
Abstract
Estimated to affect more than 8% of the population (Larson, Russ, Kahn, & Halfon, 2011), ADHD is a common mental health disorder of childhood, with associated symptoms and impairment persisting into adolescence and adulthood (Bernardi et al., 2012). Although research has established that symptoms of ADHD are equally as common among Latinos as in their European American counterparts (Morgan, Hillemeir, Farkas, & Maczuga, 2014), there is a relative disparity of research regarding the best practices for the assessment and diagnosis of ADHD in this population. Therefore, the current study examined the incremental clinical utility of adding parent- and teacher-reported functional impairment, which may be less influenced by cultural factors than symptomatology (Pelham, Fabiano, & Massetti, 2005), to a standard ADHD assessment battery in a sample of Latino children, in an effort to add to the growing knowledge base about how best to assess and treat ADHD in Latinos.
Symptoms and Clinical Correlates of ADHD
ADHD is one of the most common psychiatric disorders beginning in childhood, with a high prevalence that continues to rise. A recent study reported that 8.2% of children had a diagnosis of ADHD (Larson et al., 2011), representing an increase of 5.5% every year from 2003 to 2007 (Visser, Bitsko, Danielson, Perou, & Blumberg, 2010). Sources such as the National Institute of Mental Health (NIMH) describe ADHD as being characterized by persistent and severe inattention, hyperactivity, and impulsivity (NIMH, 2012). ADHD also is associated with a number of clinical correlates, including risky behaviors, high perceived stress, and comorbid psychiatric conditions, such as mood, anxiety, and personality disorders (Bernardi et al., 2012). Up to 67% of those with ADHD are reported to have at least one comorbid condition (Larson et al., 2011). These symptoms and clinical correlates cause significant impairment across the domains of home, school, and peer relationships (Bernardi et al., 2012).
Assessment of ADHD
The early assessment and diagnosis of ADHD is crucial in ameliorating the negative outcomes associated with leaving the condition untreated. The assessment process should be completed with as little time and expense as possible, to facilitate prompt treatment and limit financial strain on both clinicians and families (Pelham et al., 2005). However, to correctly diagnose ADHD, the assessment process also must be comprehensive, including multiple informants and addressing symptomology across all relevant domains of functioning. Pelham, Fabiano, and Massetti’s (2005) review designated several types of ADHD assessment measures as being evidence based, representing the gold standard. These include measures based on the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013), global measures of impairment, rating scales that are empirically and rationally derived, structured interviews, and behavioral observations (Pelham et al., 2005). Research also has indicated the importance of administering assessment measures to both parents and teachers, to obtain information from multiple informants across multiple settings (Pelham et al., 2005).
Functional Impairment
One important consideration related to ADHD assessment regards functional impairment. Although moderate to strong correlations have been found between teacher- and parent-reported symptoms and functional impairment in those with ADHD, the two are distinct from one another and contribute uniquely to a full understanding of the condition (Fabiano et al., 2006). It has been suggested that the main focus of ADHD assessment and treatment should be on impairment, as it is associated with parental recognition of concerns, is often the impetus for initiating the assessment process, and predicts long-term outcomes (Arcia & Fernandez, 2003; Pelham et al., 2005). Assessing impairment, as opposed to meeting a specific symptom count, may more effectively identify individuals with ADHD (Sibley et al., 2012). Impairment has been used in combination with symptoms of ADHD and comorbid disorders to differentiate between individuals with and without ADHD (Harrison, Vannest, & Reynolds, 2011).
In addition, functional impairment is considered to be a more universal concept than symptom presentation, which may be subject to cultural bias. Latino parents, for instance, have been found to be less likely to endorse biopsychosocial explanations of mental health problems than their non-Hispanic White counterparts (Yeh, Hough, McCabe, Lau, & Garland, 2004). Meanwhile, measures of impairment have been found to be less sensitive to factors, such as ethnicity, while still effectively distinguishing between children with and without ADHD, indicating their usefulness in assessing ADHD in diverse populations (Pelham et al., 2005). Research suggests that individuals at risk of experiencing barriers to problem recognition may have more limited experience with and knowledge about mental health disorders and services (Gerdes, Lawton, Haack, & Schneider, 2014). Therefore, measures of impairment may be more salient for these individuals, as impairment is more likely to be identified than are the prevailing biopsychosocial conceptualizations of etiology and symptomatology (Yeh et al., 2004).
Incremental Utility and Validity
To facilitate early and accurate identification of ADHD and subsequent intervention, research has compared various assessment measures for ADHD to identify the most diagnostically efficient and effective measures. The incremental validity and/or utility of each measure, or its ability to effectively diagnose a condition of interest and/or the benefits associated with using the measure, can be identified via hierarchical regression (see Lindenberger & Potter, 1998, for a review). A useful example of this technique can be found in Vaughn and Hoza’s (2012) study, which compared the incremental utility of a structured diagnostic interview and rating scales obtained from multiple informants in diagnosing ADHD. It was hypothesized that teacher ratings would significantly improve predictive models using parent ratings alone and that a structured diagnostic interview would not significantly improve a model including parent and teacher ratings. Hierarchical logistic regressions revealed that teacher ratings added predictive utility beyond parent ratings, whereas structured diagnostic interviews did not add predictive utility beyond that of parent and teacher ratings (Vaughn & Hoza, 2012).
U.S. Latino Youth
Despite the important advances that have been made related to the assessment of ADHD described above, certain groups have received limited research attention to date, and our knowledge about ADHD in these groups is still lacking. One such underresearched and underserved group is Latino youth. Latinos are the largest and fastest growing ethnic minority group in the United States today, making up more than 15% of the U.S. population (Ennis, Rios-Vargas, & Albert, 2011). Rates of psychopathology in Latino youth are similar or higher as compared to other groups, but Latinos are less likely to seek and receive high-quality mental health assessment and treatment services (Flores, 2010; U.S. Department of Health and Human Services [DHHS], 2001).
More specifically, while the prevalence of ADHD symptomatology has been found to be consistent between European Americans and Latinos, Latino individuals are less likely to receive an official diagnosis of ADHD and treatment for the condition. This is especially true of Latino children who do not speak English in the home (Eiraldi & Diaz, 2010; Morgan et al., 2014). In addition, as the prevalence of ADHD rises in general, the greatest increase has been found in Latinos and in individuals with a primary language other than English. The lifetime prevalence of ADHD in Latinos increased by 53% between 2003 and 2007 (Visser et al., 2010).
Factors specific to certain subgroups of Latinos in the U.S. may contribute to this disparity, including limited availability of linguistically appropriate services, financial concerns, limited positive experiences with mental health services, beliefs about the etiology of ADHD, and cultural factors, such as acculturation (Eiraldi, Mazzuca, Clarke, & Power, 2006; Lawton, Gerdes, Haack, & Schneider, 2014). It has been reported that Latino parents who subscribe to traditional cultural values are more likely to have beliefs about the etiology of ADHD that fall outside of a biopsychosocial explanation (Lawton et al., 2014). Such beliefs may interfere with seeking diagnostic services from a mental health clinician.
