
Abstract
Mild traumatic brain injury (mTBI) makes up the overwhelming majority of traumatic brain injuries (TBIs), with an estimated 600 cases per 100,000 person-years worldwide (Cassidy et al., 2004). Interest in this injury has heightened as mTBI effects people’s ability to work and go to school. The mTBI symptoms are usually of immediate or near immediate onset but can also be delayed. Although most people recover within 4 to 12 weeks, a sizable minority of patients fail to have full resolution of symptoms and remain impaired for a longer period of time.
Among the most common deficits that individuals with mTBI experience are cognitive difficulties including difficulties in attention, concentration, and distractibility. Because the symptoms are reminiscent of those associated with ADHD, stimulants could have a role in alleviating them. Although there is a body of literature supporting the use of stimulants in the context of moderate and severe TBI targeting attention, arousal, and processing speed (Giacino et al., 2012; Gualtieri & Evans, 1988; Hornstein, Lennihan, Seliger, Lichtman, & Schroeder, 1996; Whyte et al., 2004; Whyte, Vaccaro, Grieb-Neff, & Hart, 2002), much less is known about the role of stimulants in the management of mTBI, the most common form of TBI.
The main aim of this review was to evaluate the body of knowledge on the use of stimulants in mTBI across all ages. To this, we conducted a systematic review of the available published literature on stimulants in the treatment of patients with mTBI to determine (a) what symptoms were targeted, (b) stimulant type and dosing regimen, (c) study design, (d) study size, (e) study outcomes, (f) safety and tolerability, and (g) whether a diagnosis of ADHD was considered.
Method
Search Strategy and Selection Criteria
We conducted a literature search using Ovidmedline and PubMed, pscyhINFO through Ovid, CINAHL, Embase, and Cochrane. We compiled broad search terms to capture the study population, mTBI, and treatment, stimulants. Search algorithm included (brain concussion OR brain injury OR head injury) AND (amantadine OR amphetamine OR methylphenidate OR Ritalin OR Adderall OR dextroamphetamine OR Provigil OR central nervous system stimulant OR stimulant). The search yielded 1,508 articles. Three additional publications, which were obtained from reviewing references from other articles, met the search criteria. After deletion of duplicates, the remaining article abstracts were reviewed and those deemed relevant to the study topic underwent full text review.
Although we initially intended to restrict the review to studies that used stimulants in mTBI to target ADHD or deficits in attention, because of the limited number of articles available, we expanded the inclusion criteria to include articles on the use of stimulants in mTBI for any diagnosis or target. Thus, the following inclusion criteria were applied: (a) original research, (b) articles written in English, and (c) differentiation of mTBI from other severity of brain injury. Articles were excluded if they failed to (a) present original research, (b) use a stimulant medication, (c) distinguish mTBI from other severity of brain injury, or if (d) studies were not in humans. In studies that included a combination of mTBI and other TBI severity, studies were included if the number of mTBI patients in the cohort was known and the diagnostic criteria used to distinguish mTBI was defined. Studies of mixed severity that did not report the number of mTBI patients were only included if individual participant data, such as neuroimaging findings, length of posttraumatic amnesia and loss of consciousness, and Glasgow Coma Scale (GCS), were available for the reviewers to distinguish mTBI. Diagnosis of mTBI was based on clinical interview, GCS 13 to 15, length of loss of consciousness less than 30 min, length of posttraumatic amnesia less than 24 hr, and absence of intracranial lesion on cerebral imaging. Presence of ADHD was based on Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria and was distinct from presence of attention deficit.
Data Extraction
The following variables were extracted: (a) number of participants with mTBI; (b) stimulant used, dosage, and duration; (c) presence of a control group; (d) study design; (e) treatment target; (f) assessment metrics; (g) diagnosis or history of ADHD; and (h) main outcomes.
Results
As shown in the PRISMA Figure 1, there were 1,511 articles that met the initial search criteria of mTBI and stimulants, 1,508 identified through database search and 3 through review of citations of other articles. After removal of duplicates, 798 articles were screened by title and abstract for relevance based on the aforementioned inclusion criteria with 63 articles meeting eligibility. Full text review of the 63 articles produced nine original research studies that evaluated the use of stimulants in participants with mTBI. Of the 54 articles excluded, the majority did not include original research or did not study mTBI, 18 and 20 studies, respectively, four studies used a medication other than a stimulant, six results were abstracts published from conference presentations and were not peer-reviewed publications, two studies surveyed physicians’ use of stimulants, three studies did not characterize TBI severity (mild, moderate, and severe or number of participants with each designation), and one study was not in human.
