
Abstract
ADHD is a developmental mental disorder that begins in childhood and approximately half of all patients’ symptoms will persist into adulthood (Lara et al., 2009). Multidimensional impairments including executive function (EF), academic performance, and occupational achievement were found in adults with ADHD (Spencer, Biederman, & Mick, 2007). Cognitive-behavioral therapy (CBT) conducted in group and individually were both validated for adult ADHD (Jensen, Amdisen, Jorgensen, & Arnfred, 2016; Knouse & Safren, 2010), and CBT was often considered as an adjunct treatment to stimulant medications. Review of existing literature shows that CBT has been mostly studied for adult ADHD in Western countries (Bramham et al., 2009; Philipsen et al., 2015; Safren et al., 2005; Safren, Sprich, Mimiaga, et al., 2010; Weiss et al., 2012), thereby casting doubt on the generalizability of the findings to other parts of the world, including China and other Chinese-speaking regions. Since its introduction into China in the early 1990s, CBT has been primarily used for depressive and anxiety disorders (Li & Li, 2009). Attempts to use CBT for patients with ADHD, including in children, are fairly recent in China. Therefore, it is important to investigate the efficacy of CBT on adult ADHD. Moreover, previous trials mostly examined the treatment efficacy based on core ADHD symptoms (Mongia & Hechtman, 2012); the effects on other impairments, such as EF, impulsivity, self-esteem, and life quality, all important aspects of the disorder, were rarely studied.
Although its short-term efficacy is well documented, the evidence of long-term efficacy of CBT is inconsistent (Knouse & Safren, 2010). Booster sessions were first developed in behavior therapy to consolidate the skills learned and cultivate strategies dealing with recurrence or relapse after acute treatment phase, and they showed positive effects on eight different behavior problems (Whisman, 1990). Recently, this psychotherapy model was investigated in a wide range of mental disorders. For recurrent depression, patients who receivedcognitive therapy with a continuation phase had a decreased recurrence rate than those who only received acute phase cognitive therapy. And it was found that the effect of 2 years’ maintenance CBT was similar to that of medication on patients with recurrent depression (Blackburn & Moore, 1997). For children with bipolar disorder, CBT with maintenance sessions showedlong-term efficacy during 3 years’ follow-up (West, Henry, & Pavuluri, 2007). For patients with panic disorder, CBT with maintenance sessions improved their social function and prevented symptoms’ recurrence (White et al., 2013). For females with binge eating disorder, CBT with booster sessions decreased their core symptoms and depressive symptoms and improved life satisfaction at 12-month follow-up (Schlup, Munsch, Meyer, Margraf, & Wilhelm, 2009). Moreover, meta-analysis in children with mood or anxiety disorders found that CBT with booster sessions was more effective and its outcomes were more sustainable (Gearing, Schwalbe, Lee, & Hoagwood, 2013). To date, there were two CBT trials in adult ADHD (Philipsen et al., 2015; Weiss et al., 2012) including booster sessions, and they were all conducted in Western patients and none explored the effects of booster sessions on impairments.
This study aimed to investigate the efficacy of group CBT with and without booster sessions in Chinese adult patients with ADHD. We hypothesized that group CBT would improve ADHD core symptoms and reduce impairments; we also hypothesized that CBT with booster sessions would provide additional benefits to core ADHD symptoms as well as impairments.
Method
Participants
All the methodological details were described in the published trial protocol (Fang, Qiujin, & Yufeng, 2015). This study is registered at http://www.clinicaltrials.gov and the registration identification number is NCT02062411. This study received ethics approval from the Ethics Committee of the Sixth Hospital of Peking University (2013; Ethics review No. 42) and all participants signed the informed consent. The participants were outpatients of the psychiatric clinics at Peking University Sixth Hospital who were willing to receive CBT between September 2013 and February 2015. The diagnoses were based on the criteria of the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994) and diagnoses were made using the Conners Adult ADHD Diagnostic Interview (Epstein & Johnson, 2001; Qian, Li, Wang, & Zhang, 2010). The structured clinical interviews for DSM-IV Axis I (First, Spitzer, & Gibbon, 1998) and Axis II Disorders (First, Gibbon, & Spitzer, 1997) were conducted to identify patients’ comorbidities. For patients who were already on medications for ADHD, they needed to have been stable on medications for at least 2 months (drug dose was adjusted within 10% in past 2 months; Safren, Sprich, Mimiaga, et al., 2010). The exclusion criteria were (a) patients with comorbidities such as severe major depression, clinically significant panic disorder, bipolar disorder, organic mental disorders, psychotic disorders, or pervasive developmental disorders; (b) patients who were at risk for suicide, in unstable physical condition, or had received therapy before; (c) older than 45 years (Schroeder, 2014) or had an intelligence quotient (IQ) of less than 90 that might affect cognitive tests’ results. Totally, 627 people were willing to participate and 129 people, whose residence, schedule, and general psychological state were appropriate, underwent baseline psychological evaluation. Finally, 108 patients who met the inclusion criteria were included and randomized, 43 to CBT only group, 43 to CBT + booster group, and 22 to control group. The patients’ demographic and clinical characteristics are listed in Table 1. There were no statistically significant differences in demographic features or baseline clinical measures among three groups.
