
Abstract
Introduction
ADHD is one of the most common neurobehavioral disorders presented to pediatric mental health professionals, affecting one of 20 children and adolescents worldwide (Polanczyk, de Lima, Horta, Biederman, & Rohde, 2007). In addition, the syndrome often occurs with other psychiatric conditions and attendant symptoms. According to parent reports, as many as 73% of children with ADHD suffer from sleep problems (Sung, Hiscock, Sciberras, & Efron, 2008). Frequently reported sleep complaints include difficulties initiating and maintaining sleep with increased night awakening (Cortese, Faraone, Konofal, & Lecendreux, 2009). The resulting fragmentation of the physiological sleep architecture reduces the sleep recovery process and, thus, may lead to excessive daytime sleepiness in people with ADHD (Cortese et al., 2009; Yoon, Jain, & Shapiro, 2012). Overall, patients with ADHD rate their sleep quality as worse when compared with healthy peers (Owens et al., 2009). As previous research mainly focused on parental assessment of sleep, data obtained from children and adolescents with ADHD are quite rare. Such studies, however, suggest that self- and parent reports correlate weakly, with higher correspondence between self-report assessment of sleep and actigraphy data (Owens, Maxim, Nobile, McGuinn, & Msall, 2000; Owens et al., 2009). Thus, taking only the parent’s perception into consideration will lead to a biased and limited insight into the sleep’s role in ADHD.
At the present time, causal and maintaining factors of sleep problems in ADHD are of great interest, because adequate sleep and regular sleep-wake schedules are essential for general health and well-being. One potential underlying pathophysiology explaining why disrupted sleep is highly comorbid with childhood ADHD is suggested by various associations of ADHD with circadian rhythm disturbances (Coogan, Baird, Popa-Wagner, & Thome, 2016). Light, especially short-wavelength light at around 460 nm, is the dominant human “zeitgeber” generating coherent, recurring biological rhythms at different levels of organization (Czeisler et al., 1989; Duffy & Czeisler, 2009; Hastings, O’Neill, & Maywood, 2007).
Higher rates for circadian-related abnormalities in children and adolescents suffering from ADHD exist for chronic sleep-onset insomnia (Corkum, Moldofsky, Hogg-Johnson, Humphries, & Tannock, 1999; Cortese et al., 2009) accompanied by circadian phase delay with later dim light melatonin onset (DLMO; Van der Heijden, Smits, Van Someren, & Gunning, 2005), a stronger evening circadian tendency (Benk Durmuş, Rodopman Arman, & Ayaz, 2017; Gruber et al., 2012), and the association of a polymorphism (rs1801260) of the circadian locomotor output cycles kaput (CLOCK) gene (Xu et al., 2010), which was reported to be related to eveningness typology and delayed sleep onset in patients with ADHD (Mishima, Tozawa, Satoh, Saitoh, & Mishima, 2005). These findings were confirmed by a more recent study, revealing a dose-response relationship between disrupted sleep patterns including sleep-onset latency, sleep deficiency, short sleep duration, delayed sleep phase disorder (DSPD), and ADHD-like behavior, with higher odds for inattention than for hyperactive/impulsive symptoms (Hysing, Lundervold, Posserud, & Sivertsen, 2016). Similarly, Hennig, Krkovic, and Lincoln (2017) identified the evening chronotype as a predictor for inattention.
Given the important influence of bright light on the circadian system and daytime functioning, the impact of the exposure to light from self-luminous displays on biological clock functions has become a matter of great concern for researchers and clinicians. The light emitted by screen-based devices is enriched for short wavelengths in the blue range of the spectrum and, therefore, may interact with the biological clock (Touitou, Touitou, & Reinberg, 2016). Meanwhile, new media forms including screen-based electronic devices enjoy great popularity among children and adolescents. In recent years, young people’s media use has increased dramatically to an average daily screen time of more than 4.5 hr in tweens (defined as 8- to 12-year-olds) and more than 6.5 hr in teens (defined as 13- to 18-year-olds; Rideout, 2015).
Indeed, a number of studies have examined the relationship of media consumption and sleep in young people, and have demonstrated that media use, especially in the late evening shortly before going to bed and overnight, increases the risk of sleep complaints, shorter sleep duration, irregular sleep patterns, night awakening, and daytime sleepiness (Adam, Snell, & Pendry, 2007; Arora, Broglia, Thomas, & Taheri, 2014; Carter, Rees, Hale, Bhattacharjee, & Paradkar, 2016; Cespedes et al., 2014; Gamble et al., 2014; Hale & Guan, 2015; Hysing et al., 2015; Kubiszewski, Fontaine, Rusch, & Hazouard, 2014; Li et al., 2007; Van den Bulck, 2004). As confirmed in a study by Garrison, Liekweg, and Christakis (2011), evening media use had a greater impact on sleep than daytime use, showing that each additional hour of near-bedtime media use was associated with a significant increase in sleep problems in preschool children. Interestingly, Bruni et al. (2015) found that evening chronotypes have more technological devices in their bedrooms, engage in more technology-related activities after 9 p.m., and have later turning off devices time at night compared with early chronotypes.
Considering the parallel increase in both, diagnosis of ADHD and young people’s media use, there is a growing body of evidence suggesting a potential link between these factors. A meta-analysis from Nikkelen, Valkenburg, Huizinga, and Bushman (2014) revealed a significant positive correlation between television viewing/video gaming and composite ADHD-like behavior, attention problems, and impulsivity. Findings from longitudinal studies identified television viewing and video game playing in early childhood as potential contributors to greater subsequent attention problems (Gentile, Swing, Lim, & Khoo, 2012; Landhuis, Poulton, Welch, & Hancox, 2007; Swing, Gentile, Anderson, & Walsh, 2010).
Although there is still no comprehensive information about media use in ADHD, the scant studies undertaken so far indicate that individuals with ADHD are more attracted to electronic media and engage in more screen time than typically developed peers (Acevedo-Polakovich, Lorch, & Milich, 2007; Bolic Baric, Hellberg, Kjellberg, & Hemmingsson, 2018). Examining the association of the availability of a bedroom TV with total screen time among 6- to 17-year-olds with ADHD revealed that they spend 150 min per weekday watching TV, watching videos, or playing video games (Lo, Waring, Pagoto, & Lemon, 2015). As high exposure to screen-based media may exacerbate behavioral problems and attention difficulties (Johnson, Cohen, Kasen, & Brook, 2007), these results emphasize the necessity of understanding and limiting screen-based media use in youth affected by this disorder.
As previously mentioned, insufficient sleep duration and disturbed sleep are considered as risk factors for behavioral problems among children. In turn, individual sleeping behavior is highly influenced by sleep hygiene, including various practices and habits that are intended to promote a good sleep quality (Mindell, Meltzer, Carskadon, & Chervin, 2009). Especially prebedtime screen-based media use is a common activity that is not in line with principles of good sleep health. It is, therefore, of particular interest to study how these variables interrelate, as to date, surprisingly, little data exist focusing on the association between prebedtime media exposure and behavioral problems.
