
Abstract
Introduction
ADHD is a common neurodevelopmental disorder characterized by difficulties in regulating attention, activity, and impulsivity (American Psychiatric Association, 2013). Although manifesting typically during childhood and adolescence, symptoms persist into adulthood in a majority of cases, either as a full clinical picture or as a partial syndrome (Biederman, Petty, Evans, Small, & Faraone, 2010). The overall prevalence of adult ADHD in a transnational study has been estimated between 1.2% and 7.3% and averaged 3.7%, with rates typically being higher for men and individuals from lower socioeconomic status (Fayyad et al., 2007).
Previous findings suggest that individuals with ADHD are at greater risk of engaging in and being convicted of a broad range of criminal behaviors (Dalsgaard, Mortensen, Frydenberg, & Thomsen, 2013). In fact, prior research conducted within prison settings has found significantly increased rates of ADHD among inmates, when compared with nonoffender controls (Cahill et al., 2012; Einarsson, Sigurdsson, Gudjonsson, Newton, & Bragason, 2009; Hamzeloo, Mashhadi, & Salehi Fadardi, 2016; Moore, Sunjic, Kaye, Archer, & Indig, 2013; Rösler et al., 2004; Usher, Stewart, & Wilton, 2013). Thus, a recent meta-analysis showed a fivefold increase in prevalence of ADHD in youth prison populations (30.1%) and a 10-fold increase in adult prison populations (26.2%; Young, Moss, Sedgwick, Fridman, & Hodgkins, 2015).
Moreover, there is a substantial comorbidity rate between ADHD and psychiatric conditions typically seen in forensic populations, particularly oppositional defiant disorder (ODD) and conduct disorder (CD) during adolescence (Angold, Costello, & Erkanli, 1999) as well as substance abuse (González, Vélez-Pastrana, Varcárcel, Levin, & Albizu-García, 2015) and antisocial personality disorder (ASPD) later in life (Matthies & Philipsen, 2016). Despite the higher risk of deviant behavior associated with those comorbidities (Hofvander, Ossowski, Lundström, & Anckarsäter, 2009; Moffitt, Caspi, Rutter, & Silva, 2001), ADHD has been suggested as an independent risk factor for criminality (Lundström et al., 2014).
Although it remains unclear whether ADHD has a causative role in criminal behaviors, there are several theories to explain this association. A direct link between ADHD symptoms and criminal behavior has been suggested as deficiencies in self-control and self-regulation, commonly observed in ADHD patients, manifest frequently by reactive and impulsive responding, mood instability, and low frustration tolerance (Young & Thome, 2011). In addition, the higher than expected prevalence rates of ADHD in the offender population can reflect the overlap of ADHD features with other conditions associated with disruptive behaviors. For example, individuals with ADHD show a wide range of reward deficits like aversion to reward delays (Bitsakou, Psychogiou, Thompson, & Sonuga-Barke, 2009) and impaired behavioral modification to rewards (Johansen et al., 2009) also observed in individuals with antisocial personality disorder (Bjork & Pardini, 2015).
Indeed, the higher rates of criminality and prevalence of comorbid ASPD in ADHD (Hofvander et al., 2009; Matthies & Philipsen, 2016) support a possible link between this disorder and psychopathy, understood as a specific constellation of personality traits of interpersonal arrogance and deceit, lack of affective resonance, and a pattern of impulsive and irresponsible behavior (Cooke & Michie, 2001).
To add further evidence to this complex topic, the current study aimed to examine the prevalence of adult ADHD in a high-security facility in Coimbra, Portugal, and to investigate the relation between ADHD symptoms and psychopathic traits in criminal offenders.
Materials and Methods
Participants
Participants were recruited between October 2015 and January 2016 among the inmates from the Central Penitentiary of Coimbra, a high-security all-male correctional facility, located in the central region of Portugal, having a population of 424 male inmates at the study start.
