention-Deficit, S. O., 2011). However, while stimulant medications achieve strong short-term efficacy with regard to symptom reduction, symptoms typically reappear when medication ends, and few studies show medication to yield improvements in functional outcomes (e.g., academic performance; Pelham & Fabiano, 2008). In addition, stimulant medications carry risk of unwanted side effects, particularly diminished growth (Swanson et al., 2007) as well as slight risks for increases in blood pressure, heart rate, and sleep disturbances (Cortese et al., 2013). Taking medication is often met with resistance from children, particularly adolescents (Sibley, Kuriyan, Evans, Waxmonsky, & Smith, 2014), and some families are reluctant to rely on medications for their children (Johnston, Hommersen, & Seipp, 2008).
Psychosocial
While many evidence-based treatments for ADHD exist, according to recent reviews (Pelham & Fabiano, 2008) most include a behavioral reinforcement component, either delivered directly to the child by a mental health professional, or delivered via parent management training (Pelham & Fabiano, 2008). An update to that review (Evans et al. 2014) found the same to hold true (with five studies suggesting neurofeedback and organizational skill training warranting further study; Evans et al., 2014). Psychosocial treatments may offer similar symptom reduction benefits to medication without the risk of side effects (Fabiano et al., 2009), and may offer a longer lasting intervention effect after completing treatment, while medication often must be taken continuously to remain effective (Pelham & Fabiano, 2008). However, while many studies demonstrate strong efficacy in terms of symptom reduction, these treatments too are accompanied by important limitations: they require a trained professional (and training can be lengthy and expensive for community mental health agencies), typically a master’s- or doctoral-level clinician, to deliver the intervention; they require significantly more time with a provider relative to a medication consult; and insurance coverage for psychosocial treatment, despite recent advances, remains limited relative to coverage for medication (Peele, Lave, & Kelleher, 2002). In addition, some reviews have found the evidence base to be weaker versus medication treatment or have not found behavioral treatment to be effective in reducing symptoms (Sonuga-Barke et al., 2013).
Despite efforts to draw consensus around best practice for ADHD treatment, several issues drive persistent controversy over the evidence. First, there is common public perception that ADHD is overdiagnosed in the general population, which persists despite evidence suggesting otherwise (Sciutto & Eisenberg, 2007). This fear, combined with concerns over side effects (Swanson et al., 2007) and potential abuse of stimulant medications (Babcock & Byrne, 2000), influence concern regarding the sharp increase in stimulant prescription witnessed over the last 25 years (Zuvekas & Vitiello, 2008). Conversely, the psychosocial treatment literature reveals equivocal findings, both when tested independently and when combined with medication. The Multimodal Treatment of ADHD (MTA) study, to date the largest RCT of ADHD treatments, produced mixed results across different outcome categories: some showed a benefit to combined treatment while others showed no incremental gain over medication alone (The MTA Cooperative Group, 1999). Recent systematic reviews and meta-analyses, which should offer greater clarity by synthesizing the full body of literature, similarly reveal conflicting findings on the relative strength and utility of nonpharmacologic treatment for ADHD (Fabiano et al., 2009; Pelham & Fabiano, 2008; Sonuga-Barke et al., 2013; Van der Oord, Prins, Oosterlaan, & Emmelkamp, 2008). This variability may reflect differences in inclusion criteria, as suggested by the findings of a recent systematic review of 12 meta-analyses for psychosocial treatments for ADHD (Fabiano, Schatz, Aloe, Chacko, & Chronis-Tuscano, 2015). Specifically, Fabiano and colleagues found that overlap in studies meeting criteria for the meta-analyses ran as low as 2% and no higher than 46%; in fact, the meta-analyses were considered so heterogeneous (despite examining the same basic question) that the authors were unable to combine them into a single meta-analysis and concluded that further effort to define best practice is warranted.
Childhood Poverty and ADHD
Moderator analyses often are employed to disentangle discrepant findings across studies and to help explain for whom a particular treatment works, and under what conditions (Paul, 1967). Multiple factors, including baseline severity of symptoms, parental psychopathology, child gender, age, and parental education, among others, have been hypothesized to moderate treatment efficacy for ADHD. To our knowledge, the current review is the first to systematically examine the potential influence of family income and socioeconomic status (SES) on ADHD treatment outcome.
Childhood poverty represents a significant risk factor for ADHD. Children living in poverty are at higher risk for ADHD compared with higher income peers (CDC, 2005), with some studies showing prevalence twice as high in low-income populations (Burns et al., 1995). Despite increased need, low-income children with ADHD are less likely to receive services (Froehlich et al., 2007; Kataoka, Zhang, & Wells, 2002). Low-income families that do seek treatment often are responding to pressure from their child’s school or else following contact with child welfare, foster care, or juvenile justice (Chow, Jaffee, & Snowden, 2003). Furthermore, psychosocial treatment studies for other externalizing disorders (including behavior problems, Oppositional Defiant Disorder, and Conduct Disorder) also show low SES families to make fewer or slower treatment gains (Lundahl, Risser, & Lovejoy, 2006; Reyno & McGrath, 2006).