One way in which clinicians can be sensitive to these issues is to incorporate the more easily understood concept of functional impairment into the assessment and treatment of ADHD, rather than focusing on symptomology alone. For example, a culturally sensitive measure of ADHD-related functional impairment has been developed and validated specifically for use with Latinos (Haack & Gerdes, 2016; Haack, Gerdes, Lawton, & Schneider, 2014). Early research found no significant relationships between the ADHD Functional Impairment Scale (ADHD-FX Scale) and Anglo or Latino acculturation, suggesting the appropriateness of this measure as part of a comprehensive ADHD assessment for Latino youth (Haack & Gerdes, 2016).
In addition, higher maternal perceptions of functional impairment have been found to be associated with increased maternal distress in Latina mothers of children with ADHD (Arcia & Fernandez, 2003), even when the same mothers may not identify symptoms of ADHD. In other words, Latina mothers may be more likely to seek help for their children’s functional impairment, as opposed to their ADHD symptoms. A positive association between high levels of functional impairment and subsequent help-seeking behavior in Latinos has been supported in the literature as well (Eiraldi et al., 2006). This preliminary research is encouraging and supports the importance of considering functional impairment when assessing ADHD in Latino youth.
Current Study and Hypotheses
The current study makes a new contribution to the knowledge base about ADHD assessment, extending Vaughn and Hoza’s (2012) examination of the incremental utility of ADHD assessment measures by (a) incorporating a measure of functional impairment and (b) examining Latino youth, an understudied group. First, it was hypothesized that there would be a medium positive correlation, a high percent agreement, and significant agreement as indicated by kappas between each item on the parent and teacher Disruptive Behavior Disorders Rating Scale (DBD Rating Scale) and its corresponding item on the Disruptive Behavior Disorders Structured Interview (DBD Structured Interview), which reflects the clinician’s final clinical judgment regarding the symptom.
Second, it was hypothesized that after controlling for parent- and teacher-reported hyperactivity/impulsivity and inattention (parent and teacher DBD Rating Scale), parent-reported functional impairment in the home and teacher-reported functional impairment at school (parent and teacher ADHD-FX Scale) would account for additional variance in ADHD diagnostic status.It also was expected that each of these variables would individually add incremental predictive utility to a model predicting ADHD diagnostic status.
Lastly, it was hypothesized that after controlling for parent-reported hyperactivity/impulsivity and inattention and functional impairment in the home (parent DBD Rating Scale and ADHD-FX Scale), teacher-reported hyperactivity/impulsivity and inattention and functional impairment at school (teacher DBD Rating Scale and ADHD-FX Scale) would account for additional variance in ADHD diagnostic status. It also was expected that each of these variables would individually add incremental predictive utility to a model predicting ADHD diagnostic status.
Finally, exploratory analyses were conducted. Although specific predictions were not made given the lack of previous research in this area, correlations between mean functional impairment in the home and school settings (parent and teacher ADHD-FX Scale) and mean hyperactivity/impulsivity and inattention (parent and teacher DBD Structured Interview) also were examined.
Method
Participants
Participants in the current study included school-aged Latino youth who were assessed for ADHD as part of a larger research project, their primary parent, and their primary teacher. Seventy-four families consented to participate in the study and began the assessment process; of these, 71 families completed the assessment process. One additional family was missing data on outcome measures, resulting in a final sample size of 70. Approximately 86% of the youth were diagnosed with ADHD following the evaluation. The majority of the participating youth were born in the United States (94.3%) and most were male (67.1%); the mean age was 8.13 years old (SD = 2.51 years). See Table 1 for more demographic information.
Demographic Variables.
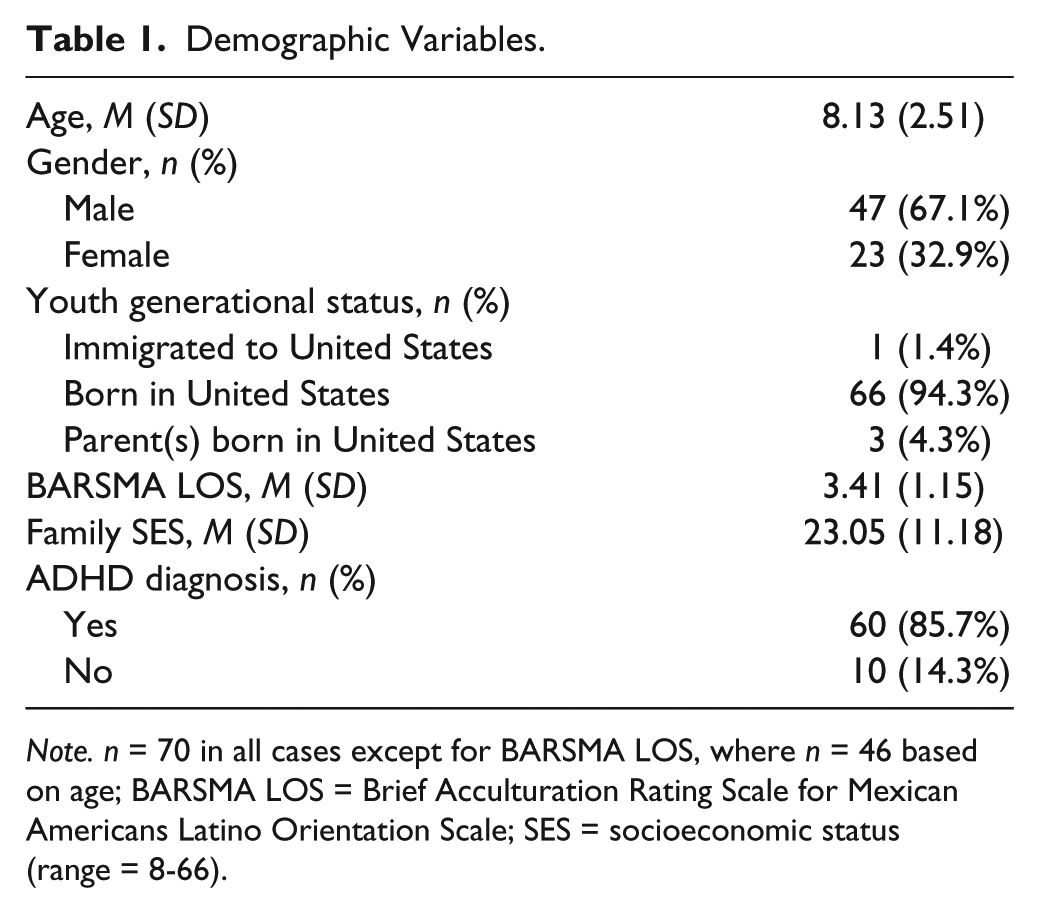
Note. n = 70 in all cases except for BARSMA LOS, where n = 46 based on age; BARSMA LOS = Brief Acculturation Rating Scale for Mexican Americans Latino Orientation Scale; SES = socioeconomic status (range = 8-66).