Prisoners with 18 to 65 years old, having at least 4 years of formal education and enough knowledge of the Portuguese language to allow the self-administration of the questionnaires were eligible to enter the study. Inmates were randomly selected by the guards, and a written informed consent was obtained from all the participants. The ethics committee of the Penitentiary of Coimbra approved all the procedures used in this study, including the method of obtaining consent, in accordance with the Declaration of Helsinki.
The participants were given a two-part questionnaire: the first part filled out with the help of the investigators and the last of self-administration.
Materials
In the first part of the interview, participants were asked regarding the following:
The second part of the assessment consisted in a self-administered questionnaire including the following:
Brief Symptom Inventory (BSI)
The BSI (Derogatis & Melisaratos, 1983) is a 53-item self-report inventory in which participants rate the extent to which they have been bothered in the past week by various symptoms, in a 5-point Likert-type scale (0 = not at all to 4 = extremely). The BSI has nine subscales designed to assess individual symptom groups: somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. This scale is reported to have good psychometric properties and has been widely used in both clinical and research settings. It has been validated for the Portuguese population.
Triarchic Psychopathy Measure (TriPM)
The TriPM (Patrick, 2010) is an Instrument based on the Triarchic Model of psychopathy, proposed by Patrick, Fowles, and Krueger (2009), which describes the psychopathic phenotype through three constructs: disinhibition (tendency toward impulsivity, irresponsibility, oppositional behavior, anger/hostility), boldness (tendency for dominance, low anxiety, venturesomeness), and meanness (tendency for superficiality, cruelty, predatory aggression, thrill seeking). Each of these constructs is assessed by one of the three TriPM subscales (20 items for disinhibition, 19 items for boldness, and 19 items for meanness). The 58 questions are assessed in a 4-point Likert-type scale (False, Somewhat False, Somewhat True, True), where 0 score is attributed if the trait is lacking (“False” in direct and “True” in reverse questions) and 3 in the opposite case, up to a maximum of 174 in the total score. We chose to use this scale over the more widely used Psychopathy Checklist-Revised (PCL-R) (Hare, 2003) as it might reveal previously ignored associations, as it divides the psychopathy construct in different personality dimensions, in contrast with PCL-R-based instruments, which assess psychopathy as a unitary construct. It has a validated Portuguese translation (Vieira et al., 2014) and has been validated for criminal populations (Stanley et al., 2013).
Adult ADHD Self-Report Scale Version 1.1 (ASRS-V 1.1)
The ASRS-V 1.1 (Kessler et al., 2005) is an instrument consisting of the 18 Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) criteria. It contains 18 questions (half for inattention symptoms, half for hyperactive/impulsive symptoms), and, using a 5-point Likert-type scale, the participants report the frequency of each item in the past 6 months, ranging from 0 (never) to 4 (very often). When used as a screening tool, it is divided in two parts: Part A is composed by six questions that were found to be the most predictive of symptoms consistent with ADHD; Part B of the Symptom Checklist contains the remaining 12 questions. Only the former is used to score individuals as ADHD positive, if more than four out of six items code positive. For the purpose of the present study, the symptom checklist was used to classify individuals with positive results as ADHD positive, but also to quantify the levels of present symptomatology, considering the total score obtained in the entire questionnaire (between 0 and 72). This tool has been substantially used in clinical and research settings, including in prisons (Young et al., 2015).
Procedure
The investigators visited the correctional facility on a weekly basis and interviewed each prisoner to obtain data for the first part of the questionnaire. Participants filled the self-report questionnaires on their own, but at least one investigator was always present to clarify some items and assure that all were filled to avoid missing data.
Statistical Analysis
The statistical analysis was conducted using Stata Statistical Software: Release 13 (College Station, TX, USA) with the significance level set at p < .05. After assessing the prevalence rate of positive screenings for ADHD, we dichotomized our sample into “ADHD” and “non-ADHD’ depending on whether they exceeded the symptom count threshold. Descriptive statistics were used to describe demographic characteristics of both groups, along with total scores of psychopathology and psychopathic traits.