Demographic and Clinical Characteristics of the 108 Participants in Different Randomized Groups.
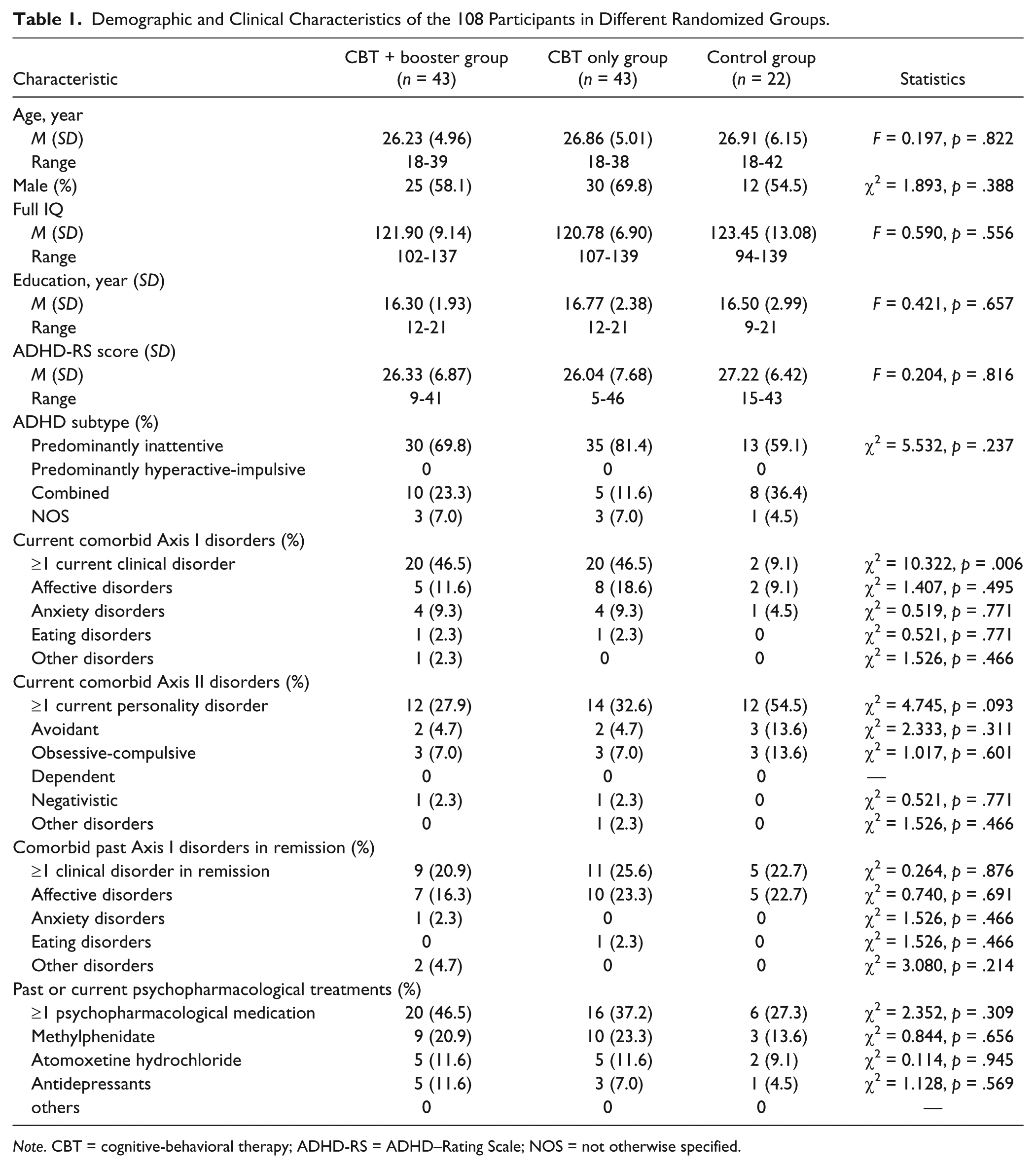
Note. CBT = cognitive-behavioral therapy; ADHD-RS = ADHD–Rating Scale; NOS = not otherwise specified.
Sample Size
The sample size was calculated based on results of our self-controlled experimental study that the score of ADHD-RS was 29.80 ± 7.67 (n = 15) at baseline, 17.22 ± 7.62 (n = 18) after CBT, and 10.56 ± 4.98 (n = 16) after booster sessions. For the comparison between CBT only group and control group at 12th week, to achieve a power of 80% and a two-sided alpha of 5% and we assume the dropout rate is 10%, 15 patients in control group and 15 patients in CBT only group were needed. For the comparison between CBT only group and CBT + booster group at 24th week, 29 in CBT only group and 29 in CBT +booster group were needed. In sum, 73 participants were needed, including 15 patients in control group, 29 in CBT only group and 29 in CBT +booster group.