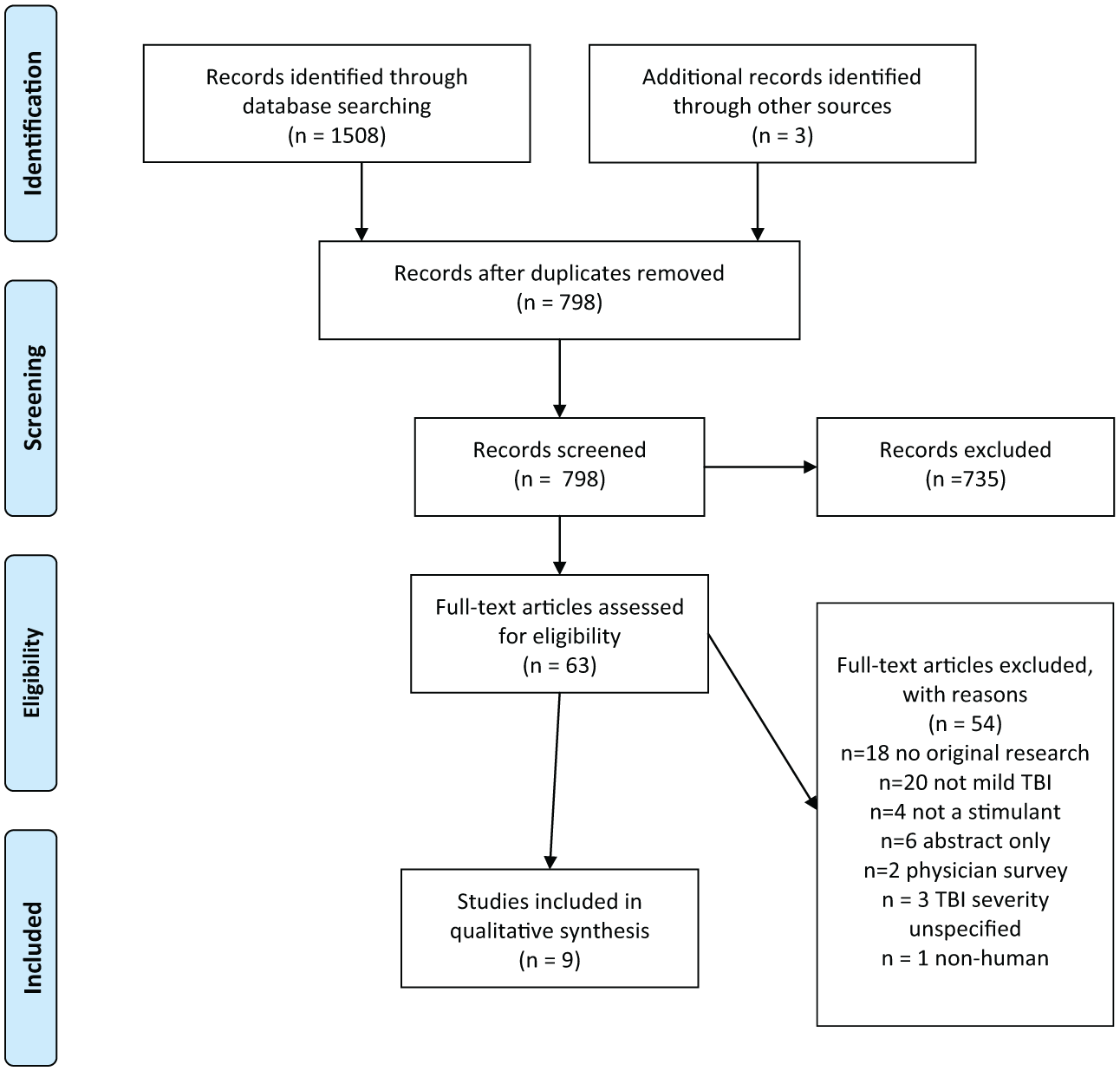
PRISMA 2009 flow diagram.
