
Abstract
Introduction
Attention-Deficit/Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder typified by symptoms of inattention, hyperactivity, and impulsivity. The estimated prevalence among school-aged children in North America is between 6% and 7% (American Psychiatric Association [APA], 2013; Thomas, Sanders, Doust, Beller, & Glasziou, 2015). Children with ADHD experience a range of comorbid psychiatric conditions and learning difficulties (Pliszka, 2000), perhaps the most prevalent being oppositional defiant disorder (ODD). ODD, typified by patterns of rule defiance, anger, and behavioral difficulties, is estimated to affect between 30% and 50% of the childhood ADHD population (August, Realmuto, Joyce, & Hektner, 1999).
The etiology of ADHD is largely due to genetic inheritance (Castellanos, Sonuga-Barke, Milham, & Tannock, 2006; Faraone & Biederman, 2000), although this does not diminish the role environmental factors, such as parenting, play in shaping the child’s overall functioning (Nigg, 2006). Genetic aberrations contribute to neurological impairments with the executive functions (EFs; Tannock, 2003), which are believed to underpin many of the behavioral symptoms associated with ADHD (Doyle, 2006). EFs are defined as interrelated higher order cognitive processes that underlie self-regulation and effortful goal-directed behavior (Pennington, Bennetto, McAleer, & Roberts, 1996). EFs are considered essential for adaptive human behavior as they are primarily engaged to help individuals interpret problems or complex situations via effortful thought and purposeful responses to novel situations (Jurado & Rosselli, 2007; Mahone et al., 2002; Pennington & Ozonoff, 1996).
Most contemporary theories proffer a multiple etiologic pathway for ADHD and consider difficulties with EF performance, referred to here as executive function difficulties (EFDs), as important impairments that underpin this neurodevelopmental disorder (Barkley, 2006; Castellanos & Tannock, 2002; Nigg, Willcutt, Doyle, & Sonuga-Barke, 2005; Sonuga-Barke, 2002, 2005). These theories have been substantiated by a large meta-analytic study (see Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005) that revealed EFDs to be “neither necessary nor sufficient to cause all cases of ADHD” but “appear to be one important component of the complex neuropsychology of ADHD” (p. 1336). Calls to have an “executive deficit” ADHD subtype considered for the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013; Nigg et al., 2005) were not warranted as testing procedures for EFDs lack sufficient sensitivity and specificity to serve as diagnostic indices (APA, 2013; Schreiber, Possin, Girard, & Rey-Casserly, 2014; Stefanatos & Baron, 2007). However, the DSM-5 has recognized the importance of neurological and neurocognitive processes by recategorizing ADHD as a neurodevelopmental disorder. Furthermore, the DSM-5 has recognized EFDs as a possible associated feature of the diagnosis by stating that individuals with ADHD “may exhibit cognitive problems on tests of attention, executive function or memory” (APA, 2013, p. 61).
Due to global EFDs being rare in the childhood ADHD population (Anderson, 2002), most research models apply a subcomponents approach that attempts to isolate children’s specific EF abilities in areas such as inhibition, working memory (WM), planning, shift, and emotional control. Research shows that children diagnosed with ADHD have pronounced difficulties in the area of inhibition control (Barnett, Maruff, & Vance, 2009; Mullane & Corkum, 2007; Willcutt et al., 2005) and WM (Barnett et al., 2009; Martinussen et al., 2005; Wahlstedt et al., 2009; Willcutt et al., 2005). There is also a modest amount of research linking ADHD with planning deficits (Barnett et al., 2009; Willcutt et al., 2005), and EFDs with cognitive and/or behavioral shift (Corbett, Constantine, Hendren, Rocke, & Ozonoff, 2009; Mullane & Corkum, 2007). Children with ADHD also experience significantly greater deficits with emotional regulation relative to nonclinical groups (Walcott & Landau, 2004), but this difference is limited to the ADHD Combined presentation (ADHD-C; Maedgen & Carlson, 2000). Research that specifically employs the Behavioral Rating Inventory of Executive Function (BRIEF), an assessment of EF, also concludes that children with ADHD are likely to experience a range of impairments with their EFs (Davidson, Cherry, & Corkum, 2016; Gioia, Isquith, Retzlaff, & Espy, 2002; Jarratt, Riccio, & Siekierski, 2005; Lyons Usher, Leon, Stanford, Holmbeck, & Bryant, 2016; Mares, McLuckie, Schwartz, & Saini, 2007; McCandles & O’Laughlin, 2007).
