
Abstract
ADHD is a neurodevelopmental disorder that begins in childhood and is characterized by difficulties sustaining attention, significant hyperactivity, and impulsivity (American Psychiatric Association, 2013). The prevalence of ADHD in youth is estimated to be 3.4% worldwide (Polanczyk, Salum, Sugaya, Caye, & Rohde, 2015) and 9.5% in the United States (Pastor, Reuben, Duran, & Hawkins, 2015). Unfortunately, despite the increase in public awareness of ADHD, only about half of the children who meet criteria for ADHD are diagnosed with the disorder and even fewer receive treatment (Froehlich et al., 2007). Untreated ADHD is associated with substantial impairment, causing youth not to reach their full potential in school and have poor social relationships (Sjöwall & Thorell, 2014). In addition, youth with untreated ADHD are more likely to engage in illicit substance use and nicotine and alcohol consumption (Elkins, McGue, & Iacono, 2007; Elkins et al., 2017).
Parental perception and beliefs about children’s behavior, as well as limitations of the educational setting may complicate diagnosis of ADHD (Hamed, Kauer, & Stevens, 2015). In addition, children with the inattentive type of ADHD are often not viewed as having difficulties as they do not exhibit significant behavioral problems (Sayal, Goodman, & Ford, 2006). Ineffective communication between parents and teachers may also prevent identification of children at risk of ADHD (Bussing, Gary, Mills, & Garvan, 2003). Furthermore, ADHD frequently presents with other conditions, such as learning disorders (DuPaul, Gormley, & Laracy, 2013), oppositional behavior and conduct disturbance, anxiety, and depression (Kessler et al., 2014), making an accurate diagnosis more challenging (Subcommittee on Attention-Deficit/Hyperactivity Disorder et al., 2011).
As core symptoms of ADHD are not always observed in the clinical setting, the current methods for diagnosing ADHD rely heavily on caregiver and teacher reports and rating scales as well as clinical interview of a child and their caregiver. Subjective information provided by family and educators could lead to overdiagnosis as well as underdiagnosis of youth with ADHD and, thereby, either delay a much-needed treatment or provide the medication management when it is not appropriate. Therefore, an objective test, such as one based on a biomarker, could help in early diagnosis and treatment of children with ADHD.
There are currently no biomarkers identified for accurately diagnosing ADHD. Of note, the blood cells’ membrane potential ratio (MPR™) was initially reported to identify participants with bipolar 1 disorder with sensitivity of 0.78 and specificity of 0.88 (Thiruvengadam & Chandrasekaran, 2007). Woodruff and colleagues later proposed measuring MPR™ of blood cells as a possible objective test for identifying ADHD (Woodruff, El-Mallakh, & Thiruvengadam, 2011). That study found that the MPR™ values of participants with ADHD differed from those with bipolar disorder or controls. The sensitivity of this test was reported as 0.75 to 0.90 and the specificity was 0.75.
The aim of the current study included comparing the MPR™ values of unmedicated youth with ADHD with controls without ADHD. The secondary objectives of this trial were to (a) evaluate the changes in MPR™ values in response to pharmacological treatment of ADHD and (b) evaluate the association between psychosocial impairment and the MPR™ values in youth.
Method
Participants
Participants were recruited between June 2016 and September 2017 from community advertisements and physician referrals in a mid-Atlantic metropolitan area. Inclusion criteria were (a) ≥6 years and ≤17 years of age, (b) having a parent who could attend the assessment and had the ability to understand and provide informed consent, (c) ability to provide assent, and (d) ability to provide a blood sample. Exclusion criteria included (a) diagnosis of bipolar disorder, (b) a current psychiatric condition that may prevent the participant from providing accurate information necessary for the diagnostic assessment, and (c) a medical condition that may place the participant at greater than minimal risk from a blood draw. Individuals diagnosed with bipolar disorder were excluded due to a prior study showing relative hyperpolarization of blood cells in these patients using MPR™ technology (Thiruvengadam & Chandrasekaran, 2007). Control group included participants with psychiatric conditions other than ADHD and bipolar disorder, as well as healthy individuals.