Of the nine studies included in this review, six studies were in adults and three studies in children below 18 including two studies which combined children and adolescents ages 6 to 16 and 5 to 14, and one study of only adolescence mean age 15.
As shown in Table 1, patient populations had substantial variability within and between studies in the characteristics of TBI severity, mechanism of injury, time since injury, age, and comorbid psychiatric and somatic conditions. Only two studies captured exclusively mTBI patients, one study evaluated adolescents (Reddy, Collins, Lovell, & Kontos, 2013) with sport concussion and the other adults of military and nonmilitary background with mTBI, posttraumatic stress disorder (PTSD), or concurrent diagnoses (McAllister et al., 2016). Seven studies had mixed populations of TBI combining mTBI with moderate and severe TBI (Beers, Skold, Dixon, & Adelson, 2005; Johansson, Wentzel, Andrell, Mannheimer, & Ronnback, 2015; Johansson et al., 2014; Johansson, Wentzel, Andrell, Ronnback, & Mannheimer, 2017; Kraus et al., 2005; Lee et al., 2005; Mahalick et al., 1998). Of these mixed severity studies, four studies (Johansson et al., 2015; Johansson et al., 2014; Johansson et al., 2017; Lee et al., 2005) included participants with mild and moderate TBI and three with mild, moderate, and severe TBI (Beers et al., 2005; Kraus et al., 2005; Mahalick et al., 1998).
Summary of the Literature on the Use of Stimulants for mTBI.
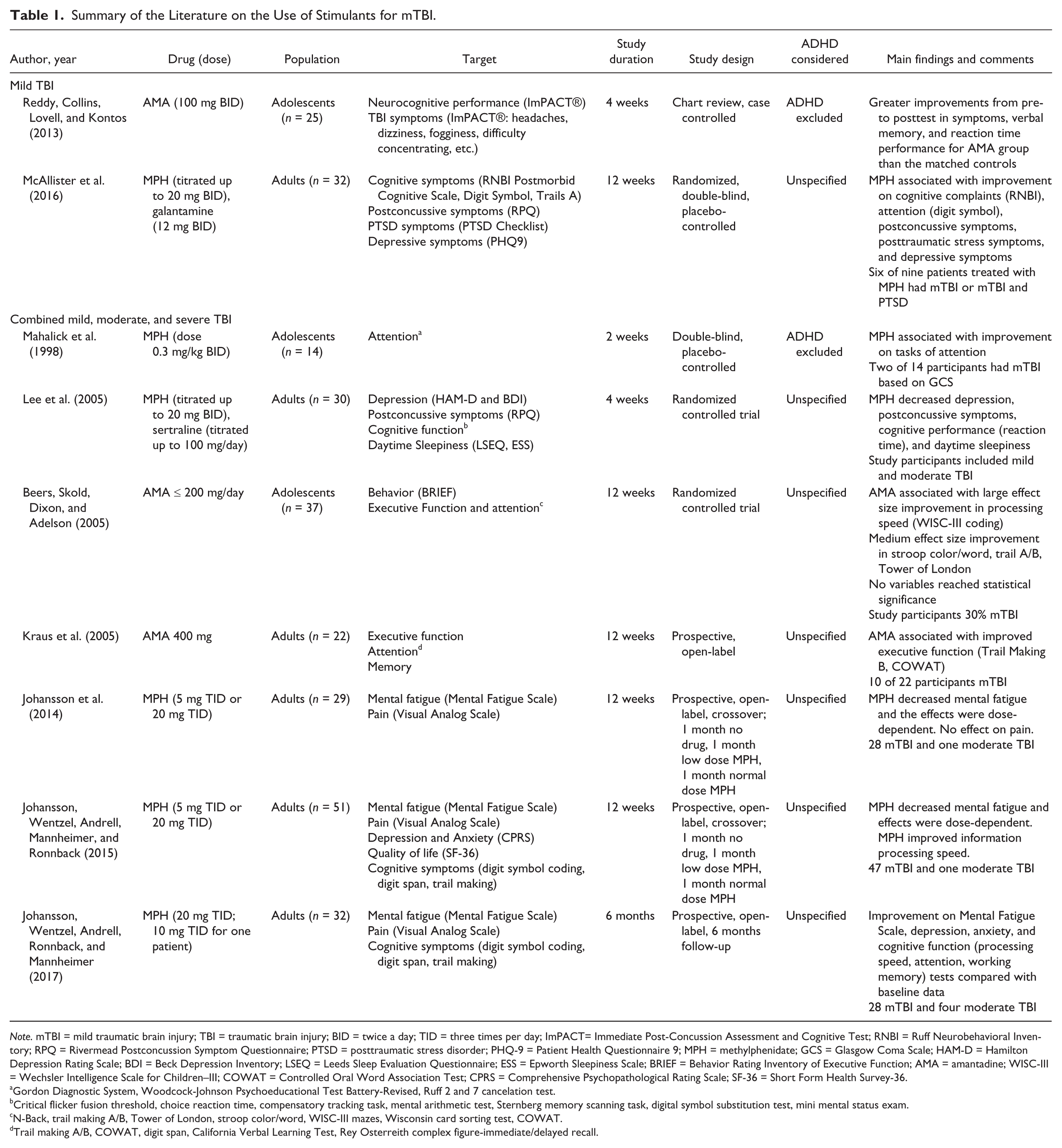
Note. mTBI = mild traumatic brain injury; TBI = traumatic brain injury; BID = twice a day; TID = three times per day; ImPACT= Immediate Post-Concussion Assessment and Cognitive Test; RNBI = Ruff Neurobehavioral Inventory; RPQ = Rivermead Postconcussion Symptom Questionnaire; PTSD = posttraumatic stress disorder; PHQ-9 = Patient Health Questionnaire 9; MPH = methylphenidate; GCS = Glasgow Coma Scale; HAM-D = Hamilton Depression Rating Scale; BDI = Beck Depression Inventory; LSEQ = Leeds Sleep Evaluation Questionnaire; ESS = Epworth Sleepiness Scale; BRIEF = Behavior Rating Inventory of Executive Function; AMA = amantadine; WISC-III = Wechsler Intelligence Scale for Children–III; COWAT = Controlled Oral Word Association Test; CPRS = Comprehensive Psychopathological Rating Scale; SF-36 = Short Form Health Survey-36.