One of the few studies related to the broader topic was provided by Arns, van der Heijden, Arnold, and Kenemans (2013), who examined the relationship of solar intensity with geographical variation in ADHD rates. Their results showed lower prevalence in areas with higher solar intensity. An apparent preventive effect of high sun intensity on ADHD was assumed, explaining 34% to 57% of the variance in ADHD prevalence across 49 U.S. states and nine non-U.S. countries. According to Arns and colleagues, this protective effect is due to the strong phase-advancing impact of natural bright light during the morning, improving circadian clock disturbances associated with ADHD. Use of electronic media shortly before bedtime might delay circadian rhythms even further through DLMO suppression, which, in turn, results in delayed sleep onset and shortened sleep duration (Arns et al., 2013). Furthermore, Arns and coworkers assume that at least a subgroup of children with ADHD are more vulnerable to sleep difficulties manifested by symptom exaggeration. As a conclusion, this subgroup would benefit from reduced evening use of modern media emitting light in the blue spectrum and increased daytime light exposure (especially in the morning) through counteracting delayed circadian phase (Arns et al., 2013).
Taken together, the current state of knowledge suggests that there may be a correlation between (prebedtime) media use, sleep difficulties, and manifestation of ADHD-related symptoms. However, there is still limited research, with the majority of studies examining solely media use or sleep and not assessing the association of these two factors with behavior and ADHD symptoms. The reported findings prompted us to hypothesize that more use of electronic media through self-luminous displays will be associated with impaired sleep quality and increased behavioral problems. Furthermore, considering the high rates of sleep complaints and disturbed circadian rhythms in individuals with ADHD, their high exposure to screen-based media, the importance of light in regulating sleep/wake cycle, and the vital necessity of sleep for optimal daytime functioning, we presume stronger relationships between time spent with screen-based media, sleep problems, and ADHD-like behavior in patients than in nonreferred children and adolescents. However, due to the strong impact of photic stimulation on neurophysiological processes and the dramatic increase in media consumption among young people, an association is also anticipated in healthy individuals. For this reason, a case-based as well as a community-based approach was conducted, allowing both categorical and dimensional conceptualization of ADHD symptomatology.
Therefore, we aimed to (a) investigate differences between ADHD patients and healthy controls regarding sleep behavior, use of screen-based media, and parameters of circadian rhythm; (b) analyze the relationship between sleep, screen-based media use, circadian rhythm, and ADHD-related behavior in a community sample; and (c) test the contribution of sleep habits and screen-based media use to the manifestation of symptoms of ADHD in healthy children and adolescents. Our cross-sectional study will, thus, assess the relationships between the relevant constructs, media consumption, sleep, and ADHD, but not test causal pathways toward ADHD, which would require a longitudinal approach.
Method
Ethical approval was obtained from the ethics committee of the Albert Ludwigs University of Freiburg, Germany. All participants and their parents signed an informed consent before enrolment in the study. Data were collected from June 2014 to June 2016.
Participants
This study included N = 357 children and adolescents from the general population and N = 61 children and adolescents with ADHD, both aged 8 to 18 years. Healthy participants were recruited through local schools and after-school programs, and through announcements in regional publications and social media. Snowball sampling was also used, whereby the initial participants acted as informants and recommended further eligible participants for the study. Of the participants with ADHD, 53 (87%) were outpatients of the Department of Child and Adolescent Psychiatry at the University Medical Centre Freiburg, where diagnosis of ADHD is based on criteria defined by the International Classification of Diseases-10 (ICD-10; World Health Organization, 1992). The remaining eight (13%) patients had received their diagnosis from office-based child psychiatrists. Psychostimulants were taken by 47 (77%) patients, but as this study was part of a larger study including a computer-based test battery on cognitive performance, they were free of medication at least 24 hr before the study day. All participants should have an IQ score ⩾70 as assessed with the Culture Fair Intelligence Test 20–Revision (CFT 20-R; Weiß, 2006). Exclusion criteria for the healthy participants were (a) any neurological or psychiatric disorders and (b) pronounced developmental delay. Exclusion criteria for patients with ADHD were (a) diagnosis of an autism spectrum disorder (ASD) or (b) pronounced developmental delay. Of the whole study population, two samples were formed to test the hypotheses. The matched sample (N1 = 122) was composed of N = 61 patients with ADHD and N = 61 healthy controls. Gender, age, and IQ score are shown in Table 1 for each sample, respectively. In the matched sample, there were no significant differences in gender distribution, mean age, or IQ (all ps > .20). The community sample (N2 = 377) included all 357 healthy participants plus, according to the prevalence of ADHD of 5.29% (Polanczyk et al., 2007), 20 randomly selected patients from the ADHD sample. Of those, 14 (70%) patients received stimulant medication.
Study Samples: Participant Characteristics Gender, Age, and IQ Score.
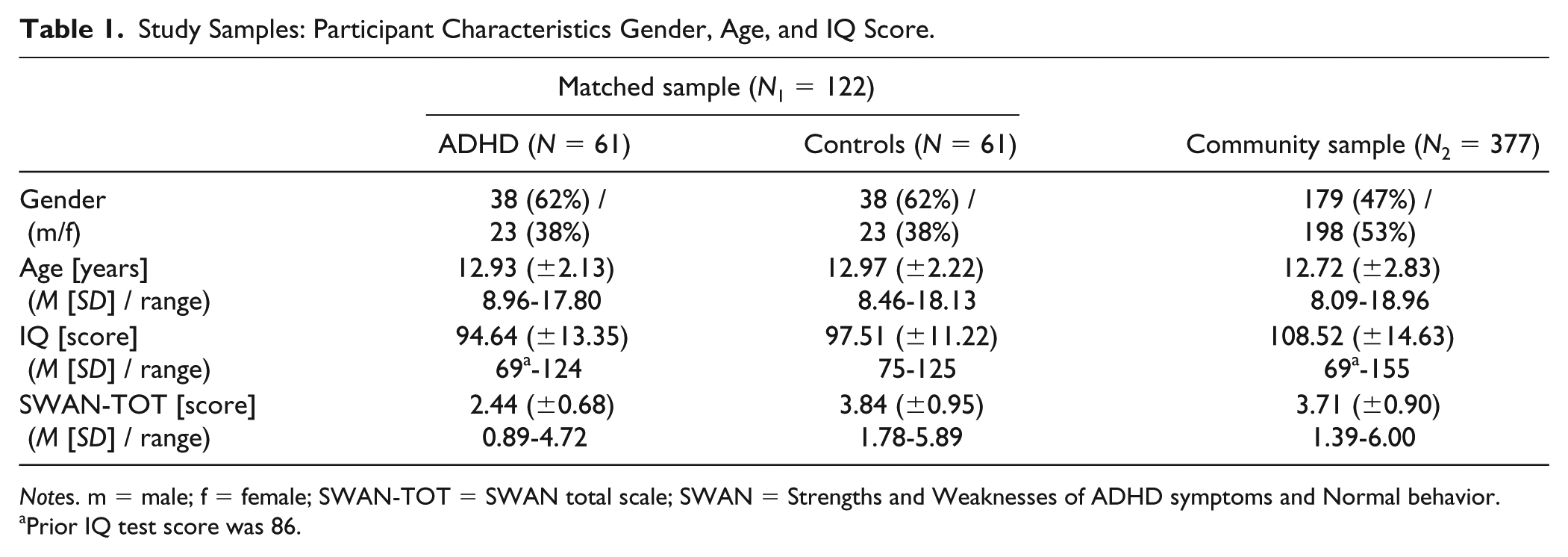
Notes. m = male; f = female; SWAN-TOT = SWAN total scale; SWAN = Strengths and Weaknesses of ADHD symptoms and Normal behavior.