Negative outcomes and functional impairments associated with ADHD are not isolated to the child, as parents of these children experience significantly higher levels of parenting stress in comparison with parents of the non-ADHD populations (Theule, Wiener, Tannock, & Jenkins, 2013). The symptoms of ADHD, and more specifically ADHD with comorbid ODD (ADHD/ODD), are most likely the principal sources of parenting stress for this population (Anastopoulos, Guevremont, Shelton, & DuPaul, 1992; Harrison & Sofronoff, 2002; Podolski & Nigg, 2001). In fact, parents raising children with ADHD may be among the most stressed caregivers of any children’s special needs population (Abidin, 1995; Theule et al., 2013), due in part to a heavy burden of daily hassles (Crnic, Gaze, & Hoffman, 2005).
The extant research literature shows a strong relationship between ADHD and EFDs (Willcutt et al., 2005), as well as a strong relationship between childhood ADHD and parenting stress (Theule et al., 2013). However, there is a paucity of research examining any associations between EFDs and parenting stress for caregivers raising children with ADHD (Graziano, McNamara, Geffken, & Reid, 2011; Hutchison, Feder, Abar, & Winsler, 2016; Joyner, Silver, & Stavinoha, 2009). The current study extends this body of research by first using the full version of the parenting stress index (PSI) that allows for the examination of the relationship between EFDs and stress specific to child characteristics (PSI Child Domain [CD]) and parent-specific characteristic (i.e., PSI Parent Domain [PD]), and second by employing both the parent- and teacher-reported BRIEFs, which enables us to examine how EFDs in the home and/or school environments may relate to parenting stress. Specifically, we examine whether parent- and teacher-reported EFDs predict increased levels of parenting stress. Furthermore, if parent- and/or teacher-reported EFDs predict increased levels of parenting stress, we seek to understand, via a subcomponents model, which specific EFDs best predict this parenting stress. We hypothesize that elevated levels of parent-reported and teacher-reported EFDs are associated with elevated parenting stress specific to the parenting role (i.e., CD parenting stress), and that EFDs with WM and emotional regulation will best predict elevated stress.
Method
Sample
To achieve the objectives of this study, an ethics-approved secondary data analysis was conducted on a cross-section of parent- and teacher-completed psychiatric assessment materials for children diagnosed with various types of ADHD at a hospital-based outpatient children’s mental health program specializing in childhood ADHD, located in Toronto, Ontario, Canada. For a further description of this clinical setting and primary purpose for data collection, refer to McLuckie (2011). For this specific study, children and their families were eligible for inclusion if they met the following inclusion criteria: (a) children were 5- to 12-year-olds, conforming to the age parameters of the psychological measures; (b) measures were complete and deemed valid by the staff psychologist; (c) the child received a primary diagnosis of ADHD from a staff psychiatrist; and (d) to ensure independence of observations, only one child per family was included in the secondary dataset, with the specific child included being determined by whichever child was first to engage in clinical services and who met additional inclusion criteria. In relation to the inclusion criteria, it is important to note that the sample was diagnosed via the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000) as this was the most current diagnostic criterion available at the time of data collection. Although the diagnostic criteria for ADHD have experienced minor modifications with the DSM-5 (APA, 2013), these changes would not likely influence the diagnostic outcomes of the present sample. The terminologies for the disorder have also undergone minor changes from the DSM-IV-TR with the subtypes of ADHD, Predominately Inattentive Type (ADHD-I), and ADHD Combined Type (ADHD-C) being referred to now in DSM-5 as specifiers including ADHD-Predominately Inattentive Presentation and ADHD Combined Presentation (APA, 2000, 2013).
The final sample (n = 243) consisted of assessment information pertaining to 169 boys and 74 girls ranging in age from 5 to 12 years (M = 8.4; SD = 1.96). Forty-two (boys = 21, girls = 21) were diagnosed with ADHD-I, 141 (boys = 99, girls = 42) diagnosed with ADHD-C, and 60 (boys = 49, girls = 11) diagnosed with ADHD with comorbid ODD (ADHD/ODD). The majority (95%) of the ADHD/ODD group were children with a diagnosis of ADHD-C (boys = 47, girls = 10), with three diagnosed with ADHD-I (boys = 2, girls = 1).
The majority (67%) of children resided in families headed by two parents, 26% resided in one-parent-headed families, and 7% did not report their family structures. Mothers completed the majority of assessment measures (89%, n = 216), with fathers completing the remainder. Mothers ranged in age from 21 to 56 years (M = 37.82; SD = 7.27), and fathers (11%, n = 27) were 30 to 62 years of age (M = 41.23; SD = 8.32). Twenty-one mothers and six fathers did not report their age.
