
Abstract
Introduction
ADHD is a neurodevelopmental disorder defined by attention dysregulation and/or high levels of activity and impulsivity (American Psychiatric Association [APA], 2013). The disorder is strongly heritable such that 70% to 80% of the variation in symptoms is explained by genetic factors, and families having one affected patient are likely to have others qualifying for the clinical diagnosis (Barkley, 2016). It typically emerges early in development (Arnett, MacDonald, & Pennington, 2013; Kieling et al., 2010; Lee, Sibley, & Epstein, 2016) and can be reliably diagnosed in children as young as 3 years (Egger, Kondo, & Angold, 2006; Lahey et al., 2004; Sterba, Egger, & Angold, 2007). Recently, the Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood (DC: 0-5) has introduced ADHD in the Axis I category of neurodevelopmental disorders and adapted it for the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) criteria (Zeanah et al., 2016). Several longitudinal studies have shown the stability of the diagnosis and demonstrated that symptoms of preschool ADHD persist into elementary school years, adolescence, and even adulthood (Barkley & Fisher, 2011; Law, Sideridis, Prock, & Sheridan, 2014; Riddle et al., 2013).
ADHD is the most common psychiatric disorder in childhood (Tandon & Pergjika, 2017). It has been associated with substantial negative impact on daily functioning and academic achievement (Polderman, Boomsma, Bartels, Verhulst, & Huizink, 2010), quality of life (Danckaerts et al., 2010), and significant levels of disability and impairment (Erskine et al., 2014; Lahey et al., 2016). Recently, preschool hyperactivity has been associated with long-term economic burden (Chorozoglou et al., 2015).
Preschool ADHD is frequently associated with other psychiatric and neurological disorders (Gillberg, 2010; Lavigne et al., 1996; Pliszka, 2000; Wakschlag & Keenan, 2001). Sixty to hundred percent of young children suffering from ADHD present with comorbid disorders (Gillberg et al., 2004; Posner et al., 2007; Wilens et al., 2002). The most common of them are oppositional defiant disorder (ODD), conduct disorder (CD), depression, anxiety, tics, sleep disorders, enuresis, encopresis (Angold, Costello, & Erkanli, 1999; Bauermeister et al., 2007; Biederman, Newcorn, & Sprich, 1991; Chronis-Tuscano et al., 2016; Harvey, Youngwirth, Thakar, & Errazuriz, 2009; Noordermeer et al., 2017; Owens, 2005), and other neurodevelopmental disorders (DuPaul, Gormley, & Laracy, 2013; Germanò, Gagliano, & Curatolo, 2010; McGrath et al., 2008; Rommelse et al., 2009; Sciberras et al., 2014; Tirosh & Cohen, 1998; Watemberg, Waiserberg, Zuk, Lerman, & Sagie, 2007; Willcutt & Pennington, 2000). Neurodevelopmental disorders often overlap, constitute amalgams of problems, and probably represent different aspects of the same underlying disorder (Reiersen, Constantino, Volk, & Todd, 2007). The number of children with developmental disorders, such as ADHD, has substantially increased, requiring more health and education services (Boyle et al., 2011).
Clinically referred preschool children with ADHD are considerably impaired in their daily functioning. They often exhibit disruptive behaviors that may lead to expulsion from day-care education setting, accidental injuries, and safety concerns (Lavigne et al., 1996). They often have significant social and learning difficulties that may lead to poor social adjustment and poor academic performance (Lahey et al., 2016). Preschool-onset ADHD appears to be a strong risk factor for persistent behavior, social and academic problems, substance abuse, and depression. So, early diagnosis and intervention are strongly recommended (Ozonoff, 2015).
According to previous studies, there are correlations between the severity of ADHD and parental ADHD (Agha, Zammit, Thapar, & Langley, 2013), the level of family support (Hurting et al., 2007), the socioeconomic status of the family (Russell, Ford, Rosenberg & Kelly, 2014), and the rate of comorbid disorders (Booster, DuPaul, Eiraldi, & Power, 2012).