Of 120 participants screened, 44 (24 with ADHD, 20 psychiatric controls without ADHD) were eligible and provided at least one blood sample. Of the 24 medication-free participants with ADHD, 11 provided a second blood sample at least 1 month after receiving a stable dose of stimulant medication. Of note, one of these samples could not be processed due to a laboratory error. Of the remaining 10, seven (70.0%) were taking methylphenidate (including dexmethylphenidate and methylphenidate hydrochloride), two (20.0%) were taking amphetamine (including lisdexamphetamine and amphetamine/dextroamphetamine), and one (10.0%) was taking clonidine. Because only one youth initiated a nonstimulant medication alone, the nine participants with ADHD who initiated a psychostimulant (methylphenidate or amphetamine) were included in the within-group secondary analysis examining whether MPRs™ differ depending on whether participants were taking psychostimulants. Participant flow is depicted in Figure 1.
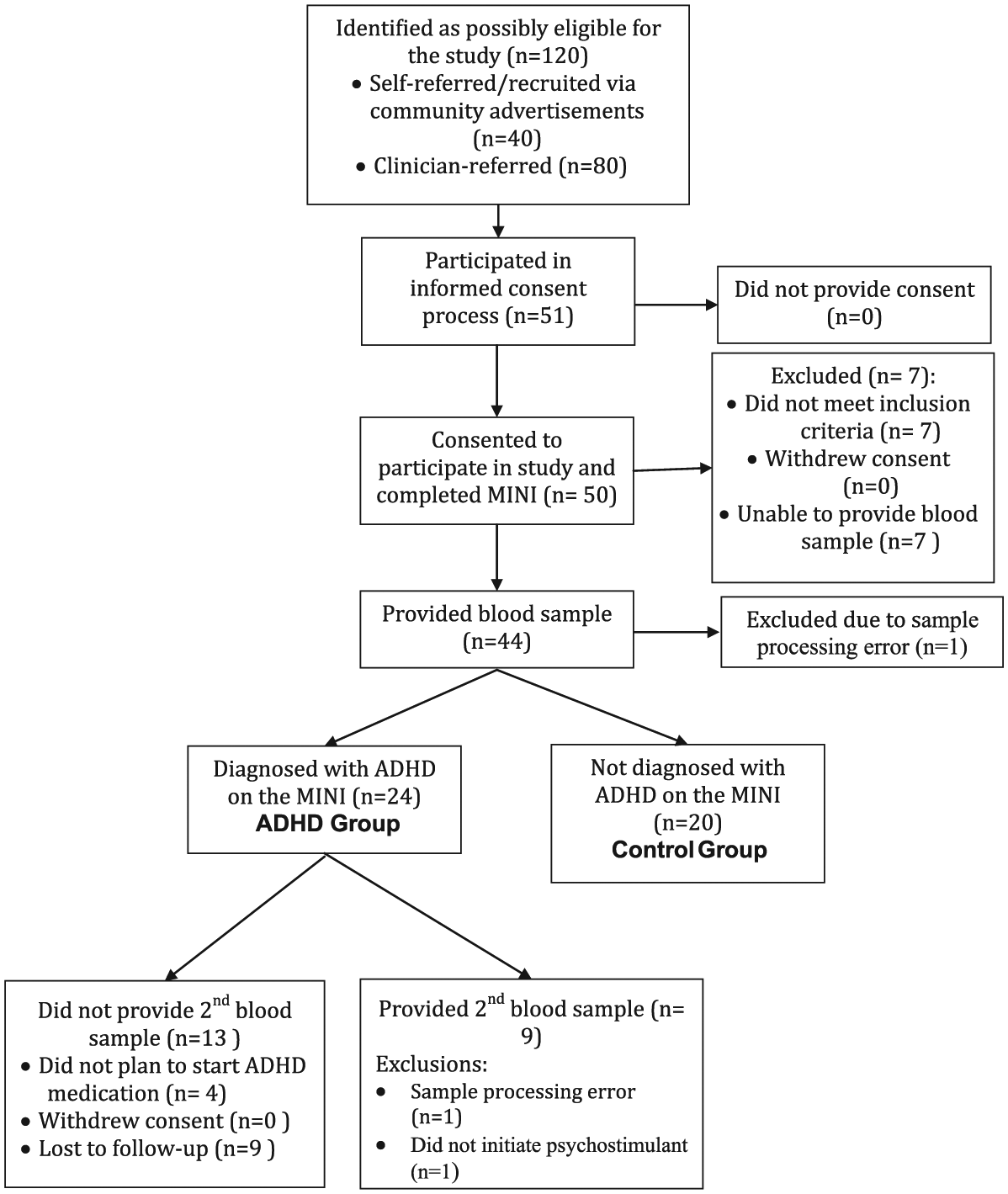
Participant flowchart.