We propose that living in poverty as a child may influence the efficacy of psychosocial treatments for ADHD through multiple direct and indirect pathways, as highlighted by the following examples. First, families in poverty experience concrete barriers to engaging in treatment (e.g., reliable access to transportation to a clinic, competing priorities during time when clinics are open, difficulty scheduling an appointment at community clinics reflecting few providers and long waitlists; Gopalan et al., 2010; Harrison, McKay, & Bannon, 2004). These types of challenges may reduce dosage—They make it difficult for a family to receive all of the recommended sessions or treatment components within the recommended time frame, even when motivation is high. Second, poverty (as well as ADHD itself) increases the risk of health, learning, and developmental risks and comorbid disorders (Brooks-Gunn & Duncan, 1997), which in turn may lead to difficulties in cognitive processing that may interfere with children’s acquisition of social skills, often taught in psychosocial treatment programs. Third, perceived barriers to treatment (e.g., lack of relevance or perceived efficacy of treatment, fear of being reported to social services for being unfit parents, poor alliance with the provider) frequently arise for families in poverty (Anderson et al., 2006; Kazdin, Holland, & Crowley, 1997). These barriers may reduce motivation to seek or complete treatment, which in turn may increase attrition or discourage families from enrolling in services. Cumulatively, these risk factors may reduce psychosocial treatment efficacy for children living in poverty.
Current Study
This review was designed to examine the relative efficacy of psychosocial treatments for children with ADHD living in low-income households relative to children from middle- and high-income families. A systematic literature search utilizing multiple electronic databases and previously existing reviews was conducted to identify studies that examined income or income proxies (e.g., SES) as potential moderators of treatment outcome for children with ADHD. We hypothesized that children from low-income families would show slower or smaller improvements relative to children from middle- and high-income families.
Method
Inclusion Criteria
Study design
Only RCTs of psychosocial treatments for ADHD, using a between-groups comparison of treatment conditions, were eligible for inclusion. Studies that used both between and within-group comparisons were included, but crossover designs without a between-group comparison were not. While Pelham and Fabiano (2008) present compelling evidence to suggest the utility of these designs, the “gold standard” for testing efficacy of psychological treatment remains the RCT (Silverman & Hinshaw, 2008). Any study with at least one group receiving psychosocial treatment only (i.e., not receiving both psychosocial and medication treatment, and that children in this condition were not currently medicated) was included. Control groups could include active treatment, community or treatment as usual, wait list control, no treatment, or medication; studies that recruited a “typically developing” sample as control group were excluded.
Sample
Inclusion required that study samples met the following criteria: (a) All participants were age 18 or younger at the time of study, (b) all participants met criteria for ADHD at intake, and (c) family income was reported. Other indicators of SES were noted when present (e.g., measures of parental education, type of parental employment, single-parent status) but were not considered sufficient replacements for income data for the purpose of this review, as these indicators (the most common of which is the Hollingshead four-factor index) do not directly measure family income and are not necessarily accurate indicators of low-income status (see Duncan & Magnuson, 2003, for further discussion). However, nonincome indicators of low-income status that could be converted to an indicator of family income (such as federal free or reduced lunch status of student participants) were permitted for inclusion, as they are based directly on family income levels.
Treatment conditions
Any treatment that demonstrated efficacy for reducing ADHD symptoms through a research trial was eligible for inclusion, assuming other inclusion criteria were met. This included treatments that utilized individual or group format and treatments delivered directly to children (e.g., social skills training) or their parents (e.g., behavioral parent training). There were no exclusions related to particular program or curriculum, provider experience or credentials (e.g., licensed mental health professional or paraprofessional), setting of service delivery (e.g., home, school, clinic), or theoretical orientation (e.g., cognitive, behavioral).
Outcome measures
Eligible studies measured reduction of ADHD symptoms. We adhered to criteria put forth in the Diagnostic and Statistical Manual of Mental Health Disorders (DSM) most current to the year of study publication (i.e., older studies were held to the diagnostic standard of the DSM in use at the time the study was conducted). Studies that analyzed both functional outcomes (e.g., school performance, social skills) and symptom reduction were retained, but only outcomes related to reduction of Inattentive, Hyperactive, or Combined type symptoms (or some combination thereof) were included. Symptom reduction must have been demonstrated quantitatively, as with a rating scale, child self-report, or coded behavioral observation, but no restriction was made to specific tools, measures, or diagnostic instruments.
Publication type
To insure the inclusion of intervention studies that have been validated with regard to rigor of design and execution, only peer-reviewed publications were included for final review.
Search Strategy
Electronic search
Database searches were performed in PsycINFO, Pubmed, Embase, and ERIC, from 1976 (or the earliest available dates in a particular database, whichever is later) until April 19, 2015. Searches utilized database-specific subject headings assigned by the database for ADHD, a free text search for income or related terms (e.g., income, SES, poverty), and a search for terms in the abstract that would imply a treatment outcome study or RCT, though these terms were deliberately kept broad to maximize reach (e.g., treatment, randomized, intervention, psychosocial, RCT), as well as search terms for common treatment approaches for ADHD (e.g., “parent training,” behavioral). “OR” strings for each grouping (RCT-related terms, SES-related terms, and ADHD-related terms) were grouped with parentheses and then connected with “AND” operators, allowing for all possible permutations of terms across groupings. The first author reviewed the titles and abstracts from each search result and selected all relevant results (erring on the side of inclusion) for a second, full read, and eligibility screening. No language restriction was applied to the database, but only articles that offered, at minimum, an English translation of the abstract were reviewed. All studies selected for full second review were downloaded into Refworks.