Prior IQ test score was 86.
Measures
Sleep habits questionnaire
A self-report questionnaire based on the School Sleep Habits Survey (SSHS) developed by Wolfson and Carskadon (1998) was used to assess participants’ usual sleep-wake behavior over the past 2 weeks. The SSHS has shown good validity and high correlation with other self-report measures (Wolfson et al., 2003). Two age-specific versions for children (8-11 years) and adolescents (12-18 years) were handed out. Information on bedtime, time to fall asleep, and total sleep time were obtained for school and weekend nights separately. Deviation from individual sleep requirement was calculated as deviation of total sleep time from self-assessed optimal sleep duration, both on school and weekend nights. The number of night awakenings was categorized (never/once/2 or 3 times/more than 3 times/I have no idea), and participants who ticked I have no idea were excluded from the data analysis. Daytime sleepiness (no problem at all/a little problem/more than a little problem/a big problem/a very big problem) was also assessed. In addition, the adolescents’ (12-18 years) version of the questionnaire contained a morningness/eveningness scale, which is composed of 10 multiple-choice items assessing the circadian preference for certain activities (derived from Smith, Reilly, & Midkiff, 1989). Total score for determining one’s chronotype ranges from 10 (evening type) to 43 (morning type). Díaz-Morales, de León, and Sorroche (2007) suggest cutoffs at the 20th and 80th percentiles (evening type = 10-20, intermediate type = 21-27, morning type = 28-43). Cronbach’s alpha of the morningness/eveningness scale is .78 (Acebo & Carskadon, 2002). Furthermore, adolescents completed a delay scale, asking about the frequency of six typical behaviors that are likely to be related to delayed sleep phase: arrived late to class because you overslept, stayed up until at least 3 a.m., stayed up all night, slept in past noon, needed more than one reminder to get up in the morning, had an extremely hard time falling asleep. Frequency of each behavior was rated on a 5-point scale from 0 (never) to 4 (every day/night) and were summed to obtain a total score. Cronbach’s alpha of the Delay scale is .70 (Acebo & Carskadon, 2002).
Media use questionnaire
Data about participants’ screen-based media use habits were collected using an adapted version of the screen time-based sedentary behavior questionnaire from the HELENA study (Rey-López et al., 2012). As demonstrated by the developers, reliability was found to be good to excellent. Two age-specific versions for children (8-11 years) and adolescents (12-18 years) were administered. To assess participants daily media use, they had to report their habitual time spent with screen-based media (television viewing/video games/computer/mobile phone) during both school and weekend days by ticking the fitting category (no time/up to 30 min/30 min to 1 hr/1 to 2 hr/2 to 3 hr/3 to 4 hr/4 to 5 hr/more than 5 hr). Similarly, information on daily media use in the 2 hr before going to bed was obtained: Children aged 8 to 11 years were asked how often (never, once a month, once a week, 2-3 times a week, 4-6 times a week, every evening) and how long (no time, 5-15 min, 15-30 min, 30 min to 1 hr, more than 1 hr) they usually use electronic devices before bedtime. Adolescents aged 12 to 18 years were asked how many time they spend with screen-based media in the last 2 hr before bedtime (television viewing/video games/computer/mobile phone) with nine categories of response (no time/up to 15 min/15-30 min/30-45 min/45-60 min/1 to 1 hr 15 min/1 hr 15 min to 1 hr 30 min/1 hr 30 min to 1 hr 45 min/1 hr 45 min to 2 hr). If this sum exceeds the threshold of 2 hr, it was capped at the peak value of 2 hr. Furthermore, the presence of screen-based devices in the bedroom (television/gaming console/computer) was assessed through yes/no questions.
Strengths and Weaknesses of ADHD symptoms and Normal behavior (SWAN) scale
Participants’ ADHD-like behavior was measured by using the German version of the SWAN scale (Schulz-Zhecheva et al., 2019; Swanson et al., 2006). Based on the diagnostic criteria for ADHD listed in Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) and Diagnostic and Statistical Manual of Mental Disorders (5th ed., DSM-5; American Psychiatric Association, 2013), the SWAN scale contains 18 items, with Items 1 to 9 corresponding to the Attention Deficit subscale and items 10 to 18 representing the Hyperactivity/Impulsivity subscale. In contrast to other behavior rating scales, the items of the SWAN scale are reworded using a neutral to strength-oriented formulation. Parents were asked to quantify each item regarding the severity of ADHD symptoms manifested in their child compared with other children of the same age by using a 7-point Likert-type scale ranging from 0 (far below average) to 6 (far above average). Due to the balanced scoring system, the SWAN scale assesses symptoms of ADHD in a dimensional manner. Dividing participants’ total scores by the number of all items produces the score of the SWAN total scale (SWAN-TOT) and ranges from 0 to 6, with low scores indicating higher level of ADHD symptoms and symptom load. The German version of this scale has recently been proven to show high reliability with an overall Cronbach’s alpha of .95 and excellent validity (Schulz-Zhecheva et al., 2019).
Data Analysis
Statistical analyses were performed using SPSS for Mac, Version 22. Descriptive statistics included frequencies (n), mean (M), standard deviation (SD), and range. Independent sample t tests and chi-square tests were run whenever patients and controls were compared. Cohen’s d was calculated to estimate the effect size. A principal component analysis (PCA) with orthogonal rotation (varimax) was performed to aggregate and reduce the number of variables. Conducted on all sleep (excepted for the adolescent-only variables chronotype and delay scale) and media items, the PCA for the community sample produced a five-component solution. Sampling adequacy was tested with the Kaiser-Meyer-Olkin (KMO) coefficient, KMO = .74 (“good” according to Hutcheson & Sofroniou, 1999) and Barlett’s test of sphericity, χ2(91.00) = 1,836.03, p < .001. All the five extracted components had eigenvalues larger than Kaiser’s criterion of 1, explaining 31%, 15%, 9%, 8%, and 7% of the variance, respectively, and 70% in sum. The resulting components, their related variables, and factor loadings after rotation are presented in Table 2. Component 1 will henceforth be called “media time,” Component 2 “sleep-wake behavior,” Component 3 “sleep onset,” Component 4 “sleep deviation,” and Component 5 “sleep quality.” As preanalysis revealed substantial correlation between chronotype and the Delay scale, both obtained for adolescents aged 12 to 18 years only, a new variable called “circadian rhythm” was created using the formula, (“chronotype” + reversed “delay scale”) / 2, with lower scores indicating more eveningness, and more behaviors presumed to be linked to a delayed sleep phase. Only this variable was used for further analysis. Pearson correlations were conducted to analyze the potential relationships between the study variables and symptoms of ADHD. Multiple regressions were conducted to identify predictors of ADHD-related behavior. Significance levels were set as p ⩽ .05.
Resulting Factors of Sleep and Media Variables Among the Community Sample.