Gordon Diagnostic System, Woodcock-Johnson Psychoeducational Test Battery-Revised, Ruff 2 and 7 cancelation test.
Critical flicker fusion threshold, choice reaction time, compensatory tracking task, mental arithmetic test, Sternberg memory scanning task, digital symbol substitution test, mini mental status exam.
N-Back, trail making A/B, Tower of London, stroop color/word, WISC-III mazes, Wisconsin card sorting test, COWAT.
Trail making A/B, COWAT, digit span, California Verbal Learning Test, Rey Osterreith complex figure-immediate/delayed recall.
What Symptoms Were Targeted by Stimulants?
Although all nine studies evaluated some components of cognitive function, only one study (Mahalick et al., 1998) evaluated attention deficits as its primary target. Five studies evaluated attention as a secondary outcome. Three studies (Lee et al., 2005; McAllister et al., 2016; Reddy et al., 2013) targeted cognitive, somatic, and emotional postconcussive symptoms using self-reported postconcussive symptoms scales. Other targets included symptoms of depression, anxiety, PTSD, fatigue, daytime sleepiness, pain, and quality of life.
What Stimulant Types and Dosing Regimens Were Used?
All studies used either immediate release methylphenidate (MPH) or amantadine. MPH was used in six studies, five studies in adults and one in children. Two studies in adults used a dose of 20 mg of immediate release MPH administered twice daily (Lee et al., 2005; McAllister et al., 2016). Three studies in adults, conducted by the same authors, compared two treatment regimens of MPH (5 mg 3 times daily and 20 mg 3 times daily; Johansson et al., 2015; Johansson et al., 2014; Johansson et al., 2017). One study in adolescents employed weight-based dosing of 0.3 mg/kg MPH twice daily (Mahalick et al., 1998). Duration of MPH treatment ranged from 2 to 24 weeks.