The normality of total (and subcategory, when applicable) BSI and TriPM distributions in both groups was determined with Kolmogorov–Smirnov test.
We used Student t test to compare both groups in respect to age at first conviction and criminal recidivism.
Pairwise correlations were established between ASRS-V1.1 total scores and BSI total and subcategory scores, in both groups, to check for any associations. Correlations were considered strong if r > |.7|, medium if |.5| < r < |.7| and weak if r < |.5|.
A logistic regression model was used to compare Psychopathy Scores between the ADHD and non-ADHD groups. Age, substance abuse, and adverse childhood experiences were used as covariates in the model.
Results
The final penitentiary sample consisted of 101 male prisoners (23.82% of the total prison population). Current imprisonment was mainly due to crime against property other than robbery (41.6%), homicide (26.7%), crime against physical integrity (15.8%), drug dealing (7.9%), and robbery (4%). The remainder four individuals had committed crimes against society (n = 3) and one had committed tax fraud.
Among the prison inmates, 17 (16.8%) screened positive for ADHD (Table 1) with three having mostly inattentive symptoms, three reporting predominantly hyperactive/impulsive symptoms, and 11 having combined symptoms. ADHD-positive inmates had higher levels of general psychopathology and psychopathic traits being significantly younger than non-ADHD counterparts by the time of their first contact with the judicial system (Table 1). The proportion of individuals with at least one previous detention was similar in ADHD and non-ADHD individuals (p = .186).