The main objective of the current study was to assess demographic and clinical characteristics of a cohort of preschool-aged children diagnosed as suffering from ADHD, who were referred to the Preschoolers’ Department of our Mental Health Center between 2009 and 2012, in an attempt to identify risk factors that may lead to inpatient treatment. To this end, we compared variables that could discriminate preschoolers who were further referred to the day-care intensive unit (DCIU): inpatients, from those who were provided treatment as outpatients.
It was hypothesized that hospitalized children will present more severe ADHD, larger number of comorbid conditions, and more familial stressors.
Method
Participants
The cohort (N = 111; aged 3 to 6 years; girls: 25, boys: 86) included all the preschoolers who were referred to the Preschoolers’ Department during 2009-2012 and met Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000) criteria for ADHD.
The Preschoolers’ Department of our Mental Health Center provides assessment and diagnostic services and intervention programs for children between 3 and 6 years of age. Children referred to the department are subject to a diagnostic evaluation by a senior child psychiatrist. It includes a semi-structured interview of the child’s parents, a set of parents’ and teachers’ questionnaires, and a psychiatric examination. The overall functioning of the patient is estimated by the Clinical General Impression Severity Scale (CGI-S; Busner & Targum, 2007). Children with mild to moderate maladjustment and functional impairment, regardless of the specific psychopathology, are treated on an outpatient basis by a senior child psychiatrist or a child psychologist, whereas children with severe maladjustment are assigned to be treated by a multidisciplinary team at the DCIU of the department: hospitalized. The unit includes a therapeutic kindergarten. Each child is assigned to an individually tailored therapeutic-educational program for at least 3 months.