Three studies used amantadine, two studies in adolescents and one in adults. Adolescents received 100 mg twice daily (Reddy et al., 2013) or a weight-based dosing of 5 mg/kg/day with a maximum of 100 mg twice daily (Beers et al., 2005). Adults received amantadine 400 mg divided in three daily doses (Kraus et al., 2005). Medication treatment exposure ranged from 4 to 12 weeks.
Study Design
There were three randomized placebo-controlled trials of MPH. Lee et al. (2005) used a parallel group design to compare MPH, sertraline, and placebo over 4 weeks. McAllister et al. (2016) conducted a 12-weeks comparison study of MPH to placebo and galantamine in participants with mTBI, PTSD, or concurrent diagnoses. Mahalick and colleague (1998) used a crossover design, treating adolescents with MPH for 2 weeks and placebo for 2 weeks. One randomized controlled trial of amantadine in adolescents (Beers et al., 2005) compared pharmacotherapy to usual care.
Two studies (Johansson et al., 2015; Johansson et al., 2014) used an open-label crossover design with participants receiving low dose MPH (5 mg 3 times daily), high dose MPH (20 mg 3 times daily), and placebo each for 4 weeks. Participants responsive to stimulants were then enrolled in a prospective open-label 6-months follow-up study (Johansson et al., 2017). Kraus et al. (2005) conducted a prospective open-label trial of amantadine. Finally, there was one retrospective chart review (Reddy et al., 2013) of amantadine treatment in sport concussion with comparison to case matched controls.
Sample Size
Sample sizes across all studies were small ranging from 14 to 32 participants in total, including those randomized to nonstimulant treatment arms. Seven of nine studies captured heterogeneous TBI populations, which included all injury types and severity, not only mTBI. In total, mTBI represented approximately 75% (202/272) of TBI cases included in this review.
Study Outcomes
Three studies (Johansson et al., 2017; Mahalick et al., 1998; McAllister et al., 2016) found improvements in measures of attention using MPH. Seven studies evaluated processing speed of which three found significant improvement in processing speed with MPH (Johansson et al., 2015; Johansson et al., 2017; McAllister et al., 2016). Reaction time was significantly improved in one study using amantadine (Reddy et al., 2013) and in one with MPH (Lee et al., 2005). Five studies evaluated working memory with one study showing improvement with MPH (Johansson et al., 2015) and one with improvement in verbal memory with amantadine (Reddy et al., 2013). Three studies found improvement in cognitive and concussive symptoms, two with MPH and one with amantadine, by patient reported rating scales (ImPACT® symptom inventory and Rivermead Postconcussion symptoms scale) Lee et al., 2005; McAllister et al., 2016; Reddy et al., 2013).
Johansson and colleagues (Johansson et al., 2015; Johansson et al., 2014) found more significant improvement on self-report measures of fatigue using MPH 20 mg 3 times daily than with 5 mg 3 times daily. Improvement in fatigue was maintained in a 6-months prospective follow-up study of MPH responders (Johansson et al., 2017). Lee et al. (2005) found improvement in daytime sleepiness and ease of awakening in the morning in participants with mTBI and depression treated with MPH as compared with those treated with sertraline.
Three studies (McAllister et al., 2016; Lee et al., 2015; Johansson et al., 2017) reported improvement in depression symptoms with MPH. Assessment measures were heterogeneous, including the Comprehensive Psychopathological Rating Scale Depression Scale, Patient Health Questionaire-9, Hamilton Rating Scale for Depression, and the Beck Depression Inventory. One study (Johansson et al., 2017) also found improvement in anxiety measures in those taking MPH. Self-reported PTSD symptoms also improved in the MPH group as compared with controls in those with comorbid mTBI and PTSD (McAllister et al., 2016). The effect of MPH on pain was evaluated in three studies (Johansson et al., 2015; Johansson et al., 2014; Johansson et al., 2017) using MPH in participants recruited from a pain management program. There was no significant improvement in pain rating base upon the visual analog scale.