Measures
Parenting stress
The Parenting Stress Inventory (PSI–Long Form: Abidin, 1995) was used to measure parenting stress. This parent-completed questionnaire is valid for parents of children aged 1 month to 12 years (Abidin, 1995) and is one of the most commonly used measures of parenting stress (Fischer, 1990). The PSI’s 101 items are presented in multiple-choice format, or as 5-point Likert-type scale questions (“strongly agree” to “strongly disagree”) across 13 subscales organized, via factor analysis, into two domains: the CD and the PD. The CD measures stress associated with the child’s characteristics and comprises six subscales, including Adaptability (11 items), Demandingness (nine items), Mood (five items), Distractibility/Hyperactivity (nine items), Acceptability (seven items), and Reinforces Parent (six items). The PD measures stress related to a parent’s personality and potential psychopathology, as well as situational stressors in the parent’s life. The PD comprises seven subscales, including Depression (nine items), Attachment (seven items), Role Restriction (seven items), Competence (13 items), Isolation (six items), Spouse (seven items), and Health (five items). The CD and PD are combined to form the total stress index, which provides an overall index of parenting stress.
The PSI demonstrates good reliability and validity (Abidin, 1995; Anastopoulos et al., 1992; Fischer, 1990). Cronbach’s alpha scores of reliability range between .70 and .83 for the CD subscales, and between .70 and .84 for PD subscales. Test–retest reliability is strong for the CD (r = .91) and total stress index (r = .96) across a 1- to 3-month period, while it is lower for the PD (r = .63). The PSI also demonstrates good discriminant validity with the ability to distinguish families with a special needs child from nonclinical controls (Abidin, 1995; Beck, Young, & Tarnowski, 1990).
EFDs
Parent and teacher versions of the Behavior Rating Inventory of Executive Function (BRIEF: Gioia, Isquith, Guy, & Kenworthy, 2000) were used to measure the child’s EFDs in the home and school settings. Valid for children aged 5 to 18 years, these standardized observational measures are completed independently by teachers and parents. Each item is rated on a 3-point scale (“never,” “sometimes,” “often”). Factor analysis used during the development of the BRIEF guided the organization of the measure into eight correlated but nonoverlapping subscales (Donders, 2002; Gioia et al., 2000) congruent with accepted subcomponent models of EFs (Pennington et al., 1996; Pennington & Ozonoff, 1996). The subscales include Inhibit (10 items), Shift (eight parent or 10 teacher items), and Emotional Control (10 parent or nine teacher items) with each producing raw and T scores that are also combined into a composite score referred to as the behavioral regulation index (BRI). The remaining subscales, Initiate (eight parent or seven teacher items), WM (10 items), Plan/Organize (12 parent or 10 teacher items), Organization of Materials (six parent or seven teacher items), and Monitor (eight parent or 10 teacher items), also render raw and T scores that when combined represent the meta-cognitive index (MI). The BRI and MI are combined to form the Global Executive Composite (GEC), which provides an overall index of EFDs for the child. The T scores exceeding 65 “should be considered as having potential clinical significance” with higher scores “indicating greater degrees of executive dysfunction” (Gioia et al., 2000, p. 14).
The BRIEF has demonstrated good internal reliability with Cronbach’s alpha coefficients ranging between .82 and .98 for the various subscales (Gioia et al., 2000). Interrater reliability between parents and teachers was moderate (Blake-Greenberg, 2003; Gioia et al., 2000). However, rather than indicate bias, dissimilar parent and teacher ratings likely reflect different situational demands placed on children at home and school (Mares et al., 2007), and/or highlight the BRIEF’s ecological validity and utility to assess children’s EF in real-world settings, such as the home and school (Denckla, 2002; Jurado & Rosselli, 2007; Riccio, Homack, Jarratt, & Wolfe, 2006). The BRIEF also demonstrates good discriminant validity by distinguishing ADHD populations from controls (Gioia et al., 2000; McCandles & O’Laughlin, 2007) and discriminating between ADHD subtypes (Riccio et al., 2006).
Data Analysis
All analyses were conducted using SPSS version 24. Hierarchical linear regression (HLR) was employed to determine whether elevated levels of childhood EFDs reported by parents and/or teachers predict increased levels of parenting stress. Specifically, HLR was used to regress the CD scores of the PSI (criterion variable) onto parent- and teacher-reported scores of the BRIEF MI and BRI composite scales (predictor variables), which were entered as four separate blocks. To determine which subcomponent EFDs best predict increased parenting stress, a series of follow-up HLR procedures were conducted, replacing the composite scores (e.g., parent BRIEF BRI) with corresponding BRIEF subscales (e.g., Shift, Inhibit, and Emotional Control). Nonsignificant subscales (p > .05) in each step of the HLR were removed allowing only significant subscales to remain in the final HLR procedure. The above processes were then repeated interchanging the CD with the PD as the criterion variable.