Additional search strategies
Two additional methods of study identification were utilized. First, the Substance Abuse and Mental Health Services Administration’s National Registry of Evidence Based Programs and Practices (NREPP) database was searched to identify all interventions listed as targeting children and adolescents with ADHD. The NREPP database is a hand-reviewed, routinely updated database of evidence-based treatments for mental health and substance use disorders, designed for frontline providers and researchers and maintained by the Department of Health & Human Services. All interventions identified were compared with results of the electronic search to ensure that all NREPP-identified interventions for ADHD were represented in the current review. Second, the authors used three recent systematic reviews of evidence-based treatments for ADHD (Pelham & Fabiano, 2008; Sonuga-Barke et al., 2013; Van der Oord, Prins, Oosterlaan, & Emmelkamp, 2008) to identify and include all studies that utilized a between-group or RCT design.
The first author then conducted a second, full review of eligible articles, assessing and recording each one’s design features in reference to inclusion criteria using a Google Docs form. All studies that met the inclusion criteria listed above were included in data abstraction.
Data Abstraction
Two independent reviewers completed abstraction electronically, recording descriptive data (author, year of publication, study type), demographic information (sample size, income data), treatment information (treatment target, outcome measures used, mean and standard deviations for Inattentive and Hyperactive subscales, and effect size estimates), moderators examined (variables related either to income or to SES, for example, income, parental education, Hollingshead scores), and results of moderator analyses (whether moderator analyses were performed by the author and, if so, what the outcome of the analysis was) on a customized Google Docs form. As noted above, although income variables or indicators convertible to an income level were required to meet inclusion criteria, moderator analyses using other indicators of SES were noted with the hope of being able to discuss the difference between the results when both were available.
Quality Analysis
The Effective Public Health Practice Project Quality Assessment Tool for Quantitative Studies was used to assess quality of studies included for data abstraction. This tool, developed specifically to aid in classification of studies for systematic reviews and meta-analyses, can be downloaded and viewed at http://www.ephpp.ca/PDF/Quality%20Assessment%20Tool_2010_2.pdf. All studies included in the final sample received a Strong or Moderate rating.
Data Analysis
Findings were summarized in tables illustrating number of studies reporting moderation, direction and strength of moderating effects, and relevant differences in effect sizes, in addition to demographic and study design variables discussed above. Missing data were recorded as missing.