Procedures
Recruitment and randomization
All referred patients by their treating psychiatrists were contacted by research staff through the telephone. The study description was provided, and initial screening and assessments were conducted over the telephone. A written informed consent was provided by participants at the first face-to-face assessment. The assessments were conducted by trained research staff members (Y.W. and M.P.) as blinded assessors. Participants in CBT only group and CBT + booster group were told about receiving treatment the next week, while those in control group would wait for treatment after 3 months. According to the ethical requirements, patients in control group would receive 12 weeks of CBT after waiting, should they so choose. Participants were enrolled at four different times during 2013 to 2015. At the first three times, participants were randomized into three groups in a 1:1:1 ratio, and at the last time, they was randomized into CBT only group and CBT +booster group in a 1:1 ratio based on the larger sample size for these two groups. The randomization was conducted by an independent statistician using the Statistical Package for the Social Science (SPSS) Version 22 (IBM; Chicago, IL). Figure 1 is the Consolidated Standards of Reporting Trials (CONSORT) flow chart of patients in the trial.
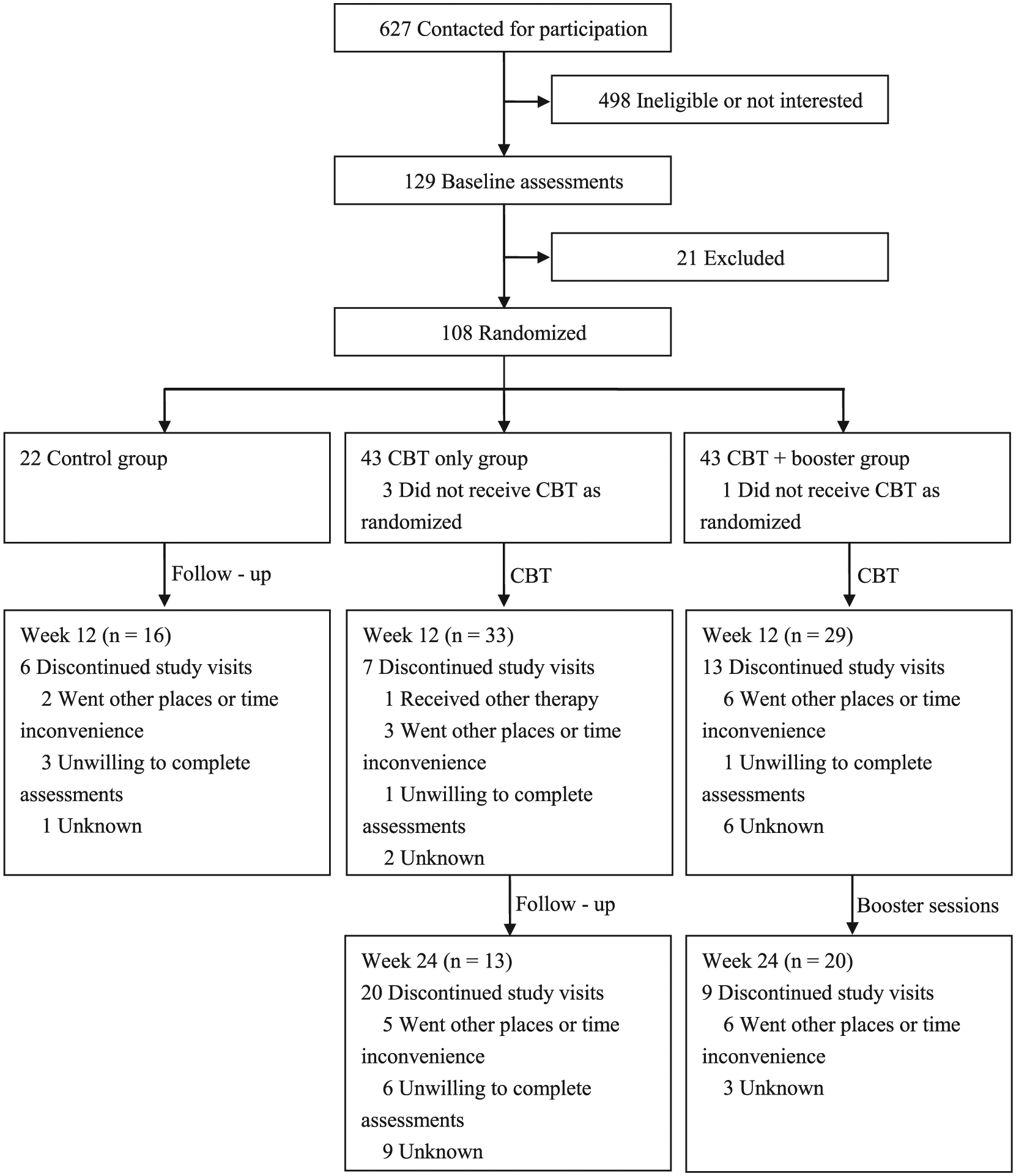
Patient flow.