Results
Parent and teacher scores on the BRIEF are presented in Table 1, and scores on the PSI are presented in Table 2. In relation to examining the PSI CD scores as the criterion variable, the results reveal that the linear combination of childhood EFDs measured by the teacher BRIEF BRI, and parent BRIEF MI and BRI scales accounts for 49% of the variance in child-related parenting stress. On their own, scores from the MI scale of the teacher BRIEF were not a significant predictor of CD parenting stress, and teacher BRIEF BRI scores account for a small, albeit statistically significant amount (3%) of the variance. Parent-reported scores on the BRIEF MI and BRI scales account for 17% and 29% of the variance in child-related parenting stress, respectively. In relation to examining PSI PD scores as the criterion variable, the results show that the linear combination of parent BRIEF BRI and MI scores accounts for 13.5% of the variance in PD parting stress. On their own, teacher-completed BRIEF MI and BRI scores were not significant predictors. Scores on the parent BRIEF MI account for approximately 4% of the variance, and parent BRIEF BRI scores account for 9.5% of the variance in PSI PD scores (see Table 3).
Executive Function Difficulties Measured by the Parent and Teacher BRIEF.
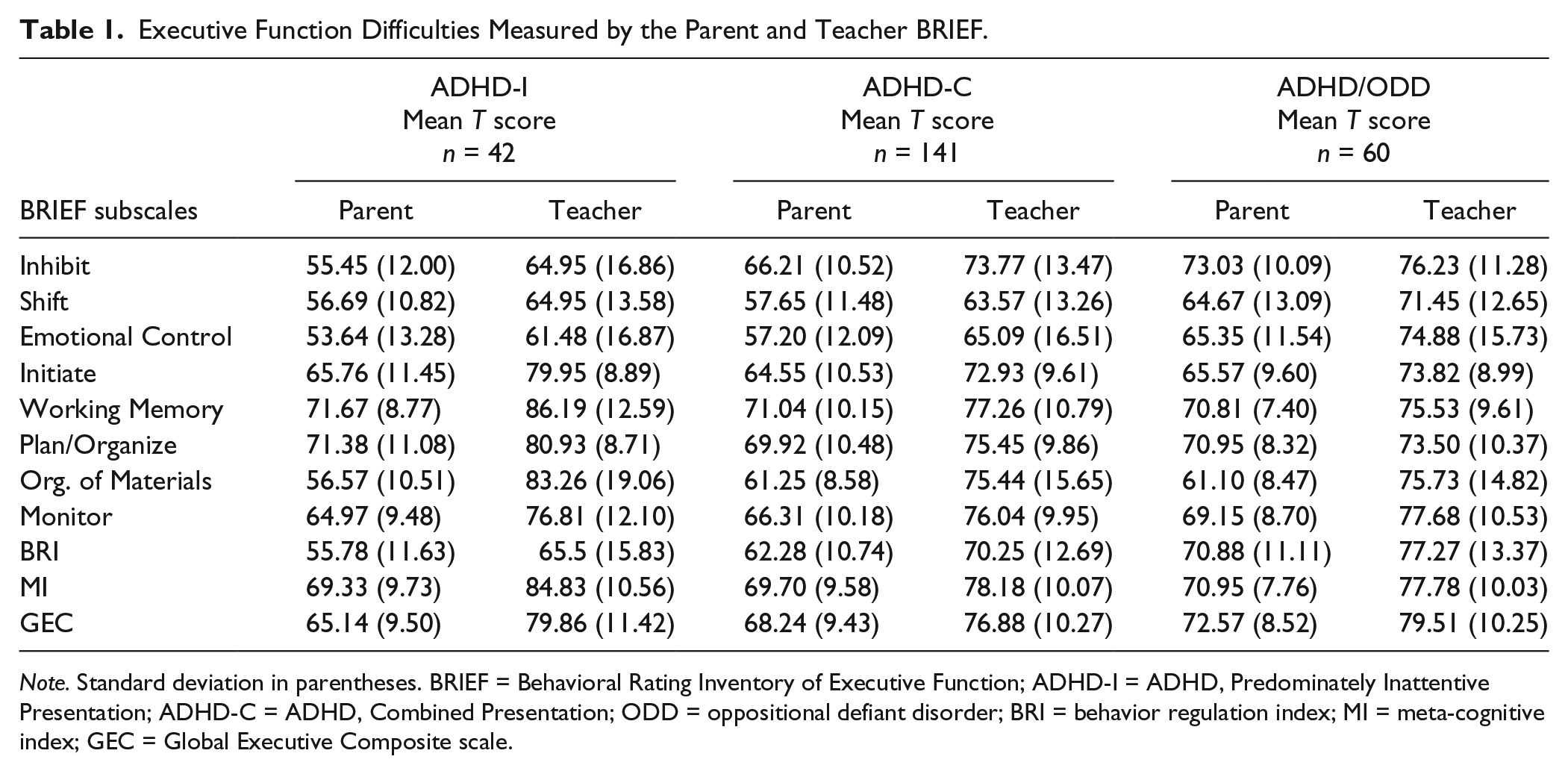
Note. Standard deviation in parentheses. BRIEF = Behavioral Rating Inventory of Executive Function; ADHD-I = ADHD, Predominately Inattentive Presentation; ADHD-C = ADHD, Combined Presentation; ODD = oppositional defiant disorder; BRI = behavior regulation index; MI = meta-cognitive index; GEC = Global Executive Composite scale.