Procedure
To facilitate recruitment, partnerships were established with a number of local schools and a local community center that provides services related to health and human services, education, and the arts to families, with an emphasis on Hispanic culture. Specific recruitment efforts included in-person contact with families at school-sponsored events, such as back-to-school night, flyers distributed at school, and staff meetings with schools and community center personnel.
Interested families participated in a brief phone screening to determine eligibility for the larger study, after which a comprehensive, multimodal, multi-informant ADHD assessment either at a university lab or the community center was scheduled for families who appeared to be eligible. Eligibility criteria included that participating parents self-identified as Latino and were fluent in Spanish (to allow for participation in the Spanish language treatment provided through the larger study), and that participating children self-identified as Latino, were between 5 and 13 years of age at the time of the assessment, displayed symptoms and functional problems consistent with ADHD, and did not have an existing diagnosis of intellectual disability, autism spectrum disorder, or a psychotic disorder. The entire assessment process with the family took approximately 4 hours; the parent portion was conducted in Spanish, and the child portion was conducted in either Spanish or English, depending on the child’s preference.
After obtaining consent and assent from the parent(s) and child, respectively, a graduate student clinician conducted an unstructured interview with the parent(s) and assisted them, as needed, in completing several measures assessing ADHD symptomatology, functional impairment, parental and family factors, and acculturation and cultural factors, as well as a demographic form. The participating child also completed an unstructured interview with a trained undergraduate research assistant and completed several measures assessing mood, anxiety, and acculturation and cultural factors. The measures relevant to the current study are described in more detail below. Each family received a US$100 Target gift card once they completed the assessment.
After the initial assessment appointment with the parent and child, the graduate student clinician contacted the child’s primary teacher and arranged a date to meet at the school. Following the consent process, the graduate student clinician conducted a brief unstructured interview with the teacher and provided him or her with several measures assessing ADHD symptomatology and functional impairment to complete. The measures relevant to the current study are described in more detail below. Each teacher received a US$5 Target gift card once he or she completed the interview and measures.
Diagnostic and subtype decisions were made based on all available information gathered during the assessment, with a specific focus on parent and teacher unstructured interviews, parent and teacher responses on the DBD Rating Scale and ADHD-FX Scale, and behavioral observations. Specifically, graduate student clinicians and a faculty expert on ADHD used the above information to make a final clinical judgment regarding the severity of each ADHD symptom on the DBD Structured Interview.
Measures
The measures of interest for the current study include a demographic form, the DBD Rating Scale, ADHD-FX Scale, DBD Structured Interview, and Brief Acculturation Rating Scale for Mexican Americans–II (BARSMA-II).
Demographic form
Parents completed a demographic form that served to gather information about participating children and parents, including age, gender, socioeconomic status (SES), and generational status.
DBD Rating Scale
The DBD Rating Scale is a well-known, DSM-based parent and teacher report measure of ADHD, oppositional/defiant disorder (ODD), and conduct disorder (CD) symptoms (Pelham, Gnagy, Greenslade, & Milich, 1992). The scale has 45 items that are endorsed by parents and/or teachers on a Likert-type scale from 0 (symptom is not at all a problem) to 3 (symptom is very much a problem). Sample items assessing inattention, hyperactivity, and impulsivity, respectively, include “[child] often does not seem to listen when spoken to directly,” “[child] is often ‘on the go’ or often acts as if ‘driven by a motor,’” and “[child] often blurts out answers before questions have been completed.” The original English language version, which was completed by teachers, has high internal consistency and acceptable test–retest reliability, as well as treatment outcome validity (as described in Pelham et al., 2005). The Spanish language version of the DBD Rating Scale (DBD-S), which was completed by parents, has good internal consistency and convergent validity (Gerdes, Lawton, Haack, & Dieguez Hurtado, 2013). For the purposes of the current study, the means of items assessing inattention and hyperactivity/impulsivity from both the parent and teacher scales were used in statistical analyses, as were the ratings of nine individual items from the inattentive category and nine individual items from the hyperactive/impulsive category from both the parent and teacher scales. Means were used as opposed to symptom counts to facilitate comparison with previous research (Vaughn & Hoza, 2012). In the current study, the parent DBD Rating Scale demonstrated a Cronbach’s alpha of .91 for the items assessing inattention and a Cronbach’s alpha of .90 for the items assessing hyperactivity/impulsivity, while the teacher DBD Rating Scale demonstrated a Cronbach’s alpha of .88 for the items assessing inattention and a Cronbach’s alpha of .89 for the items assessing hyperactivity/impulsivity.
ADHD-FX Scale
The ADHD-FX Scale is a measure of functional impairment commonly associated with childhood ADHD. It was developed as a practical and effective measure of ADHD-specific functional impairment appropriate for families of diverse backgrounds (Haack et al., 2014). The scale has 32 items that are endorsed by parents and/or teachers on a Likert-type scale from 0 (this does not affect [child’s] day-to-day life) to 3 (this affects [child’s] day-to-day life very much). Examples of items assessing impairment in the home setting, in the school setting, and with peers, respectively, include “[child] doesn’t effectively complete home routines/tasks (e.g., the morning routine, chores),” “[child] doesn’t pay attention to, follow, and/or obey teacher instructions,” and “[child] doesn’t respect peers’ personal space.” An overall impairment score, as well as three subscale scores for school, home, and peers may be created. The Spanish language version of the parent ADHD-FX Scale, which was completed by parents, has been shown to have adequate reliability, divergent and convergent construct validity, and cultural properties (Haack, Gonring, Harris, Gerdes, & Pfiffner, 2019). Teachers completed the English language version of the teacher ADHD-FX Scale (Haack et al., 2014). Statistical analyses utilized the home subscale score on the parent ADHD-FX Scale and the school subscale score on the teacher ADHD-FX Scale. In the current study, the home subscale of the parent ADHD-FX Scale demonstrated a Cronbach’s alpha of .93, whereas the school subscale of the teacher ADHD-FX Scale demonstrated a Cronbach’s alpha of .94.
DBD Structured Interview
Parents also responded to the Spanish version of the DBD Structured Interview, in which the same 45 items that make up the DBD Rating Scale were administered in the form of a semistructured diagnostic interview. The final rating of each ADHD symptom on the DBD Structured Interview reflects the clinical judgment of the graduate student clinicians and an ADHD expert. ADHD diagnostic status was determined by symptom count.