Demographic characteristics, psychopathology, and psychopathic traits scores in the ADHD and non-ADHD groups (n = 101).
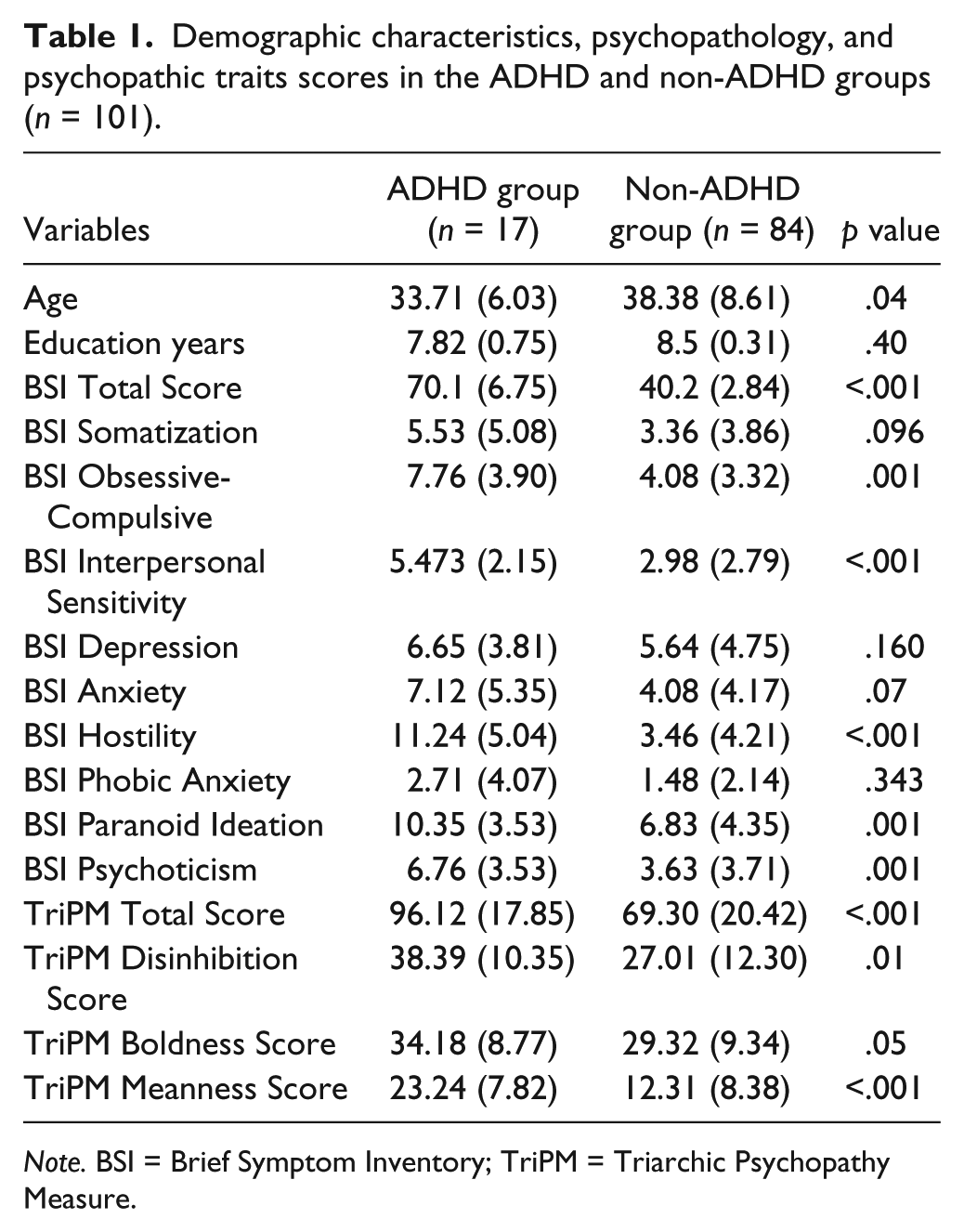
Note. BSI = Brief Symptom Inventory; TriPM = Triarchic Psychopathy Measure.
The correlation between ASRS total score and the BSI total score was weak, but a medium correlation was found between BSI total score and ASRS hyperactivity/impulsivity (ASRS HI) score (Table 2). BSI hostility scores correlated with ASRS total score (r = .64), and this was explained by an association with ASRS HI score (r = .69). Interpersonal sensitivity, anxiety, and psychoticism were mildly correlated with the ASRS total and HI scores (Table 2).
Pairwise Correlations (Pearson’s r) Between Total and Subdomain Scores of the ASRS v1.1 and BSI Total and Subscores (n = 101).

Note. ASRS v1.1 = Adult ADHD Self-Report Scale Version 1.1; BSI = Brief Symptom Inventory; ASRS HI ASRS hyperactivity/impulsivity symptoms; ASRS A ASRS attention symptoms
Medium correlations |r| > .5.
In the logistic regression model, a higher burden of psychopathic traits was an independent predictor of being ADHD positive (OR = 1.07, p = .002) with age, substance abuse, and early childhood adversities as covariates (Table 3). This was observed for disinhibition and meanness subscales (OR = 1.07, p = .037; OR = 1.13, p = .001, respectively). When including all subscales in the model, only meanness remained significant (OR = 1.11, p = .013) as shown in Table 4.
Logistic Regression Model to Estimate the Probability of Being ADHD Positive, Based on Age, Psychopathic Traits, Substance Abuse and Early Childhood Adversity (n = 101).