The rate of ADHD in our department in the last 10 years is between 84% and 89%, which is similar to the ADHD rate in a comparable setting (Wilens et al., 2002).
The cohort was divided according to the functioning level and adaptive capacities of the preschoolers, as assessed by the CGI-S, into severely impaired (CGI-S ≥ 5) children, who were referred to the DCIU (hospitalized participants group), and mild-moderately impaired (CGI-S ≤ 4) children, who were referred to outpatient intervention (outpatient participants group). Their demographics are summarized in Table 1.
Demographic Characteristics of the Study Sample (N = 111).
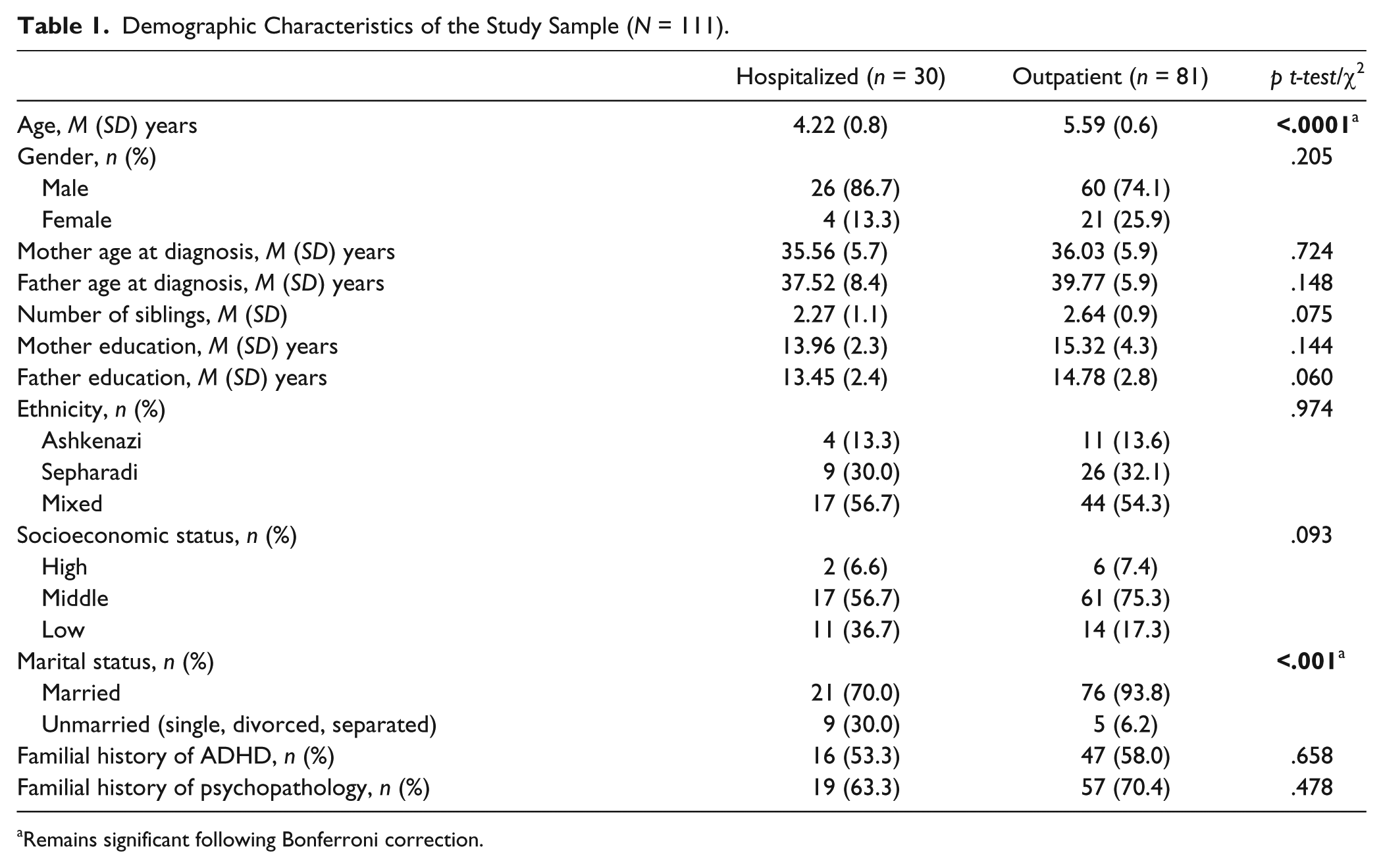
Remains significant following Bonferroni correction.
The study was approved by the Mental Health Center Review Board. Due to the chart review nature of the study, the need for obtaining informed consent from participants and their parents was waived.
Instruments and Procedure
The assessment and diagnosis of ADHD were conducted by a senior child psychiatrist. They were based on (a) a semi-structured interview, following the guidelines of the Kiddie Schedule for Affective Disorders and Schizophrenia–Present and Lifetime Version (K-SADS-PL) with adaptation to preschoolers; (b) interviews with the parents for a full developmental and familial history; (c) evaluation regarding each of the DSM-IV-TR (APA, 2000) criteria for ADHD; (d) the ADHD Rating Scale–IV (DuPaul, Power, Anastopoulos, & Reid, 1998) completed by the parents; (e) the Conners’ Rating Scales (CRS) completed by the parents (parent’s version) and by the teachers (teacher’s version; Conners, Sitarenios, Parker, & Epstein, 1998a, 1998b); (f) a clinical psychiatric assessment of the global functional status, the CGI-S, completed by the psychiatrist. The clinical characteristics of the participants are summarized in Table 2.
Clinical Characteristics of the Study Sample (N = 111).