BARSMA-II
Children at least 7 years old completed the BARSMA-II, which is a 12-question rating scale designed to assess acculturation in Mexican Americans (Cuéllar, 2004). In the current study, the words “Mexican” and “Mexican American” were replaced by “Latino” and “Latin American,” respectively, so as to make the measure more appropriate for the current sample; this method has been used previously and has been found to maintain the psychometric properties of the measure (Lawton et al., 2014). Participants completed the measure in either English or Spanish, depending on their preference, and responded to each question on a Likert-type scale from 1 (not at all) to 5 (almost always or extremely often). Examples of questions addressing Anglo and Latino cultural orientation, respectively, include “I enjoy English language movies” and “I enjoy reading books in Spanish.” Statistical analyses in the current study used both the Anglo Orientation Subscale (AOS) and the Latino Orientation Subscale (LOS). Adequate validity and internal consistency for both subscales has been demonstrated for the BARSMA-II when used with children and adolescents (Bauman, 2005). In the current study, the LOS demonstrated a Cronbach’s alpha of .84, whereas the AOS demonstrated a Cronbach’s alpha of .60. Given the low reliability of the AOS in the current sample, this subscale was not used in subsequent analyses.
Results
Preliminary Analyses
Descriptive analyses were conducted to examine the demographic characteristics of the sample. A series of t tests and a chi-square test of independence were conducted to examine potential group differences between children diagnosed and not diagnosed with ADHD with respect to child age, gender, and Latino acculturation, as well as family SES. The chi-square test revealed that male participants were more likely than female participants to be diagnosed with ADHD, χ2 = 3.90, p < .05. Given that more than 20% of expected counts in the chi-square table was less than five, a variation known as the N − 1 chi-square (Busing, Weaver, & Dubois, 2016; Campbell, 2007) also was performed; even with this correction, males were still more likely than females to be diagnosed with ADHD, N − 1 χ2 = 3.84, p < .05. No other significant differences between participants with and without ADHD were found.
A series of correlations and ANOVAs was conducted to examine potential differences in severity of parent and teacher reports of ADHD symptoms and functional impairment and final clinical judgment of ADHD symptoms based on child age, gender, and Latino acculturation, as well as family SES. Results indicated statistically significant differences based on gender for teacher reports of inattention, hyperactivity/impulsivity, and functional impairment in the classroom, as well as the final clinical judgment of inattention and hyperactivity/impulsivity, with boys rated as more severe in each of these categories (see Table 2). No other statistically significant relationships were revealed.
ANOVAs for Predictor Variables by Gender.

Note. PDBD IA = Parent Disruptive Behavior Disorders (DBD) Rating Scale: Inattention; PDBD HI = Parent DBD Rating Scale: Hyperactivity/Impulsivity; TDBD IA = Teacher DBD Rating Scale: Inattention; TDBD HI = Teacher DBD Rating Scale: Hyperactivity/Impulsivity; FCJ IA = Final Clinical Judgment: Inattention; FCJ HI = Final Clinical Judgment: Hyperactivity/Impulsivity; PFX = Parent ADHD Functional Impairment Rating Scale (ADHD-FX Scale): Home; TFX = Teacher ADHD-FX Scale: School; 0.2 = small effect, 0.5 = medium effect, 0.8 = large effect (Cohen, 1988); *p≤ .05; **p≤ 0.01; ***p≤ .001.
To examine the exploratory questions related to correspondence between parent and teacher reports of ADHD symptoms and parent and teacher reports of functional impairment in the home and at school, correlations were examined between the mean of parent-reported inattention and hyperactivity/impulsivity, mean of parent-reported functional impairment in the home, mean of teacher-reported inattention and hyperactivity/impulsivity, and mean of teacher-reported functional impairment at school, as well mean of final clinical judgment of inattention and hyperactivity/impulsivity. Several significant relationships were revealed, including between parent reports of hyperactivity/impulsivity and parent reports of inattention (r = .72, p < .001) and functional impairment (r = .76, p < .001), as well as between parent reports of inattention and parent reports of functional impairment (r = .65, p < .001). Similarly, significant relationships were noted between teacher reports of hyperactivity/impulsivity and inattention (r = .56, p < .001) and functional impairment (r = .70, p < .001), as well as between teacher reports of inattention and teacher reports of functional impairment (r = .73, p < .001). Significant relationships also were revealed between parent reports of hyperactivity/impulsivity and teacher reports of hyperactivity/impulsivity and functional impairment (r = .49, p < .001 and r = 0.33, p < .01, respectively; see Table 3).
Correlations Among Parent- and Teacher-Reported ADHD Symptoms and Functional Impairment.
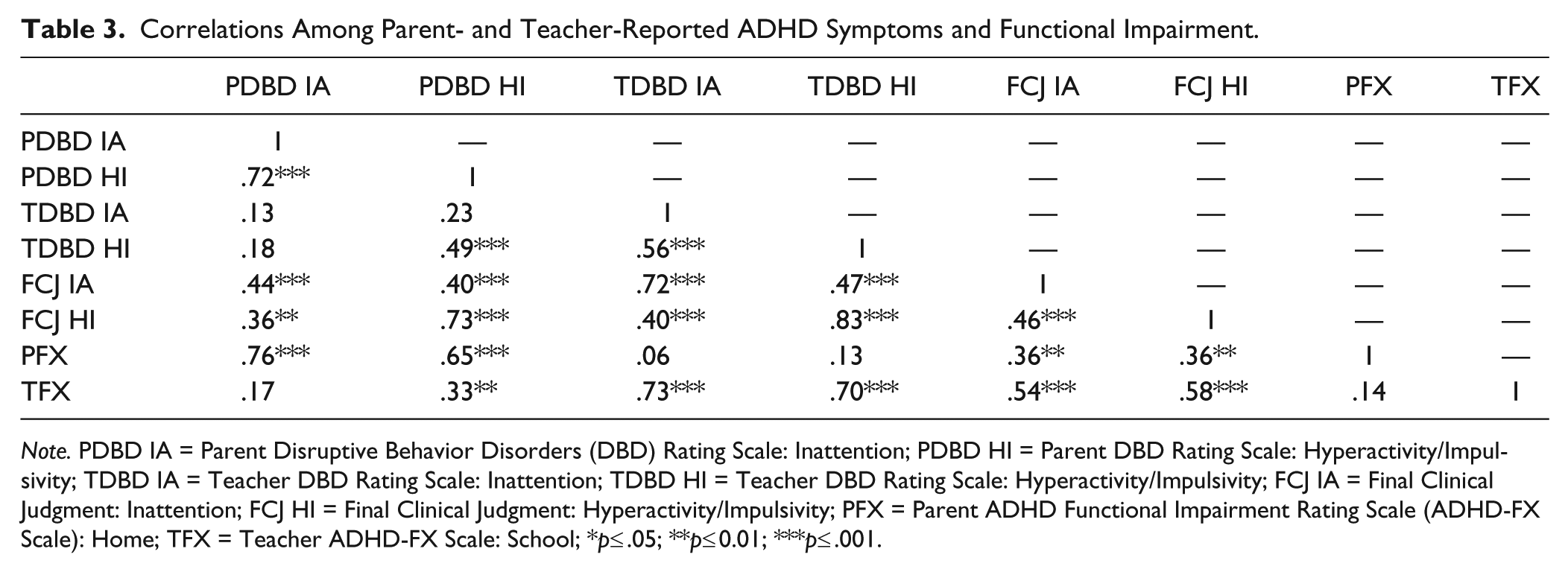
Note. PDBD IA = Parent Disruptive Behavior Disorders (DBD) Rating Scale: Inattention; PDBD HI = Parent DBD Rating Scale: Hyperactivity/Impulsivity; TDBD IA = Teacher DBD Rating Scale: Inattention; TDBD HI = Teacher DBD Rating Scale: Hyperactivity/Impulsivity; FCJ IA = Final Clinical Judgment: Inattention; FCJ HI = Final Clinical Judgment: Hyperactivity/Impulsivity; PFX = Parent ADHD Functional Impairment Rating Scale (ADHD-FX Scale): Home; TFX = Teacher ADHD-FX Scale: School; *p≤ .05; **p≤ 0.01; ***p≤ .001.