Procedure
Prior to completing any study assessment, parents/guardians and participants provided written informed consent and assent, as approved by the local institutional review board. The study interview assessed the following:
Medical history
A board-certified psychiatrist (study principal investigator [PI]: ES) obtained relevant medical, social, psychiatric, and neurological history including a record of current medications/medication response and substance use history.
Diagnosis of ADHD, comorbid diagnoses, and functioning
A board-certified psychiatrist or bachelor-level study coordinator (under the supervision of the psychiatrist/PI) administered the Mini-International Neuropsychiatric Interview 7– Child Version (MINI-Kid), a structured psychiatric diagnostic interview with good reliability and validity (Sheehan et al., 1998). If the study coordinator administered the initial assessment, the participants were then reassessed by the board-certified psychiatrist using the MINI-Kid to confirm the diagnosis. The MINI-Kid, which screens for 30 Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) and International Classification of Diseases–10 (ICD-10) psychiatric disorders or disorder subtypes, was used to verify ADHD diagnoses in the study group, the absence of ADHD diagnosis in the control group, and the absence of bipolar disorder in all participants. The ADHD Rating Scale–IV (ADHD-RS-IV), a clinician-administered rating scale (DuPaul, Power, Anastasopoulos, & Reid, 1998), assessed ADHD symptom severity. The ADHD-RS-IV has been shown to be a valid assessment of ADHD severity in youth (DuPaul et al., 1998; Goodman et al., 2010). In addition, the Children’s Global Assessment Scale (C-GAS) provided a clinician rating of overall psychosocial functioning with scores ranging from 1 to 100 (Shaffer et al., 1983).
Demographics
Parents/guardians provided demographic information including child’s age, sex, race, ethnicity, and socioeconomic status (household income, parents’ employment status, etc.), which was used to characterize the sample.
MPR™ measurement
After completing the study interview, participants provided a 5.4-mL blood sample, which was sent to PPD Labs for processing. During the first blood sample collection, none of the participants was taking psychostimulants. Among youth with ADHD, a second blood sample was collected at least a month after receiving a stable dose of psychostimulant medication. Procedures for measuring MPR™ have been previously reported (Thiruvengadam & Chandrasekaran, 2007; Woodruff et al., 2011). To summarize, a lipid soluble fluorescent dye, DiOC6(3), was used to measure the membrane potentials in a plate reader (FLx 800 model manufactured by BioTek). Whole blood cells were incubated in a reference buffer and in a test buffer separately. The reference buffer contained NaCl, CaCl2, and glucose at physiological concentrations; the test buffer contained 30% of ethyl alcohol in addition to the chemicals contained in the reference buffer. The buffering agent hepes was also added to the buffer to maintain the pH. The MPR™ is the ratio of the membrane potential in the test buffer to the membrane potential in the reference buffer.
A subsample of participants with ADHD provided a second blood sample after starting their ADHD medication and remaining at a stable dose for at least 1 month. This second blood sample allowed for examination of whether MPRs™ are sensitive to psychopharmacologic treatment for ADHD.
Laboratory staff who processed blood samples were masked to participants’ psychiatric diagnoses to avoid introducing bias in the MPR™ measurement.
In addition to MPR™ values, the laboratory provided study staff with an MPR™ test result indicating whether each participant’s value was above the MPR™ test developers’ cutoff for ADHD (MPR™ values > approximately 0.75 are considered positive for ADHD). This cutoff score was derived from the developers’ prior work (Thiruvengadam & Chandrasekaran, 2007; Woodruff et al., 2011) and was set a priori to data collection for the current study.