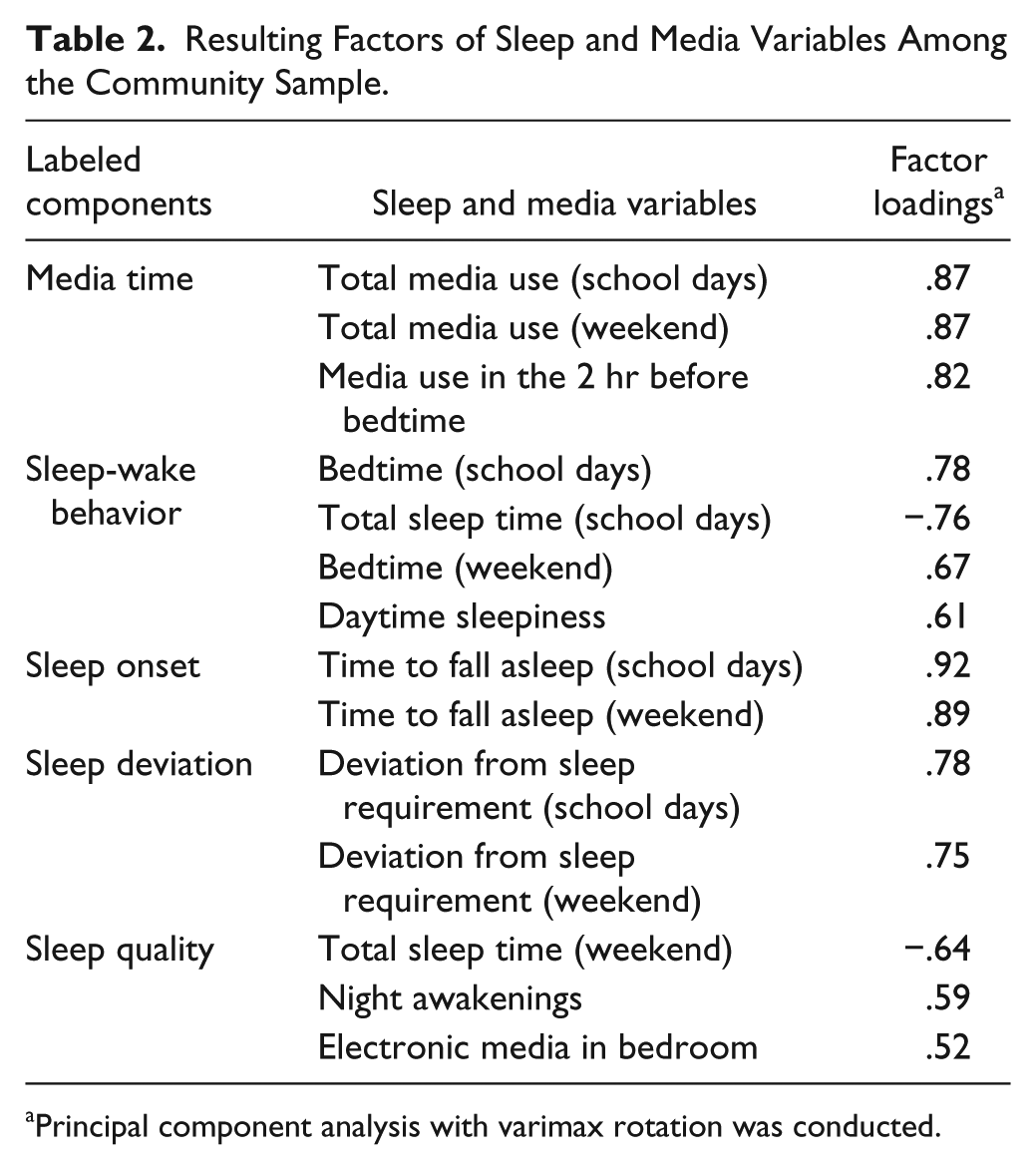
Principal component analysis with varimax rotation was conducted.
Results
Comparisons Between ADHD Patients and Controls (Matched Sample)
Mean and standard deviation of the subjective sleep and media measures of ADHD patients and controls are presented in Table 3. Between-group comparison of sleep parameters revealed a significant longer sleep-onset time on school days in patients compared with the control group, t(104.55) = −2.34, p = .021, Cohen’s d = 0.43. There were no significant differences in bedtime, total sleep time, deviation from individual sleep requirement, daytime sleepiness, or night awakenings. As adolescents were further asked about behavior regarding circadian tendencies, between-group comparison showed more delayed sleep in youth with ADHD compared with their healthy peers, t(67.31) = −2.19, p = .032, Cohen’s d = 0.49.
Sleep Habits and Screen-Based Media Use in ADHD Patients and Controls (Matched Sample).
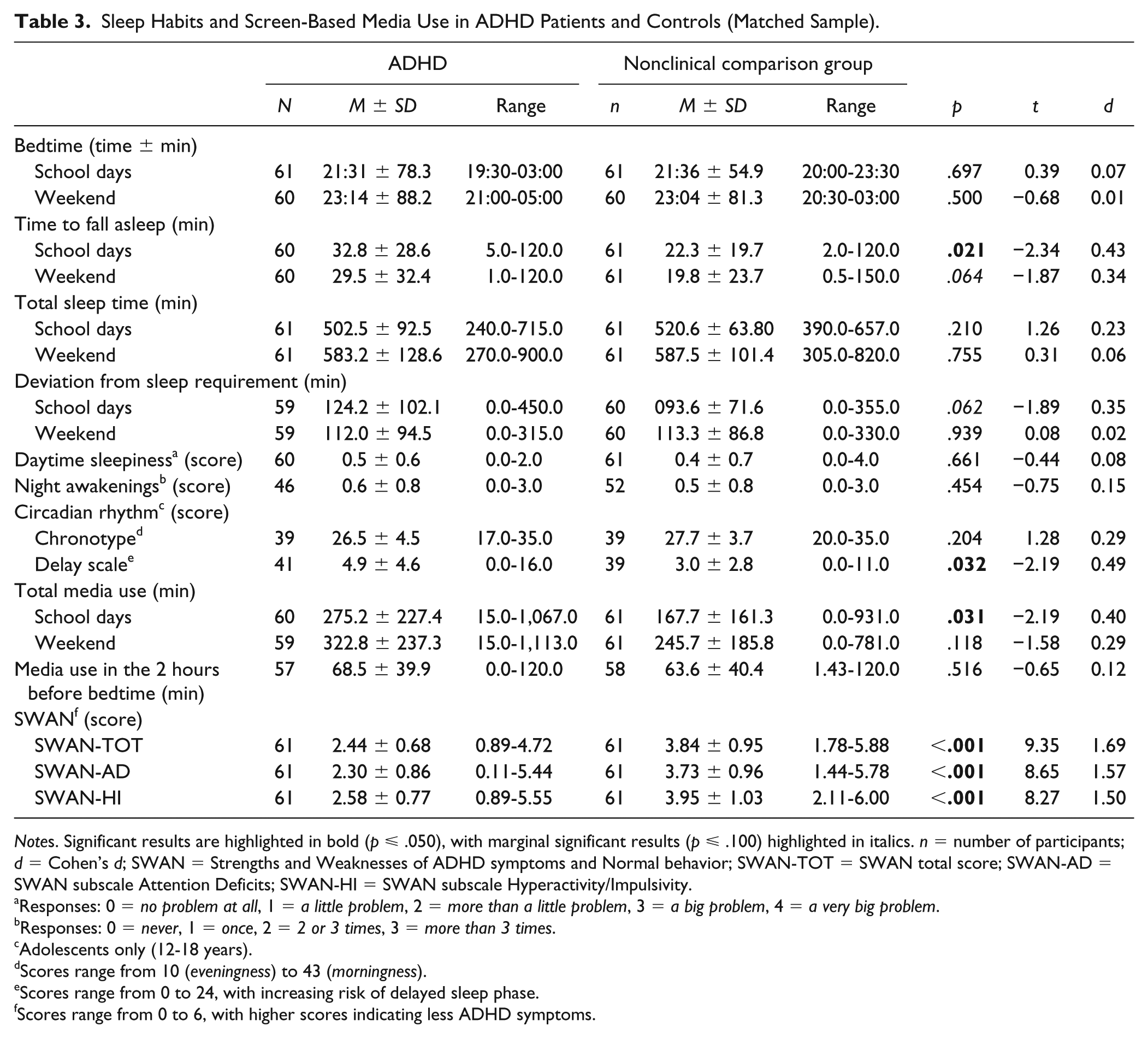
Notes. Significant results are highlighted in bold (p ⩽ .050), with marginal significant results (p ⩽ .100) highlighted in italics. n = number of participants; d = Cohen’s d; SWAN = Strengths and Weaknesses of ADHD symptoms and Normal behavior; SWAN-TOT = SWAN total score; SWAN-AD = SWAN subscale Attention Deficits; SWAN-HI = SWAN subscale Hyperactivity/Impulsivity.