Significant relationships also were noted between final clinical judgment of inattention and hyperactivity/impulsivity and parent and teacher report of symptoms and functional impairment. Specifically, final clinical judgment of inattention was significantly related to parent and teacher reports of inattention (r = .44, p < .001 and r = .72, p < .001, respectively), hyperactivity/impulsivity (r = .40, p < .001 and r = .47, p < .01, respectively), and functional impairment (r = .36, p < .01 and r = .54, p < .001, respectively). In addition, final clinical judgment of hyperactivity/impulsivity was significantly related to parent and teacher reports of inattention (r = .36, p < .01 and r = .40, p < .001, respectively), hyperactivity/impulsivity (r = .73, p < .001 and r = .83, p < .001, respectively), and functional impairment (r = .36, p < .01 and r = .58, p < .001, respectively). Finally, final clinical judgment of inattention and final clinical judgment of hyperactivity/impulsivity were significantly related to one another (r = 0.46, p <.001) (see Table 3).
Primary Analyses
Hypothesis 1
Correspondence between each item on the parent and teacher DBD Rating Scale and its corresponding item on the DBD Structured Interview was determined via correlations, percent agreement, and kappas; exact ratings on the DBD Rating Scale and Structured Interview were used. As can be seen in Table 4, two thirds of the correlations between items assessing inattention on the parent DBD Rating Scale and corresponding items on the DBD Structured Interview were significant, ranging from .03 to .52 with a mean of .31. All of the correlations between items assessing hyperactivity/impulsivity on the parent DBD Rating Scale and corresponding items on the DBD Structured Interview were significant, ranging from .28 to .68 with a mean of .57. In contrast, correlations between all 18 items on the teacher DBD Rating Scale and the corresponding items on the DBD Structured Interview were significant, ranging from .44 to .70 and with a mean of .61 for inattention item pairs and from .56 to .77 with a mean of .69 for hyperactive/impulsive item pairs (see Table 4). Based on the preliminary analyses, these correlations also were examined taking into account gender. Because the pattern of findings remained the same, results were reported without controlling for gender.
Summary of Correlations, Percent Agreement, and Chance-Corrected Agreement (κ) Between Parent and Teacher Ratings of ADHD Symptoms on the DBD Rating Scale and Final Clinical Judgment of ADHD Symptom Severity on the DBD Structured Interview.
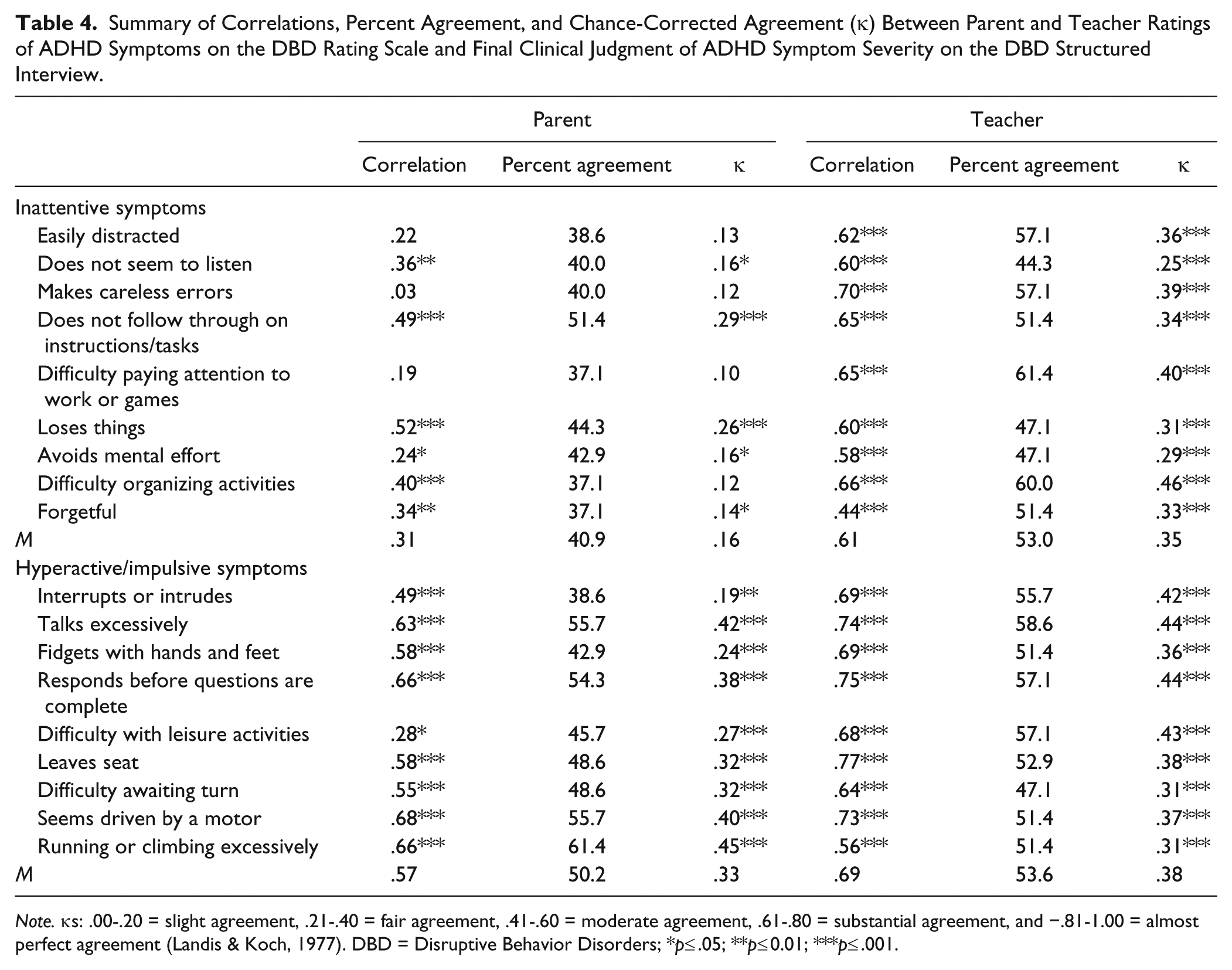
Note. κs: .00-.20 = slight agreement, .21-.40 = fair agreement, .41-.60 = moderate agreement, .61-.80 = substantial agreement, and −.81-1.00 = almost perfect agreement (Landis & Koch, 1977). DBD = Disruptive Behavior Disorders; *p≤ .05; **p≤ 0.01; ***p≤ .001.