Data Analytic Plan
All the following analyses were planned analyses. Descriptive statistics were presented to characterize the sample; t tests and chi-square analyses examined whether there were differences in demographics between the ADHD group and the control group. The a priori primary analysis was a logistic regression analysis examining whether MPR™ values were significantly associated with ADHD diagnosis among participants at the first assessment (including controls and youth with ADHD prior to initiating stimulant medication). To further assess how well the MPR™ test discriminates between individuals with ADHD (while not taking medication for ADHD) and controls, sensitivity (the probability that someone with ADHD would be correctly identified by the MPR™ test as having ADHD) and specificity (the probability that individuals in the control group would be correctly identified as not having ADHD) were calculated using the results of the logistic regression. Sensitivity and specificity were also calculated based on a cross tabulation of ADHD diagnosis based on the clinical interview and MPR™ test categorization based on the test developer’s a priori cutoff for ADHD. Planned secondary analyses included the following: (a) Pearson’s r characterizing the correlation between C-GAS scores and mean MPR™ values to determine whether MPR™ values are significantly associated with psychosocial impairment among controls and youth with ADHD prior to initiating psychostimulants and (b) paired samples t test examining whether mean MPR™ values significantly differ when individuals with ADHD are taking psychostimulant medication compared with when they are not taking psychostimulants. Only the nine participants with ADHD who initiated a psychostimulant (methylphenidate or amphetamine) were included in the within-group secondary analysis examining whether MPRs™ differ depending on whether participants were taking psychostimulants. All analyses were run in IBM SPSS Statistics 23.0 using p < .05 as the criterion for statistical significance.
Results
Participants
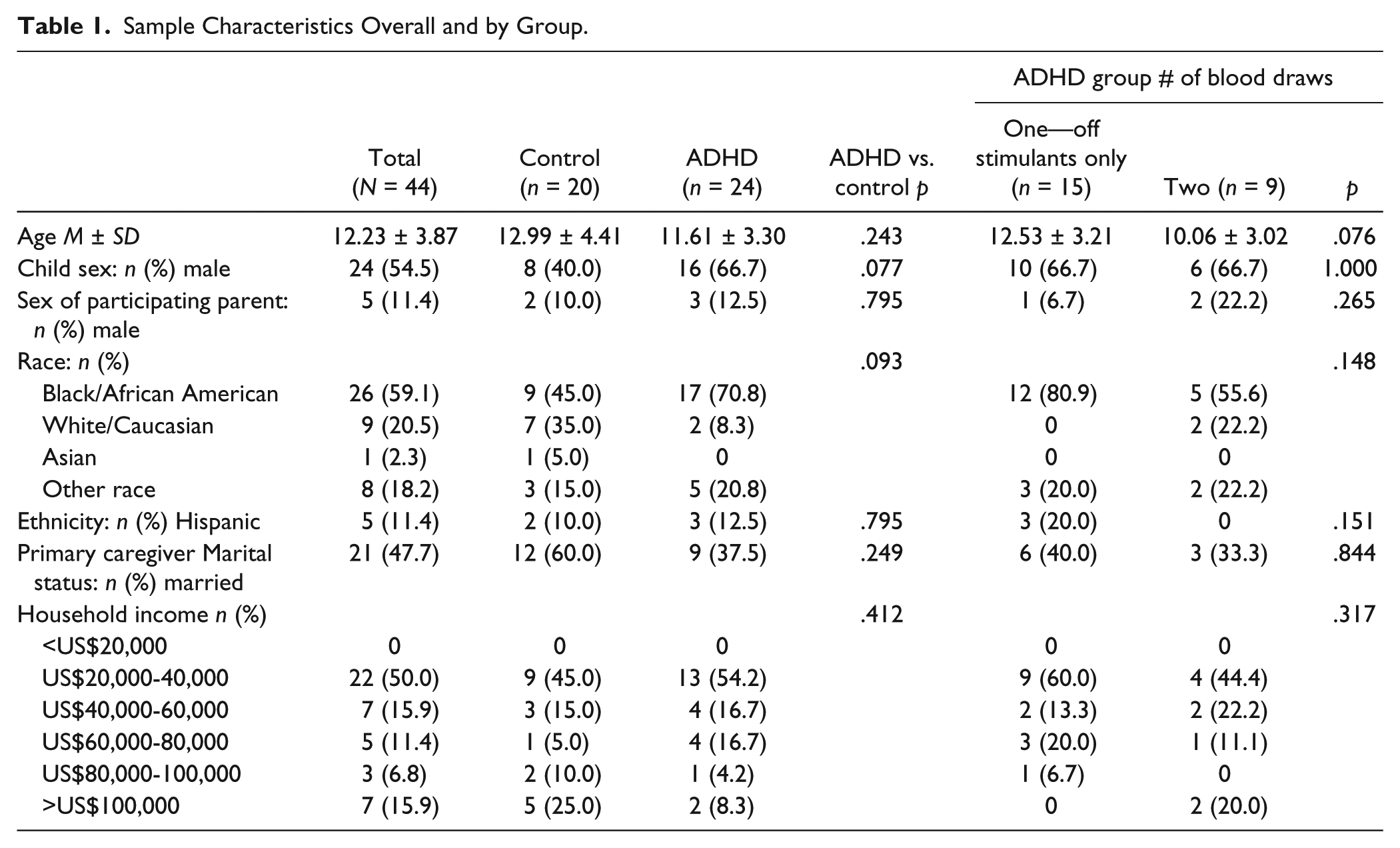
Demographic information by study group is presented in Table 1. The sample was 54.5% male, 59.1% were Black/African American, 20.5% were White/Caucasian, and 11.4% were Hispanic. Participants were 12.23 ± 3.87 years old on average and 50.0% reported a household income <US$40,000. Participants with (n = 24) and without (n = 20) ADHD did not significantly differ on any demographic variables examined; among participants with ADHD, those who provided a blood draw only off stimulants (n = 15) did not significantly differ from those who provided a blood draw both on and off stimulants (n = 9; Table 1). Table 2 lists the medications taken by study participants.