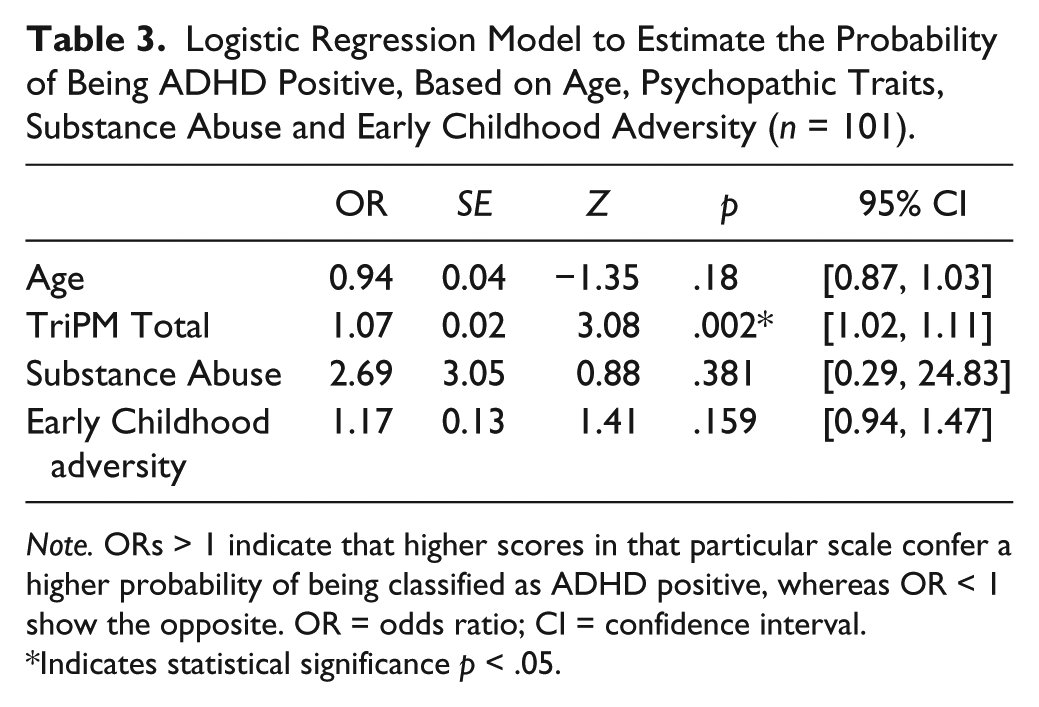
Note. ORs > 1 indicate that higher scores in that particular scale confer a higher probability of being classified as ADHD positive, whereas OR < 1 show the opposite. OR = odds ratio; CI = confidence interval.
Indicates statistical significance p < .05.
Logistic Regression Model to Estimate the Probability of Being ADHD Positive, Considering Previous Covariates and Psychopathic Subdomains (n = 101).
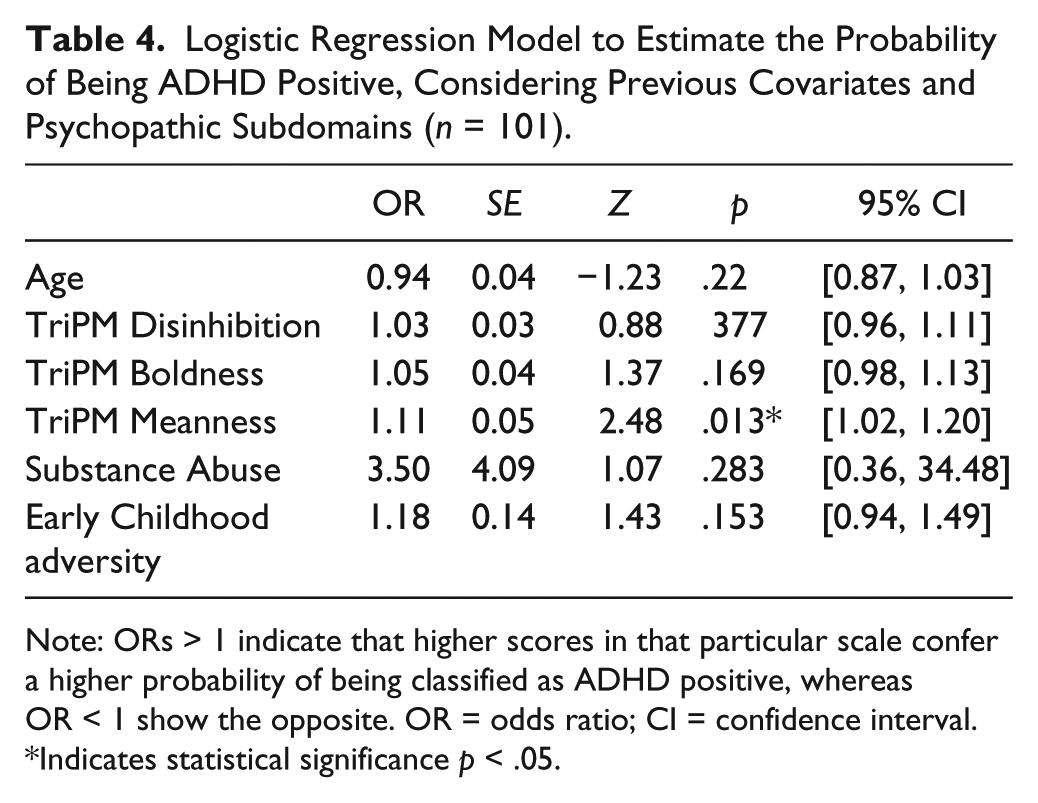
Note: ORs > 1 indicate that higher scores in that particular scale confer a higher probability of being classified as ADHD positive, whereas OR < 1 show the opposite. OR = odds ratio; CI = confidence interval.