Results
Search Results
Initial electronic search across PyscINFO, Pubmed, Embase, and ERIC revealed 1,172 studies for initial review (Preferred Reporting Items for Systematic Reviews and Meta-Analyses [PRISMA] flow diagram in Figure 1). A close read of titles and abstracts of those 1,172 studies by the first author revealed 44 studies that met criteria for second review (i.e., abstract did not provide sufficient detail regarding sample, inclusion/exclusion criteria, or research design to determine eligibility for the present review). Additional search strategies (i.e., reviewing reference lists for recent meta-analyses as described above) added 35 studies for second review. Cross-checking via the NREPP database identified four treatments considered to be evidence based; the relevant articles cited in the NREPP’s review of evidence already had been identified through the other search methods. After removing duplicates from the combined list, a total of 59 studies were identified for second review. Four of these were not accessible electronically, and requests to primary authors for the articles were unsuccessful, leaving a final sample of 55 studies for second review.
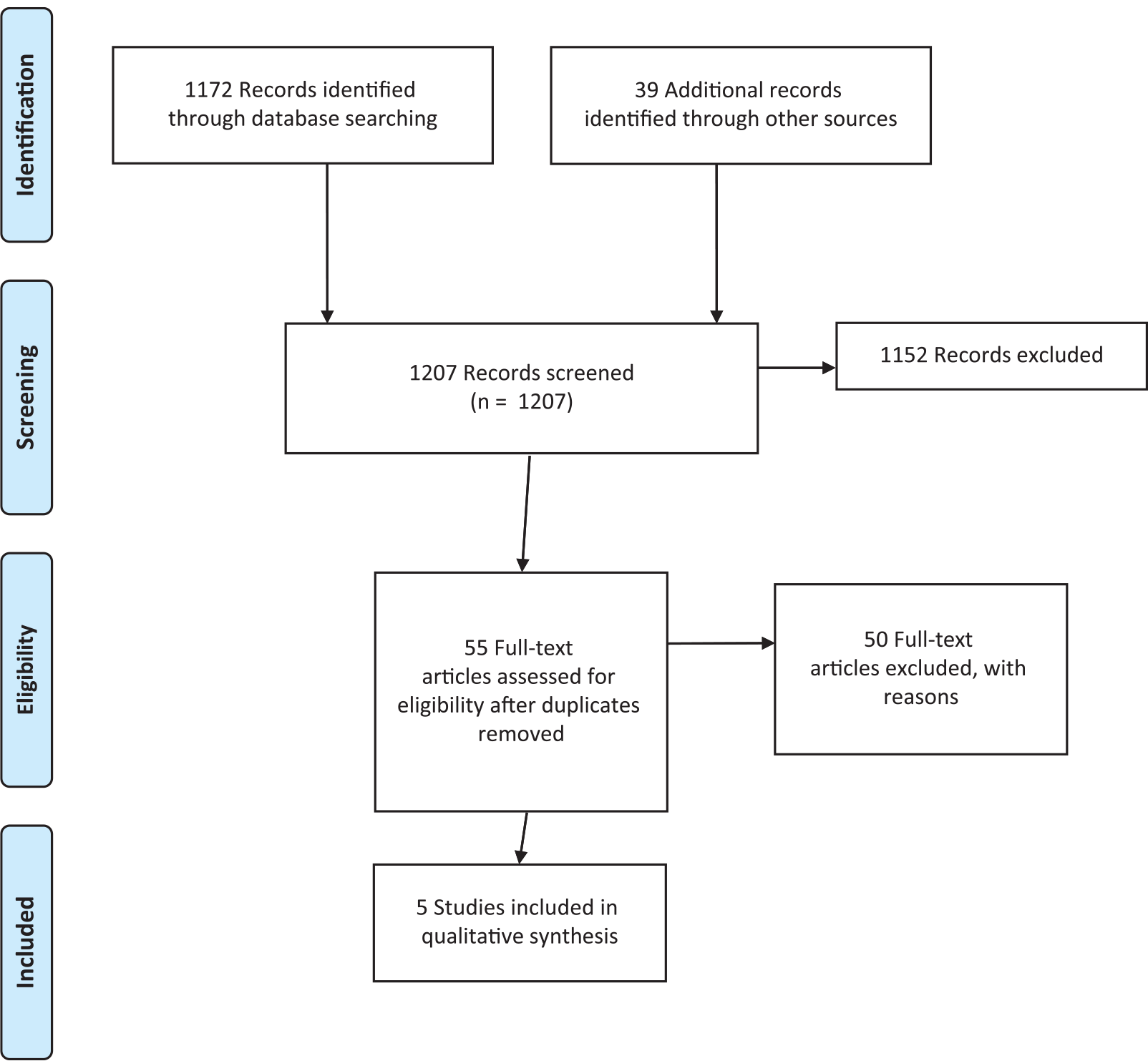
PRISMA flow diagram.
Second Review and Final Sample
Table 1 summarizes all studies included in the second review. All studies met criteria for age of sample (18 years or younger at baseline). Of the 55 studies in the second review, 23 (41.8%) failed to meet criteria for RCT, and thus were excluded leaving 33 eligible studies. Of these 33, six (10.9% of second review sample) failed to meet criteria for a psychosocial-only treatment condition, and thus were excluded, leaving 27 eligible studies. Of these 27, four failed to meet criteria for all participants holding an ADHD diagnosis at baseline. Five (9% of second review sample) failed to meet criteria for outcome measures that directly examined ADHD symptom outcomes, leaving a final sample of RCTs examining the effect of psychosocial treatment on ADHD symptom reduction in children at 17, or 30.9% of the original total for second review, and 53.1% of the identified RCTs.
Second Review Studies Excluded From Data Abstraction and Reasons for Exclusion.
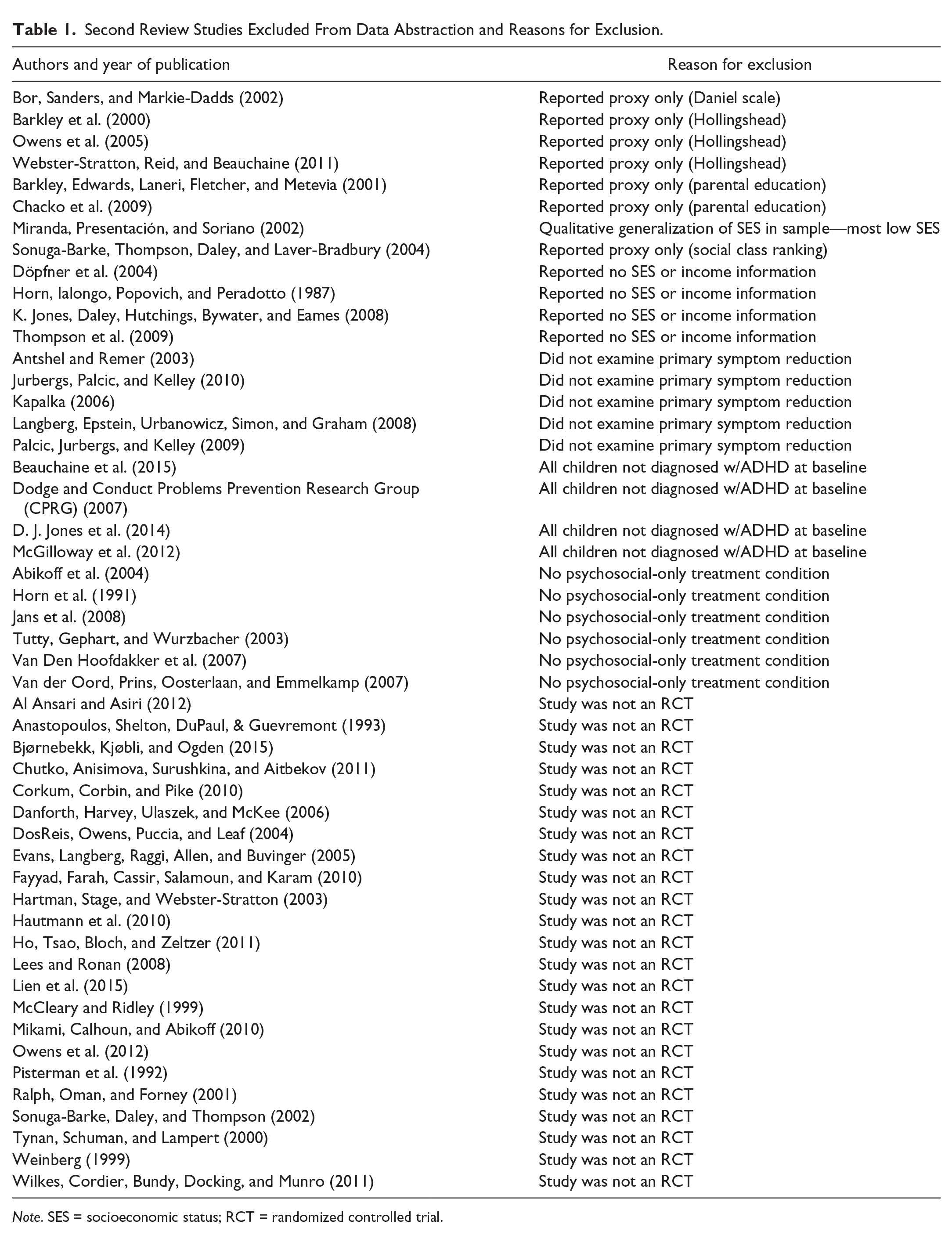
Note. SES = socioeconomic status; RCT = randomized controlled trial.
Reporting of Income and Indices for SES
Of the 17 RCTs, four were excluded for not reporting any income or SES data whatsoever. Of the 13 remaining, five (9%) reported income numbers directly and eight (14.5%) reported some form of proxy measure: three used the Hollingshead social class index, one the Daniel scale (an Australian measure similar to the Hollingshead), one qualitatively described the sample as having a majority of low-income participants, and one provided a social class ranking that resembled the Hollingshead but did not report a citation or describe the numbers within the text. Encouragingly, these numbers are significantly higher than those reported in an often cited 2005 review of youth psychotherapy research, which reported that only 22.5% of studies examining ADHD treatments reported any information on SES or income (Weisz, Doss, & Hawley, 2005).