Therapy
The 12 weeks of group CBT was based on a published and validated manual (Safren et al., 2005; Safren, Sprich, Mimiaga, et al., 2010). This manual was translated into Chinese language and was suitable for Chinese patients (Wang, Shan, Cai, & Wang, 2014). As the manual was conducted individually by previous studies, we added some strategies of group CBT in practice based on a published book (Bieling, Mccabe, & Antony, 2006). Three booster sessions were added to CBT + booster group and they were designed based on previous studies (Philipsen et al., 2015; Weiss et al., 2012; see details in Supplement 1). CBT was conducted weekly from the first to 12th week and booster sessions were conducted monthly from the 13th to 24th week. All sessions were of 120 min duration and they were conducted in groups, with each group having 8 to 12 patients. The weekly CBT sessions had six modules, including organization and planning, reducing distractibility, adaptive thinking, dealing with procrastination, building helpful relationship, and review. The main goal of booster sessions is to consolidate the skills learned and to develop strategies dealing with recurrence or relapse. Thus, the booster sessions contained the induction of the first three modules described above as organization and planning, reducing distractibility and adaptive thinking, and practicing activities based on the patients’ questions in the real world. Some psychological games were also added to improve the acceptability of booster sessions.
Therapists training and treatment adherence/competence
All group CBT sessions were led by two trained psychiatrist-therapists, who had received systematic training of CBT through a 2-year continuous workshop sponsored by the Chinese Psychological Association. There were written and audio records of each therapy session, and the therapists were supervised by a senior psychiatrist and a psychotherapist on weekly basis. Treatment adherence and competence were rated by these two independent supervisors using the Cognitive Therapy Rating Scale (CTRS; Creed, Wolk, Feinberg, Evans, & Beck, 2014; https://www.beckinstitute.org). Ten percent of treatment sessions were randomly selected for rating and psychotherapists were not aware of which sessions would be checked. The average score of 11 general items, ranging from 0 to 6 of CTRS, which was 59.67, represented relatively good quality of treatment.
Measures
ADHD–Rating Scale (ADHD-RS)
It is a self-report 18-item scale corresponding to the DSM-IV symptoms of ADHD (DuPaul, Power, Anastopoulos, & Reid, 1998). Items are rated from 0 to 3 based on symptom frequency. There are two subscales: Inattention subscale and Impulsiveness-Hyperactivity subscale. Higher scores reflect severer symptoms. The primary outcomes were the ADHD-RS score changes from the baseline at 12th and 24th week. The ADHD-RS was also rated by patients weekly, during the 12 weeks of CBT, and monthly, during booster sessions. The internal consistency and construct validity of ADHD-RS have been established (Rösler et al., 2006). Internal consistency reliability of the ADHD-RS in this study is shown in Supplement 2.
Conners Adult ADHD Rating Scale–Self-Report Screening Version (CAARS)
The CAARS has 30 items and is rated by patients based on a 0 to 3 scale according to the frequency of ADHD symptoms (Conners, Erhardt, & Sparrow, 1999; Wu, Sun, Li, & Guo, 2009). Eighteen of the 30 items are the same items on the ADHD-RS and the sum of another 12 items is the so-called “ADHD index.” Higher scores represent severer symptoms. Internal consistency reliability of CAARS is shown in Supplement 2.
Self-Rating Anxiety Scale (SAS) and Self-Rating Depression Scale (SDS)
They are both 20-item self-report scales (Duan & Sheng, 2012; Zung, 1967, 1971). Items are rated on a scale from 1 (not at all) to 4 (most of the time). Higher total scores indicate severer symptoms. Internal consistency reliability of SAS and SDS is shown in Supplement 2.
Barratt Impulsiveness Scale (BIS)
It is a 30-item self-report scale and the most widely used self-report measure of impulsiveness (Luengo, Carrillo-De-La-Pena, & Otero, 1991; Zhou, Xiao, He, Li, & Liu, 2006). The items are rated 1 to 4 based on frequency of impulsive behaviors, and higher scores mean higher impulsivity. Results include three factors: attention, motor, and nonplanning impulsiveness. Internal consistency reliability of BIS is shown in Supplement 2.
Behavior Rating Inventory of Executive Function–Adult Version (BRIEF-A)
It is a 75-item self-report scale that captures views of an adult’s EFs or self-regulation in the patient’s everyday environment (Du, Qian, & Wang, 2010; Roth, Isquith, Gioia, & Widows, 2005). It is rated 1 to 3 based on the frequency of actions. It has nine clinical subscales that measure various aspects of executive functioning and two broader indexes: Behavioral Regulation Index (BRI) and Metacognition Index (MI). Higher scores indicate severer impairment of EF. Internal consistency reliability of BRIEF-A is shown in Supplement 2.
Cambridge Neuropsychological Testing Automated Battery (CANTAB)
It is a computerized test for EF (Robbins, 1994). We chose the Stockings of Cambridge (SOC) and the rapid visual information processing (RVP) of CANTAB to reflect the function of spatial planning and spatial working memory and attention. Results include problem solved in minimum moves (higher result means better ability) and mean subsequent thinking time (higher result means worse ability) of SOC and total misses (higher result means worse ability) and probability (higher result means better ability) of hits of RVP. It was validated to identify the endophenotype of ADHD (Gau & Huang, 2014). CANTAB was conducted to control group at baseline but not at 12th week as we assume their EF would not change without intervention and to avoid practice effect.