Safety and Tolerability
One study (Johansson et al., 2014) of adults had a primary aim of determining safety and tolerability of immediate release MPH. Mean heart rate was mildly increased from baseline in participants taking MPH 20 mg 3 times daily but remained within normal physiologic limits. Four participants had tachycardia on electrocardiography (ECG). Although mean blood pressure did not differ between MPH and control groups, hypertension was observed in three participants that had borderline hypertension prior to the study. Of these, one subject withdrew from the study due to hypertension refractory to treatment. In all, 86% of participants tolerated the treatment well; minor adverse effects included depressed mood, anxiety, and fatigue. More participants receiving MPH 20 mg 3 times daily reported minor adverse effects than did those receiving MPH 5 mg 3 times daily. No changes in body weight and no arrhythmias were observed.
McAllister et al. (2016) reported no serious adverse events in their study of MPH in participants with mTBI and PTSD. Although minor side effects occurred in 62.5% of participants, there was no difference in side effect reporting between active drug and placebo groups.
Kraus et al. (2005) reported one case of livedo reticularis, a vascular patterned mottling of the skin, in a subject receiving amantadine 400 mg daily. Minor side effects including nausea and lightheadedness were also reported. At a dose of 200 mg daily or less based on weight, Beers and colleagues (2005) reported no major adverse events. Overall, 47% of adolescent participants receiving treatment with amantadine reported minor side effects of nausea, sleep problems, vomiting, constipation, and rash in the first week of treatment, with a minority persisting into Weeks 2 through 6, and complete resolution of side effects Weeks 6 through 12.
Consideration of a Diagnosis of ADHD
There were no studies that evaluated the use of stimulants in participants with mTBI and ADHD. Although Mahalick et al. (1998) studied the effects of MPH on adolescents with deficits in task of attention and concentration, there is no mention if these participants met criteria for ADHD. Reddy et al. (2013) excluded participants with a history of ADHD. The remaining seven studies did not specify if premorbid or postinjury diagnoses of ADHD were considered in the study populations treated with stimulants.
Discussion
Our systematic review of the extant literature found very few studies that evaluated the effect of stimulants in the treatment of mTBI and its complications. In addition, the few studies available were small and included heterogeneous clinical targets, making it difficult to draw any meaningful conclusions.
This literature review found that immediate release MPH and amantadine were the only two stimulants used in the studies of participants with mTBI. No studies were identified that tested the efficacy and safety of amphetamines or sustained release formulations in patients with mTBI. Clearly, more and better powered studies are needed to further evaluate the efficacy and safety of stimulants in mTBI including short and long acting formulations of both MPH and amphetamine products. Future work should also use therapeutically acceptable daily doses such as those proven to be safe and effective in the management of ADHD. For example, greater improvement in fatigue and processing speed were seen in participants on higher dose MPH than in those receiving lower doses (Johansson et al., 2014). These findings suggest a possible dose-dependent effect and call for trials of higher dose MPH to maximize their potential benefit.
Although not a stimulant, amantadine seems to potentiate dopamine in the frontal-striatal networks through both direct action on dopamine receptors and its antagonism of N-methyl-D-aspartate (NMDA) giving it a stimulant-like effect. Amantadine has been used in a small number of studies of moderate and severe TBI at doses ranging from 200 to 400 mg/day (Giacino et al., 2012) with good tolerability but uncertain benefits. Similarly, there is insufficient studies in mTBI to determine its benefit.
Studies in this review use MPH and amantadine to target a broad range of symptoms including attention, processing speed, working memory, depression, anxiety, PTSD, fatigue, and pain. This broad range of targets is a stark contrast to the limited known indications for stimulants and amantadine. Although the symptoms of ADHD are the most well-known target for MPH, stimulants have also been used off-label to target cognitive symptoms, low energy, lethargy, and fatigue. Consistent with these clinical uses, some studies in this review found stimulants to be beneficial for inattention and deficits in processing speed. These findings are consistent with studies in moderate and severe TBI that show similar benefits (Gualtieri & Evans, 1988; Hornstein et al., 1996; Whyte et al., 1997; Whyte et al., 2004). Conversely, other measures of executive dysfunction were less responsive to stimulants. This is consistent with studies outside the TBI literature that show limited benefit of stimulants in executive function deficits (Biederman et al., 2011).