Average Levels of Parenting Stress for ADHD Diagnostic Categories.

Note. Standard deviations are included in the parentheses. PSI = parenting stress index; ADHD-I = ADHD, Predominately Inattentive Presentation; ADHD-C = ADHD, Combined Presentation; ODD = oppositional defiant disorder.
For increased precision, the PSI offers age norms for the composite scales Child Domain and Parent Domain (Abidin, 1995).
Hierarchical Linear Regression for EFDs Predicting Scores on PSI (Criterion Variable).

Note. EFDs = executive function difficulties; PSI = parenting stress index; BRIEF = Behavioral Rating Inventory of Executive Function; MI = meta-cognitive index; BRI = behavior regulation index.
In relation to the EF subcomponents predicting CD parenting stress, the results indicate that teacher-reported EFDs specific to emotional control, along with parent-reported EFDs with initiate, monitor, inhibit, shift, and emotional control, account for 51% of variance in CD parenting stress levels. These results reveal that these subcomponents are the key predictors of CD parenting stress accounting for approximately half of the variance in child-related parenting stress within the current sample. In relation to subcomponents predicting PD PSI scores, parent-reported EFDs with inhibit and shift were significant predictors explaining 8.5% of the variance in these scores (see Table 4).
Hierarchical Linear Regression for EFDs Subcomponents Predicting Scores on PSI (Criterion Variable).
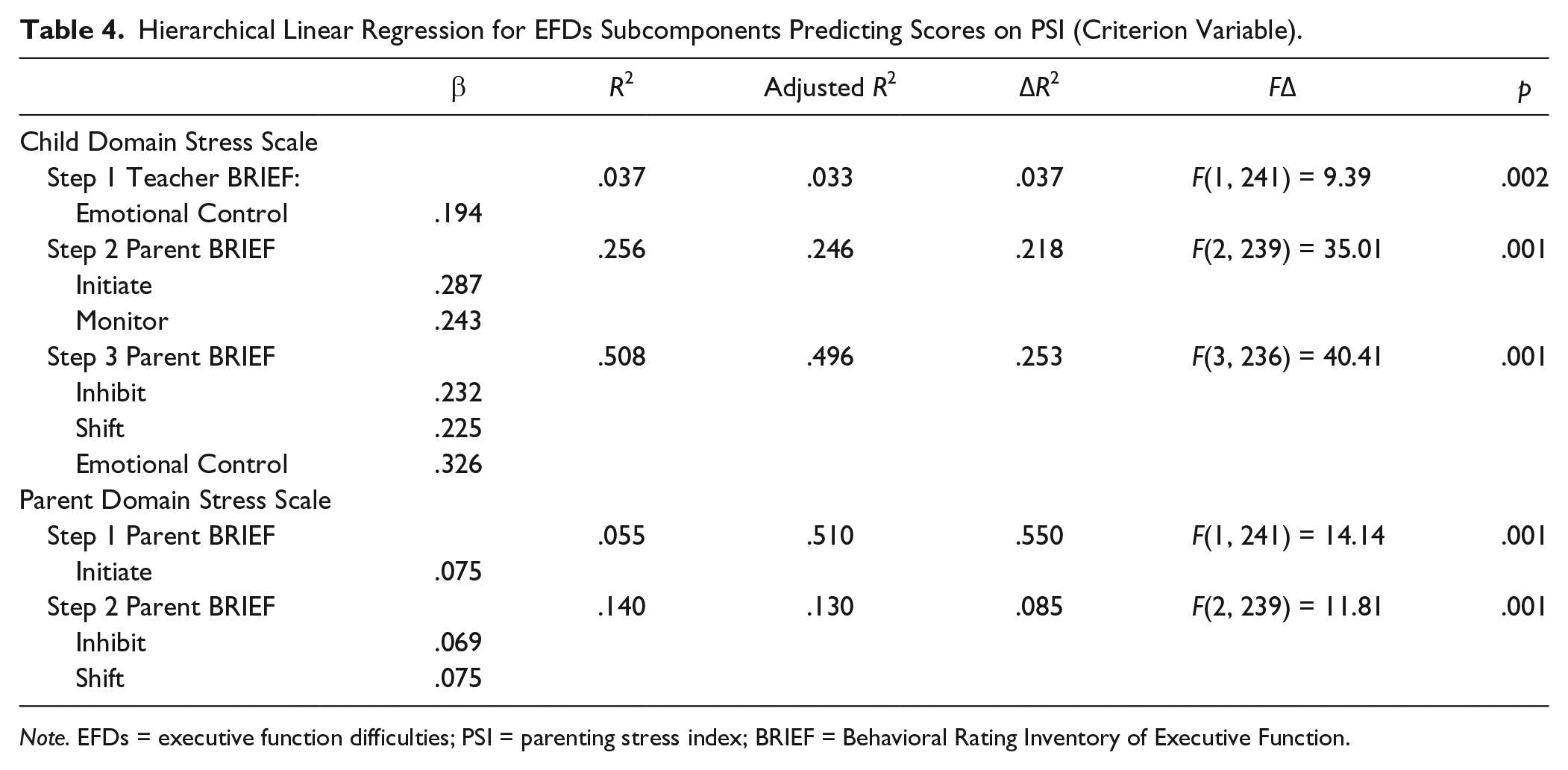
Note. EFDs = executive function difficulties; PSI = parenting stress index; BRIEF = Behavioral Rating Inventory of Executive Function.