Sample Characteristics Overall and by Group.
Medication Use Overall and by Group.
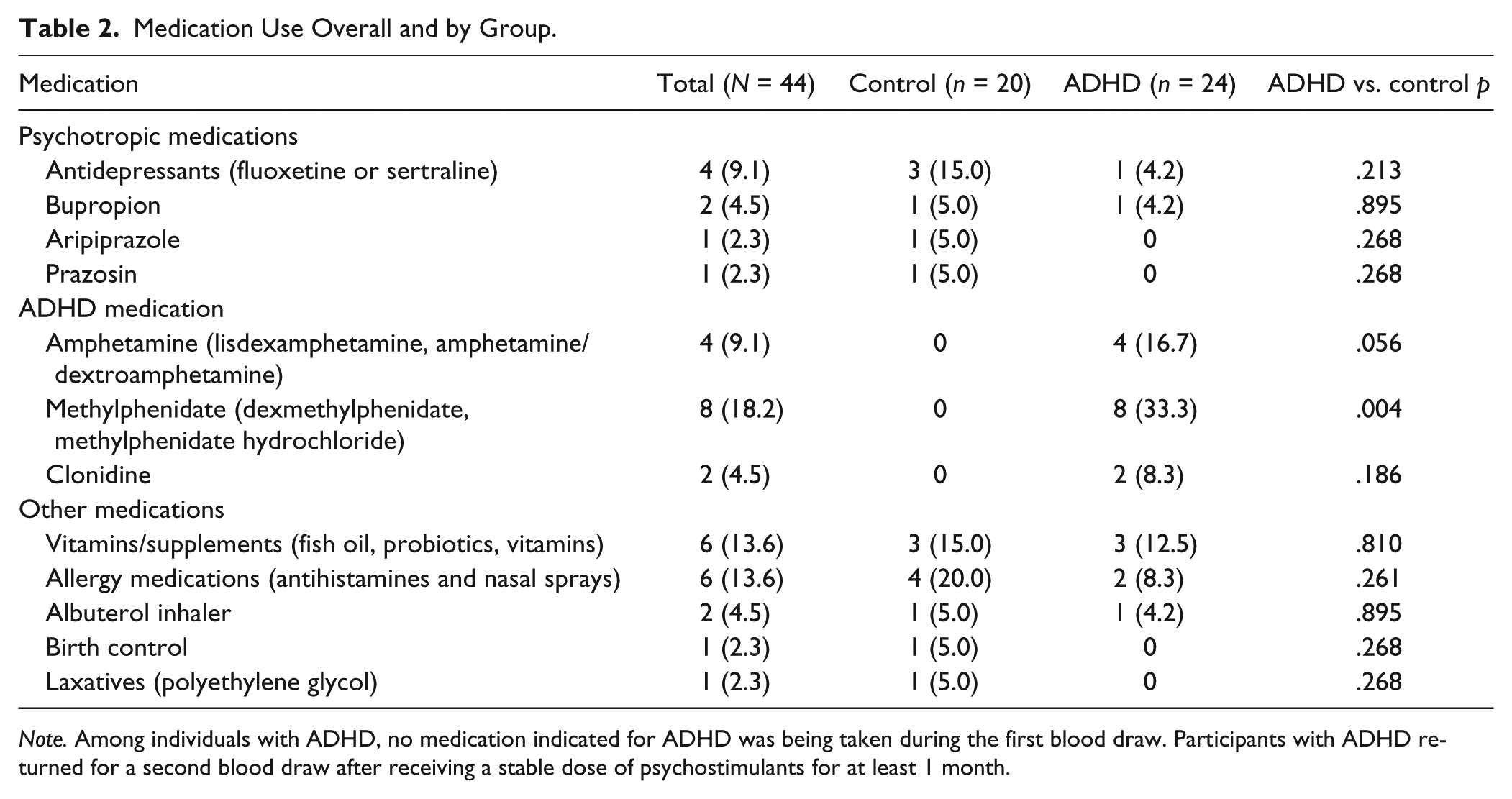
Note. Among individuals with ADHD, no medication indicated for ADHD was being taken during the first blood draw. Participants with ADHD returned for a second blood draw after receiving a stable dose of psychostimulants for at least 1 month.