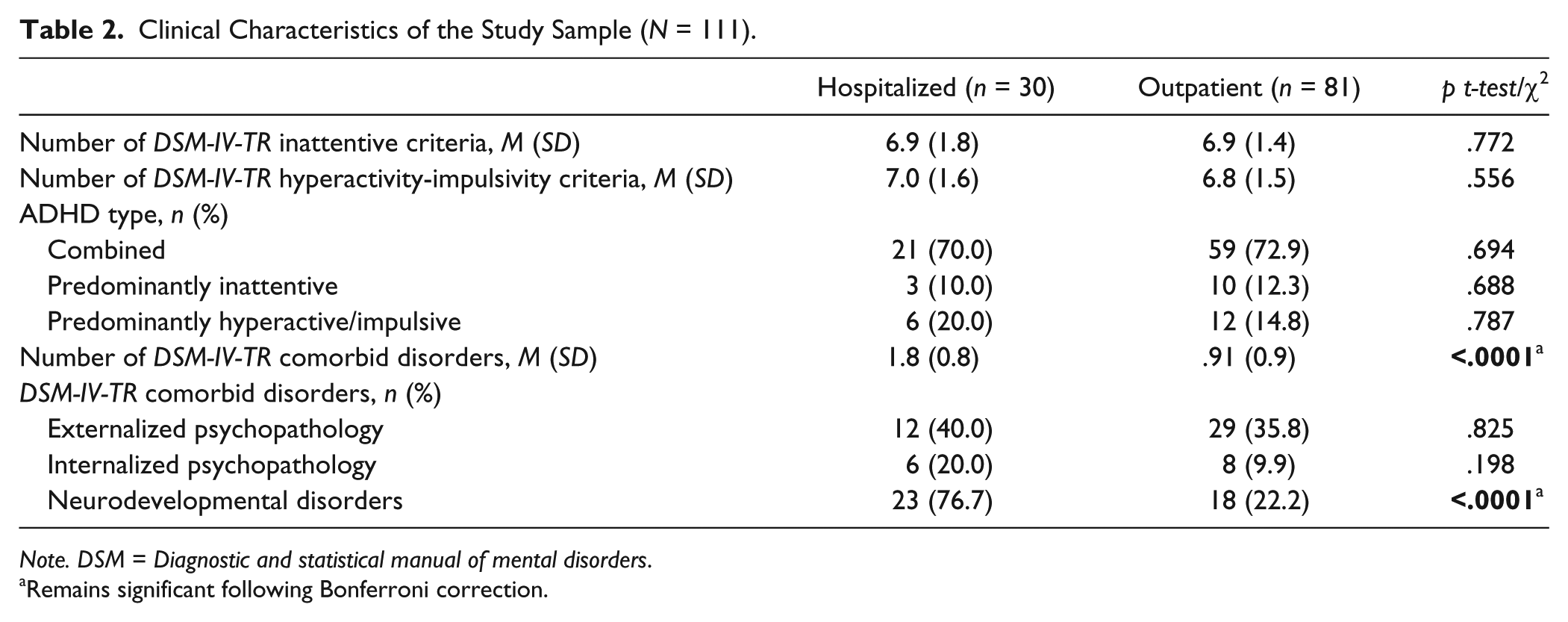
Note. DSM = Diagnostic and statistical manual of mental disorders.
Remains significant following Bonferroni correction.
Medical files were reviewed and the following information was collected: (a) personal demographic data: age, gender, and ethnicity; (b) familial demographic data: socioeconomic status, parents’ age, years of education, marital status, number of siblings, familial history of ADHD, and other psychopathologies; (c) clinical data: number of inattentive and hyperactive-impulsive criteria according to the DSM-IV-TR (APA, 2000), number and type of comorbid disorders.
The DSM-IV-TR (APA, 2000) disorders were divided into three categories: (a) externalized psychopathology: ODD- and CD-onset type, (b) internalized psychopathology: mood disorders and anxiety disorders, and (c) neurodevelopmental disorders: learning disorders, motor skills disorders, communication disorders, tic disorders, and enuresis (Not Due to a General Medical Condition).
According to the DSM-IV-TR (APA, 2000), the diagnosis of ADHD is excluded in cases of pervasive developmental disorders (PDD); thus, our cohort does not include children with autism spectrum disorders (ASD).
Data Analysis
The demographic and clinical variables were analyzed using Student’s t test or χ2 as appropriate. Bonferroni correction was used for multiple comparisons.
Results
Demographic Data
Hospitalized children with ADHD were found statistically significantly younger than those who were treated as outpatients (p < .0001). The rate of unmarried parents of the hospitalized children was found statistically significant higher than in the outpatient population (p < .001). There were no other statistically significant differences in any of the personal and familial demographic collected data (Table 1).
Clinical Data
Hospitalized children with ADHD exhibited statistically significantly higher rate of comorbid conditions than those who were treated as outpatients (p < .0001). Analysis of the type of comorbid conditions showed a higher rate of neurodevelopmental disorders in the hospitalized group (p < .0001). There were no statistically significant differences in any of the other recorded clinical data (Table 2).
The rate of inattentive symptoms was high (≥6 inattentive ADHD criteria) for both hospitalized and nonhospitalized subjects.