Self-Esteem Scale (SES)
It is a 10-item self-report scale (Rosenberg, 1965; Wang, Wang, & Hong, 1999). The total score is calculated from 1 to 4 based on the agreement of self-description. Higher score reflects higher self-esteem. Internal consistency reliability of SES is shown in Supplement 2.
World Health Organization Quality of Life–Brief Version (WHOQOL-BREF)
It is a 26-item self-report scale (Hao & Fanc, 2000; Power et al., 1998). Items are rated from 1 to 5 based on the degree of satisfaction. It produces scores in four domains related to quality of life: physical health, psychological, social relationships, and environment. Higher scores suggest better quality of life. Internal consistency reliability of WHOQOL-BREF is shown in Supplement 2.
Statistical Analysis
The SPSS Version 22 (IBM; Chicago, IL) was used for all analyses. The multiple imputation (imputation for 5 times) was conducted in the original data set to address the missing data for its advantages (Scheffer, 2002). The main analysis was a two-group ANCOVA of scores of ADHD-RS at the 12th week (CBT only group vs. control group) and the 24th week (CBT only group vs. CBT +booster group) with baseline scores as covariates. Secondary outcomes including emotional level, EF, impulsivity, self-esteem, and quality of life were also analyzed using two-group ANCOVA at the 12th week (CBT only group vs. control group) and the 24th week (CBT only group vs. CBT +booster group) with baseline scores as covariates. Because of the lack of the 12th week retest of the CANTAB in control group, the student t test was conducted between the results of CBT only group combined with CBT + booster group at 12th week and the results of control group at baseline. And when the data were not normal distribution, Mann–Whitney U test was used. The between-group differences were calculated with 95% confidence intervals (CIs) and it was statistically significant if p < .05. All the means displayed were the combined estimated marginal means after multiple imputations.
The proportion of treatment responders was the percentage of participants whose score of the ADHD-RS decreased 30% or more from baseline in the original data set, which was mostly used in studies of medication (Steele, Jensen, & Quinn, 2006) and psychotherapy (Safren, Sprich, Mimiaga, et al., 2010) for patients with adult ADHD. The effect sizes were calculated in the full analysis data set after multiple imputations using the variance of mean of ADHD-RS scores between groups divided by its standard deviation.
Results
Study Completion
One hundred four of 108 participants underwent baseline assessments, and the scores of ADHD-RS of the remaining four participants at baseline were replaced by the second week’s scores. Before multiple imputations, the primary outcome data at 12th week were available for 16 of 22 participants (72.73%) in control group, 33 of 43 (76.74%) in CBT only group, and 29 of 43 (67.44%) in CBT +booster group. At the 24th week, that was 13 of 43 (30.23%) in CBT only group, and 20 of 43 (46.51%) in CBT +booster group. The pattern of data missingness was missing completely at random (MCAR) based on the result of Little’s MCAR Test (p = 1.000). The descriptive statistics of original data set is displayed in Supplement 2. All results were normal distribution (all p > .05) through one-sample Kolmogorov–Smirnov test except the results of mean subsequent thinking time (three moves) of CANTAB (p < .001).
Primary Outcomes
At the 12th week, a significant decrease was found in ADHD-RS score comparing CBT only group with control group (Table 2). The treatment response rate was 60.6% (20 out of 33) in CBT only group and 18.8% (three out of 16) in control group (χ2 = 7.58, p = .006).
Results of ADHD-RS, CAARS, SAS, SDS, SES, BIS, and WHOQOL-BREF for Three Groups at 12th Week (T2) and at 24th Week (T3) After Multiple Imputation and Adjusted for Baseline Measurement.