As can be seen in Table 4, percent agreement between the parent DBD Rating Scale and the DBD Structured Interview ranged from 37.1% to 51.4% with a mean of 40.9% for items assessing inattention, and from 38.6% to 61.4% with a mean of 50.2% for items assessing hyperactivity/impulsivity. Percent agreement between the teacher DBD Rating Scale and the DBD Structured Interview ranged from 44.3% to 61.4% with a mean of 53% for items assessing inattention, and from 47.1% to 58.6% with a mean of 53.6% for items assessing hyperactivity/impulsivity.
Finally, slightly less than two thirds of kappas for items assessing inattention on the parent DBD Rating Scale items and corresponding items on the DBD Structured Interview were significant, ranging from .10 to .29 with a mean of .16. All kappas for items assessing hyperactivity/impulsivity on the parent DBD Rating Scale and corresponding items on the DBD Structured Interview were significant, ranging from .19 to .45 with a mean of .33. In contrast, all 18 kappas were significant for items on the teacher DBD Rating Scale and corresponding items on the DBD Structured Interview, ranging from .25 to .46 with a mean of .35 for items assessing inattention and from .31 to .44 with a mean of .38 for items assessing hyperactivity/impulsivity (see Table 4).
Hypothesis 2
The incremental utility of measures of ADHD symptoms and functional impairment was explored with two hierarchical binary logistic regressions, with a categorical variable representing ADHD diagnostic status as the dependent variable in both cases. In the first of these regressions, parent- and teacher-reported hyperactivity/impulsivity and inattention (means of items assessing each symptom domain on the parent and teacher DBD Rating Scales) were entered at Step 1, with parent- and teacher-reported functional impairment (the home subscale score of the parent ADHD-FX Scale and the school subscale score of the teacher ADHD-FX Scale) entered at Step 2. Parent and teacher reports of ADHD symptoms alone correctly predicted 92.9% of cases, Block χ2(4, N = 70) = 34.87, p < .001. Adding parent and teacher reports of functional impairment to this model did not result in statistically significant model improvement; nonetheless, the overall model remained significant, Block χ2(2, N = 70) = 5.29, ns; Model χ2(6, N = 70) = 40.16, p < .001 (see Table 5).
Summary of Hierarchical Binary Logistic Regressions Predicting ADHD Diagnostic Status.
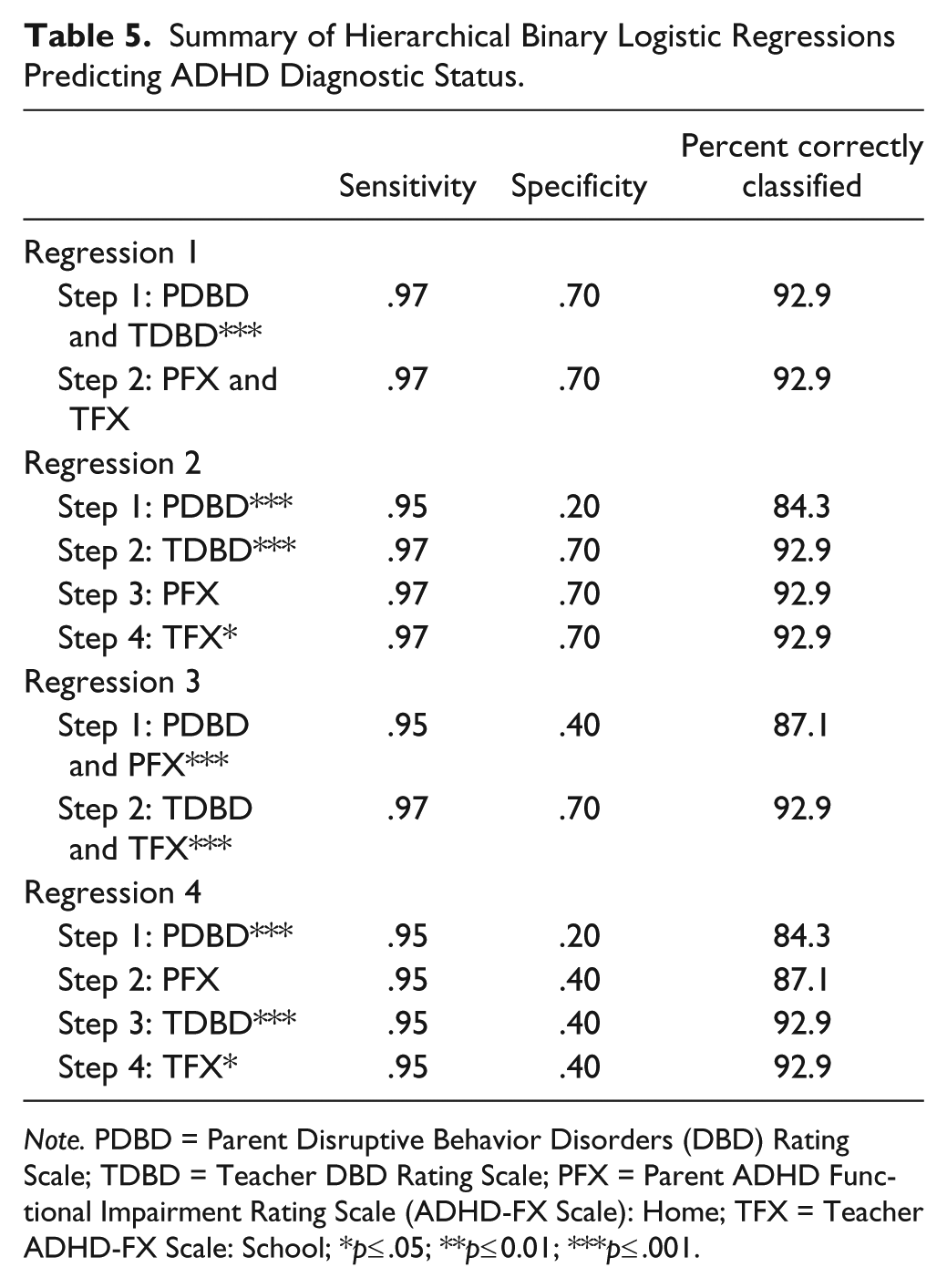
Note. PDBD = Parent Disruptive Behavior Disorders (DBD) Rating Scale; TDBD = Teacher DBD Rating Scale; PFX = Parent ADHD Functional Impairment Rating Scale (ADHD-FX Scale): Home; TFX = Teacher ADHD-FX Scale: School; *p≤ .05; **p≤ 0.01; ***p≤ .001.