Third Review
Given the limited number of studies remaining under the original search criteria, we employed an expanded supplemental literature search and review to determine if our inclusion criteria were too narrow or too stringent, despite our original effort to balance rigor and inclusion. Toward this end, we conducted two additional searches. First, we returned to Fabiano’s review of recent meta-analyses (Fabiano et al., 2015) and read each of the meta-analyses from that article (n = 7) not included in our original abstraction. From these, the first author then reviewed all of the articles (total n = 43) included in each of those seven reviews to identify additional studies that met our second review criteria and were assigned to two independent reviewers for abstraction as per our second review procedure. Second, we modified eligibility criteria to allow studies that employed a non-RCT. Keeping all other criteria the same, we then reviewed the studies excluded in the second review once more. Of those, 22 had been excluded due to not being randomized, and the first author hand-reviewed these 22 to determine if they met the rest of the inclusion criteria and we reviewed again studies that were excluded from our original review during the second read (n = 22) that had been excluded previously for failure to meet the RCT inclusion criteria. These combined strategies revealed only one additional article that met all criteria, but the income data in that article remained insufficient to abstract.
Does Income Influence Treatment Response for ADHD?
Five studies met criteria for final inclusion in the review. Of the five, two studies examined income as a moderator directly, one of which also discussed nonincome socioeconomic variables as a moderator (specifically parent education, occupation, and Hollingshead ratings). The other three studies did not examine the moderating relationship but did report income data (moderator analysis in the article was not part of the inclusion criteria). Only one of the five studies explicitly and entirely recruited a low-income sample. Complete results and characteristics of these studies are reported in Table 2. Given the small number of available studies and the heterogeneity among them, quantifiable estimates of the moderating effect of poverty could not be computed; however, we present the following evidence that closer examination of the potential influence of poverty on treatment response for children with ADHD remains warranted.
Characteristics of Studies Meeting Inclusion Criteria.