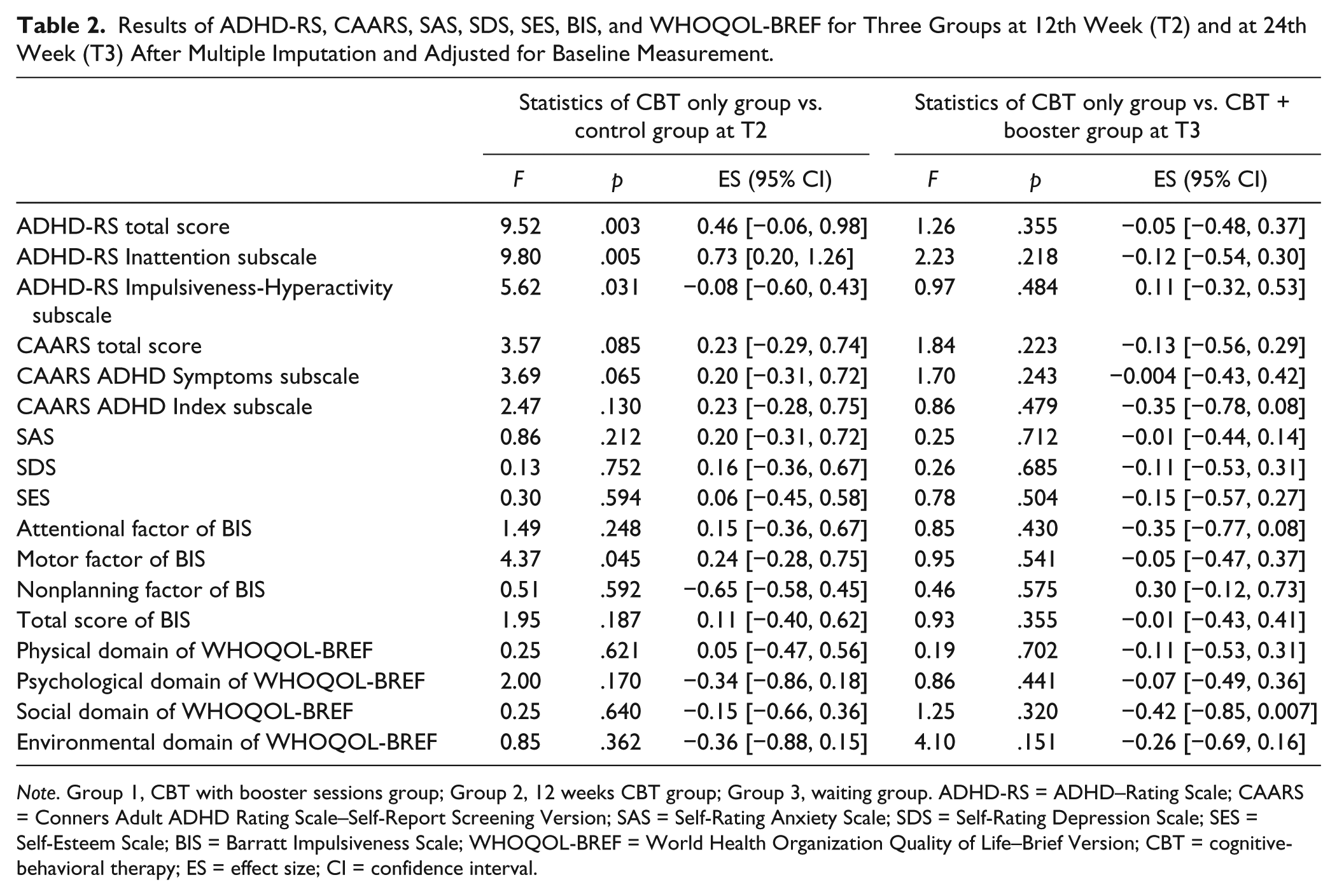
Note. Group 1, CBT with booster sessions group; Group 2, 12 weeks CBT group; Group 3, waiting group. ADHD-RS = ADHD–Rating Scale; CAARS = Conners Adult ADHD Rating Scale–Self-Report Screening Version; SAS = Self-Rating Anxiety Scale; SDS = Self-Rating Depression Scale; SES = Self-Esteem Scale; BIS = Barratt Impulsiveness Scale; WHOQOL-BREF = World Health Organization Quality of Life–Brief Version; CBT = cognitive-behavioral therapy; ES = effect size; CI = confidence interval.
At 12th week, the differences between CBT +booster group and control group were similar to those between CBT only group and control group (total score, 18.80 vs. 23.22, F = 7.52, p = .010; the Inattention subscale, 12.40 vs. 14.83, F = 7.22, p = .011; the Impulsiveness-Hyperactivity subscale, 6.43 vs. 8.67, F = 3.16, p = .093). The differences between CBT only group and CBT +booster group were not significant (total score, 18.80 vs. 18.11, F = 0.19, p = .698; the Inattention subscale, 12.40 vs. 11.67, F = 0.35, p = .634; the Impulsiveness-Hyperactivity subscale, 6.43 vs. 6.49, F = 0.05, p = .882). The treatment response rate was 41.4% (12 of the 29) in CBT +booster group, which was not significantly different from that of CBT only group (χ2 = 2.29, p = .131).
However, at the 24th week, there was no significant difference in ADHD-RS score between CBT only group and CBT +booster group (Table 2). The treatment response rates were 40% (eight of the 20) in CBT only group and 69.2% (nine of the 13) in CBT +booster group, respectively (χ2 = 2.70, p = .101). The weekly or monthly continuous changes of ADHD-RS of CBT only group and CBT +booster group in original data set were also displayed in Figure 2.

The score changes of ADHD-RS during 12 weeks of CBT and booster sessions.
Secondary Outcomes
At 12th week, the score of BRIEF-A MI in CBT only group significantly decreased compared with control group. Other results of BRIEF-A were not significant between groups. Also, no significant differences were found at 24th week between CBT only group and CBT +booster group (Supplement 3).
Comparing with control group, both CBT only group and CBT +booster group performed significantly better in SOC problem solving and SOC thinking time (three moves) at 12th week. No significant difference in RVP was found between groups (Supplement 4).
For BIS, the only significant difference between CBT only group and control group was the motor factor: Patients in CBT only group had significantly less impairment than control group (Table 2).