Responses: 0 = no problem at all, 1 = a little problem, 2 = more than a little problem, 3 = a big problem, 4 = a very big problem.
Responses: 0 = never, 1 = once, 2 = 2 or 3 times, 3 = more than 3 times.
Adolescents only (12-18 years).
Scores range from 10 (eveningness) to 43 (morningness).
Scores range from 0 to 24, with increasing risk of delayed sleep phase.
Scores range from 0 to 6, with higher scores indicating less ADHD symptoms.
When looking at media use, we found that patients with ADHD spent significant more time using screen-based media on school days than the reference group, t(119.00) = −2.19, p = .031, Cohen’s d = 0.40. No significant differences were found in total media use on weekends and media use in the 2 hr before bedtime. Also, availability of screen-based devices in the sleep environment did not differ significantly: 69% of participants with ADHD have at least one device in their bedroom compared with 61% of the healthy participants, χ2(1.00) = 0.77, p = .380. No significant gender differences were found in these variables.
Correlations Between the Study Variables in the Community Sample
Descriptive statistics about sleep habits and screen-based media use in the community sample are summarized in Table 4. Pearson correlations between gender, age, IQ, the sleep and media consumption components, and symptoms of ADHD are given in Table 5. In our community sample, there were no gender associations but some age associations with the study variables, such as participants tended to report more media time, more unfavorable sleep-wake behavior, less deviation from individual sleep requirement, later circadian rhythmicity, and more symptoms of hyperactivity/impulsivity the older they were. Children and adolescents with higher IQ tended to have less favorable sleep-wake behavior and scored higher on the entire SWAN (sub)scale, indicating less ADHD-related behavior. Participants who engaged longer in screen-based media showed more symptoms of inattention. Deviation from individual sleep requirement was also related to more ADHD symptomatology on the entire SWAN (sub)scale. Circadian rhythm toward eveningness and delayed sleep phase was correlated with higher media time, unfavorable sleep-wake behavior, more deviation from subjective sleep requirement, as well as more ADHD-related behavior in adolescents. The described correlations were all statistically significant (p ⩽ .05).
Sleep Habits and Screen-Based Media Use and Comparisons Between Children (8-11 Years) and Adolescents (12-18 Years) in the Community Sample.

Notes. Significant results are highlighted in bold (p ⩽ .050), with marginal significant results (p ⩽ .100) highlighted in italics. n = number of participants; d = Cohen’s d; SWAN = Strengths and Weaknesses of ADHD symptoms and Normal behavior; SWAN-TOT = SWAN total score; SWAN-AD = SWAN subscale Attention Deficits; SWAN-HI = SWAN subscale Hyperactivity/Impulsivity.
Responses: 0 = no problem at all, 1 = a little problem, 2 = more than a little problem, 3 = a big problem, 4 = a very big problem.
Responses: 0 = never, 1 = once, 2 = 2 or 3 times, 3 = more than 3 times.
Adolescents only (12-18 years).
Scores range from 10 (eveningness) to 43 (morningness).
Scores range from 0 to 24, with increasing risk of delayed sleep phase.
Scores range from 0 to 6, with higher scores indicating less ADHD symptoms.
Pearson Correlation Between Study Variables in the Community Sample.
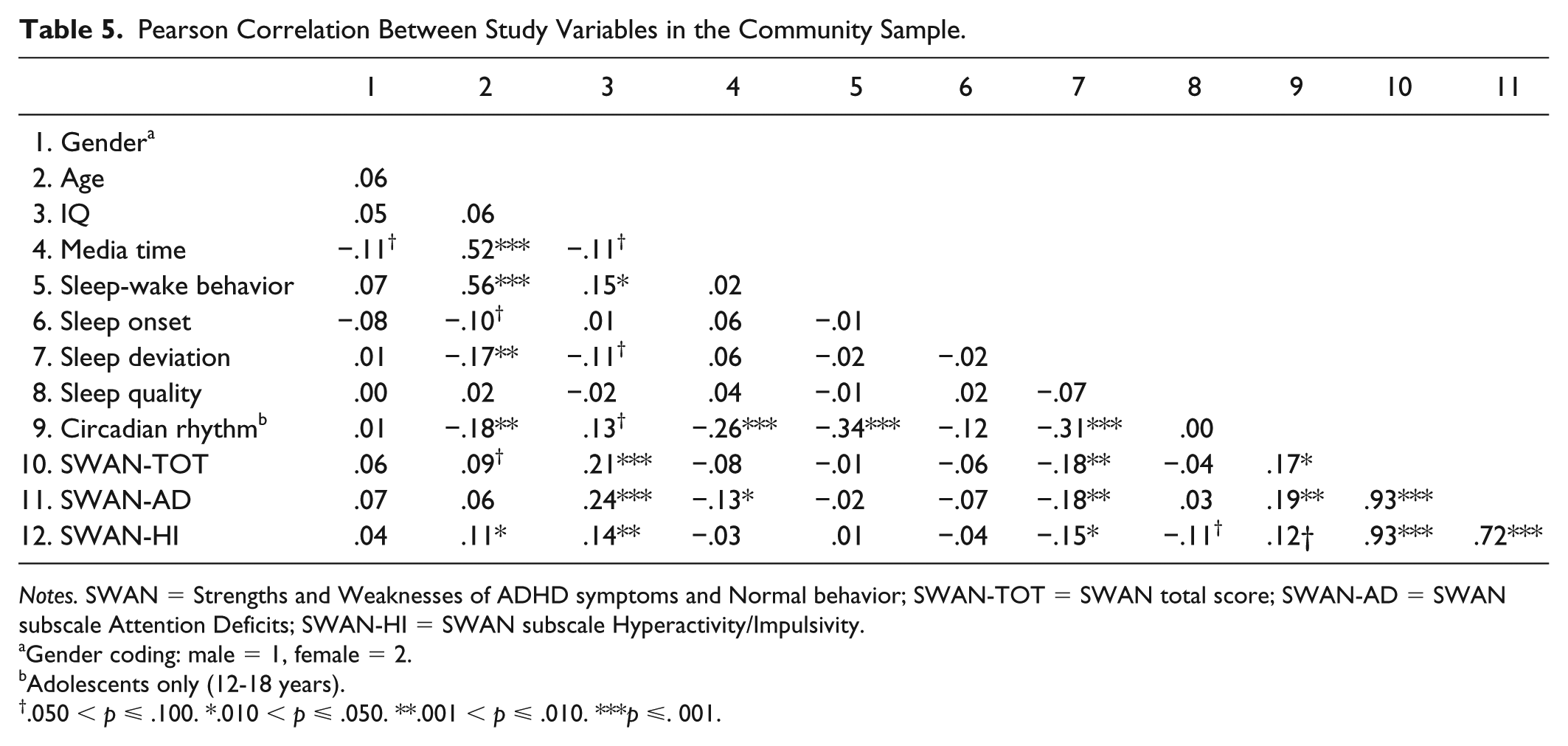
Notes. SWAN = Strengths and Weaknesses of ADHD symptoms and Normal behavior; SWAN-TOT = SWAN total score; SWAN-AD = SWAN subscale Attention Deficits; SWAN-HI = SWAN subscale Hyperactivity/Impulsivity.