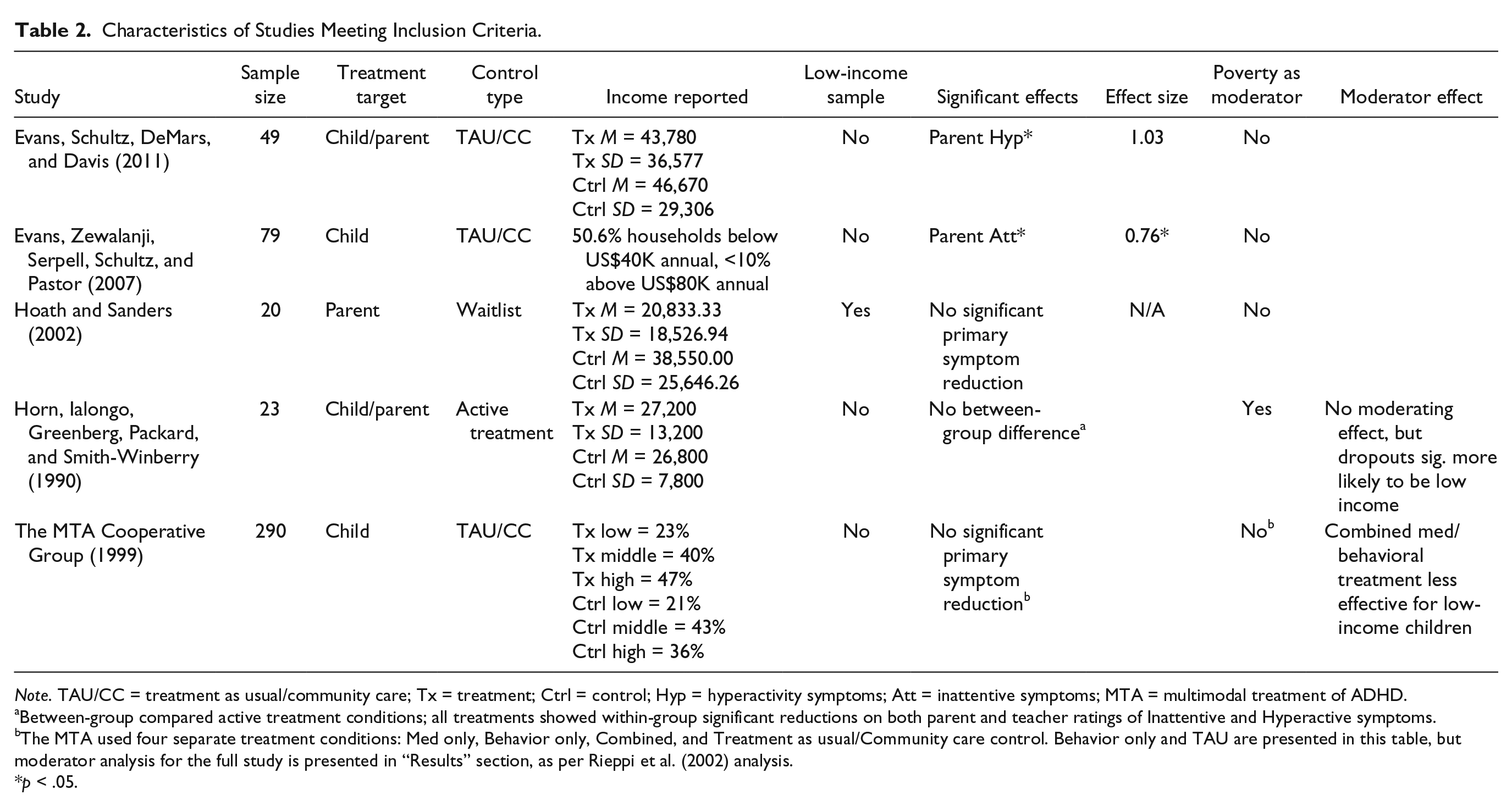
Note. TAU/CC = treatment as usual/community care; Tx = treatment; Ctrl = control; Hyp = hyperactivity symptoms; Att = inattentive symptoms; MTA = multimodal treatment of ADHD.
Between-group compared active treatment conditions; all treatments showed within-group significant reductions on both parent and teacher ratings of Inattentive and Hyperactive symptoms.
The MTA used four separate treatment conditions: Med only, Behavior only, Combined, and Treatment as usual/Community care control. Behavior only and TAU are presented in this table, but moderator analysis for the full study is presented in “Results” section, as per Rieppi et al. (2002) analysis.
p < .05.
Studies examining moderation by income
Two studies (Horn, Ialongo, Greenberg, Packard, & Smith-Winberry, 1990; Rieppi et al., 2002) directly examined income as a moderator of treatment effect. Horn and colleagues did not report a moderating effect of poverty on ADHD symptom outcomes; however, families that dropped out of treatment before completion had a lower mean income than any of the treatment groups as a whole (the authors report the results of the significance test but not the income of the dropouts specifically), and this income difference reached significance compared with the self-control only group (one of two active controls). Rieppi and colleagues did not find a significant difference on household income in the MTA study, but found differences with a proxy for SES (see below).
Studies examining a nonincome SES variable as a moderator
Rieppi and colleagues (2002) reported, in a secondary analysis of the MTA study, a significant effect of parent education on combined medication and psychosocial intervention, such that families reporting higher parental education had children with bigger improvements in functioning at posttest relative to those in lower educated households; other treatment groups did not show these effects, however, nor did other proxies for SES (Hollingshead index, parental occupation).