Symptoms of fatigue were responsive to MPH in three studies by Johansson (Johansson et al., 2015; Johansson et al., 2014; Johansson et al., 2017). These studies showed improvement in measures of fatigue at 12-weeks and 6-months follow-up. This outcome is supported by a body of literature in which stimulants have successfully targeted symptoms of fatigue in the geriatric population, cancer patients, and those with sleep disorders. Fatigue and psychomotor symptoms associated with depression have been targeted with stimulants and several studies support their use as adjunctive treatment in depression (Abbasowa, Kessing, & Vinberg, 2013; Corp, Gitlin, & Altshuler, 2014; Goss, Kaser, Costafreda, Sahakian, & Fu, 2013). Although a few studies targeted depressive symptoms in patients with mTBI (Lee et al., 2005), whether depression is a good target for stimulants in the setting on mTBI is very unclear.
McAllister et al. (2016) reported improvements in symptoms of PTSD with MPH in participants with mTBI. This finding is unusual as side effects of stimulants including anxiety, agitation, and nervousness overlap with symptoms of PTSD, and it would seem more likely that stimulants would exacerbate the PTSD condition. More work is certainly needed to clarify the role that stimulants may have in treating mTBI and concurrent PTSD.
Although amantadine has been used off-label to target parkinsonian symptoms and as an aid in the recovery of disordered consciousness after severe TBI, its role in the management of cognitive and noncognitive postconcussive symptoms remains uncertain. Anxiety, depression, and pain are unlikely to be good targets for the use of stimulants or amantadine.
Improvement in self-reported poorly defined postconcussive symptoms was seen in three studies using both MPH and amantadine. These inventories collect data on cognition, mood, sleep, and somatic symptoms that are not necessarily specific to mTBI. The energizing effect of stimulants may produce improvements in symptoms assessed by postconcussive symptom inventories without actually influencing recovery from mTBI.
Of the studies that used MPH to treat mTBI in this review, only one considered the presence of ADHD in their participants and it was used as exclusionary (Table 1). Nevertheless, in that study, Mahalick et al. (1998) found significant improvement in measures of attention with 2 weeks of treatment with low doses of MPH in adolescents with TBI excluding patients with a premorbid diagnosis of ADHD. Unfortunately, of the 14 participants in this study, only two met criteria for mTBI based on GCS while the remaining participants had moderate or severe brain injuries. Other studies have shown consistent and robust benefit of stimulants on attention and other cognitive function in more severely brain injured individuals (Whyte et al., 1997; Whyte et al., 2004; Whyte et al., 2002; Willmott & Ponsford, 2009).
The absence of attention to the presence or absence of ADHD in the studies that use stimulants to treat mTBI is surprising considering that a strong association between mTBI and ADHD has been documented (Biederman et al., 2015). The work on the association between mTBI and ADHD has demonstrated that ADHD is not only overrepresented in mTBI victims (Biederman et al., 2015) but also frequently preceded the mTBI. Clearly, more work is needed to characterize the clinical phenotype of ADHD and mTBI and further evaluate the role of stimulants in the management of ADHD symptoms in these participants.
Our findings need to be viewed in light of limitations in the source studies. The most significant limitation of the literature is the small number of available studies, the small sample sizes in the available studies, and the heterogeneity of targets chosen. Moreover, most studies included heterogeneous populations incorporating mild, moderate, and severe TBI patients or targeting mTBI patients with other diagnoses including, PTSD, depression, and pain. Only two studies exclusively targeted mTBI participants and, of these, only one study captured a relatively homogeneous population of mTBI participants without significant comorbidities in the form of youth sport concussion patients. All studies included in this review are of short duration of treatment and relied on doses of MPH that would be considered subtherapeutic for the treatment of ADHD.
Conclusion
Our literature review identified only a handful of small studies on the use of stimulants in mTBI relying on highly heterogeneous populations and targeting widely heterogeneous symptoms. Only three randomized controlled studies were identified that evaluated the use of stimulants in mTBI. These studies only evaluated low doses of MPH and, the dopaminergic medicine, amantadine. Studies of MPH targeted cognitive deficits, depression, and fatigue showing some improvement in these symptoms. The benefits of amantadine are very unclear. Although stimulants are most effective in the management of ADHD and ADHD has been shown to be overrepresented in mTBI, no study considered the diagnosis of ADHD either pre- or postconcussion. This state of affairs calls for more robust research in this clearly neglected area of clinical and scientific inquiry.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.