Among participants with ADHD, eight (33.3%), none, and 16 (66.7%) presented with inattentive, hyperactive/impulsive, and combined subtypes, respectively; common comorbid diagnoses included disruptive behavior disorders (n = 14, 58.3%) and anxiety disorders (n = 7, 29.2%). In the control group, the most common diagnoses were anxiety disorders (n = 8, 45.0%), depression (n = 5, 25.0%), and disruptive behavior disorders (n = 3, 15.0%); six (30.0%) had no psychiatric diagnosis.
Primary Analyses
Results of the planned logistic regression using a cut value of 0.50, χ2(1) = 0.01, Nagelkerke R2 < .01, p = .937, indicated that MPR™ values of participants with an ADHD diagnosis who were not taking medication were not significantly different from those of participants in the control group. MPR™ values correctly characterized 54.5% of the sample: sensitivity = 100% and specificity = 0% (classification table presented in Table 3 and box plot presented in Figure 2).
Classification Table Based on Results of a Logistic Regression Analysis: Observed (via Diagnostic Interview) by Predicted (via MPR™ Values) ADHD Classification.
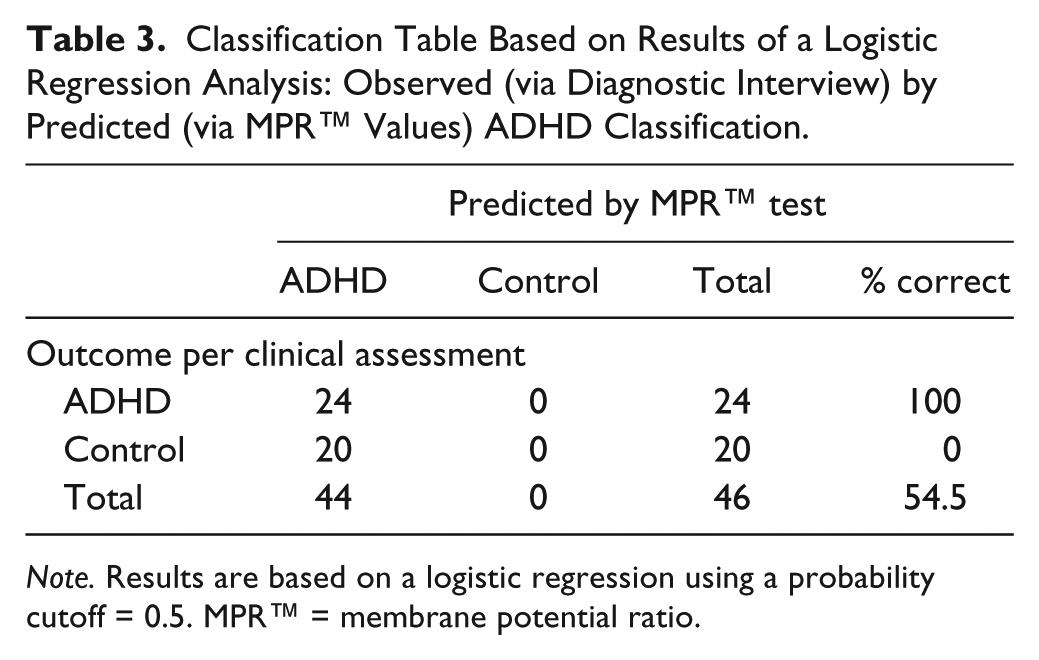
Note. Results are based on a logistic regression using a probability cutoff = 0.5. MPR™ = membrane potential ratio.