Discussion
The present study was designed to compare two groups in a cohort of ADHD preschoolers, differentiated by the severity of their dysfunction, according to the CGI-S, and need for intensive treatment at the DCIU. We attempted to identify discriminative demographic and clinical variables that may predict the need for comprehensive treatment (hospitalization) of preschoolers with ADHD. The major findings of the study were the younger age and the higher rate of unmarried mothers (single, divorced, separated) of the hospitalized children. In contrast, the rate of inattentive/ hyperactive-impulsive symptoms was similar in the two groups. In addition, the hospitalized children had a significant higher rate of comorbidities. It is of note that the rate of neurodevelopmental disorders was significantly higher in the hospitalized children and was the only clinical factor discriminating between the two groups.
Surprisingly, unlike previous studies (Russell et al., 2014), socioeconomic status did not discriminate between the hospitalized and nonhospitalized preschoolers with ADHD, although a trend toward higher SES was observed in the outpatients (p = .092).
The rate of divorced/separated/single parents was significantly higher in the hospitalized preschoolers. This association may be related to the impact of limited support of key family members in preschoolers with ADHD that required hospitalization (Hurting et al., 2007).
Like in previous studies (Lahey, Pelham, Loney, Lee, & Willcutt, 2005; Riley et al., 2008), the number of DSM-IV-TR (APA, 2000) inattentive criteria in our cohort of preschoolers with ADHD was high and similar in both groups (≥6/9). This finding suggests that preschoolers with ADHD have similar profile of attention deficits as older children. Similarly, the number of hyperactive-impulsive criteria did not discriminate between the groups. Thus, it seems that the clinical severity of the ADHD, as determined by the number of inattentive and hyperactive-impulsive criteria, does not explain the level of functional impairment that was responsible for the decision to hospitalize these children. This finding indicates that behavioral-regulatory dysfunction, as reflected by the increased rate of neurodevelopmental comorbidities, is more important than counting the number of Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria in the decision on the appropriate setting for treatment of preschoolers with ADHD.
The higher rate of comorbidity in the more impaired group was found to be related to a higher rate of neurodevelopmental disorders, and not to internalized or externalized disorders. This result stresses the importance of considering ADHD in the context of neurodevelopmental disorders, as it was recently adopted in the DC 0-5.
Numerous studies have shown that neurodevelopmental disorders, which include ADHD, tend to be associated and influence each other’s expression (Neville, 2013). It appears that high rate of comorbid neurodevelopmental disorders is the main discriminator between the two groups, displaying the same disorder, but with a different expression of pathological phenotype. This observation has important implications in the prognostic expectations of a preschooler with ADHD. Noteworthy, the presence of neurodevelopmental disorders seems to be more influential clinically than the externalized or internalized psychopathology (externalized behavioral-emotional presentations).
Strengths and Limitations
The major strengths of the study include the availability of hospitalized and nonhospitalized preschoolers with ADHD, and the thorough and comprehensive assessment by experts in the field of preschoolers’ psychopathology.
Despite these strengths, this study has several limitations. First, the relatively small size of the sample (N = 111). This is a frequent obstacle in the field of clinical research in the preschool years. Second, the lack of a comparison group of internalized psychopathology, like depression or anxiety. A third limitation is the lack of a group of preschoolers with combined ADHD and ASD, however, according to the DSM-IV-TR (APA, 2000) requirements, ASD, termed then PDD, was exclusion criterion in the diagnosis of ADHD.
Conclusion
The level of functional impairment and the coexistence of neurodevelopmental disorders are the leading factors in determining the severity of the psychopathology, and the appropriate setting for treatment in preschoolers with ADHD. Not surprisingly, single parent homes and the unmarried status of the mother are very likely to affect the presenting phenotype of the preschooler with ADHD. It seems that an interaction between the presence of ADHD and other neurodevelopmental disorders influences the functional severity of the clinical presentation, such that these preschoolers require a controlled environment to better manage their presenting symptoms, which include more than the symptoms/signs of inattentiveness and hyperactivity.
It is suggested that there is a need for a comprehensive assessment of the various neurodevelopmental areas in the regular psychiatric examination of preschool children, especially in cases of ADHD.
Furthermore, it is suggested that there is a need for a comprehensive assessment of the various neurodevelopmental areas in the regular psychiatric examination of preschool children, especially in cases of ADHD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.