No significant differences were found between CBT only group and control group in the following measures at 12th week: CAARS, SAS, SDS, SES, and WHOQOL. Similarly, no significant differences were found between CBT only group and CBT +booster group at 24th week (Table 2).
Discussion
Primary Outcomes
Our results on core ADHD symptoms were consistent with previous findings (Safren et al., 2005; Safren, Sprich, Mimiaga, et al., 2010; Weiss et al., 2012). Treatment response rates of previous trials using the same CBT manual and recruiting all medication-treated patients were 56% (Safren et al., 2005) and 67% (Safren, Sprich, Mimiaga, et al., 2010), which are similar to ours (60.61% in CBT only group at 12th week). The effect size of ADHD-RS total score of previous studies (Safren et al., 2005; Safren, Sprich, Mimiaga, et al., 2010) was a little bit larger than that of this study (1.2 vs. 0.46; 0.60 vs. 0.46), which might be related to different percentage of participants on medications (100% vs. 38.89%) and different CBT format (individual vs. group). We found the response rate for patients who were currently on or had received medication treatment before at 12th week in CBT only group combined with CBT + booster group was 36.00%, suggesting CBT can still have additional benefits in these patients. This rate is lower than that of medication-naive patients (62.16%) in this study, partly because seeking for psychopharmacological treatments might be associated with severer functional impairments. Although previous study found that the use of medication + CBT did not significantly improve outcome over and above use of placebo + CBT (Weiss et al., 2012), the complex interaction between CBT and medications remains to be explored.
Secondary Outcomes
Systematic review showed that CBT is more effective for anxiety and depression symptoms of adult ADHD than other psychotherapy approaches (Vidal-Estrada, Bosch-Munso, Nogueira-Morais, Casas-Brugue, & Ramos-Quiroga, 2012) and previous studies showed significantly decreased symptoms of anxiety and depression (Safren et al., 2005; Safren, Sprich, Mimiaga, et al., 2010). However, our study failed to show the efficacy on anxiety and depressive symptoms. Similarly, recent randomized controlled trials (RCTs) with relatively large samples (n = 433 and 95, respectively) also failed to show the efficacy on depression or anxiety (Philipsen et al., 2015; S. Young et al., 2015). There are several possible explanations for the different findings, including different patient samples and baseline clinical features. For example, the percentage of patients on medications in Safren et al. (2005), and Safren, Sprich, Mimiaga, et al. (2010) studies was 100%, but it was merely 38.89% in our sample. And it was reported that stimulants and tomoxetine could improveADHD patients’ anxiety and depression symptoms (Atomoxetine ADHD and Comorbid MDD Study Group et al., 2007; Coughlin et al., 2015). Also, the severity of comorbid depression and anxiety at baseline might be different in different study samples. For example, in our study, only 20.37% met the diagnosis of mood disorders and 0.93% with anxiety disorders; this could mean limited space for improvement by CBT.
Comparing with control group, both CBT only group and CBT + booster group performed significantly better in SOC problem solving and SOC thinking time. This suggests CBT improved the spatial planning and spatial working memory. This improvement on planning is corresponding to the content of organization and planning of CBT. The RVP was suggested as an endophenotype of ADHD (Gau & Huang, 2014); however, this study did not find significant improvement after CBT. One previous study using computerized tests also failed to show significant improvement after CBT (Virta et al., 2010). One possible reason was that these tests were too simple for adult patients (Virta et al., 2010), especially those with high IQ. The mean IQ of all three groups in this study was above 120 in our study, which could compensate for EF’s deficits (Milioni et al., 2014).
EF in everyday life is an important supplement to conventional neuropsychological tests (Kamradt, Ullsperger, & Nikolas, 2014), and we found the MI on BRIEF-A significantly improved after CBT. MI included five factors and reflected the individual’s ability to initiate tasks and generate problem-solving thoughts, to maintain working memory, to organize and monitor problem-solving processes, and to organize one’s materials and environment (Roth et al., 2005). Comparing with healthy controls, patients with adult ADHD had more difficulties on items belonging to MI than the BRI, which was the other part of BRIEF-A (Grane, Endestad, Pinto, & Solbakk, 2014). Our study showed that CBT was associated with significant improvement on MI, which consisted of several subscales rather than in a separate factor; this could mean CBT is nonspecific and may target different EFs at the same time. Previous studies also showed similar findings. For example, Stevenson, Whitmont, Bornholt, Livesey, and Stevenson (2002) reported that cognitive remediation program improved the ability of planning and organization (Stevenson et al., 2002), and another study showed metacognitive therapy improved the ability of time management (Bramham et al., 2009).
We found CBT could improve motor impairments on BIS. The motor factor represented the tendency to act without thinking and restlessness (Patton, Stanford, & Barratt, 1995), a core impairment of ADHD. This finding is important as it supports CBT’s efficacy on one of the core symptoms.