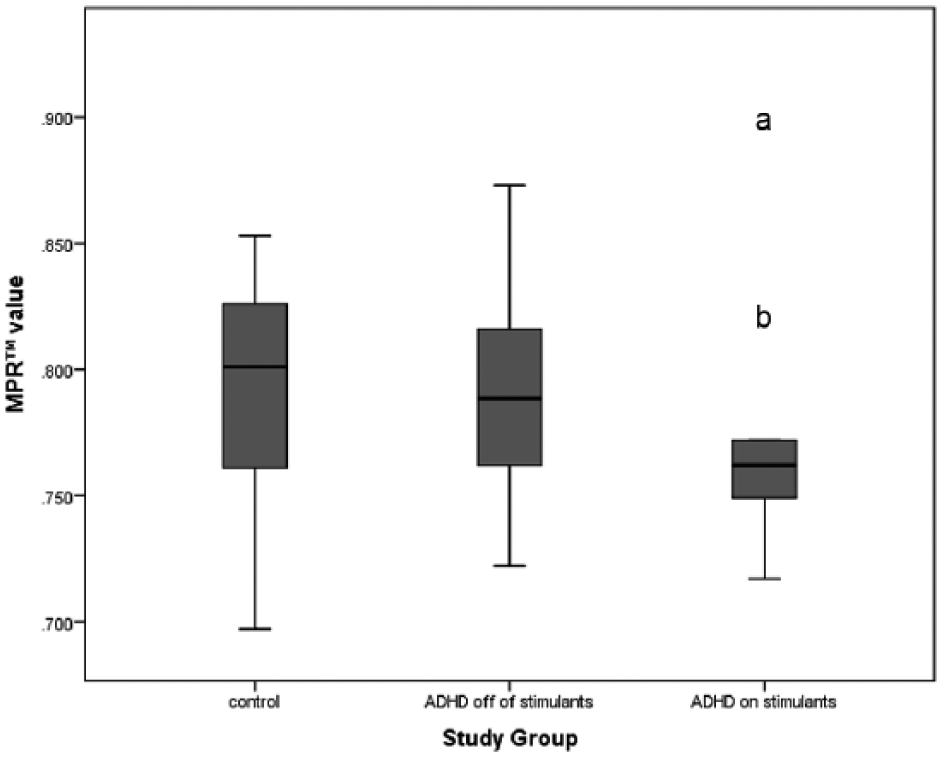
Box plot of MPRs™ by study group.
A second classification table using cutoff scores derived by the developers of the MPR™ test is presented in Table 4. Using the developer’s cutoff, 54.5% of participants were correctly categorized with sensitivity = 79.2% and specificity = 25.0%.
Classification Table: ADHD Diagnosis From the Clinical Interview by MPR™ Test ADHD Classification (Based on an a Priori Cutoff Set by Test Developers).

Note. Results are based on a cross tabulation using the ADHD cutoff score provided by the MPR™ test developers (MPR™ values >.75 are considered positive for ADHD). MPR™ = membrane potential ratio.
Secondary Analyses
MPR™ values were not significantly associated with C-GAS scores (r = −.13, p = .463); similarly, they were not associated with ADHD-RS hyperactivity/impulsivity (r = .12, p = .456), inattention (r = –.06, p = .706), or total (r = .03, p = .873) scores across the complete sample. Post hoc additional analyses indicated that, among youth with ADHD prior to initiation of psychostimulants, there was a significant correlation between MPR™ values and C-GAS scores (r = −.45, p = .027), but not ADHD-RS scores (ps > .05).
Among participants who provided a blood sample before taking stimulant medication and after remaining on a stable dose of stimulant medication for at least 30 days, time between blood draws was 41.11 ± 8.33 days on average. A planned paired samples t test indicated that MPR™ values did not significantly differ by medication status, t(8) = 1.09, p = .306. However, an additional analysis run excluding a participant with an extreme value before taking medication (MPR™ value >3 times the interquartile range; see Figure 2) indicated a trend for lower MPR™ values after taking stimulant medication (M = 0.76 ± 0.03) compared with before (M = 0.80 ± 0.05), t(7) = 2.20, p = .064.