Gender coding: male = 1, female = 2.
Adolescents only (12-18 years).
.050 < p ⩽ .100. *.010 < p ⩽ .050. **.001 < p ⩽ .010. ***p ⩽. 001.
Prediction of ADHD Symptomatology in the Community Sample
Due to the large age range (8-18 years), the community sample was further divided into smaller, more homogeneous groups (8-11 years and 12-18 years). Adolescents showed later bedtimes, decreased time to fall asleep on weekends, shorter sleep duration on school days, and reduced deviation from sleep requirement on weekends compared with children. They also reported more daytime sleepiness, but less nocturnal awakenings. With regard to media consumption, adolescents compared with children spent more time with electronic media during the day, as well as before going to bed. The reported group differences were all statistically significant (p ⩽ .05). Furthermore, 67% had at least one screen-based media device in their bedroom compared with 40% of the children, χ2(1.00) = 25.67, p ⩽ .001. There were no age differences in any of the SWAN (sub)scales.
For each age group, as well as for the total sample, a multiple regression analysis was conducted to assess whether sleep habits and media usage would contribute to the prediction of ADHD symptoms in children and adolescents from the general population. Therefore, three regression analyses with SWAN-TOT, SWAN subscale Attention Deficits (SWAN-AD), and SWAN subscale Hyperactivity/Impulsivity (SWAN-HI) as criteria were performed in each of the three groups. The results, presented in Table 6, showed that total ADHD symptomatology was predicted by deviation from subjective sleep need in the total age group, R2 = .04, F(5, 265) = 2.37, p = .040, and by adverse sleep-wake behavior in children, R2 = .13, F(5, 84) = 2.46, p = .039. In adolescents, the regression model showed no significance for the impact of sleep and media on ADHD-related behavior. Inattentive symptoms of ADHD in children were predicted by higher media time as well as unfavorable sleep-wake behavior, R2 = .15, F(5, 84) = 2.86, p = .020. Although the full regression model explained inattention in the total age group, R2 = .05, F(5, 265) = 2.83, p = .016, as well as in adolescents, R2 = .08, F(6, 172) = 2.33, p = .034, significantly, neither of its components alone showed a significant association with inattentive behavior. The regression model for hyperactive/impulsive behavior patterns failed to reach significance in all the three (sub)groups.
Multiple Regression Analysis Showing Standardized Regression Coefficients (β) for Prediction of ADHD-Related Behavior by Sleep and Media Habits in the Community Sample.
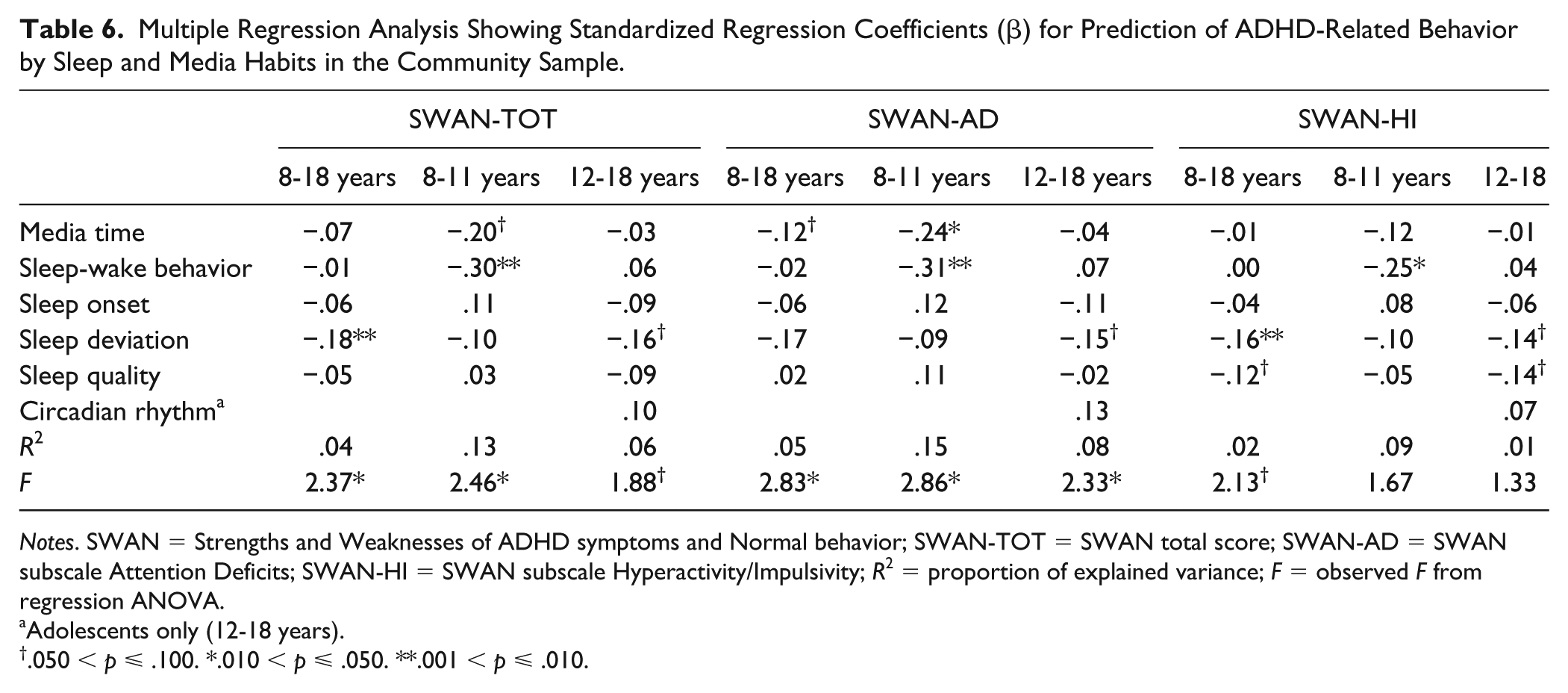
Notes. SWAN = Strengths and Weaknesses of ADHD symptoms and Normal behavior; SWAN-TOT = SWAN total score; SWAN-AD = SWAN subscale Attention Deficits; SWAN-HI = SWAN subscale Hyperactivity/Impulsivity; R2 = proportion of explained variance; F = observed F from regression ANOVA.