Indicates statistical significance p < .05.
Discussion
In the present study, 17% of the prisoner sample screened positive for ADHD which is in line with the estimated proportion among offenders (Moore et al., 2013; Usher et al., 2013; Young et al., 2009) and considerably higher than estimates in the general population (3.4%, Fayyad et al., 2007).
While two previous studies showed a predominance of inattentive symptoms (Konstenius et al., 2015; Moore et al., 2013), the majority of the individuals who screened positive for ADHD in our sample had both symptoms of hyperactivity/impulsivity and inattention. It has been well established that the prevalence and severity of hyperactive and impulsive symptoms decrease from childhood to adulthood (Mick, Faraone, & Biederman, 2004). Nevertheless, considering that the presence of hyperactivity/impulsivity (but not inattention) is an independent contributor to criminal behavior (Babinski, Hartsough, & Lambert, 1999), a higher prevalence of these symptoms in forensic settings is expected.
Also in agreement with previous reports, individuals who screened positive for ADHD in our sample were significantly younger when first contacting with the criminal system (De Sanctis, Nomura, Newcorn, & Halperin, 2012; Silva, Colvin, Glauert, & Bower, 2014). This suggests that strategies aimed to reduce ADHD-related criminal behavior should be implemented before adulthood. Although at the descriptive level the results of the current study point to higher recidivism rates among ADHD individuals, these differences were not significant. Our findings are similar to those of Grieger and Hosser (2012) who found that ADHD was not a predictor of recidivism among offenders, although offenders diagnosed with ADHD were found to reoffend sooner after release.
Our ADHD group showed a higher burden of general psychopathology, particularly due to higher scores in the Obsessive-Compulsion, Paranoia, Interpersonal Sensitivity, Hostility, and Psychoticism subdomains. Although we expected depression/anxiety to be more prevalent in ADHD inmates, as these are common comorbidities of this disorder, hyperactivity and impulsivity symptoms, which were highly prevalent in our sample, are more frequently associated with externalizing patterns of psychopathology rather than internalizing disorders, such as depression or somatization (Murphy, Barkley, & Bush, 2002), which could explain our results.
When using ASRS as a trait measure, we found that higher ADHD symptoms correlated with higher levels of psychopathology, with hyperactivity/impulsivity symptoms showing the biggest correlation. Studies previously conducted in adult outpatients with ADHD have shown that psychiatric comorbidities are more frequent among hyperactive and combined subtypes (Piñeiro-Dieguez, Balanzá-Martínez, García, Soler-López, & The CAT Study Group, 2014; Wilens et al., 2009). Furthermore, other studies have shown that hyperactivity/impulsivity symptoms are associated with greater social maladjustment than inattention symptoms (Murphy et al., 2002). As so, the available evidence suggests that hyperactivity/impulsivity symptoms may act as independent risk factors for comorbid psychiatric disorders in ADHD patients.