Discussion
In the current study, the MPR™ values of unmedicated youth with ADHD were not different from a group of psychiatric and healthy control participants. In addition, there was no significant association between the MPR™ values and C-GAS scores in the full sample. Thus, these results do not replicate the prior findings reported by Woodruff et al. (2011). The reasons behind such discrepancy in the findings could be due to the lower power of our study. The pilot trial by Woodruff and colleagues included 148 participants with ADHD, whereas the present study had only 24 youth with ADHD. The laboratory processing blood samples was blinded to the results of the clinical assessment in this study; however, it is unclear whether this was the case with the Woodruff’s study.
The control group in the current study included youth with and without psychiatric diagnoses other than ADHD and bipolar disorder. The purpose behind including other diagnoses in the control group was to assess the utility of the MPR™ test in a community clinic, where youth present with a variety of psychiatric problems and it would be most helpful to have a test that distinguished ADHD from other conditions. Although enrolling psychiatric, rather than healthy, controls may have contributed to the observed low specificity of the MPR™ test in this study, it also suggests that this test is unlikely to correctly distinguish patients with ADHD from those with other conditions.
After excluding one outlier from the analysis, we have identified a trend in lowering of the MPR™ values in youth taking stimulant medications for ADHD when compared with their baseline MPR™ values before taking. The reasons for these findings are not yet clear because the MPR™ values of control participants are not significantly different from unmedicated youth with ADHD. However, if this finding is replicated, it could possibly lead to utilization of MPR™ test to monitor adherence to stimulant medications for ADHD. All except one participant with ADHD took stimulant medications in this trial (one youth took an alpha2-agonist and was excluded from the analysis). This study was not sufficiently powered to explore the effects of different classes of stimulant medications on MPR™ values. In addition, we have not found meaningful differences in identified comorbidities or demographic factors between the outlier excluded from the analysis and the rest of the participants; therefore, this result could be due to the lab error or other factors that we were not able to identify.
Our group recently conducted a similar study with adult participants, which did not show significant changes in MPR™ values between adults diagnosed with ADHD and psychiatric controls. Unlike the present study, we did not detect any effects of stimulant medications on the MPR™ values in adults. The reasons for this finding are yet to be determined.
Interestingly, there was a significant association between the MPR™ values and C-GAS scores in the ADHD group such that as MPR™ values increase, functioning decreases among kids with ADHD prior to initiating psychostimulants, but this was not the case for ADHD-RS scores (ps > .05). Although this could be an incidental finding, another possibility may be that MPR™ values are correlated with other symptoms associated with ADHD (such as emotional lability or irritability) rather that with ADHD diagnosis itself. This hypothesis needs to be explored in a larger trial.
The results of the current study need to be replicated on a larger sample of youth. The effect of comorbid psychiatric diagnoses, medical conditions, and psychotropic medications other than the stimulants on the MPR™ values should be explored. Given the trend in MPR™ values based on the participants’ medication status observed in this study, it may be important to further explore the association between MPR™ and the degree of symptom reduction with medication management. Another potential application of this test could be to monitor adherence with medication management.
One other limitation of the current study is that it did not address the stability of the MPR™ values over time. Therefore, there is no information available on the potential changes of the blood cells’ MPR™ independent of medication administration over the course of 1 month. In addition, the specified 1-month period of having controlled symptoms of ADHD on medication was chosen based on clinical experience; perhaps, a different length of time would have shown different results. It is important to investigate the timeline of changes in the MPR™ values after participants initiate medication management for ADHD and the stability of the MPR™ values after medications are discontinued. These limitations can be better addressed in a longitudinal study.
Footnotes
Declaration of Conflicting Interests
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Findling receives or has received research support, acted as a consultant and/or served on a speaker’s bureau for Aevi, Akili, Alcobra, Amerex, American Academy of Child & Adolescent Psychiatry, American Psychiatric Press, Bracket, Epharma Solutions, Forest, Genentech, Guilford Press, Ironshore, Johns Hopkins University Press, KemPharm, Lundbeck, Merck, NIH, Neurim, Nuvelution, Otsuka, PCORI, Pfizer, Physicians Postgraduate Press, Purdue, Roche, Sage, Shire, Sunovion, Supernus Pharmaceuticals, Syneurx, Teva, Tris, TouchPoint, Validus, and WebMD.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding for this project was provided by PsychNostics, LLC.