A second follow-up regression was conducted to further examine the incremental utility of these measures individually. Parent-reported hyperactivity/impulsivity and inattention were entered at Step 1, teacher-reported hyperactivity/impulsivity and inattention were entered at Step 2, parent-reported functional impairment was entered at Step 3, and teacher-reported functional impairment was entered at Step 4. Parent reports of ADHD symptoms alone correctly predicted almost 85% of cases, Block χ2(2, N = 70) = 18.33, p < .001. Adding teacher reports of ADHD symptoms resulted in statistically significant model improvement and increased the predictive power of the model to 92.9%, Block χ2(2, N = 70) = 16.54, p < .001; Model χ2(4, N = 70) = 34.87, p < .001. The addition of parent reports of functional impairment to this model did not result in statistically significant model improvement; nonetheless, the overall model remained significant, Block χ2(1, N = 70) = 0.17, ns; Model χ2(5, N = 70) = 35.04, p < .001. Finally, adding teacher reports of functional impairment to this model resulted in statistically significant model improvement, Block χ2(1, N = 70) = 5.12, p < .05; Model χ2(6, N = 70) = 40.16, p < .001 (see Table 5).
Hypothesis 3
The subsequent set of regressions further examined the incremental utility of parent and teacher report measures. In the first of these regressions, parent-reported hyperactivity/impulsivity, inattention, and functional impairment were entered at Step 1, while teacher-reported hyperactivity/impulsivity, inattention, and functional impairment were entered at Step 2. Parent reports of ADHD symptoms and functional impairment alone correctly predicted ADHD diagnostic status for 87.1% of cases, Block χ2(3, N = 70) = 19.32, p < .001. Adding teacher reports of ADHD symptoms and functional impairment to this model resulted in statistically significant model improvement and an increase in predictive power of the model to 92.9%, Block χ2(3, N = 70) = 20.83, p < .001; Model χ2(6, N = 70) = 40.16, p < .001 (see Table 5).
An additional follow-up regression served to further examine the incremental utility of these measures individually. Parent-reported hyperactivity/impulsivity and inattention were entered at Step 1, parent-reported functional impairment was entered at Step 2, teacher-reported hyperactivity/impulsivity and inattention were entered at Step 3, and teacher-reported functional impairment was entered at Step 4. Parent reports of ADHD symptoms again correctly predicted ADHD diagnostic status for approximately 85% of cases, Block χ2(2, N = 70) = 18.33, p < .001. The addition of parent reports of functional impairment did not result in statistically significant model improvement, but did result in an increase in predictive power of the model to more than 87%, Block χ2(1, N = 70) = 0.99, ns; Model χ2(3, N = 70) = 19.32, p < .001. Adding teacher reports of ADHD symptoms to this model, however, did result in statistically significant model improvement, as well as an increase in the predictive power of the model to about 93%, Block χ2(2, N = 70) = 15.71, p < .001; Model χ2(5, N = 70) = 35.04, p < .001. Finally, when teacher reports of functional impairment were added to this model, statistically significant improvement of the model again resulted, Block χ2(1, N = 70) = 5.12, p < 0.05; Model χ2(6, N = 70) = 40.16, p < .001 (see Table 5). Based on the preliminary analyses, the regressions also were examined taking into account gender. Because the pattern of findings remained the same, results were reported without controlling for gender.
Discussion
The goal of the current study was to extend Vaughn and Hoza’s (2012) findings on the incremental utility of ADHD assessment measures by adding a parent- and teacher-report measure of functional impairment and by examining Spanish-speaking Latino families. Although the current teacher findings mirrored Vaughn and Hoza’s results, findings for Latino parents in the current study differed from parent findings reported by Vaughn and Hoza. Specifically, correlations, percent agreements, and kappas suggested that teachers consistently agreed with the final clinical judgment for both hyperactive/impulsive and inattentive symptoms. On the other hand, parents seemed to be in less agreement with the final clinical judgment when identifying inattentive symptoms relative to hyperactive/impulsive symptoms, based on mainstream DSM-based understandings of these symptoms. Surprisingly, results indicated that parent and teacher reports of functional impairment did not consistently add incremental diagnostic utility beyond that of parent and teacher reports of ADHD symptoms; however, follow-up analyses to be discussed shed more light on why this may be. Finally, results demonstrated that teacher reports of ADHD symptoms and functional impairment added incremental diagnostic utility beyond that of parent reports of ADHD symptoms and functional impairment, indicating the importance of obtaining teacher reports of symptomatology and functioning in the context of an ADHD assessment.
Correspondence Between Parent and Teacher DBD Rating Scales and DBD Structured Interview
Partial support was found for the first hypothesis, which predicted a medium positive correlation and a high percent agreement and kappa between each item on the parent and teacher DBD Rating Scale and its corresponding item on the DBD Structured Interview. This prediction held true for the correspondence between teacher reports and the final clinical judgment, as all items on the teacher DBD Rating Scale and corresponding items on the DBD Structured Interview were significantly positively related to each other, and most were medium in magnitude. In addition, kappas and percent agreement demonstrated fair to moderate agreement for inattentive and hyperactive/impulsive item pairs on the teacher DBD Rating Scale and corresponding items on the DBD Structured Interview. On the other hand, this prediction partially held true for the correspondence between parent reports and the final clinical judgment. Although all correlations between items on the parent DBD Rating Scale and corresponding items on the DBD Structured Interview were positive and all but one of the correlations for hyperactive/impulsive item pairs were significant, only two thirds of the correlations for inattentive item pairs were significant. Similarly, percent agreement and kappas demonstrated slight to moderate agreement for hyperactive/impulsive items on the parent DBD Rating Scale and corresponding items on the DBD Structured Interview, and slight to fair agreement for inattentive items on the parent DBD Rating Scale and corresponding items on the DBD Structured Interview.
It appears that Latino parents in the current sample were in agreement with the final clinical judgment when reporting on their children’s symptoms of hyperactivity/impulsivity more often than when reporting on their symptoms of inattention. This result differs from that of Vaughn and Hoza’s (2012) study, in which a significant positive relationship was found between the parent DBD Rating Scale and the DBD Structured Interview, with no difference for items assessing inattention versus hyperactivity/impulsivity. One possible explanation for these findings is that Latino parents may find their child’s hyperactive/impulsive behaviors to be more salient, as this type of behavior may be perceived as a lack of respect for authority figures, an important cultural value for many Latinos (i.e., Calzada, Fernandez, & Cortes, 2010). Thus, hyperactive/impulsive behaviors may be more noticeable and distressing to Latino caregivers. Given that symptoms of inattention do not necessarily suggest disrespect toward authority in the same way, they may be less salient to Latino parents.
Although findings from the current study indicate that parents are most often in agreement with the final clinical judgment when reporting on their children’s symptoms of hyperactivity/impulsivity, previous research with a community sample of Latino families suggested that parent reports of hyperactive/impulsive symptoms had lower diagnostic utility than parent reports of inattentive symptoms (Gerdes et al., 2013). Parents in the current study, however, were able to report on symptoms of hyperactivity/impulsivity in a way that was more diagnostically useful, possibly because the current study was made up of a treatment-seeking sample. The discrepancy in parental report of inattention and hyperactivity/impulsivity highlights the importance of obtaining teacher reports of symptoms as well, so as to best inform the assessment and diagnostic process.