Adolescents only (12-18 years).
.050 < p ⩽ .100. *.010 < p ⩽ .050. **.001 < p ⩽ .010.
Further multiple regression analyses in each age group were performed for boys and girls separately. Results showed negligible gender differences concerning all regression models.
Discussion
This study set out to investigate the relation between subjective sleep parameters, screen-based media consumption, and symptoms of ADHD. To that end, we tested patients with ADHD and a large sample of healthy children and adolescents using sleep and media consumption questionnaires (Rey-López et al., 2012; Wolfson & Carskadon, 1998) as well as the German version of the SWAN ADHD symptom scale (Schulz-Zhecheva et al., 2019; Swanson et al., 2006).
Comparisons Between ADHD Patients and Controls (Matched Sample)
The main results for the matched sample can be summarized as follows: Regarding the obtained sleep parameters, patients suffering from ADHD reported a significant prolonged sleep-onset latency on school days, whereas adolescent patients tended to be at higher risk of delayed sleep phase. Furthermore, our study provides new and important insights into screen-based media use in children and adolescents with ADHD. Patients with ADHD reported to spend more than 4.5 hr with screen-based media on school days and exceeded the screen time of healthy participants by almost 2 hr.
Although previous studies on sleep in ADHD revealed increased overall prevalence of sleep-related complaints in young patients with ADHD, this could not be verified by our results. However, these studies mainly rest on parents’ ratings of sleep. Meanwhile, results from the few studies based on empirical self-report data as well as objective measures of sleep suggest that parents may tend to overestimate their children’s sleep problems: Owens et al. (2009) found low correlation between parent- and self-reported sleep patterns, whereas actigraphy data in children correlated well with data obtained using daily child diaries about sleep and daytime behaviors. Similarly, several studies assessing sleep in ADHD children with multiple measures showed, that the majority of the parent-reported sleep difficulties could not be verified through objective sleep data (Choi, Yoon, Kim, Chung, & Yoo, 2010; Corkum, Tannock, Moldofsky, Hogg-Johnson, & Humphries, 2001; Cortese et al., 2009; Hvolby, Jørgensen, & Bilenberg, 2008; Wiggs, Montgomery, & Stores, 2005). Corkum et al. (2001) conclude that challenging behaviors around bedtime may account for parents’ perception of problematic sleep patterns in children with ADHD. Therefore, parents may be more likely to remember and report all behavioral problems. Notwithstanding, the prolonged time of sleep onset in children with ADHD is one of the most commonly described sleep complaint, both in subjective and objective sleep studies (Cortese et al., 2009).
Regarding parameters assessing circadian tendencies in adolescents, patients from the current study showed more behavior that is related to a delayed sleep phase than healthy peers. This result supports findings from previous studies, reporting higher prevalence of DSPD in patients with ADHD (Coogan & McGowan, 2017). Given the frequently reported sleep-onset delays in children with ADHD, Van der Heijden et al. (2005) observed that DLMO, which is thought to be a reliable marker of the circadian phase (Klerman, Gershengorn, Duffy, & Kronauer, 2002), is markedly delayed in patients with ADHD-related sleep-onset insomnia. This is of particular relevance for clinicians, because coexisting delayed sleep phase can increase core symptoms of ADHD; meanwhile, chronotherapeutics (e.g., bright light, melatonin treatment) can improve sleep-onset time, advance evening increase in endogenous melatonin, and reduce ADHD symptom severity (Coogan & McGowan, 2017; Gruber, Grizenko, & Joober, 2007; Niederhofer, 2012; Snitselaar & Smits, 2014; Van der Heijden, Smits, Van Someren, Ridderinkhof, & Gunning, 2007). Taken together, these findings provide evidence for underlying delayed circadian phase in sleep-disturbed children with ADHD.
Furthermore, our study showed that screen-based media enjoy great popularity among patients with ADHD expressing in longer media use on school days, compared with healthy participants. As expected, total media time increased on weekends in both groups; however, patients’ screen time exceeded remarkable 5 hr per day, suggesting that affected children spend a great amount of their spare time with electronic devices. In support of our findings, there is evidence that girls and boys with ADHD are less frequently involved in traditional leisure activities, such as meeting with friends, sports, and acting/dancing, and express less enjoyment in extracurricular activities than typically developed children do (Bolic Baric et al., 2018; Shimoni, Engel-Yeger, & Tirosh, 2010). Bolic Baric et al. (2018) found that patients with ADHD prefer Internet-based channels to engage in social interactions with their peers, possibly to avoid confrontation with their behavioral difficulties and ascertaining feelings of competence (Shimoni et al., 2010). Moreover, in skill-based activities, such as sports, music, and acting/dancing, perseverance and motivation are influenced largely by one’s sense of achievement, whereas ADHD is linked to reward-motivation deficits and inability to delay gratification (Douglas & Parry, 1983, 1994; Rapport, Tucker, DuPaul, Merlo, & Stoner, 1986; Shimoni et al., 2010; Tripp & Alsop, 2001).
Until now, there has been a lack of studies on gender differences regarding sleep and media use in individuals with ADHD. In our study, we found no differences between boys and girls with ADHD.
Correlations Between the Study Variables in the Community Sample
Considering ADHD as a quantitative dimension, we found various significant correlations between sleep, screen-based media consumption on one side, and ADHD-related behavior on the other. Looking at relationships regarding ADHD-related symptoms, there was a significant positive correlation between time spent with electronic media and attention problems. This is in accordance with a meta-analysis, showing that screen time is more strongly associated with symptoms of inattention than with hyperactivity/impulsivity (Nikkelen et al., 2014). Furthermore, our study revealed that sleep deviation was significantly related to the entire ADHD core symptom triad as well as to inattention and hyperactivity/impulsivity separately. To our knowledge, this is the first study considering both too little and too much sleep (i.e., deviation from individual sleep requirement in either direction) when assessing behavioral difficulties. Although physiological pathways and consequences of insufficient sleep have been thoroughly investigated and demonstrated (Beebe, 2011), research on cognitive and behavioral consequences of prolonged sleep is still a largely unknown field. In addition, we found later circadian rhythmicity to be associated with more ADHD symptoms, corroborating nicely previous work on the association of symptoms of ADHD with eveningness and DSPD (Caci, Bouchez, & Baylé, 2009; Sivertsen, Harvey, Pallesen, & Hysing, 2015; Van der Heijden, de Sonneville, & Swaab, 2013; Voinescu, Szentagotai, & David, 2012). Moreover, Tzischinsky and Shochat (2011) found that evening types show more sleep problem behavior and sleepiness compared with morning types.