Although higher scores in all variables (i.e., psychopathic traits, early childhood adversities, and substance abuse) resulted in an increased likelihood of being classified as ADHD positive, psychopathic traits emerged as the only independent factor in the logistic regression model. This is in accordance with prior findings from other researchers (Eisenbarth et al., 2008; Retz, Boureghda, Retz-Junginger, Philipp-Wiegmann, & Rösler, 2013; Soderstrom, Nilsson, Sjodin, Carlstedt, & Forsman, 2005), revealing a significant association between ADHD symptoms and psychopathic features. Fowler and colleagues previously reported higher total psychopathy and emotional dysfunction scores in ADHD adolescents; however, none scored in the clinical range of psychopathy (Fowler et al., 2009). Eisenbarth et al. (2008) reported higher behavioral features of psychopathy in adult ADHD patients, despite less emotional features, such as cold heartedness and stress immunity, compared with controls. A correlation between PCL screening version and ADHD-ASRS mean scores was reported in another study with incarcerated male individuals, but with no association between diagnostic items of ADHD with those of psychopathy (Retz & Rösler, 2010).
When analyzing the different subscales of the Triarchic Psychopathic Measure separately, both disinhibition and meanness were significantly associated with ADHD symptoms. However, when using all three subscales together in the model, only meanness remained significant. Meanness entails deficient empathy, disdain for and lack of close attachments with others, rebelliousness, excitement seeking, exploitativeness, and empowerment through cruelty (Patrick, 2010) and has been related to PCL-R affective and interpersonal symptoms (Venables, Hall, & Patrick, 2014). In contrast to our findings, the few published studies addressing the relation between psychopathic traits and ADHD found that only the behavioral (but not the emotional) features of psychopathy were affected in ADHD (Eisenbarth et al., 2008; Retz et al., 2013; Soderstrom et al., 2005). Importantly, all previous conducted studies used different instruments (PCL-R or the Psychopathic Personality Inventory [PPI]) to measure psychopathic traits.
One possible explanation for our results is that individuals with ADHD symptoms, being more impulsive and lacking inhibitory control, can be more prone to admit cruelty acts and/or feelings when compared with individuals without ADHD symptoms. In addition, a higher burden of ADHD symptoms can be associated with a more pronounced development of newly acquired psychopathic features through deviancy training during the stay in a high-security facility. Furthermore, ADHD is known to be associated with social cognition impairments involving emotional face and prosody perception not only in children but also in adult patients (Bora & Pantelis, 2016). While most studies have evaluated children or adolescents so far, there is evidence for theory of mind deficits and reduced empathy in ADHD (Schwenck et al., 2011). Social cognition impairments could justify higher scores in the meanness subscale in relation to low affective and/or cognitive empathy and further limitations reading social cues, like sadness or fear that can modulate aggressive behavior. This is further corroborated by neuroimaging studies in ADHD patients showing functional and/or morphometric abnormalities not only in the orbitofrontal cortex (OFC) but also in other brain regions implicated in social cognition and emotional processing such as caudate nucleus, the ventral striatum, and the cerebellum (Soliva et al., 2009; Ibáñez et al., 2011).
As psychopathy usually presents with impulsive, irresponsible, frequent, and severe antisocial behavior, including proactive violence (Swogger, Walsh, Lejuez, & Kosson, 2010) and most psychopaths also meet the diagnostic criteria for ASPD (a frequent comorbid diagnosis in ADHD), ADHD and psychopathy share some similarities in respect to impulsive traits and deviant behavior. As so, because we used a screening tool and not a diagnostic procedure, there might be an overlap between self-reported psychopathic and ADHD symptoms, increasing the likelihood that prisoners with high levels of psychopathic traits present a positive screening for ADHD. Indeed, there is growing evidence suggesting that both conditions share neurobiological changes in similar brain networks. Thus, higher psychopathic scores have been associated with impaired deactivation of the default mode network (DMN) during an attentional task (Freeman et al., 2015). This relation was particularly significant between PCL-R Factor 1 scores and dysfunction of the DMN in the medial prefrontal area suggesting that attentional deficits can underlie the affective and interpersonal deficits with increased self-focus manifested by patients with psychopathy. Higher psychopathic traits among prison inmates were also related to functional connectivity abnormalities between the anterior cingulate cortex (ACC) and posterior cingulate cortex, underlying deficits in internal monitoring of cognitive and attentional processes (Juárez, Kiehll, & Calhoun, 2013). These connectivity impairments were also significantly correlated with PCL Factor 1, revealing that DMN dysfunction could be implied in callous unemotional traits associated with psychopathy. Similarly, abnormal connectivity patterns between the DMN and ACC have also been found in adults with ADHD (Castellanos et al., 2008), and the dorsal ACC is the most consistently reported region to be dysfunctional in ADHD (Bush, 2011), with a crucial physiological role in attention, cognition, and emotion processing.