Discussion
The present study demonstrates an association between parent-reported EFDs and parenting stress for children diagnosed with ADHD and ADHD/ODD. These findings are consistent with prior research demonstrating an association between parent-reported EFDs and parenting stress for caregivers raising children with ADHD (Graziano et al., 2011; Hutchison et al., 2016; Joyner et al., 2009). The current study extends this body of research by employing both the parent- and teacher-reported BRIEFs. To date, there are no known studies that have used both the parent- and teacher-reported BRIEFs to explore the relationship between EFDs and parenting stress for children diagnosed with ADHD.
Results of the HLR analyses reveal elevated scores on the parent BRIEF BRI to be the strongest predictor of elevated levels of CD parenting stress. Elevated scores on the parent BRIEF MI subscale and elevated scores on the teacher BRIEF BRI subscale also predict elevated levels of CD parenting stress. However, both these predictor variables explain a much smaller portion of the occurrence of CD parenting stress. The combined influence of these three variables accounts for approximately half of the variance in CD parenting stress, meaning that almost half the reason parents are stressed can be explained by the presence of child EFDs. The elevated parenting stress related to the child may be best explained by parent’s difficulties in relation to their child’s EFDs with shift, inhibit, and in particular emotional control. This finding is consistent with parallel research that shows parents raising children with ADHD are particularly stressed by their children’s oppositionality, defiance, and aggression (Anastopoulos et al., 1992; Harrison & Sofronoff, 2002; Podolski & Nigg, 2001; Ross, Blanc, McNeil, Eyberg, & Hembree-Kigin, 1998) associated with, or underpinned by, EFDs with emotional control/regulation (Garcia-Sancho, Salguero, & Fernandez-Berrocal, 2014; Roll, Koglin, & Petermann, 2012; Schoorl, van Rijn, de Wied, van Goozen, & Swaab, 2016).
Consistent with Lazarus’s (1966) definition of psychological stress, Abidin (1995) conceptualized parenting stress as the negative mental response of a parent created by a mismatch between the perceived demands of parenting and the perceived availability of parental resources to meet these demands. Applying Abidin’s (1995) model of parenting stress to interpret these findings, the behavioral difficulties related to emotional control, inhibition, and shift may impose demands on parents and/or the parenting role that likely exceed their perceived parenting resources and parenting abilities (i.e., their ability to cope). The behaviors of children with ADHD are the most probable source of parenting stress (Mash & Johnston, 1990). However, the current findings reveal that it is not just any behavioral difficulties associated with ADHD that contribute to high levels of parenting stress but rather those behavioral difficulties specifically associated with inhibition, regulating emotionality and shifting between tasks. Children with ADHD who are prone to emotionally volatile, unrestrained, unpredictable, and/or rigid behavior patterns were experienced as highly stressful to their parents.
In addition to EFDs with emotional and/or behavioral control, the current results revealed that parent-reported EFDs in the meta-cognitive domain account for a meaningful amount of variance (17%) in child-related parenting stress. In terms of the subcomponents driving this association, difficulties with initiation and monitor were associated with parenting stress, whereas difficulties with WM and planning were not. These findings are somewhat perplexing considering that the research literature implicates WM and planning as central impairments to ADHD (Barnett et al., 2009; Brocki, Eninger, Thorell, & Bohlin, 2010; Castellanos et al., 2006; Martinussen et al., 2005; McCandles & O’Laughlin, 2007; Re, De Franchis, & Cornoldi, 2010), which is strongly associated with parenting stress (Theule et al., 2013). Further obfuscating our interpretation is the fact that difficulties with WM (M = 71; SD = 9.31) and planning (M = 70; SD = 10.13) were the most pronounced EFDs reported by parents across all three ADHD grouping variables in our results (see Table 1), a finding consistent with other research employing the BRIEF (Gioia, Isquith, Retzlaff, & Espy, 2002; McCandles & O’Laughlin, 2007; Riccio et al., 2006). The overall means for WM and Plan/Organize were the only two subscales to significantly exceed a T score of 65 (i.e., the clinical cut-point for the BRIEF) using a Bonferroni-corrected one-sample t test—WM: t(239) = 6.14, p < .0001, and plan/organize: t(239) = 5.4 p < .0001.