With respect to quality of life, previous studies showed that health condition (Philipsen et al., 2007), relationship (Antshel, Faraone, & Gordon, 2014), and social functioning (Weiss et al., 2012) improved after CBT. Using the WHOQOL-BREF, we did not find significant improvement in quality of life, which is consistent with the findings of S. Young et al. (2015). Although the WHOQOL-BREF may be a good instrument for a wide range of people (Agarwal, Goldenberg, Perry, & Ishak, 2012), some suggest more specific tools for adults with ADHD such as Adult ADHD Quality of Life (AAQoL; Brod, Perwien, Adler, Spencer, & Johnston, 2005) should be used. However, Young et al. found a significant time effect on quality of life and suggested that functional improvements may take longer to improve compared with ADHD core symptoms (S. Young et al., 2015). Similarly, in our study, immediate improvement was mostly restricted to core ADHD symptoms, so long-term effects of CBT on real-world functions need to be explored.
The Effects of Booster Sessions
Booster sessions were included in the study based on the following considerations: First, although the acute effect is validated, lasting effect of CBT for adult ADHD is unclear (Knouse & Safren, 2010). Second, based on the data in our previous follow-up study (Wang et al., 2014), patients reported that they forgot some skills learned in CBT and had difficulties in applying them into practice in real life. Third, booster sessions are rather easy to do as their contents are mainly the summary of previous therapy and they also make economic sense to review and consolidate what patients have already learned in the acute phase.
However, contrary to our expectation, comparing with CBT only group, the booster sessions were not associated with significant additional improvement. This could be due to several factors. First, as we discussed above, outpatients in this study had relatively high IQ and education; thus, they might be only representative of patients with mild impairments (Milioni et al., 2014) and there could well be a ceiling effect for CBT in this sample. Our data showed that the proportion of treatment responders of CBT +booster group was larger than that of CBT only group at 24th week; although not significant, this suggests some patients, who did not respond to the acute CBT treatment, improved further during the booster sessions. Second, some of the measurements we used, while they might be appropriate for the acute phase, might not be appropriate for the booster sessions. Third, outcomes were only evaluated at the end of booster sessions; hence, long-term outcomes needed to be explored, as suggested by some authors (S. Young et al., 2015).
Limitations
A few limitations of this trial need to be acknowledged. First, the samples and diagnostic criteria. Overall, patients enrolled in this trial had relatively high IQ and education level, which is not representative of the entire adult ADHD population. It is unclear how this could have affected the results, although some suggested that “average-IQ” adult patients with ADHD display similar patterns of functional impairments and psychiatric comorbidities that parallel those found in the high-IQ patients (Antshel et al., 2009). We used diagnostic criteria based on DSM-IV instead of Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013), which might exclude participants who meet the diagnosis of adult ADHD of DSM-5. Of note, the patients who were able to commit to the clinical trial and attend the weekly CBT might have less impairments, which might limit the generalizability.In order to recruit a large sample, we included patients with some mild comorbidities and who were on current ADHD medications, which could also have influenced the results, although their percentage in the sample was less than 50%.
Second, the measures of outcome. We used the core ADHD symptoms as the primary indicator of the efficacy, as reported in previous studies (Safren, Sprich, Mimiaga, et al., 2010; Steele et al., 2006), but social functional impairments are prominent in patients with adult ADHD (Safren, Sprich, Cooper-Vince, et al., 2010) and might be a sensitive index to CBT and boosters, which need to be explored in the future. And in this study, we did not select patients who had severe general functional impairments like previous studies (Safren et al., 2005; Safren, Sprich, Mimiaga, et al., 2010), which could also limit our findings. On the other side, we only used self - reported measures in this study. Measurements based on informant perspectives need to be included in the future.
Third, the placebo effects could not be ruled out as the design of the waiting group could not fully reflect the effect of CBT or booster sessions by comparison, and a control group with nondirective activities such as self-help group and psychoeducation might be better.
Finally, the dropout rate of this study was relatively high, especially at the 24th week, which is in line with previous studies and reflects the very nature of adult ADHD (Philipsen et al., 2015). Although multiple imputation helped with missing data, it may also ignoresome potential factors related to drop out (such as socioeconomic status). These drop-out related factors need to be analyzed further in the future. In this study, efficacy of booster sessions might be limited by decreased attendance, so future studies should apply more psychotherapy strategies to retainpatients or change the form to investigate the outcomes of boosters.
Conclusion
To our knowledge, this study is the first RCT of CBT for adults with ADHD in China and it is also the first to examine the multidimensional effects of CBT and its booster sessions. We found that 12 weeks of group CBT was effective for adults with ADHD on core ADHD symptoms, impulsivity, daily life EF, spatial planning, and working memory, which suggests that CBT is a cross-cultural therapy for adult ADHD. This study did not find group CBT to be efficacious for anxiety and depressive symptoms, self-esteem, and quality of life. These findings, if replicated, will help us identify target symptoms of CBT and improve our understanding of the mechanism of CBT. To our surprise, we found that three monthly booster sessions were not associated with more sustained or additional benefits. In summary, we found that group CBT was effective for Chinese adult patients with ADHD. Booster sessions do not appear to provide additional benefits. Replication studies in larger samples with more representative patients are needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Beijing Municipal Science and Technology Commission (Z131107002213068), the National Key Technology R&D Program (2015BAI13B01), and the Capital Health Research and Development of Special (2016-2-4113).
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.