Incremental Utility of Parent and Teacher Report of Functional Impairment
The second hypothesis that parent- and teacher-reported functional impairment would account for additional variance in ADHD diagnostic status beyond parent and teacher reports of ADHD symptoms was not supported. This prediction was made based on previous research suggesting that measuring functional impairment is a valuable component of an ADHD assessment (i.e., Pelham et al., 2005), particularly for Latino families (Haack & Gerdes, 2016; Haack et al., 2019). Although parent and teacher reports of ADHD symptoms alone correctly predicted ADHD diagnostic status for the vast majority of cases, adding parent and teacher reports of functional impairment to this model did not add incremental predictive utility to the model. Nonetheless, it should be noted that the addition of teacher reports of functional impairment alone did result in statistically significant model improvement.
One possible explanation for these findings is that parent and teacher reports of ADHD symptoms accounted for so much of the variance in ADHD diagnostic status that it was not possible for parent and teacher reports of functional impairment to result in statistically significant improvement of the model. Follow-up analyses were conducted to further examine this possibility, in which the predictor variables were entered in reverse order, such that parent and teacher reports of functional impairment were entered first and parent and teacher reports of ADHD symptoms were entered second. Results indicated that parent and teacher reports of functional impairment correctly predicted the vast majority of cases when they were entered first in a model predicting ADHD diagnostic status. Furthermore, although adding parent and teacher reports of ADHD symptoms to the model resulted in statistically significant improvement of the model, it did not increase predictive power of the model. Thus, parent and teacher reports of functional impairment accounted for so much of the variance in ADHD diagnostic status that it was not possible for the addition of parent and teacher reports of ADHD symptoms to result in statistically significant improvement of the model. These findings suggest that both parent and teacher reports of both ADHD symptoms and functional impairment were able to predict ADHD diagnostic status for the vast majority of the current sample when entered first, indicating that both can be critical to the diagnostic process.
Incremental Utility of Teacher Report of ADHD Symptoms and Functional Impairment
Finally, the hypothesis that incremental utility of teacher reports of ADHD symptoms and functional impairment would predict ADHD diagnostic status was supported. It was predicted that these measures would account for additional variance in ADHD diagnostic status, beyond parent reports of ADHD symptoms and functional impairment. Although parent reports of ADHD symptoms and functional impairment alone correctly predicted ADHD diagnostic status for the majority of cases, the addition of teacher reports of ADHD symptoms and functional impairment to this model added incremental predictive utility to the model. When examining the incremental utility of teacher reports of ADHD symptoms and functional impairment separately, the addition of teacher reports of ADHD symptoms to a model including parent reports of ADHD symptoms and functional impairment added incremental predictive utility. Adding teacher reports of functional impairment to this model, however, did not result in statistically significant improvement of the model.
Teacher reports of ADHD symptoms and functional impairment facilitated accurate diagnostic decision making in the current study, whereas parent reports of ADHD symptoms and functional impairment provided a different and valuable perspective, in that parents understood their children’s behavior differently than did teachers and clinicians. These results fit well with previous research, as the importance of gathering information from both parents and teachers and across multiple settings is considered a gold standard in ADHD assessment (i.e., Pelham et al., 2005). For example, Sibley and colleagues (2012) suggested that using both parent and teacher reports to assess ADHD is the best practice, as it resulted in the most accurate diagnoses over time. In addition, Vaughn and Hoza (2012) found that both parent- and teacher-report measures play an important role in ADHD assessment and that both contribute unique predictive utility to models predicting ADHD diagnostic status. Similarly, the results of the current study emphasize the important role that both parent and teacher reports play in ADHD assessment and diagnosis.
Limitations
Several limitations of the current study should be noted. The current study had a relatively small sample size, especially in terms of children not diagnosed with ADHD, which may have limited the specificity of predictive models. Future research could aim to recruit a larger sample, including more children without ADHD. In addition, the current study’s relatively homogeneous sample of Latinos from a midsized Midwestern city may limit the generalizability of the findings to Latinos in other areas. Future research should strive to recruit a more diverse group of Latinos, across both geographic regions and Latino subgroups, so as to obtain a clearer understanding of to whom the findings of the current study apply. The sample was somewhat homogeneous in terms of SES as well; future research also could examine whether the findings of the current study apply to a broader range of SES. In addition, although participants in the current study ranged in age from 5 to 13 years, the mean age was approximately 8 years, with a relatively small standard deviation of 2.5 years. Given that the sample was relatively homogeneous in this sense as well, future research should examine whether the findings hold true in a sample of students of different ages.
Summary and Clinical Implications
In sum, the current study extended Vaughn and Hoza’s (2012) study on the incremental clinical utility of ADHD assessment measures by examining a measure of functional impairment as part of an ADHD assessment battery with Spanish-speaking Latino families. Results of the current study support those of Vaughn and Hoza’s study in terms of the correspondence between teacher reports of ADHD symptoms and the final clinical judgment, but diverge from Vaughn and Hoza’s findings regarding the relationship between parent reports of ADHD symptoms and the final clinical judgment. Although teachers were consistently in agreement with the final clinical judgment when reporting on symptoms of inattention and hyperactivity/impulsivity, Latino parents in the current sample were more often in agreement with the final clinical judgment when reporting on symptoms of hyperactivity/impulsivity than when reporting on symptoms of inattention. Contrary to expectations, results of the current study also indicate that parent and teacher reports of functional impairment did not consistently add incremental utility beyond that of parent and teacher reports of ADHD symptoms, although teacher reports of functional impairment did significantly improve predictive models. Follow-up analyses, however, revealed that both parent and teacher reports of ADHD symptoms and functional impairment have high diagnostic utility when examined individually. Finally, results indicate that teacher reports of ADHD symptoms and functional impairment add incremental utility beyond that of parent reports of ADHD symptoms and functional impairment, highlighting the importance of obtaining both parent and teacher reports in ADHD assessments.
The current study also has important clinical implications. Previous research has shown that, although rates of psychopathology in the Latino population are similar to or higher than other groups, Latinos are less likely than other groups to seek and receive high-quality mental health assessment and treatment services (Flores, 2010; U.S. DHHS, 2001). As this population continues to grow, mental health service providers need to know how to best serve this group. Research must continue to identify the most efficient and effective measures in diagnosing mental health conditions in Latino youth, including ADHD. Results of the current study shed further light on the degree of agreement between clinicians and parents and teachers, and support the use of parent and teacher reports of symptoms and functional impairment in assessing ADHD. Use of evidence-based practice is vital to promoting efficient, effective ADHD assessment. This is of the utmost importance when working with Latino families, as both cultural and practical barriers may otherwise interfere with individuals receiving the care they need (Kouyoumdjian, Zamboanga, & Hansen, 2003).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding Sources Eunice Kennedy Shriver National Institute of Child Health and Human Development (Grant/Award Number “R21HD078553”).The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.