These findings may suggest that despite being visible to parents, behaviors related to WM and planning difficulties may not always translate into parenting stress. It seems that there is a distinct difference between parents being aware of their children’s EFDs with WM and planning, and parents being stressed out by these EFDs. This finding underscores a major tenet of leading models of parenting stress (Abidin, 1990; Mash & Johnston, 1990) that parenting stress is likely mediated by the appraised mismatch between demands and available resources, and not just the presence/occurrence of potentially noxious stimuli within the environment. Simply stated, parents may not appraise their child’s difficulties with WM and/or planning to exceed their parenting abilities and/or resources, and therefore, they are coping adequately and/or remaining resilient to this potential stress factor.
Theories of appraisals/attributions offered by Weiner (1985) and Lazarus (1966; Lazarus & Folkman, 1984) may provide a further lens through which to interpret these findings. Weiner (1985) theorizes that increased helping behaviors should be expected in situations where the difficulty is attributed to factors beyond the individual’s control. In relation to attributions within ADHD populations, research shows that inattentive symptoms are considered to be outside of the child’s control (Freeman, Johnston, & Barth, 1997). As theory and research have established a strong link between meta-cognitive EFDs and inattentive symptoms (Castellanos et al., 2006; Willcutt et al., 2005), it is reasonable to surmise that parents also consider EFDs with WM and planning to lie outside of the child’s willful effortful control. Our findings showing parent-reported difficulties with initiate and monitor to be significant predictors of CD parenting stress still beg interpretation. The answer may lie, in part, with Gioia and colleagues’ (2000) description of the behaviors captured by these two BRIEF subscales. The authors suggest that difficulties with initiate encapsulate problems getting started on activities such as household chores, homework, or getting off to school in the morning. These childhood behaviors often coincide with the need for parents to engage in “extensive prompts or cues in order to begin a task or activity” (Gioia et al., 2000, p. 18). Furthermore, the Monitor subscale of the BRIEF captures the child’s abilities in areas such as accuracy and completion rates for homework and household chores, as well as self-awareness of their impact on others (e.g., failing to effectively self-monitor their noise level while the caregiver is on the phone or attempting to nap). Different from coping with WM and planning difficulties, behaviors associated with initiation and monitoring may have more potential to contribute to stressful interactions between the parent and child, best described by Lazarus and Cohen (1977) as daily hassles.
Daily hassles have been theorized to play an important role in the occurrence and maintenance of parenting stress levels (Mash & Johnston, 1990). A credible explanation for why meta-cognitive EFDs, such as initiate and monitor, predict heightened CD parenting stress may be found by conceptualizing initiate and monitor as being related to daily hassles.
Research in this area reveals that daily hassles for parents are not merely related to the child’s ADHD symptomatology but are also affiliated with the overall practice of providing specialized care for their child which can meaningfully contribute to parenting stress levels (Cronin, 2004; Johnson & Reader, 2002; Theule et al., 2013). For parents of children with initiation difficulties and/or self-monitoring difficulties, engaging in the daily grind of “getting kids going to school” or the need for a constant shepherding role to “keep kids on task” may lead to the heightened stress reported in the current study linked to EFDs with initiate and monitor. This interpretation is congruent with findings from qualitative research by Firmin and Phillips (2009) who noted that parents are quite stressed with getting their children going in the morning (e.g., preparing children for school) and helping keep their children at tasks and focused on things such as homework. Viewing difficulties with initiation and monitoring as contributing to daily hassles may also explain why research finds mothers, and not fathers, experience elevated parenting stress in relation to inattentive symptoms (Podolski & Nigg, 2001), as mothers are shown to bear more responsibility for the hassles of day-to-day child care duties (Lee, Vernon-Feagans, Vazquez, & Kolak, 2003). In sum, findings from parent reports show that in addition to CD parenting stress being associated with EFDs pertaining to behavioral/emotional regulation, EFDs with initiation and monitoring are associated with CD parenting stress likely due to the role that these meta-cognitive EFDs play in the daily hassles experienced by parents.
A novel contribution of the current research is the finding that teacher-reported EFDs with behavioral/emotional regulation only account for a small portion (less than 3%) of the variance in CD parenting stress within the current sample. The strength of this relationship may be further reduced by the presence of error variance within this step of the HLR. This suggests that parents may not experience significant levels of CD parenting stress in relation to the behaviors displayed within the school environment. These findings were somewhat surprising, in that they contradict previous research showing that parenting stress levels are significantly higher for parents whose children display difficulties in multiple settings (e.g., school and home) related to ADHD (Anthony et al., 2005; Beck et al., 1990).