Studies examining a low-income population
Only one of the five studies (Hoath & Sanders, 2002) explicitly targeted a primarily low-income sample (though low- and low-middle-income families were represented across studies). According to Australian poverty income statistics during the time the study was completed, 50% of the sample was below the poverty line. Hoath and Sanders examined the efficacy of the Triple P Positive Parenting Program with families whose children ranged in age from 5 to 10 and who had been diagnosed by a pediatric or mental health professional with ADHD (diagnosis subsequently confirmed during enrollment using the Health of the National Outcome Scales for Children and Adolescents). Findings revealed no significant effects on any of the four ratings of ADHD symptomatology, from teachers or parents. We interpret this finding with some caution because the original intervention was not developed specifically for ADHD, but rather for children exhibiting a broader range of externalizing behaviors and disorders, and other studies by the authors have found some evidence of effect on ADHD.
Discussion
The current review was designed to examine the influence of poverty on psychosocial treatment outcome for children with ADHD. Unfortunately, our review offered limited ability to draw meaningful conclusions about income as a potential moderator of treatment efficacy. Despite broad review criteria and a comprehensive literature search, only five studies emerged with sufficient income data to meet inclusion criteria. Of those, two studies showed some indication of a negative effect of low SES on treatment response and attrition, and one study conducted with a primarily low-income population showed no significant treatment effect on core ADHD symptoms.
The limited evidence presented here, while too sparse to draw conclusions, does offer a compelling reason to more systematically assess the extent to which living in poverty may disrupt treatment progress and interfere with documented benefits of psychosocial treatment for families of children with ADHD. Rieppi and colleagues’ data revealed that lower educated families exhibited less symptom improvement relative to higher educated families. Horn and colleagues (1990) reported that income did not significantly affect treatment outcome but may have influenced attrition. Perhaps Hoath and Sanders (2002) data are of greatest concern; their entire sample was comprised of low-income families whose children showed no decrease in ADHD symptoms (but improvements in other domains) following behavioral parent training (specifically the Triple P Positive Parenting Program). These data lie in contrast, though, to the other studies and MTA moderator analysis, all of which have revealed reductions in core symptoms for low-income families—but while those low-income youth did show symptom reduction, in some areas, those reductions were slower and smaller compared with their higher income counterparts in the same study (Rieppi et al., 2002). Thus, while the rich body of efficacy literature (Pelham & Fabiano, 2008) suggests psychosocial treatment for ADHD may still be warranted for low-income families, the stress and correlates associated with being financially underresourced may interfere with treatment completion or outcome. Although data presented here are not sufficient to draw definitive conclusions, we believe the evidence does suggest the question merits closer study. A review of feasibility studies with less restrictive criteria might help to further illuminate these relationships.
The Good News
Encouragingly, the percentage of studies reporting information relating to SES, whether income directly or a proxy, is higher than previous reviews of psychosocial treatment efficacy (Weisz et al., 2005). The current review reported both more studies reporting SES information (13 vs. 2) and better reporting percentages (23.6% nonreporting vs. 77.5% nonreporting). Whether the increase reflects an improvement in editorial guidelines or author practices in child clinical research or a tighter set of inclusion restrictions (though we feel the criteria adopted here were fairly minimal), it is nevertheless encouraging to see that investigators are obtaining SES information, at minimum, in light of disparities related to ADHD diagnosis and service use.
The Not-So-Good News
Despite this modest improvement, however, the reporting of indicators of poverty remains insufficient to draw meaningful conclusions from the data as a whole. The results of the current review suggest three main challenges. First, studies are not consistently reporting information on poverty: Many studies report no information on income or SES, while others mention it qualitatively but do not provide actual data. Some investigators control for SES differences across treatment groups, but provide limited information about their analytic method, though increasing levels of detail appear in more recent work. Among the studies that do report information, that reporting is often inconsistent. Some studies report values as means and standard deviations, others separate into categories (e.g., between US$10,000 and US$20,000, US$20,000 and US$30,000); some report separate statistics by treatment group, while others report only on the sample as a whole. Expanding our sample to include non-RCT between-group studies did not yield any additional results, suggesting that the low number of adequate studies accurately reflects the overall state of the literature.
The limited available data may also result, in part, from the nature of efficacy trials themselves, which exclude by design participants with comorbid disorders or complex life circumstances to maximize internal validity. Given the disproportionate rates both of ADHD and comorbidities in low-income populations, this may mean that families in poverty are unlikely to make it into efficacy trials. As a result, our evidence-based treatments may systematically lack evidence with the population that needs them the most (Weisz et al., 2005). As a field, clinical psychology has improved with regard to recruiting diverse samples and reporting race and ethnicity, as evidenced by National Institute of Mental Health (NIMH) requirements for targeted enrollment and monitoring of minority recruitment; we propose the time has come for the same rigor and representativeness in sampling to be applied to indicators of income.
Third, when information is provided on indicators of poverty, it is typically limited in utility. Only a handful of studies offer clear information on the income level and distribution of their sample. Many studies use a single indicator or proxy (e.g., parental income, single-parent status, Hollingshead ratings) of SES, even though this approach holds limited potential for identifying families living in poverty (Braveman et al., 2005; Duncan & Magnuson, 2003). The most popular measure of SES, the Hollingshead index, is now more than 40 years old, and its rankings of occupational prestige suffer from significant limitations (Hauser & Warren, 1997), that are rarely reported in the authors’ discussion or interpretation of findings. The risk inherent to this type of reporting is twofold: First, the information required to draw meaningful conclusions is missing and, second, by presenting incomplete information as sufficient, without discussing limitations, the field implies these indicators are enough to demonstrate efficacy with a low-income population. The biggest conclusion to be drawn from the results of the current review is that there is a need for more consistent and higher quality reporting of income information.