Overall, we found that the burden of psychopathic traits in incarcerated individuals was independently associated with ADHD symptoms suggesting a phenotypic overlap between both conditions. Emerging evidence raises the hypothesis that ADHD and psychopathy might share a common neurobiological background. Therefore, although our results were obtained in a cross-sectional design and cannot be used to determine causality, the possible relation between ADHD symptoms and psychopathic traits can explain behaviors associated with criminal offenses such as impulsive acts, breaking rules, interpersonal problems, criminal actions, substance abuse, and sensation seeking.
Further understanding of the role of psychopathic traits in ADHD could lead to more adequate treatment protocols of this disorder among criminal populations.
Limitations
A number of limitations from the current study should be considered when interpreting the results. We did not include all prison inmates in the study, and this can be a source of selection bias. However, as volunteer prisoners interviewed for the study were randomly selected, it is not likely that included participants had different characteristics from those who were not interviewed.
Also, as we only used a screening measure and not a diagnostic procedure, the reported ADHD symptoms can be a manifestation of a diversity of conditions such as substance abuse disorders, head trauma, or other mental disorders, commonly associated with inattention and hyperactivity features.
The data collected came from prisoners and was based entirely on self-report. As official criminal records or collateral reports were not available, the information on criminal history could not be corroborated, and this may have introduced some recall bias.
Comorbidities like CD and ASPD could not be excluded. These conditions have been consistently associated with criminality and can modulate the relationship between ADHD and offending. Consequently, future studies of this type should also measure these variables and attempt differentiation of their effects.
Due to time and cost constrains, we were unable to measure the IQ in our sample. Therefore, despite all included individuals had at least 4 years of education, we could not rule out the participation of individuals with learning disabilities and this may have influenced some responses.
Finally, we only used male participants; therefore, the effect of gender on psychopathy and offending in individuals with ADHD symptoms was not assessed in the present study.
Conclusions
In agreement with previous reports, the present study indicates that there is a significantly higher prevalence of ADHD symptoms among offenders that can have a modulating effect on the course of delinquent behaviors. This highlights the need for instructing professionals in the criminal justice system to be aware of common behavioral patterns of ADHD offenders, recognize these individuals, and refer them to mental health services, for proper diagnosis and intervention. Recognizing that some of the offender’s behavior may be related to the symptoms of ADHD will help in providing better recommendations at all stages of the justice process, providing a better experience for these offenders in the criminal justice system and possibly also a better reintegration to the community setting
Another important finding of our study is the cross-sectional association between ADHD symptoms and psychopathic traits. Although it is hard to disentangle the unique contribution of ADHD to this complex relationship, our results are an additional piece of evidence contributing to clarify the determinants of criminal behavior in individuals with ADHD symptoms. Some of the limitations of the current study could be addressed in the future with a baseline assessment before the occurrence of criminal behaviors; a comprehensive characterization of participants with clinical, psychological, and social features; and a longitudinal follow-up assessing clinical, social, and criminal outcomes.
Overall, our findings enhance the importance of health and criminal justice entities working together, providing healthier communities, more efficient services, and better social outcomes, by establishing ADHD diagnosis and treatment protocols among criminal offenders. It is important to highlight that these findings were obtained in a specific underrepresented population and should not be generalized to other groups, including individuals with ADHD symptoms in other settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.