Interestingly, these findings show that teachers reported all of the EF subcomponents measured by the BRIEF (i.e., WM, planning, initiate, plan/organize, organization of materials, and monitor) to be elevated, exceeding the concern for EFDs expressed by parents. Therefore, teachers in the current study were well aware of their students’ EFDs; however, these concerns did not correspond with an increase in parent’s stress. From a theoretical perspective, these findings suggest that children’s difficulties in school related to EFDs, as noted by teachers, pose fewer demands on parent’s resources and/or coping capacities, and therefore they do not experience school-based EFDs as stressful. These findings can also be interpreted to mean that teaching staff are coping effectively with meta-cognitive EFDs, and therefore involve parents less in relation to problems with WM and planning than they might in regard to EFDs with emotional regulation. In essence, teachers may act as a coping resource for parents by addressing the difficulties related to children’s meta-cognitive challenges, thereby buffering any parenting stress.
Teachers may, however, perceive some children’s EFDs as too demanding or beyond their resources/capacities to address with their teaching roles. Findings from the current study show that teacher-reported EFDs with emotional regulation are significantly related to CD parenting stress, albeit at low levels. This can be interpreted to mean that teaching staff are less able or less willing to tolerate the child’s display of emotionality and behavioral issues without involving parents than they might in relation to children’s difficulties with meta-cognitive-related EFs. As noted in research by Riley and colleagues (2006), demands on parents have grown in relation to supporting the unique needs of ADHD children to include organizing and managing school-based interventions. To fulfill the role of “good parent,” parents of children with special needs, such as ADHD, often perceive that they must actively engage the school system in meeting the child’s needs (McKeever & Miller, 2004). Parents of children with ADHD may feel indirectly responsible for the child’s success in the school (Bendell, Stone, Field, & Goldstein, 1989), and even link their sense of pride and competency in their parenting role to these successes or failures (Cronin, 2004). As a result, parents may be more likely to engage in problem-focused coping procedures which see them advocating on their child’s behalf to improve the child’s learning and social experience.
Conclusion
The current study was undertaken to address the gap in knowledge as to whether parent- and/or teacher-reported EFDs are associated with elevated levels of parenting stress (CD and PD). By utilizing parent-reported and teacher-reported measures of EFDs, rather than measures of ADHD behavioral symptoms, this study offered an alternate route to explore how children’s symptoms of ADHD and ADHD/ODD might influence levels of CD parenting stress. Mining more deeply into the possible sources of parenting stress associated with childhood ADHD, such as EFDs, will provide a more precise picture of why parents feel highly stressed raising children with ADHD. Gaining such insight is vital to the design or redesign of programming and services for this population. The current study produced a number of important findings that have numerous implications for mental health professionals working with young people and parents affected by EFDs, ADHD, and parenting stress.
The present study represents a newly developing area of research within the field of parenting stress. It utilized a sizable cross-sectional sample of children attending a clinic specializing in ADHD assessment. By garnering input from both parents and teachers, we were able to ensure the veracity of the ADHD diagnosis, and identify a range of EFDs displayed by children in both the home and school environments, as well as using the full version of the PSI.
Another strength is the study’s theoretical grounding, theoretical transparency, and theoretical congruence. Congruence between theory and measures was achieved through the congruence between Abidin’s model of parenting stress that draws upon Lazarus’s (1966) Interactional Model of Stress (IMS) (Burke & Abidin, 1978, as cited in Abidin, 1995) and the PSI. This congruence allowed for an interpretation of the findings, such as parental coping in a manner that was well grounded in the theory and literature base of accepted models of psychological stress.
Despite these strengths, the present study is not without limitations. First, the generalizability of the results of the current study may be limited due to the clinical nature of the sample and inclusion criteria used, restricting participation to children diagnosed with ADHD and their parents. Second, due to parameters of the secondary dataset utilized for the current study, our insights into the demographics of our sample are somewhat limited, and we were unable to speak about factors such as family socioeconomic status, parent’s sexual orientation, possibility of children being adopted, parental mental health, or other such factors that could inform the generalizability of findings. Third, the levels of parenting stress were provided by parents who have accessed a psychiatric assessment for their child, suggesting the possibility that these parents may be coping less well and experiencing more stress than other parents who did not pursue this type of assessment. The fact that they pursued an assessment with a psychiatrist suggests that these parents may have a particular view of their child’s learning/behavioral difficulties, which can influence how they cope with parenting stress (i.e., problem-focused coping). However, the findings of this study are consistent with other clinical samples, and may be generalizable and highly relevant to children with ADHD and their parents.
Footnotes
Acknowledgements
The authors would like to thank the staff and physicians of The Scarborough Hospital, as well as the families who participated in this research, without whom this study would not have been possible. They also acknowledge the late Dr. Atilia Turgay, MD, whose commitment to clinical excellence and his passion for helping young people with ADHD and their families inspired the current research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the lead author’s doctoral fellowship from the Social Sciences and Humanities Research Council of Canada as an important support that enabled this research.