Prediction of ADHD Symptomatology in the Community Sample
Overall, our findings showed that screen-based media time, unfavorable sleep-wake behavior, and amount of sleep deviation are significantly related with composite ADHD-like behavior and attention problems, whereas no such relationship was found for symptoms of hyperactivity/impulsivity. In contrast to previous research, this study not only covers a relatively wide age range but also our methodical approach allowed us to compare children and adolescents. We could show that symptoms of ADHD were differently predicted in the age groups and, therefore, provide important additional information for potential interventions: In children, especially screen time and sleep-wake behavior, whereas in adolescents, most likely sleep deviation was associated with ADHD symptomatology. Hence, our results are in agreement with recommendations by the American Academy of Pediatrics (AAP) to limit children’s daily sedentary screen time to no more than 1 to 2 hr (AAP, 2001; AAP Council on Communications and Media, 2016) and emphasize the importance of the consequent implementation of good sleep hygiene. In adolescents, the combination of circadian changes toward a later sleep phase as well as environmental factors, including leisure activities, homework load, or constant engagement in screen-based media, may interfere with sleep timing and duration (Lufi, Tzischinsky, & Hadar, 2011). Therefore, this age group might benefit from appropriate sleep-wake times to ensure getting the right amount of sleep, which, in turn, positively affects cognitive and academic functioning (Dahl, 2005; Fallone, Acebo, Seifer, & Carskadon, 2005; Lufi et al., 2011).
Additional Findings From the Community Sample
According to our results, age plays a significant role, with older children reporting more adverse media and sleep habits. The observed age differences in screen-based media behavior reflect the expected usage patterns and have been widely reported (Pedagogical Media Research Centre Southwest, 2016, 2017; Rideout, 2015). Meanwhile, as there are no age-related changes regarding sleep requirement across adolescent development (Carskadon, 2011), the strong relationship between age and sleep-wake behavior may be due to profound changes in circadian rhythms, manifested in later bedtimes, rising times, and diminished sleep time during puberty. This hypothesis is supported by our findings, that in older children circadian preference tends toward eveningness. Similarly, media time was strongly correlated with measurement of circadian profile. That is in line with previous work showing that evening types engage more in screen-based media; however, altogether less data are currently available (Kauderer & Randler, 2013; Urbán, Magyaródi, & Rigó, 2011; Vollmer, Michel, & Randler, 2012). But given the presented relationships between both sleep and media habits with circadian rhythm, the question arises whether chronotype acts as a probable confounder, particularly with regard to technology-related prebedtime behaviors (Harbard, Allen, Trinder, & Bei, 2016).
We found an inverse relationship between participants’ IQ and their sleep-wake behavior. This result replicated previous reports indicating that higher cognitive abilities are related to later bedtimes and shorter sleep duration; however, our correlational findings were weaker (Geiger, Achermann, & Jenni, 2010; Kanazawa & Perina, 2009). One possible explanation is provided by Geiger et al. (2010). The authors argue that children with short night sleep, in turn, may benefit from a longer waking state, which offers cognitive, social, and multisensory stimulation contributing to child’s development. But more research needs to be done in this area.
In line with prior general population studies, we found that children and adolescents with higher IQ scores showed less symptoms of ADHD (Fergusson, Horwood, & Lynskey, 1993; Goodman, Simonoff, & Stevenson, 1995; Simonoff, Pickles, Wood, Gringras, & Chadwick, 2007). In addition, findings from a longitudinal study, on how ADHD symptomatology and IQ influence one another, identified core symptoms of ADHD at age 12 years as a strong predictor of IQ scores, suggesting ADHD-related behavior may put adolescents at risk of lower IQ 2 years later (Rommel, Rijsdijk, Greven, Asherson, & Kuntsi, 2015).
Limitations of the Present Study and Directions for Future Research
To the best of our knowledge, the present study is the first to investigate media consumption and sleep conjointly regarding their potential relationship with ADHD symptomatology. Although we do indeed find significant relationships between these constructs, as discussed before, looking at the effect sizes, we find that some of the relationships correspond to large effects, most of them to lower medium effect sizes, and some of them to smaller effect sizes.
Finding, overall, mainly medium-to-small effect sizes points to a major limitation of the present study, namely, that it is based exclusively on questionnaire data. Such data provide, in general, only limited reliability, and this holds in particular if subscales are composed of few items only, as is the case in our study. If, however, the reliability of a measure is low, its correlation with another measure cannot be high.
Therefore, the fact that we do find significant associations between the core constructs of this study despite the relatively low reliability of our measures is indeed suggestive of a true association between ADHD, media consumption, and sleep that is worth being further explored with more sophisticated and psychometrically reliable tools.
Future research should employ multimethod assessments, combining observation (e.g., sleep diaries or sleep logs) and objective (e.g., actigraphs with integrated light sensor) methods to add validity. Media consumption could be estimated by proactive ecological momentary assessment (EMA; Stone & Shiffman, 1994) or smartphone-based sampling methods, asking participants continuously or at random to record any electronic media they are using. Similarly, further information on regular weekly activities (e.g., sports, social interactions) and different aspects of current well-being (e.g., mood, stress, sleepiness) should be obtained and taken into consideration.
With respect to the nature of the media use, content as well as different conditions of use (passive vs. active, parent accompanied vs. alone) should be obtained, as this distinction will lead to a more precise classification of screen time (Sweetser, Johnson, Ozdowska, & Wyeth, 2012), providing important information to further specify the role of screen-based devices, especially when assessing sleep problems and behavior.
Furthermore, data collection should be carried out over a time period of sufficient length and include at least two weekends to reflect habitual sleep and media use behavior and to minimize the influence of illness, unusual circumstances, or other intervening factors.
Subsequent studies should also control for socioeconomic background and psychosocial characteristics not only in patients with ADHD but also in community samples, as these factors may have potential impact on behavior too.
Finally, because we used cross-sectional data, we are unable to draw causal links. Longitudinal or experimental studies are necessary to further investigate the dynamic relationships between sleep, screen-based media use, and symptoms of ADHD.
Conclusion
This study provides insights into the association between sleep, media use, and ADHD-related behavior among a German, 8 to 18 years old, population. Compared with healthy peers, on school days, patients with ADHD need more time to fall asleep and reported increased screen-based media consumption, whereas affected adolescents are more likely to show symptoms of delayed sleep phase. Furthermore, our findings from the community sample allow us to conclude that children and adolescents with longer media time, more inadequate sleep-wake behavior, and more deviation from their individual sleep need are at significant higher risk to show behavioral problems with symptoms of ADHD. Given the fact that screen-based media use is at an all-time high and the vital role of sleep during development, children and adolescents of all ages might benefit from education and information when it comes to negative effects associated with heavy media exposure and bad sleep.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Deutsche Forschungsgemeinschaft (Kl 985/13-1).