Opportunities for Sampling, Measuring, and Reporting Income
We have an opportunity to invoke advances in other disciplines related to measuring and understanding poverty. To begin with, developing precise definitions of SES and poverty, and understanding differences between different types of poverty, is critical to better understanding its relationship to treatment outcomes. There are several lenses through which to understand the resources-to-need gap that characterizes poverty as a construct (e.g., absolute, relative, and subjective poverty; Yoshikawa, Aber, & Beardslee, 2012). We selected income for the current study because it is used to calculate official poverty statistics in the United States (Fox, Garfinkel, Kaushal, Waldfogel, & Wimer, 2014); however, income does not capture subjective or relative poverty, which may have just as large, if not larger, of an effect as absolute poverty on treatment. Yoshikawa and colleagues (2012) argue, for example, that absolute poverty may be better suited to examine lack of material needs and subsequent risk, while relative poverty may better differentiate families within a low-income sample, and absolute and relative poverty may differentially influence risk profiles and mental health outcomes.
We may also borrow from other disciplines to improve the tools we use to measure poverty in all of its forms. Braveman and colleagues (2005) offer several recommendations for improving how we measure correlates of poverty to make better inferences about poverty and its consequences. By example, they compared several nationally representative data sets using multiple indicators of income and SES on a variety of health outcomes, including overall health status, mortality, high risk and violent behavior, sexual risk-taking, and substance use. In comparing several variables related to SES (e.g., income level, educational attainment, poverty level, income/needs ratios), their analyses revealed a consistent pattern of correlations insufficient to suggest that these factors are interchangeable or useful proxies for each other. Furthermore, the predictive power of a model increased as more variables were included simultaneously, suggesting each contributes to a better understanding of risk when used in conjunction with another. Including more than a single indicator of SES will move us toward a more accurate picture of which facets of poverty most affect treatment outcomes.
Finally, as our ability to measure poverty and its effects improves, we will become better equipped to systematically recruit more economically diverse and vulnerable samples into psychosocial treatment studies. Until now, investigators seeking to protect the internal validity of their studies may have hesitated to recruit families in poverty because of the potential confounds introduced by their complex life circumstances. Precise measurement, though, would enable us to embrace and examine (rather than control) these factors that in turn may become critical data by which to modify and improve our treatment modalities.
Limitations and Future Directions
We employed a stringent set of inclusion criteria that yielded a small sample of five studies for close consideration. First, we initially restricted our sample to studies that employed RCT designs and examined symptom reduction as a primary outcome. Although these criteria resulted in a small number of eligible studies, they reflect recommendations for best practice in methods for validating evidence-based psychological treatments (Chambless et al., 1998) and examining impact (Pelham & Fabiano, 2008). Second, we required income reporting, as opposed to other proxies of SES, both to maximize comparability across studies (as it is difficult to establish equivalency of income against social class in terms of relative risk and implications with regard to other risk factors) and because income, in addition to suggesting the presence of other risk factors, has been shown to have a direct impact on mental health functioning and difficulties associated with living in poverty (Noble et al., 2015; Yoshikawa et al., 2012). Finally, we included only peer-reviewed publications to ensure rigor in research design, given controversy over whether to include treatment studies with nonsignificant results in reviews (Pelham & Fabiano, 2008). The Hoath and Sanders (2002) study, however, hints at the drawback of this approach. If treatments for low-income families tend to yield a higher frequency of nonsignificant results, then the publication bias toward significant results may prevent publication of these efficacy trials. This may mean that the findings that best address our question may not be finding a home in the literature.
Given the limitations of the current data set and the infrequent examination of the moderating effect of poverty, a possible next step could be to relax the inclusion criteria further to increase the number of available studies and, if possible, to use metaregression techniques to pool the effects of multiple studies and examine the effect of poverty on outcome. The studies included in this review did not meet the requirements for metaregression, primarily due to heterogeneity, but a different set of inclusion criteria might yield a more homogeneous or sufficiently large sample to analyze in this way (though we suspect the overall level of methodological rigor of included studies might decrease). Furthermore, because working with low-income populations runs a high risk for comorbid disorders, it may be that much of the work being done with this population tends to forego using more rigorous, efficacy-focused designs in favor of examinations of effectiveness from the outset. A review that relaxes criteria and includes feasibility studies examining these questions may help to further illuminate work being done with low-income families that shows potential avenues both for understanding the moderating impact of poverty and identifying methodologies to study in greater detail.
Concluding Remarks
We need look no further than the recent explosion of functional magnetic resonance imaging (fMRI) data to see the value to the field in utilizing more precise measurements. For children living in poverty, the constellation of risk factors that influence mental health is complex and multidimensional. If we seek to promote mental health through psychosocial treatments, then our measurement of factors that may affect treatment progress, completion, and outcomes must be correspondingly complex and multidimensional. It is only with more precise, comprehensive, and nuanced reporting of poverty as a construct that we can begin to truly answer Paul’s (1967) question: Which of these treatments, under what set of circumstances, works for children in poverty?
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.